
Abstract
Background:
To explore the association between functional limitation due to subjective cognitive decline (SCD) and falling by focusing on exercise intensity in the Korean population aged 45 years and older.
Study Design:
The 2019 Korean Community Health Survey (KCHS) was used to analyze 35,387 people by applying individual weights imposed from the raw data.
Methods:
To analyze the association between functional limitation due to SCD and falling in the Korean population aged 45 years and older, weighted logistic regression analysis and weighted zero-inflated Poisson regression analysis were used.
Results:
In both the middle-aged group and the older adult group, the functional limitation due to SCD had a higher fall experience rate and more falls than the non-functional limitation due to SCD group. Additionally, the middle-aged group and the moderate or vigorous physical exercise (MVPE) group had a higher fall experience rate and number of falls than the non-MVPE group; however, the older adult group walking regularly and performing MVPE had a lower fall experience rate and number of falls than the non-exercise group.
Conclusions:
Active participation in exercise is encouraged and should lead to fewer falls in older adults. Furthermore, a group with functional limitations due to SCD should be provided with exercise guidelines and a community program and facilities that enable regular participation should be developed.
Introduction
Korea National Statistical Office in 2021 announced that the older adult population in Korea, which comprised 16.5% of the total population, had entered an aged society; the proportion of the middle-aged and older adults population in Korea is 56.5%, showing the fastest growth rate among the Organisation for Economic Cooperation and Development (OECD) member countries. 1 The increase in the middle and old age population is accompanied by various social problems 2 ; in particular, it affects the onset of cognitive disorders such as Alzheimer’s disease and mild cognitive impairment. 3 Therefore, recent studies on subjective cognitive decline (SCD), which is considered an early prevention index to arrest cognitive impairment, are being actively conducted. 4 SCD is experienced by 11% of the population aged 45 and over in the United States 3 ; in Korea, 24.6% of the middle and old age population experience SCD, indicating that Korea’s SCD experience rate is higher than other countries. 5 Compared to the younger population group, SCD in older adults occurs with age, resulting in decreased cognitive as well as physical function 6 and 50.6% of middle-aged and older Americans who experienced SCD experienced functional limitations. 3 According to the U.S. Centers for Disease Control and Prevention (CDC), functional limitations due to SCD are defined as the inability to perform activities due to limitations in cognitive and physical abilities to perform household chores, medication use, and social activities. 7 Naturally, functional limitation due to SCD leads to decreased physical movements, increased falls and the number of falls.8–10 In particular, the fall experience rate of the functionally limited group in Korea was more than twice that of the non-functionally limited group. 11
In the functional limited group, physical exercise is considered an important factor in preventing falls by slowing the rate of decline and sarcopenia. 12 Due to its importance, there is an attempt to actively intervene in exercise programs to prevent falls in middle-aged and older adults with functional limitations.13–15 In particular, the American Geriatrics Society (AGS) provides detailed guidelines based on exercise intensity, such as regular walking exercise (RWE) and moderate or vigorous physical exercise (MVPE), which can be done by the older people in their local community. 13 The group with functional limitations has effectively reduced the fall experience rate by 32% by providing exercise guidelines with relatively easy exercise intensity, time and frequency.14,15
Nevertheless, as exercise programs and guidelines for fall prevention are not universally active worldwide, 16 the number of falls continues to rise, 17 resulting in accidental deaths of older adults in the United States. Furthermore, 42% of total medical expenses are related to falls.17,18 Falls cause various social problems and are considered among the most urgent public health problems among middle-aged and older adults. 19
Moreover, in Korea, compared to foreign countries, due to the tendency of middle-aged and older people to avoid physical exercise 20 and a lack of physical exercise programs to prevent falls, 21 the rate of physical activity is also in steady decline, from 58.3% in 2014 to 47.8% in 2019. 22 The fall experience rate among middle-aged and older adults with functional limitations is also high. 11 Compared to overseas countries, the middle-aged Korean group is more susceptible to functional limitations due to SCD and falls.
This study focuses on the rapidly growing middle-aged and older population in Korea. Previous studies show that the rate of experience with functional limitation due to SCD is high, but physical exercise is low,1,5,8–10 and that falls and the number of falls can be reduced through physical activity.14,15 The aim of this study was to examine the relationship between functional limitation due to SCD and falls, as well as the number of falls depending on whether exercise was undertaken and the exercise intensity of middle-aged and older adults in Korea. In addition, we intend to provide baseline data for enacting policies and institutional measures to prevent falls by advocating for physical exercise for groups vulnerable to falls.
Methods
Study design
This study used the 2019 Korea Community Health Survey (KCHS) surveyed by the Korea Ministry of Health and Welfare’s KDCA (Korea Disease Control and Prevention Agency). It is a secondary analysis study that uses raw data from Korea Community Health Surveys and related pledges to investigate the association between functional limitation due to SCD and falling, the number of falling for middle-aged group and old-aged group living in Korea, and used them for analysis after approval of data requests. The KCHS was conducted to establish and evaluate health policies by securing local health statistics according to the implementation of the local government system to understand the health status of local residents. In addition, it will be used as basic data for calculating health statistics at the city, county, and district levels necessary for establishing local health care plans, expanding infrastructure, and evaluating the performance of local health projects. The Korea community health survey is an annual sample survey of 251 public health centers in 16 cities/province since 2008, and was extracted using a systematic extraction method in consideration of the number of households based on the number of households by type of house in Tong, Ban/ri. In addition, this is the data surveyed so that representative samples can be extracted from adults aged 19 or older among the sample household members. A total of 229,099 people participated in the 2019 Korean Community Health Survey, and trained investigators visited sample households in person and conducted measurement surveys and 1:1 interviews.
This study analyzed the association between functional limitation due to SCD and falling, the number of falling of the middle-aged group (45–64 years) and the old-aged (Over 65 years) group by applying individual weights imposed on 35,387 people, excluding 66,627 people under 45 years of age and people diagnosed the dementia, 126,589 missing values for functional limitation due to SCD, 59 missing values for falling and the number of falling, 437 missing values for control variables
Independent variables
Independent variable was functional limitation due to SCD. SCD was self-observed impairment of more frequent or worsening of memory loss or confusion within the prior 12 months. SCD and functional limitation due to SCD were measured by the Behavioral Risk Factor Surveillance System (BRFSS), “During the last year, have you experienced memory loss or confusion getting worse or happening more often?“” If participants indicated that SCD was present, they were asked about functional limitation due to SCD, as follows: “During the last year, how often have your day-to-day activities (ex: cooking, cleaning, taking medicine, driving, or paying bills, etc.) been hindered or needed help because of your confusion or memory loss?”; “If you needed help in daily life because you were confused or your memory was poor, how often did you receive help when you needed it?”; and “During the last year, how often have you been disturbed in your work life, volunteering, and social activities?” The response categories included always, usually, sometimes, rarely, or never. functional limitation due to SCD was identified by memory loss or confusion that disturbed the participants’ work life, volunteering, and social activities, or day-to-day activities (e.g. cooking, cleaning, taking medicine, driving, or paying bills). This study classified these responses into two groups as follows: functional limitation due to SCD group (always, usually, or sometimes) and non-functional limitation due to SCD group (rarely or never).
Dependent variables
The dependent variables in this study were falling and the number of falls. A falling was defined as one or more falls in the past 12 months. To assess the history of falling, participants were asked “whether they had fallen during the past 12 month”; If the response was “yes,” the response was defined as a fall experience group, and if the response was “no,” it was defined as a fall experience group. Also, the number of falls was defined in response to “How many times have you fallen during the past 1 year ?.”
Control variables
In this study, predefined data such as “Sex,” “Education level,” “Marital status,” “Residential area,” and “Household monthly income” of the community health survey were selected as variables. sex was classified into “male” and “female.” Marital status was classified into “married” and “single (including separated, divorced).” Education level was classified into “elementary school graduates or lower,” “middle school graduates,” “high school graduates,” and “college graduates or higher,” and residential areas were classified into “Capital area,” “ Metropolitan city” and “ Rural area.” and household monthly income was classified into “≤ 100,” “100–200,” “200–300” and “≥ 300.” As variables for health behavior factors, predefined data such as “Smoking status,” “Drinking status,” “Regular Walking,” “Moderate or vigorous Exercise,” “Self-rated health,” “Perceived stress level,” “Diabetes diagnosis” and “ Hypertension diagnosis” were selected as variables. Smoking status and Drinking status were classified as “Ever” and “Never.” Regular Walking and Moderate or vigorous Exercise were classified into “Yes” and “No.” Self-rated health and Perceived stress level were classified into “very,” “less” and “low.” Diabetes diagnosis and Hypertension diagnosis were classified into “Yes” and “No.”
Analytical approach and statistics
In this study, to analyze the association between functional limitations due to SCD and falls, the number of falls in the middle-aged and old-aged group, after controlling the correction variables of the study subjects, to check the difference in the distribution of the dependent variable according to the independent variable, the Rao-Scott Chi square test was used for the “Whether or not falls” dependent variable. and Mann-Whitney U (for two-group comparisons) or Kruskal-Wallis test (for more than two-group comparisons) was used for the “number of falls” dependent variable. In addition, weighted logistic regression analysis was used to investigate the association between functional limitations due to SCD and falls, and weighted zero-inflated Poisson regression analysis was used to investigate the association between functional limitation due to SCD and the number of falls. For all analyses, the criterion for statistical significance was p ≤ 0.05, two tailed. All analyses were carried out using the SAS statistical software package, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Table 1 shows the general characteristics of participants in determining the relationship between functional limitation due to SCD and falls and the number of falls among the middle-aged and older adult groups.
General characteristics of subjects included for analysis.

RWE: Regular Walking Exercise; MVPE : Moderate or Vigorous Physical Exercise.
Number of Falling*: experienced falling down at least once in the past 1 year.
Weighted.
Rao Scott chi square test.
Mann-Whitney U or Kruskal-Wallis test.
In the middle-aged group, of the total of 14,122 participants, the fall experience rate was 18.2% (n = 2551), and the mean number of falls was 1.83. The percentage of middle-aged people with functional limitations due to SCD was 20.2% (n = 2875). The fall experience rate for this group was 27.7% (n = 799), and the mean number of falls was 2.20.
In the older adult group, of the total of 21,265 participants, the fall experience rate was 24.1% (n = 5146), and the mean number of falls was 1.79. The percentage of older people with functional limitations due to SCD was 36.3% (n = 7915). The fall experience rate in this group was 31.3% (n = 2405), and the mean number of falls was 2.00.
Table 2 shows the results of the control variable correction to determine the association between functional limitation due to SCD and falls and the number of falls among the middle-aged and older adult groups.
Factors associated with falling in the group of Functional limitation due to SCD.

RWE: Regular Walking Exercise; MVPE: Moderate or Vigorous Physical Exercise.
Falling*: Weighted logistic regression analysis predicting the likelihood of experiencing a falling in the past 1 year among all participants.
The number of falling*: Weighted zero-inflated Poisson regression analysis predicting the number of falling in the past 1 year among all participants.
Weighted.
In the middle-aged group, functional limitation due to SCD group had a higher fall experience rate (Odds Ratio [OR]:1.58, 95% Confidence Interval [CI]:1.40–1.79) and also had more falls (Incidence Rate Ratio [IRR]:1.41, 95% CI:1.40–1.42) than the non-functional limitation due to SCD group. In the older adult group, functional limitation due to SCD group had a higher fall experience rate (OR:1.40, 95% CI:1.29–1.53) and also had more falls (IRR:1.41, 95% CI:1.40–1.41) than the other group.
Table 3 shows the subgroup analysis results of the association between functional limitation due to SCD and falls based on exercise was undertaken and exercise intensity among middle-aged and older adult groups.
The association between Functional limitation due to SCD and Falling by RWE and MVPE.
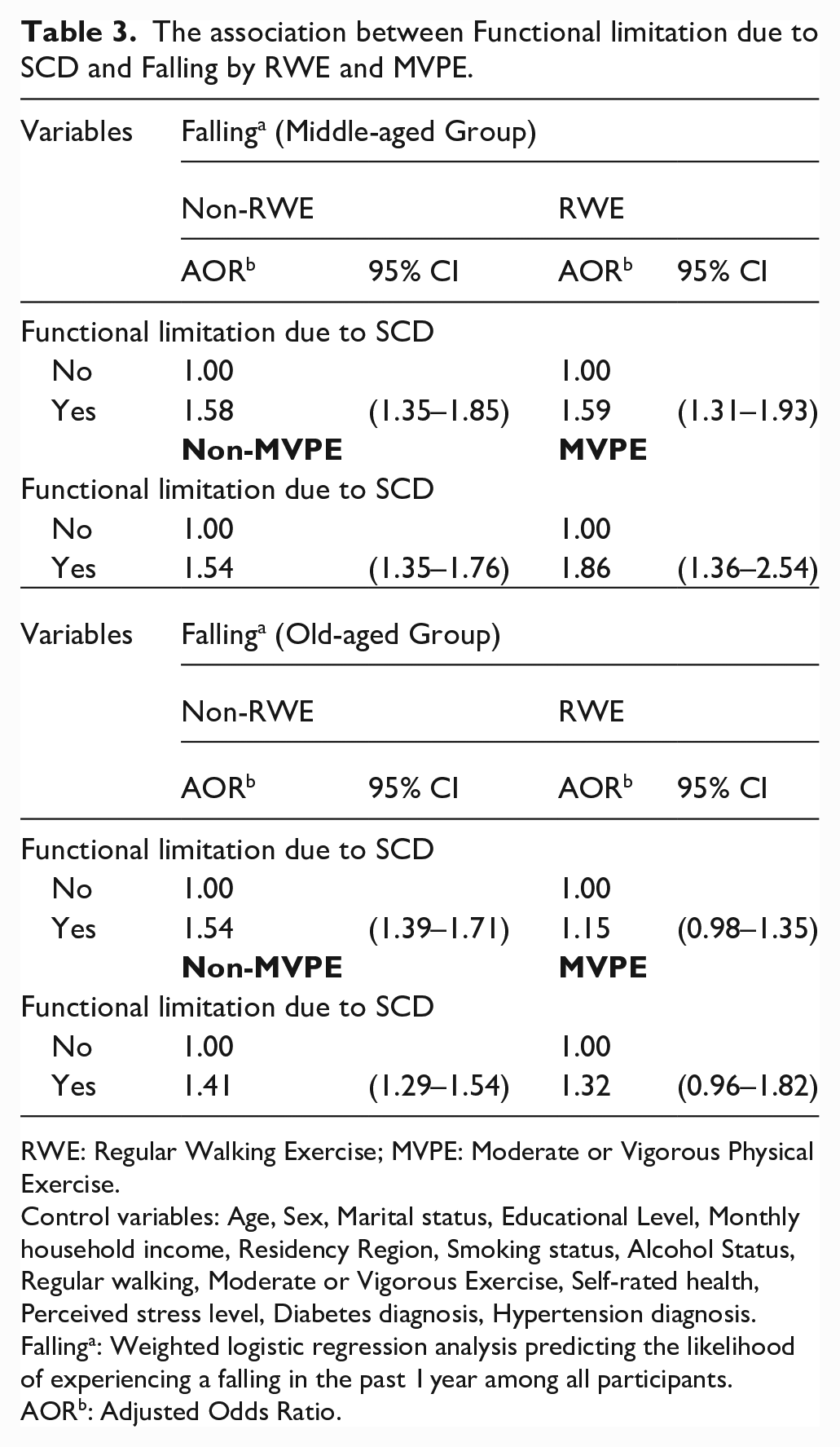
RWE: Regular Walking Exercise; MVPE: Moderate or Vigorous Physical Exercise.
Control variables: Age, Sex, Marital status, Educational Level, Monthly household income, Residency Region, Smoking status, Alcohol Status, Regular walking, Moderate or Vigorous Exercise, Self-rated health, Perceived stress level, Diabetes diagnosis, Hypertension diagnosis.
Fallinga: Weighted logistic regression analysis predicting the likelihood of experiencing a falling in the past 1 year among all participants.
AORb: Adjusted Odds Ratio.
In the middle-aged group, there was no difference in the fall experience rate between the RWE and non-RWE groups, but the fall experience rate of the MVPE group was higher than the reference group (OR:1.54, 95% CI:1.35–1.76), while the fall experience rate for the non-MVPE group was higher than the reference group (OR:1.86, 95% CI:1.36–2.54).
In the older adult group, the fall experience rate of the non-RWE group was higher than the reference group (OR:1.54, 95% CI: 1.39–1.71), whereas the fall experience rate of the RWE group was higher than the reference group (OR:1.15, 95% CI:0.98–1.35). The fall experience rate of the non-MVPE group was higher than the reference group (OR:1.41, 95% CI:1.29–1.54), whereas the fall experience rate of the MVPE group was higher than the reference group (OR:1.32, 95% CI:0.96–1.82) (Figure 1).

Adjusted effect between functional limitation due to SCD and falling by the intensity of exercise.
Table 4 shows the subgroup analysis results of the association between functional limitation due to SCD and the number of falls based on exercise and exercise intensity among the middle-aged and older adult groups.
The association between Functional limitation due to SCD and the Number of falling by RWE and MVPE.
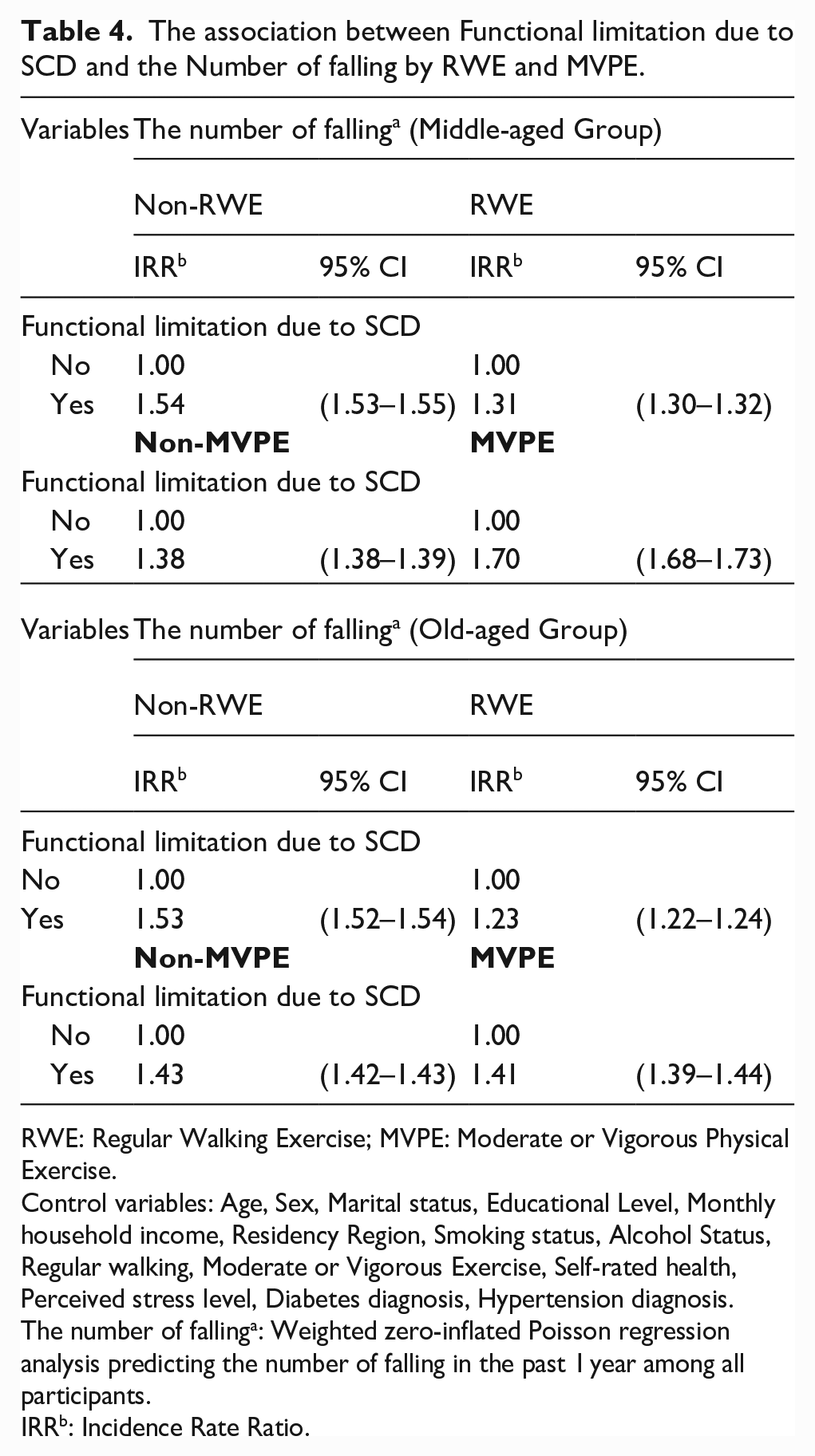
RWE: Regular Walking Exercise; MVPE: Moderate or Vigorous Physical Exercise.
Control variables: Age, Sex, Marital status, Educational Level, Monthly household income, Residency Region, Smoking status, Alcohol Status, Regular walking, Moderate or Vigorous Exercise, Self-rated health, Perceived stress level, Diabetes diagnosis, Hypertension diagnosis.
The number of fallinga: Weighted zero-inflated Poisson regression analysis predicting the number of falling in the past 1 year among all participants.
IRRb: Incidence Rate Ratio.
In the middle-aged group, the number of falls in the RWE group was lower than in the non-RWE group (IRR:1.31, 95% CI:1.30–1.32), but the MVPE group had a higher number of falls than the non-MVPE group (IRR:1.70, 95% CI:1.68–1.73).
In the older adult group, the number of falls in the RWE group was lower than that in the non-RWE group (IRR:1.23, 95% CI:1.22–1.24), and the number of falls in the MVPE group was lower than that in the non-MVPE group (IRR:1.41, 95% CI:1.39–1.44) (Figure 2).

Adjusted effect between functional limitation due to SCD and the number of falling by the intensity of exercise.
Discussion
With the rapid increase of the population aged 45 and over in Korea, the rate of experience with functional limitations due to SCD has also increased. 5 Despite physiological weakness due to aging and the reduction and avoidance of physical exercise, they become more vulnerable to falls.8–10 There have been no studies on the relationship between functional limitation due to SCD and falls. Therefore, using the 2019 KCHS on adults, this study aimed to present basic policy and institutional data to prevent falls among this vulnerable group by analyzing the functional limitations due to SCD and falls in relation to exercise and exercise intensity among middle-aged and older adults.
The results are summarized as follows: In the middle and older age groups, the group with functional limitation due to SCD had a higher fall experience rate and a higher number of falls than the non-functional limitation group. Additionally, when analyzing the association between functional limitation due to SCD and falls according to whether exercise was performed and its intensity, in the middle-aged group, the RWE group had a higher fall experience rate and lower number of falls than the non-RWE group. Furthermore, the experience rate and the number of falls for the MVPE group were higher than for the non-MVPE group. By contrast, in the older age group, the RWE and MVPE groups had lower fall experience rates and fewer falls than the non-exercise group.
The study’s findings, that the fall experience rate and the number of falls in the functional limitation due to SCD group were higher than those in the non-functional limitation group, are consistent with previous studies23–32. SCD, which has a high incidence among middle-aged and older adults, can induce psychological effects, such as depression and stress, that could increase the risk of falls 23 In particular, according to a previous study that analyzed the relationship between SCD and falls in 92,323 middle-aged and older adults, SCD caused problems in executive functions that connect cognition to behavior, causing difficulties in walking stability and maintaining posture. The SCD group had a 1.61 OR higher fall experience rate than the non-SCD group.24,25 Furthermore, when SCD leads to functional limitations with physical difficulties, the fall rate increases by 40%. 26 According to a previous study in the United States, the group experiencing functional limitations due to SCD needed the help of others for indoor and outdoor activities because of poor health and various diseases. 8 As a result, RWE and MVPE participation rates were significantly lower 27 ; rather, the increase in sedentary static exercise did not meet the amount of physical activity needed to prevent falls. 28 Consequently, the weakening of the musculoskeletal and neuromuscular systems, which can replace the center of gravity and balance,29,30 sarcopenia due to aging and muscle weakness due to decreased exercise, makes them more vulnerable to falls.31,32
In addition, the results of this study, that exercise performed in the older age group with functional limitation due to SCD was associated with decreased falls, are also consistent with previous studies.33–36 According to a previous study,33–35 as a result of intervening in RWE for 30 min or more, 5 days per week and MVPE for 20 min per day to prevent falls in older adults over the age of 65 with cognitive impairment, the mismatch in executive function, which was the cause of falls, was improved, and the fall experience rate decreased by 30%. In addition, as cardiac output and oxygen consumption increased, cerebral blood flow also increased. As a result, exercise in the older age group had a greater effect on fall prevention than in the middle-aged group. 36
In this study, the result that the middle-aged MVPE group had a higher fall experience rate and number of falls than the non-MVPE group is consistent with previous studies.37–39 As a result of a follow-up on 2193 Americans aged 45 and over for 5 years, the overall level of physical health of the middle-aged was higher than that of older adults. As a result of high level of outdoor activity and subjective health awareness, the fall rate of the middle age group was 24.6% higher than the older adults performing high intensity exercises. Among the middle-aged group with functional limitations, there was a stronger association with falls [37]. This was because older people had lower health awareness and used fewer outdoor activities than the middle-aged, and improving their physical health through MVPE and RWE. The fall experience rate and number of falls among the older people were relatively lower than those of the middle-aged.37–39 In addition, according to a previous study, the fall experience rate for older people with cognitive decline and functional limitations decreased by 34% when they were provided with a customized exercise program that performed walking exercises at an appropriate and fast pace (pace of 10 m) or performed MVPE 10 times to overcome virtual obstacles. 40
However, according to an announcement from the Korean Ministry of Health and Welfare, no exercise facilities and programs in the local community were provided for the middle-aged group. In 2019, the RWE and MVPE practice rates among middle-aged and older adults were 39.9% and 33%, respectively, which did not consistently achieve the target rates set at the beginning of the project. 41 In particular, the rate of physical exercise practice among older people, who can effectively prevent falls through exercise, was 22.4% in Korea compared to 33.5% in Japan, which was lower than in other countries. 42
This study hopes to help prevent falls and improve physical health by encouraging appropriate policy and institutional exercise guidelines, exercise programs that encourage regular participation, and physical exercise environments for older people with functional restrictions.
This study had some limitations. First, we were unable to identify a causal relationship between functional limitation due to SCD and falls and the number of falls because the study was cross-sectional. Second, because of limited data, we were unable to use accurate measures, such as biomarkers, to measure functional limitations due to SCD. In addition, functional limitations due to SCD were self-reported and therefore did not imply a diagnosis of cognitive impairment. Thus, it was impossible to determine whether participants were cognitively impaired. Third, functional limitation due to SCD measurement could result in greater bias when people subjectively evaluate themselves. Using the mean value of several functional limitations due to SCD measured within a certain time period (e.g. 1 week) in a single participant may be a more reliable method of determining the functional limitation due to SCD. Finally, our study did not assess a dementia variable, which is a confounding factor in the weighted logistic regression model between functional limitation due to SCD and falling.
However, this study has several strengths. First, this was the first study to analyze the association between functional limitation due to SCD and falling. Second, it used national survey data as well as imposed weights on individuals in the population, so the results represent the entire Korean population among adults over the age of 45. Third, this study investigated a variety of variables, such as socio-economic characteristics (e.g. age, gender, area of residence, education status, marital status, and family income), chronic diseases (diabetes and hypertension), perceived stress level and health-related behaviors (e.g. drinking alcohol, smoking, self-rated health). Fourth, unlike prior studies that focused on the relationship between SCD and falling or depression, this study focused on this relationship in older adults who are most vulnerable to functional limitations due to SCD and falls.
Conclusions
This study investigated the relationship between functional limitation due to SCD and falls in middle-aged and older individuals using the 2019 KCHS, a survey of adults living in Korea. The study found that the functional limitation group due to SCD had a higher number of falls than the non-functional limitation group, and falls and the number of falls were relatively reduced when RWE and MVPE were practised in the older adult group compared to the middle-aged group. In old age, the amount of physical exercise decreases rapidly, and it is predicted that falls can be reduced by encouraging active exercise participation by providing functional them with exercise guidelines for the prevention of falls, exercise programs that encourage regular participation and an exercise environment.
Footnotes
Acknowledgements
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education (NRF-2021R1A6A3A01086576).
Author contributions
Jeong Min Yang designed this study, performed statistical analysis, drafted and completed the manuscript. Hyeon Ji Lee contributed to the concept and design of the study, and provided statistical expertise and interpretation. Jae Hyun Kim conceived, designed and directed this study. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The data is an open access dataset and did not contain any personal information on patients, therefore no ethical approval was required.
Patient consent for publication
Not required.
Data availability statement
Data are owned by and are available from the database of Korea National Health and Nutrition Examination Surveys (KNHNES) https://knhanes.kdca.go.kr/knhanes/main.do. KNHNES allows all of this data freely for any researcher who promises to follow the research ethics. The data that support the findings of this study are openly available in the Korea Community Health Survey at ![]() .
.