
Abstract
Background:
Occupational hazards believed to cause musculoskeletal disorders in rope workers are traditionally associated with maintaining incongruous postures for prolonged periods of time.
Design and methods:
A cross-sectional survey was conducted on 132 technical operators in the wind energy and acrobatic construction sectors, who work on ropes, analysing the ergonomic characteristics of the environments, the way in which tasks are carried out, the strain perceived by individual workers, and assessing the presence of any musculoskeletal disorders (MSDs) by means of an objective examination focused on the anatomical districts that were the object of our study.
Results:
Analysis of the data obtained showed that there were differences in the perception of the level of physical intensity and perceived exertion between the groups of workers. Statistical analysis also revealed a significant association between the frequency of MSDs analysed and perceived exertion.
Discussion:
The most significant finding to emerge from this study is the high prevalence of MSDs of the cervical spine (52.94%), the upper limbs (29.41%), and the dorso-lumbar spine (17.65%). These values differ from those classically found in those exposed to the risk of conventional manual handling of loads.
Conclusions:
The high prevalence of disorders of the cervical spine, the scapulo-humeral girdle and the upper limbs, indicates the need to consider the forced position to be assumed for a large part of the work activity, staticity, and the inability to move the lower limbs for long periods as the predominant risk in rope work.
Keywords
Introduction
Occupational hazards believed to cause musculoskeletal disorders in technical operators in the field of wind energy and aerobatic construction are traditionally associated with performing tasks in confined environments and at heights that involve maintaining incongruous, non-ergonomic postures for prolonged periods of time, with the inability to use all the systems to reduce the manual handling of loads, commonly used in conventional physical activities. 1
The protection measures provided for workers exposed to such risks are regulated by the rules described in Title IV in Chapter II ‘rules for the prevention of accidents at work in construction and work at heights’ of Legislative Decree 81/08 and s.m.i. and in Presidential Decree 177/11 ‘personnel working in environments suspected of pollution or confined’.2,3 In Italy, however, protective initiatives for workers exposed to manual handling of loads generally include health surveillance measures. These measures are linked to the type of activity carried out, which on a daily basis may entail the need for workers to assume obligatory postures for prolonged periods of time that can lead to a biomechanical overload of the musculoskeletal system, predisposing to the onset or aggravation of symptoms affecting various anatomical districts. 4
With regard to the role of postures assumed during work at height, often on ropes or other elevation systems, it is difficult to determine its specific impact on the onset of musculoskeletal disorders. It is probably for this reason, together with the problems associated with the criteria for defining musculoskeletal disorders of the spinal column and upper limb,5,6 that few studies have been conducted to date on these new types of work activities. However, the information that can be obtained from health surveillance could provide preliminary elements, which can be defined as ‘sentinel events’, capable of representing a first step in assessing the extent of the risk, which can be further investigated in subsequent phases, including through the use of more specific assessment methods. 7
The main objective of our work was to determine the prevalence indices of musculoskeletal disorders (MSDs) in a sample of technical workers in the field of renewable energy and construction, who carry out a large part of their activity working at height, using various fall-prevention devices as a protection system, including double rope systems or basket work, and thus assuming obligatory incongruous postures for prolonged periods of time. A further aim of our study was to assess the existence of possible associations between MSDs and the demographic, occupational characteristics of the workers in our sample.
Materials and methods
The number of specialised workers subject of our study was 132 subjects, belonging to the professional categories of workers specialised in working at heights, employed in the installation and maintenance of wind turbine blades, and in acrobatic construction, which normally involve the need to assume incongruous compulsory postures during the work shift at wind farms, or construction sites without scaffolding where the activities are carried out exclusively on ropes. The data of 18 workers were not included in the statistical analysis, since specifically 3 were absent due to illness, 6 did not agree to participate in the study, and 9 had had acute episodes of muscular-skeletal pathologies in the last 3 months, of a magnitude that required abstention from work due to illness, which were considered confusing for the study. For each of them, during the health surveillance visit, anthropometric and demographic data were collected (Table 1), elements concerning previous pathologies of the musculo-skeletal apparatus, the presence of possible alterations and deficits of the visual apparatus, the modalities of the onset of possible mild MSDs, occurring in the last 12 months, not requiring abstention from work, affecting the neck, the lumbosacral tract of the spinal column and the upper limbs, were collected by means of a specific questionnaire; an objective examination was also carried out to highlight symptoms or discomfort affecting the anatomical districts covered by our study, through the consultation of an orthopaedist.
The table shows demographic data and other basic characteristics for the population included in our study.

na: number; %: percentage; mean: mean value; SD: standard deviation; Range Min, Med and Max: respectively, minimum, median, and maximum; BMI: body mass index.
The Borg Roating Perceived Exertion (RPE) was used to assess the exertion perceived by individual workers specialised in working at height. This test is capable of assessing the level of physical intensity and perceived exertion of the individual subject based on the physical sensations they experience during physical activity, such as changes in heart rate and respiratory rate, degree of sweating and muscle fatigue. The assessment is based on a linear scale with a score between 0 (no effort) and 20 (maximum effort). The responses obtained from the RPE were divided into four different categories in order to obtain a final score between 0 and 3, the total score was interpreted as follows zero exertion to minimal recognition of effort (0–8) = 0; very to light exertion (9–12) = 1; somewhat hard to Hard (13–16) = 2; very hard to maximal effort (17–20) = 3.8–10
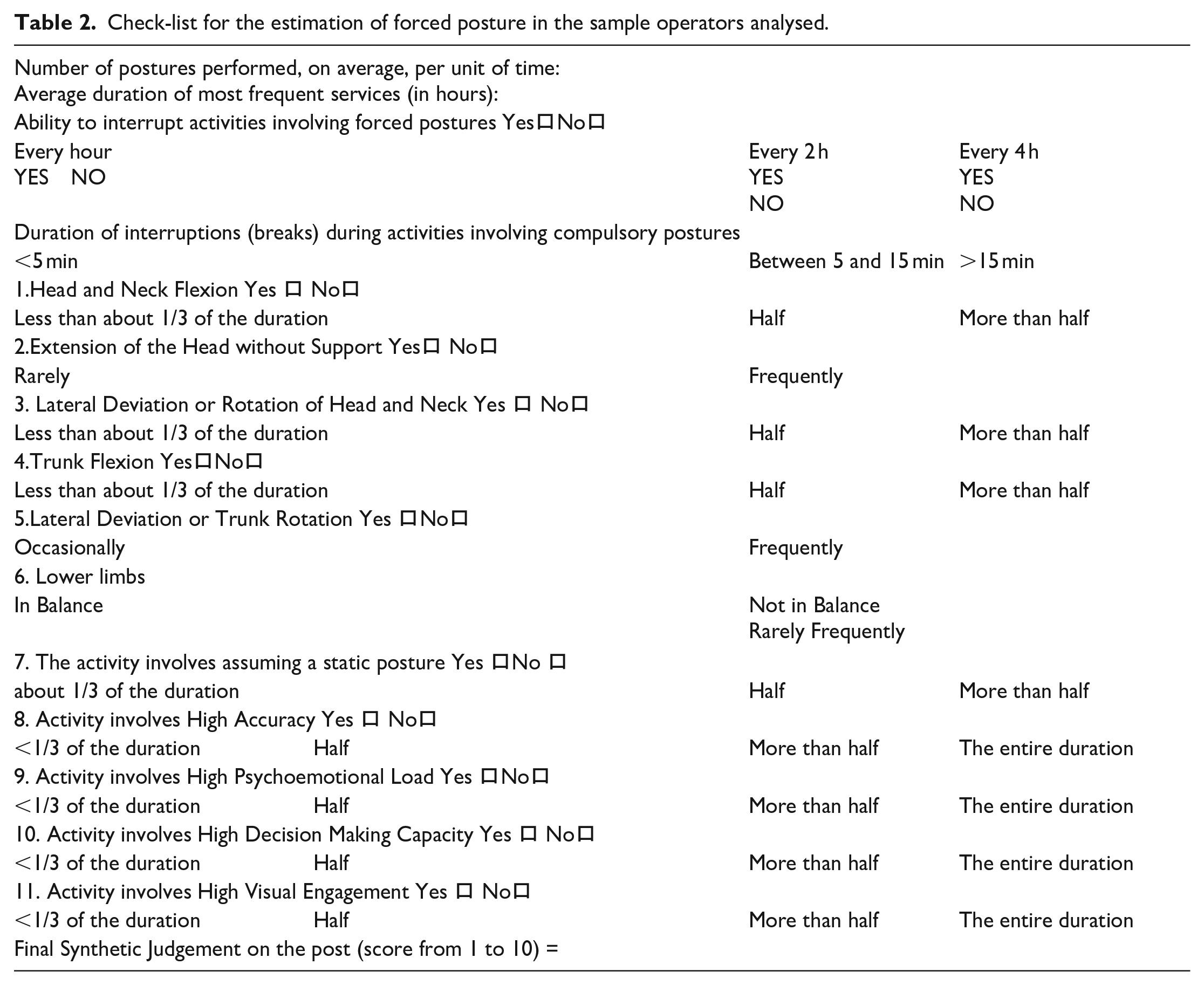
A method based on direct observation carried out by means of on-site visits and interviews with personnel was used to survey the ergonomic characteristics of the environments and the way in which work tasks are carried out. The on-site inspections were carried out over a period of 3 months, between March 2022 and July 2022, using a summary report on the way the activity was carried out, provided by the company, and a specifically prepared check-list (Table 2) which, by integrating the elements taken from different evaluation criteria available in the literature, describes the risk factors in a standardised manner. The selected variables are represented by the way in which the work activity is carried out 11 ; by the duration of the tasks that require either a forced postural commitment on the head and neck, back, limbs, or the need to assume and maintain a prolonged static posture 12 ; by the frequency and duration of interruptions of activities during which forced postures are assumed. 13 Lastly, the responses to items concerning the requirements of precision, psycho-emotional load, decision-making ability and visual commitment required during the performance of manoeuvres were taken into account; at the end of the data collection, a synthetic subjective judgement was made by assigning each homogeneous group a score from 1 to 10 (from worst to best).
Check-list for the estimation of forced posture in the sample operators analysed.
Finally, the index of manual handling of loads in these activities was assessed using the NIOSH method. 14
Statistical analysis
The analysis of the data obtained was conducted using the GraphPadPrism 8.01 statistical software package (GrapPad Company, San Diego, CA, USA). Initially, the collected data were analysed to understand whether they were normally distributed or not in order to choose the most suitable statistical analysis to apply. To do this, we applied the D’Agostino Pearson omnibus normality. Given that our data did not follow a normal distribution, we used the non-parametric Chi-square test in order to determine whether the frequency values obtained with the survey were significantly different from the frequencies obtained with the theoretical distribution. Specifically, the Chi-square test was applied to evaluate the data from the RPE analysis.
For the correlation data between the frequency of DMS and the scale of RPE, we performed a Pearson’s correlation coefficient test. Simple linear regression analyses were generated as predictive models to assign the correlation found.
Results
The average score of the check-list used to evaluate the way the activity was performed by the two homogeneous groups assessed was 5 (range from 4 to 6). The lowest value was found in the rope construction workers. The assessment of the NIOSH index, aimed at examining the manual lifting of loads, yielded a value of between 0.65 and 0.75, which is equivalent to a low risk of manual handling of loads and for which no specific preventive action is required.
Evaluation of perceived exertion
The analysis of the data obtained from the REP revealed that there are differences in the perception of the level of physical intensity and perceived exertion between the groups of workers in our research (Table 3). In detail, the statistical analysis conducted by means of the Chi-square test showed that there is a higher number of subjects with no MSDs who have no perception of intensity and physical exertion than those with MSDs (χ2 = 17.56, z = 4.190 p < 0.0001), which is in line with what was obtained with regard to the perception of slightly harder (χ2 = 14.34, z = 3.787 p < 0.0002) or very hard (χ2 = 6.415, z = 2.533 p < 0.0113) work by workers with MSDs compared to those without MSDs (Table 4).
Zero exertion to minimal recognition of effort (6–8) = 0; very to light exertion (9–12) = 1; somewhat hard to Hard (13–16) = 2; very hard to maximal effort (17–20) = 3.

The table shows the percentages of subjects without and with musculoskeletal disorders and, among the latter, the most frequent.

NMD: No Musculoskeletal disorders; MD: Musculoskeletal disorders; MDCST: Musculoskeletal disorders of the cervical spine tract; MULD: Musculoskeletal upper limb disorders; MDDLS: Musculoskeletal disorders of the dorso-lumbar spine.
Evaluation of correlations between MSDs and RPE
In order to understand whether there was a correlation between the various MSDs analysed in the study, and the values obtained from the RPE, a statistical analysis was conducted using Pearson’s correlation coefficients between the RPE scores obtained from those who stated they had different MSDs and the RPE score of the total sample. The statistical analysis revealed a significant association between the frequency of MSDs analysed and the score obtained on the RPE scale: MDCST (r = 0.4015, CI 0.08401–0.6449, p = 0.0152); MULD (r = 0.4598, CI 0.02115–0.745, p = 0.0416); MDDLS (r = 0.6071, CI 0.05098–0.8759, p < 0.0363) (Figure 1).

Correlation between the frequency of MSDs analysed and score obtained on the RPE scale. Musculoskeletal disorders; MDCST: Musculoskeletal disorders of the cervical spine tract; MLLD: Musculoskeletal lower limb disorders; MDDLS: Musculoskeletal disorders of the dorso-lumbar spine.
Discussion
The most surprising result that emerges from this study is the high MSD prevalence index equal to 59.65% of the population interviewed. These MSDs involve, to varying degrees, the cervical spine (52.94%), the upper limbs (29.41%), and the dorso-lumbar spine (17.65%). These values are different from those classically found in those exposed to the risk of conventional manual handling of loads, where, although there has been a significant mechanisation of production processes, it is still the main factor correlated with the onset of musculoskeletal pathologies mainly of the dorso-lumbar tract. 15 Let us recall how the intervertebral disc, consisting of a gelatinous nucleus covered by a fibrous ring, is capable of withstanding even considerable loads, deforming following the mechanical stimulus and recovering its original size and shape with the cessation of the same 16 ; if, however, this structure is subjected to an excessive load, exceeding its tolerance limits, it undergoes those degenerative processes that in the first analysis are the cause of the painful symptoms.
Among the numerous causes that could have contributed to the high prevalence level reached in our study of MSDs are: a more thorough anamnestic collection, and above all, greater attention in the objective examination; carried out by the orthopaedic specialist, and aimed at the anatomical districts, of the cervical spine and upper limb, which are generally neglected in comparison to the dorso-lumbosacral area of the spine. 17
The analysis of the results of the check-list for the estimation of the compulsory posture in rope or confined space operators, of the anamnesis collected, and of the objective examination, made it possible to highlight that there is a greater occurrence of cervical spine disorders in those subjects who carry out their work mainly maintaining an incongruous position with their gaze and upper limbs elevated upwards, with few rest breaks, in which they can alternate more ergonomically correct positions.
With respect to the listed elements, which may have partially contributed to the high final value of the prevalence index, the data obtained nevertheless appears capable of demonstrating the existence of a causal link between MSDs and objectively dysergonomic working conditions requiring corrective action. The variables that proved capable of predicting the occurrence of MSDs, especially in the cervical district and upper limbs, were: a positive remote history of MSDs and the Rating of Perceived Exertion (RPE). As far as the first variable is concerned, a positive history of MSDs would indicate how a previous clinical history involving the anatomical features studied may contribute to favouring, especially in the most severe clinical cases, the possibility of new recurrences. In fact, a significant proportion of cases with a positive pathological history of musculoskeletal disorders reported having been affected in the past by protrusions and/or herniated discs, affecting the L4-L5 or L5-S1 tracts of the spine. The strong correlation between MSDs and the Rating of Perceived Exertion (RPE) scale agrees, in turn, with the results obtained by other authors18,19 and may reflect the difficulty that some practitioners have in devising effective coping strategies when the symptoms have already occurred and the workload is perceived as very high. This impression seems to be confirmed by the high percentage of answers to the questionnaire which, in almost 50% of the cases, attribute the prevalent cause of the onset of the disorders to a work environment with sub-optimal organisational and ergonomic characteristics.
Although this study provides an overview of how working at height may lead to a higher incidence of MSDs in the cervical spine and upper extremities, it has several limitations. Although the number of subjects recruited in our study is sufficient to assess the correlation between musculoskeletal disorders and incongruous postures in a group of workers specialised in working at height, we believe it is inadequate to draw definitive conclusions; in this regard, we are collecting additional data to enlarge our sample. Another limiting aspect of the study relates to not having taken into consideration the workers’ age and length of service in the sector under investigation, and not having investigated other psychosocial factors capable of influencing the onset of MSDs. Specifically, with the exception of the Rating of Perceived Exertion (RPE) scale, other psychosocial factors, possibly disturbing, that are considered important risk factors such as relative stress, any other work or sports activities practised, the responsibility of the task performed and the relative mental commitment resulting from it were not investigated.20–23
Conclusions
The topic of the correlation between MSDs and their occupational origin among those employed in activities that do not involve the traditional handling of loads has so far been a little dealt with. The high prevalence of disorders of the cervical spine, scapulo-humeral girdle and upper limbs indicates the need to consider as a predominant risk, in the work activities considered in our study, the forced position to be assumed for a large part of the work activity, static, and the inability to move the lower limbs for long periods. In addition to all this, for activities that take place on ropes or in cramped spaces, there are the difficulties in using common mechanical systems to reduce the risk related to MMC (forklifts, trolleys, mechanical bridges).
The concept of ‘occupational risk from incongruous postures’, classically considered to be fatiguing for the knee and lower limb joints, must therefore be supplemented for the problems we have highlighted in order to implement appropriate assessment initiatives and to put in place appropriate containment measures.
In light of the patterns of occurrence of MSDs found in the workers surveyed, proposals for improvement focus on planning the assessment of the postures assumed and the risks associated with them, using specific systems, methods and tools to identify the joints and anatomical areas most affected. Future research could therefore focus on the development of primary forms of prevention, such as better design of the work environment, paying greater attention to organisational-managerial aspects and the provision of better ergonomic work devices and equipment. Last but not least, we believe it is essential to increasingly benefit from information and training measures focused on the new types of activities in the sphere of tasks requiring physical effort, which are increasingly affecting the world of work.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.