
Abstract
Background:
Dementia prevalence among Indonesian older people is increasing. Community health centers (CHCs) as primary care providers have a responsibility to meet the need of their community. This study aims to measure the response of CHCs to the growing of dementia cases and to investigate factors associated with the knowledge of CHC staff on dementia symptoms in Special Region of Yogyakarta (DI Yogyakarta), Indonesia.
Design and methods:
This study used a cross-sectional design to obtain census data from 121 CHCs in DI Yogyakarta by interviewing 121 older person program managers of the CHCs via telephone between January and February 2021. Data on knowledge of 10 dementia symptoms, participation in dementia prevention and treatment with dementia, dementia/cognitive screening and coverage as well as factors associated with memory loss and change in mood and behavior were assessed. Data were analyzed using descriptive, bivariate, and multiple logistic regression.
Results:
The knowledge of dementia symptoms among health workers was low (15%–37%). CHCs had not yet received training on dementia prevention and treatment (58%). Only a few of CHCs treated patient with dementia (36%). Dementia screening and coverage were also low. Engaged in dementia training were more likely to have higher knowledge of dementia symptoms, particularly memory loss and changes in mood and behavior.
Conclusions:
Dementia training and education are needed to increase knowledge among care providers which would eventually improve CHC response to dementia. Priority should also be in place to support dementia care management.
Introduction
Dementia is a syndrome of declining memory, thoughts, behavior that interferes with the ability to perform daily activities. Globally, over 50 million people are suffering from dementia in 2020 of which 60% reside in low and middle-income countries and is projected to rise by 71% in 2050. 1 The risk of dementia increase as people age with the older group demonstrating a higher prevalence of dementia.2,3 The prevalence of dementia among people over 60 of age in Central Asia and North Africa/Middle East is 5.75 and 8.67. The number is estimated to increase exponentially from year to year. 4 Other risk factors of dementia include less education, being female, physically inactive, and having a history of stroke. 2 Those who have chronic diseases such as hypertension and diabetes are also more likely to develop dementia. 5
Indonesian older population (more than 26 million) is dominated by females and had lower education than males. 6 The basic health study recorded heart disease, stroke, and diabetes as major degenerative diseases found among older people. 7 These statistics show that both the male and female population is at risk of developing dementia. Meanwhile, dementia is an issue that remains under-prioritized and awareness is still lacking. The Ministry of Health launched the national strategy on dementia in March 2016 which focuses on seven areas including risk reduction and early detection. 8 Even though the Minister of Health delivered the current progress on this national strategy on a webinar with ADI (Alzheimer’s Disease International) in May 2021, the result is not yet apparent. 9
Special Region of Yogyakarta (DI Yogyakarta) is home to the highest proportion of older people in Indonesia, reaching 15.75%. 10 A study reported that the prevalence of dementia among older people in this region is 20.1, higher than in other countries. 11 People with dementia need to receive continuous care due to the complexity and the impact of the disease on the sufferer and caregivers. 12 In many settings, primary health care is where the first contact of the patient with the health system to receive treatment occurred and to decide whether patients should be referred for assessment and treatment by a specialist or not. Primary care in Indonesia is provided by a community health center (CHC) called puskesmas, non-specialist health care services located in each sub-district to serve community members in its catchment areas, which term will be used in the rest of this paper. In the UK, most patients in primary care had their first dementia diagnosis in primary care, and had 60% of those identified will then be referred to a specialist. 13 This shows the prominent role of primary health care as the first gate to provide dementia care for people with dementia.
Even with the advanced dementia care system, the diagnosis coverage in high-income countries is low, around with advanced 50%. 12 Meanwhile in low-middle-income countries, the coverage is even lower, about 5%–10%. 12 The low rates of diagnosis was affected by the low levels of awareness and training of health staff as many of them considered dementia as a part of normal aging. 14 On the other hand, early detection is crucial to recognize that dementia may be present and treatment could be introduced on time. 15 However, the lack of knowledge and awareness of health providers about dementia could hinder the administration of early diagnosis.16,17 In Indonesia, cognitive screening test is mandatory in CHCs as regulated by the Minister of Health Regulation number 67/2015 and number 43/2019. Yet, the screening implementation and coverage remain unknown due limited data on national health reports and research. Furthermore, most studies of dementia in Indonesia have focused on the prevalence and incidence of dementia as well as the associated risk factor.18–20
To prepare adequate health care for the upcoming surge of dementia cases among older person in Indonesia, primary health care need to be evaluated to measure its response to dementia. However, studies pertaining CHC’s response to the increasing number of dementia among older person is unknown. This study aims to evaluate the response of CHC to the growing cases of dementia in DI Yogyakarta by examining cognitive screening implementation, knowledge of dementia symptoms, participation in dementia training, and whether CHCs treated dementia patients to attain information related to community health centers response to dementia. In particular, as knowledge represents the state of awareness about something, we also examine factors associated with knowledge of dementia symptoms of CHC’s staff to ensure timely diagnosis and treatment of older patients.
Design and methods
Design and setting
This study applied a quantitative method to acquire cross-sectional data from all CHCs across five districts/cities in DI Yogyakarta (census). Data collection was conducted between January and February 2021 via telephone due to the COVID-19 pandemic. Most of the contact numbers of participants were retrieved from District Health Office. In cases where the office could not provide the number, the interviewer visited CHC to meet with the head of CHC to seek permission and obtained the contact number of the targeted participants. We tried to minimize as little as human contact to reduce the risk of contracting COVID-19. Interview appointment was made prior to data collection and consent from participants was obtained orally before the interview began. We assigned a data manager to check data quality and completeness. If missing data were found, the data manager would inform the study coordinator to ask the interviewer to revise the data, thus we have zero missing data.
Participants/data sample
Study sample and data sources
Our target is all CHCs in DI Yogyakarta. The initial discussion with five district health offices suggested that the older person program manager was the right person to be interviewed and represented the CHC. During permission process, we met with the head of CHCs and confirmed older person program manager was indeed the right respondent and that the information provided would be accurate for this study. The older person program manager was selected due to the responsibility in managing older person program in the clinic and are knowledgeable about older person situation in their catchment areas. We interviewed a total of 121 participants from each CHC, forming a total of 121 CHCs being interviewed without any missing values (Figure 1).

Flow diagram of participants in this study.
Study items and variables
Data were collected using a CATI (Computer-Assisted Telephone Interview) questionnaire on topics related to training and socialization received, service provision to older patients among others, which were largely adopted from several indicators in the National Action Plan on Older person Health 2020-2024, Minister of Health Regulation 67/2015, and Minister of Health Regulation 4/2019. The first policy includes prevention indicators toward dementia such as screening, training, and knowledge of dementia. Second regulation provides details on provision of polite, respectful services for older people while the last one lists the standards of services given in the CHC which includes types of screening need to be administered for older people.
Questionnaires were piloted before the study was rolled out. Several dementia-related questions which were focusing on care provider’s knowledge of 10 dementia symptoms, training about dementia prevention and treatment, whether the CHCs had and treat patients with dementia and questions about dementia/cognitive screening and coverage were taken to measure CHC’s response to the need for dementia care.
Staff knowledge of dementia symptoms was measured by asking the following question “To your knowledge, is [. . .] a sign of a disease or aging?” If the participant answered the sign of “disease,” they would be asked a follow-up question that is “What part of the disease is [. . .]?” to which they might respond with the name of a disease, dementia/Alzheimer, or don’t know. Ten symptoms being asked were (a) memory loss; (b) problems with concentration; (c) difficulty performing familiar tasks; (d) disorientation; (e) trouble with images or spatial relationships; (f) problems with languages; (g) misplacing things; (h) poor judgment; (i) withdrawal from social activity; and (j) changes in mood and behavior.
Experience in receiving dementia prevention and care training was asked by asking the participant question “Did you or other staff have participated in training about dementia prevention and care?” and the available answers were “Yes” or “No.” To measure CHC’s response to dementia cases, the participant was asked “Does this CHC treat patient with dementia?” to which they can respond with “Yes” or “No.”
Administration of dementia/cognitive screening in CHCs was obtained from two questions that is “Did CHC conduct dementia/cognitive using AMT (Abbreviated Mental Test) in 2019?” and “Did CHC conduct dementia/cognitive using MMSE (Mini-Mental State Examination) in 2019?” with “Yes” and “No” responses. These two assessments referred to the instruments in the Minister of Health Regulation 67/2015. We also asked “How many percent of older persons did [. . .] screening covered?” to measure the coverage of the screening and “Reason why [. . .] percent of screening?” to understand why the screening achievement was as indicated in the previous question.
Statistical analysis
We first used descriptive statistics to summarize the characteristics of the participants of the study and to measure the CHC’s response to dementia care. Second, as we mentioned earlier in this paper that knowledge represents the foundation of awareness about an issue, in this case, represents how well the response is to the need for dementia care, we’d like to further investigate factors affecting care provider’s knowledge of dementia symptoms using bivariate and multiple logistic regression. We selected two symptoms as our dependent variables namely memory loss and changes in mood and behavior to be examined further to see whether independent factors such as sex, age, dementia training, stratification of CHC and cognitive screening were associated with care providers’ knowledge of these symptoms. Stratification of CHC referred to the classification of the community health center when they were assigned as age-friendly community health center consisting of three levels from the bottom to the top that is pratama, madya, and paripurna.
We chose memory loss as it reflects the key symptom of dementia. Meanwhile, changes in mood and behavior represent behavioral disturbances that present in almost all stages of dementia, typically in later stages. 21 All analyses were performed by using STATA 14.
Ethical approval
This study was approved by the Ethics Committee of Medical Faculty of Atma Jaya Catholic University of Indonesia (no. 1447A/III/LPPM.PM.10.05/12/2020).
Results
Participants and community health center’s characteristics
Table 1 shows the characteristics of the participant and the community health centers as well as other descriptive statistics of variables in interest. Of the total 121 participants, the majority were female (93%) and older than 30 years old. We found that more CHCs were without age-friendly programs and with pratama level of the age-friendly health center stratum (52%) than those with higher stratification of age-friendly programs.
Descriptive statistics (N = 121).
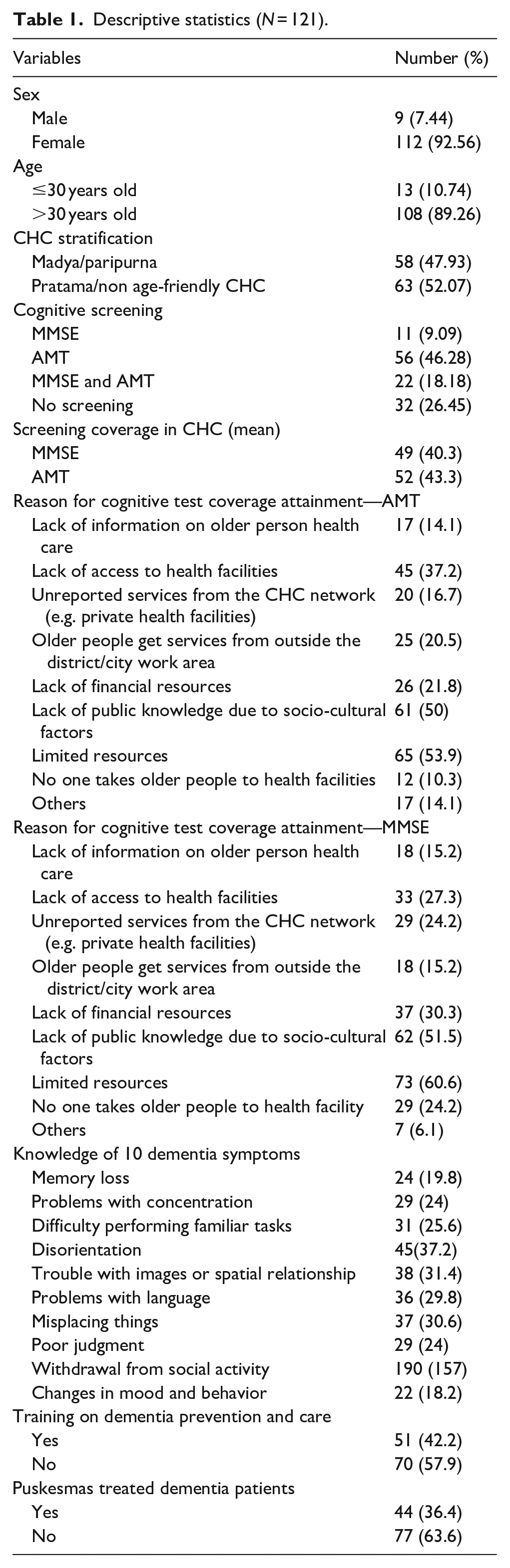
Cognitive screening and coverage
Even though the Minister of Health Regulation number 43/2019 recommends an AMT instrument to assess cognitive status, the Minister of Health Regulation number 67/2015 suggests AMT and MMSE forms are utilized as cognitive measurement tools. Furthermore, in the Older Person Health Book, care providers are allowed to choose one of the instruments. In the present study, CHC in DI Yogyakarta conducted the cognitive screening using AMT or MMSE by 46% and 9% respectively. However, 26% of CHCs did not administer cognitive screening either AMT or MMSE. Of CHCs that have administered the test, the coverage of older people receiving the test was around 40% which implied the screening coverage was low for both tests.
The result suggests not all CHCs conducted cognitive test to screen for dementia even when the screening tools were present. Care providers appeared to use more AMT than MMSE. It is plausible that care providers chose the first tool due to the simplicity of the instrument. AMT consists of 10 simple questions while MMSE has a more complex questions design.22,23 Furthermore, MMSE required a longer time of administration, which might not be suitable in the primary care setting, and caution to interpreting the scores. 24
We examined the reason why the cognitive test coverage results were as such and found that limited resources, the public’s low knowledge, and lack of access to health facilities were three major factors influencing coverage of screening both in AMT (54%, 50%, 37.2% respectively) and MMSE (61%, 51%, and 27%). Our screening questions were asked in the 2019 context so they did not related to the shortage of healthcare workers due to the COVID-19 pandemic.
Knowledge of 10 dementia symptoms
Care providers’ knowledge of 10 dementia symptoms was low. Of the 10 symptoms, “changes in mood and behavior” was marked as the lowest percentage at 16% and the highest was “disorientation” at 37%. Memory loss as a major symptom in early stage of dementia was only acknowledged by 20% of the participants.
Dementia training participation
Our findings showed that 58% of CHCs had not yet obtained training on dementia prevention and treatment. It indicated that many of the care providers have not yet attained adequate information on dementia. This lack of dementia training might be the reason to justify the low knowledge of dementia symptoms among healthcare providers.
Provision of dementia care
We found that only a few of CHCs treated patient with dementia (36%). The number indicated two possibilities. First, the cognitive decline is not considered as a part of the disease. Second, the dementia screening coverage is low which leaves those in the need of care missed.
Factor associated with the knowledge of dementia symptoms
Table 2 shows the result of bivariate data of knowledge of memory loss and changes in mood and behavior. The bivariate analysis showed that the knowledge of memory loss as a dementia symptom was 20%. The result shows that males, aged more than 30 years old, participate in dementia training, had higher CHC stratification of the age-friendly community health center, conducted cognitive screening using AMT, had higher knowledge to answer that memory loss was part of dementia by 22.2%, 27.5%, 20.4%, 22.4%, and 26.8%, respectively. From these five factors, those who received training on dementia acquired the highest percentage, indicating the importance of training among care providers.
Bivariate data of knowledge of memory loss and changes in mood and behavior as one of the dementia symptoms.

On the second symptom which is changes in mood and behavior, we observed similar result to the first one. Those who previously participated in dementia training and CHCs with stratification of madya or paripurna (higher stratification) were associated with a higher understanding that the particular symptom was a sign of dementia than their counterparts (27.4% and 29.3%). As opposed to the first symptom, younger participants demonstrated a higher knowledge to say that change in mood and behavior was part of dementia.
We then run a multiple logistic regression to see the relationship between the two aforementioned symptoms as 1 of the 10 dementia symptoms, with the variable listed in Table 2. We initially included the education of the participant in our regression but we decided to omit it since only 1 out of 121 participants had different education attainment. We discovered that CHCs with higher stratification of age-friendly programs increased the likelihood of knowledge of memory loss as one of the dementia symptoms by 37%. Community health centers that performed cognitive screening using AMT have higher odds of understanding that memory loss was part of dementia signs by 88% than those who did not. Participants who participated in dementia training were significantly more related to acknowledging memory loss as one of the dementia symptoms than those who did not by more than twofolds. Nonetheless, a significant association was found only for memory loss and participation in dementia training (Table 3).
Factors associated with knowledge of memory loss and changes in mood and behavior as one of the dementia symptoms.

Significant at p < 0.05.
On the second regression, CHCs with madya or paripurna stratification had higher odds of identifying changes in mood and behavior as one of the dementia symptoms than CHCs with lower stratification. Participants who said they had engaged in dementia training were more likely to acknowledge the change in mood and behavior as one of dementia symptoms by 3.2 times than those who did not receive training. From both regressions, we highlighted that dementia training was an important factor to improve care providers’ knowledge of dementia, and hence plays a critical role to enhance CHC response to dementia.
Discussion
Lack of knowledge of dementia symptoms suggests that the majority of providers thought dementia symptoms as a normal aging process, one factor that would obstruct the provision of dementia care in primary health care centers. Memory loss as a typical symptom of dementia was not considered as a sign of dementia by most participants. A study by Wilson et al. 25 showed that very mild memory changes are associated with Alzheimer’s disease, a common form of dementia, and thus cannot be taken lightly as part of old age. However, caregivers of people with dementia perceived that memory loss was not an issue that care providers would aware of even when they mentioned their concern. 26
Our finding is similar to the result of other studies16,27,28 which is largely associated with the delayed in early diagnosis of dementia and care.14,29 If these dementia symptoms were failed to be recognized by health providers then dementia may grow progressively, leaving those in need for treatment behind and losing the opportunity to improve older person’s quality of life. This situation indicated a low response of health providers that is the CHC to the need for dementia care since detection and treatment were missed and delayed.
We have argued previously that lack of training on dementia prevention and treatment could relate to insufficient knowledge of the health care providers. The need for dementia training was raised by other studies in dementia diagnosing and care management.16,27 Care providers who have received training on dementia demonstrate a higher knowledge of dementia28,30 and confidence in using screening tools. 31 This evidence marks the necessity of dementia education and training for care providers. Training and dementia education would improve the CHC response to the need for dementia care by making them more sensitive to the presence of dementia cases, particularly among older persons.
Comprehension of the risk factors of dementia would also improve the likelihood of receiving treatment for older people in need. 32 Failure to understand the risk factors of dementia affects care providers to recognize and diagnose dementia accurately. 28 Nevertheless, care providers in primary care tend to interact with the patient briefly while older patients may have multiple conditions. 14 As consequence, the opportunity to identify dementia signs, plan care, and support both older person and their caregivers could be missed because the focus of treatment is established on one condition rather than examining the older patients thoroughly.
Most dementia care in developed countries is provided by specialists 12 yet CHC provide a non-specialist services. In the case where CHCs are not able to provide appropriate care, the referral of older patients to a secondary care can be carried out. A study in the UK found by identifying risk factors of dementia in older people and screening those with associated risk factors help them to get a referral to specialists. 32 It implies that awareness of the risk factors of dementia may determine the certainty of proper treatment and support obtained by older patients which reflects the response of the health center to dementia cases.
Low screening and coverage of screening percentage in CHCs found in this study implied that dementia occurrence among the older population was likely to underestimate. Care providers might not have the experience to administer the screening tool 33 and therefore reducing the chance for the older person to be screened. Confidence in using the screening instrument increases the likelihood of case findings by employing cognitive screening tool more frequently. 34 If care providers were provided with sufficient dementia knowledge and care, including cognitive assessment, they would have greater confidence to perform a cognitive assessment that can improve the number of case findings. Again, it highlights the importance of dementia assessment, dementia care and management training and education in meeting the need for dementia care in primary care like CHC.
Health professionals play an important role in providing care for the community but Indonesia faces a critical shortage of healthcare workers. Despite the increasing number of physicians, nurses, and midwives, Indonesia has the lowest ratio of these health workers to population. 35 On the other hand, cognitive screening for older person are often absent due to a large number of patients which causes restriction of time for examination. 36 In our study, CHC staff who provides care for older person works in other areas as well such as maternal and child health which limit their time to serve older patients. These circumstances point out that workloads among these health workers are high and may reduce the response to the presence of dementia cases among older patients.
Our study revealed that low public knowledge about dementia obstructs the screening test being administered. Family or caregivers of the older person might not aware if they appear to behave oddly or being forgetful as a sign of dementia. Caregivers could also think that the changes are part of normal aging.26,29 Lack of understanding between dementia and normal aging means that many people including older person are missed and unlikely to seek help and miss the opportunity for the symptom treated or to obtain support. Strategy to increase public awareness such as dementia campaign should be available for the caregivers and community members so that they can identify dementia symptoms and support early detection.
Lack of access to health facilities means that older people only get screened when they visit CHC. Meanwhile, most Indonesian opted to visit health facility only when the symptom was persistent. 37 Moreover, older people would only seek help from professionals when they felt the symptom inhibited their activities. 38 This surely would not meet the 100% screening coverage and early detection as many older people will visit health facilities only when they constantly disrupt by the symptom.
To improve screening coverage and improve health centers’ responses to the need for dementia care, CHCs may shift the task of screening and identifying dementia to community health workers (CHWs) known as kader posyandu. CHW is available in most of the communities in Indonesia and has been working significantly to improve the health of community members.39,40 WHO defined task shifting as “a process of delegation whereby tasks are moved, where appropriate, to less specialized health workers.” 41 With proper training and supervision, CHWs were seen as a potential agent in managing non-communicable disease and mental health.39,42–44 Furthermore, task shifting is promising to increase the effectiveness of health care services delivery. 45 Given the availability and prominent role of CHWs in the community, identification of dementia can be employed to increase case finding through screening. However, further research to evaluate the effectiveness of CHWs to screen dementia is needed.
Another important finding of this study is those with higher stratification of the CHC that implemented an age-friendly community health center strategy were more knowledgeable in recognizing dementia symptoms than lower stratification or those without age-friendly programs. Perhaps it is due to certain standards that need to be met by the service providers that make those with higher stratification of CHC with age-friendly community health center strategy more familiar with one of dementia symptoms. Unfortunately, the literature discussing CHCs providing age-friendly programs for the older people in Indonesia is very limited. Primary health care in Indonesia remains to concentrate its provision to serve groups such as maternal and child health and putting older person health deprioritized. 46 Moreover, health programs for the older person in CHCs are not within the list of essential health programs and remain extended programs which means their planning and implementation comes after all essential programs are met. However, one of the objectives of the age-friendly primary health care initiative by the WHO is to improve the response of primary health care to older people which emphasizes the relevance of this initiative to be implemented in community health centers to strengthen service provision for older people. 47
Contextual factors like cultural differences could influence our findings. It is common in our society to perceive that dementia is natural as part of aging because people do not understand what dementia is.48,49 They consider dementia or “pikun” in Indonesian language to be a normal condition. 50 Global report also corroborates this notion where two third of the general public and 62% of health care practitioners believe that dementia is natural and part of normal aging. 51 This is probably why the diagnosis rate is low, even in most high-income countries. 12
Policies to support the management of dementia are in place such as the National Action Plan on Dementia in 2016 and National Action Plan on Older Person Health 2020–2024 launched in 2020 by the Indonesian Ministry of Health but results of its implementation in the ground level of the health system are not yet apparent particularly when our study was carried out. Dementia as a public health priority, recommended as of the seven action areas of the Global dementia action plan, is not yet fully recognized in Indonesian health policy and regulation, which is also an issue in other low and middle-income countries and few high-income countries with great variation among countries. 52
Our findings highlight the need for health system transformation where older people health program need to be prioritized. As we discussed earlier in this section, health programs dedicated to older people are not within the essential health programs administered in the CHC which may have implications for dementia care and management for older people. Strong political commitment and leadership are required to leverage the provision of health care for people with dementia.
The current study has several limitations. First, the study had a relatively small sample even when we employed the census method. We have reached the maximum number of community health centers because we already included all health centers in DI Yogyakarta. Second, the health system in Indonesia follows the decentralization policy which means the projection of results to other contexts is limited. However, data derived from this study are important to portray the situation in CHCs regarding the unmet need of older people with dementia so that the local health office could take action accordingly.
Conclusions
The CHC’s response to the need for dementia care was low despite the growing need for care for older people with dementia. While CHCs were available for older community members with dementia, care providers were lacking in recognizing the symptom of dementia possibly due to the lack of training in dementia prevention and care. Training on dementia knowledge and care management should be in place for healthcare providers to increase dementia detection and treatment and to improve CHCs responsiveness toward the growing number of the older population with dementia as well.
To avoid the situation of Indonesian older people becoming a catastrophe for users and providers, we encourage all stakeholders to increase their attention to older person by checking older person’s cognitive function regularly, taking them to health services or integrated health posts to get cognitive function checked, and to recognize dementia symptoms. Priority on dementia care specifically for older people should also be highlighted as a specific health program with strong commitment from all health stakeholders to reduce the risk of developing dementia, improve early detection, and provide care tailored to the need of older people with dementia.
Footnotes
Acknowledgements
The authors would like to thank all participants for participating and supporting this study.
Author contributions
Conceptualization, NWS; Data curation SI, DO, KWL; Methodology, NWS; Project administration, DA; Supervision NWS, DA, BS; Data analysis and interpretation RU, DO; Writing original draft, DO; Writing review & editing, DO, NWS, BS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Knowledge Sector Initiative from Department of Foreign Affairs and Trade (DFAT) [grant number 1301001-G-2018-004].
Previous presentation
Part of this paper was presented at the 16th IRSA International Conference on 12 July 2021.
Significance for public health
The older people population in Indonesia increases gradually over time and care should be prepared to meet the need of the older population including those with dementia. Dementia cases are emerging among older people yet this critical issue remains overlooked. This study highlights the areas that need for improvement in community health centers as a response to the growing cases of dementia. The result of this study would be valuable for health policymakers and other health stakeholders to act accordingly.