
Abstract
Background:
Self-medication is a global phenomenon and a potential contributor to negative health consequences on human health including emergence of antibiotic drug resistance globally.
Objective:
The primary objective of this study was to estimate the prevalence and determinants of self-medication in Thimphu, Bhutan and Chattogram, Bangladesh, two neighbouring South Asian country.
Methodology:
A community-based cross-sectional study was conducted in the city of Thimphu, Bhutan and Chattogram, Bangladesh. A pre-tested and semi-structured questionnaire was used to collect information on socio-demographic characteristics, health status and self-medication practices in the previous year.
Results:
Out of the 998 recruited participants, 61.8% (170/275) from Thimphu and 41.5% (300/723) from Chattogram reported self-medication practices in last year of interview. In Thimphu, eye/ear infection (90.9%), fever (84.9%), headache (80.5%) and cough and cold (78.2%) were the major illnesses reported for self-medication, whereas in Chattogram people mostly self-medicated for skin disorder (74.4%), diarrhoeal illness (59.1%) and eye/ear infection (48.1%). Knowledge on side-effects of the drugs taken for self-medication was comparatively higher in Thimphu than in Chattogram. Both in Thimphu and Chattogram, higher odds of self-medication were found for common illnesses with adjusted OR 7.8; 95% CI 3.3–18.4 and adjusted OR 2.0; 95% CI 1.4–2.8, respectively in Thimphu and Chattogram.
Conclusion:
Self-medication was found to be substantially high in both the cities, however, rate of self-medication was higher in Thimphu compared to Chattogram. Knowledge and awareness raising about harmful effect of self-medication and effective regulation over selling of prescription medication in pharmacies should be strengthened in both countries.
Introduction
Self-medication as part of self-care is a global phenomenon, which is a pressing concern health-care systems in many countries. 1 Self-medication generally refers to the use of non-prescription medicines; usually over-the-counter (OTC) drugs to treat minor ailments without a medical practitioner’s consultation or with no medical supervision.2–4 In many countries, people self-medicate antibiotics and other prescription medicines when there is less regulation over selling antibiotics without a prescription. The prevalence of self-medication in developing countries ranges from 12.7% to 95%, whereas the prevalence in western countries has been reported as low as 3%.5,6 The prevalence of self- medication has been increasing for all kinds of drugs, especially in the developing countries. 5
Easy accessibility, low awareness about side effects, poor regulation and guidelines over usage of prescription and non-prescription drugs facilitates self-medication. 7 In many cases people obtain information about self-medication from friends, and family, and most importantly from internet without having much knowledge about side effects and other negative consequences of the drugs they take for self-medication. 8 Antibiotic resistance has become a serious public health concern worldwide due to irrational use of antibiotics, including self-medication and incomplete dosage, hence the evaluation of self-medication at the population level is needed. 9
Self-medication is a worldwide problem for many developing countries like Sudan, Trinidad and Tobago, Brazil, including south Asian countries such as Pakistan, India, Nepal, Afghanistan.10–16 In Bangladesh, self-medication practice is very common and about 16% - 81% of self-prescription and 26.7% of self-medication with antibiotics were reported by previous studies among urban population.17–19 However, these studies were conducted mainly among university students in certain part of the country. There is a clear data gap on the prevalence and determinants of self-medication in Bangladesh, especially from Chattogram. Chattogram is the second largest city in Bangladesh located in the south-eastern part of the country near Myanmar. It has the largest seaport is located offering the main route for almost all of country’s import and export. In South-east Asia, Bhutan has the highest levels of government health spending; however, self-medication in Bhutan has been reported to be common like in other south Asian countries but only limited information available on prevalence and determinants of self-medication from Bhutan.20,21
The government, medical professionals, pharmacists, chemists and numerous non-governmental organisations will be benefited from evidence on self-medication generated in this study in order to close the information gap and help them take the necessary steps to address the situation. This study aimed to determine the prevalence rates of self-medication and to explore the factors associated to self-medication among general population in Thimphu and Chattogram, two major cities of Bhutan and Bangladesh. Information obtained from this study will potentially guide the interventions and policies to address compounding self-medication issues the region and raise awareness at a community level.
Methodology
Study design and sampling
A cross-sectional study was carried out in Bhutan, Thimphu and Chattogram, Bangladesh. Both male and female of aged 18 years and above were included in the study. The study was conducted in selected hospital out-patient departments and pharmacies, where the study subjects who came to buy medicine or seeking health care were recruited using consecutive sampling methods following the study inclusion criteria. In Thimphu, private pharmacies in the city centre were purposively selected, whereas in Chittagong, both public and private hospitals, and private pharmacies were selected for recruitment of subjects. Written informed consent was received from all participating study subjects. The study was approved by the Ethical Review Committee of Asian University for Women in Chattogram, Bangladesh.
Data collection
In-person face-to-face interviews were conducted between late May and early December 2019 using a semi-structured questionnaire. The questionnaire had separate sections to collect information on demographic characteristics, practice self-medication, the reason of medication, commonly used drug and knowledge about drug resistance. The questionnaire was developed and reviewed by the study investigators including an epidemiologist, a public health expert, a pharmacist and a physician.
The questionnaire was developed in English before being translated back into Bengali and Dzongkha. Before the collection of data, we assigned two research assistants who were fluent in the local dialect and provided them with extensive training.
Sample size
For study in Thimphu, sample size was calculated considering 50% prevalence of self-medication, 6% margin of error and 95% confidence level giving 267 study subjects to include. In Chattogram, the sample size was calculated at 385 people, based on a 49.9% prevalence rate of self-medication, a 5% margin of error and a 95% confidence level. 22 Finally, 275 participants from Thimphu and 723 participants from Chattogram were included in this study.
Data analysis
All the collected data were coded and entered directly in SPSS data entry platform after checking for consistency, and missing values. Descriptive analyses were done as frequencies and percentages for demographic characteristics and other key variables. Chi-squared test was performed of the key categorial variables to determine any association with self-medication. Both bivariate and multivariate logistic regression analyses were done to determine the factors associate self-medication. Self-medication for any drug in last year of interview was used as a dependent variable, while the explanatory variables included sociodemographic factors, type of sickness and knowledge of medicine side effect. A 95% confidence interval and p-value ≤0.05 was used in assessing the statistical significance of association.
Results
Socio-demographic characteristic
In total, 275 participants were recruited in Bhutan, of them 41.8% male and 58.2% female and 723 participants were recruited in Bangladesh, of them, 68.5% male and 31.5% female. Mean age of the participants in Chattogram (34.1 ± 12.1) were higher than Thimphu (28.7 ± 12.6). In Thimphu, about 31.6% of the respondents were employed, 80.7% had an educational level of Primary or more. On the other hand, 50.9% of the subjects in Bangladesh were employed but only 5.1% of them were uneducated (Table 1).
Socio-demographic of the participants.

Practice of self-medication
The prevalence of self-medications was 20% higher in Thimphu (61.8%) than in Chattogram (41.5%) (Figure 1(a)). In Chattogram, 44.3% of the females and 40.2% males used self-medication, while in Thimphu, it was 65.0% 57.4%, respectively (Figure 1(b)). In both the cities, self-medication was more common among people aged 18 to 25 years (Figure 1(c)). Although self-medication practice in Thimphu less by 33.3% among people over 45 years, there was no major change by age in Chattogram (Figure 1(c)).

Prevalence of self-prescribed medicine in Thimphu and Chattogram: (a) self- medication practices in Thimphu and Chattogram, (b) self-medication by gender, (c) self-medication practice by age groups.
Purpose of self-medication practices
Among the reported diseases, gastric problems were three times more common among participants in Chattogram than in Thimphu (Figure 2(a)). Bhutanese participants mostly used self-medication for eye/ear infection (90.9%), fever (84.9%), headache (80.5%); gastric problems (79.2%), cough and cold (78.2%); and diarrhoea (78.0%), (Table 2). The tendency to self-medicate was significantly higher in Thimphu than in Chattogram for Headache, fever, diarrhoea and gastric problems.

Pattern of disease prevalence and self-prescribed medicine in Thimphu and Chattogram: (a) Frequency of diseases and symptoms in last 1 year and (b) types of drugs mostly used in Thimphu and Chattogram.
Self-medication practices among the participants.

N/A: not available; NS: non-significant.
Antihistamines were the most widely used drugs among participants in Chattogram, while the most widely used drug in Thimphu was antipyretic (Figure 2(b)). Nearly, 55.5% participants in Chattogram take antihistamines on their own, only 4.7% of people in Thimphu use such drugs. On the other hand, the rate of antipyretic drug use was nearly double that of Thimphu (54.2%) compared to Chattogram city (27.8%) (Figure 2(b)). Antipyretics (71.8%), Antibiotics (68.3%), NSAIDs (72.5%), Multivitamins (80.0%), these are the most common self-medications among the people of Thimphu (Table 2). Self-medication of antibiotics was higher among the people of Chattogram, than in Thimphu (Table 2).
Information and sources of drugs for self-medication
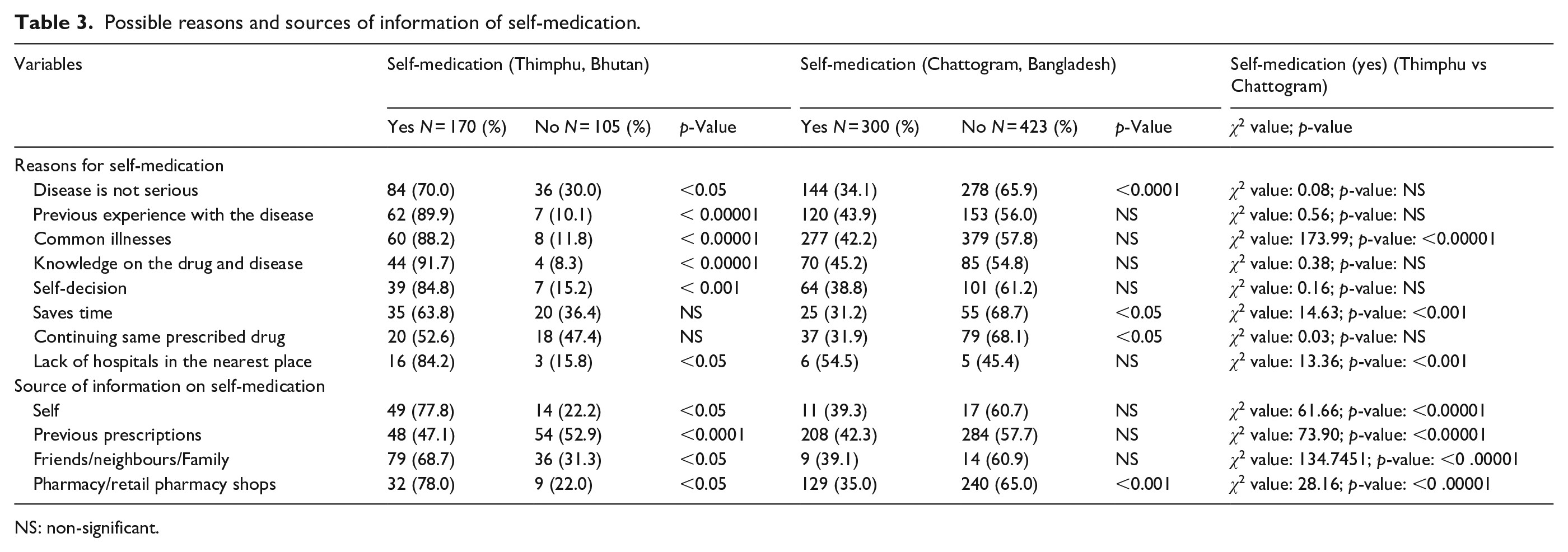
Common reasons for self-medication included lack of perceived seriousness of disease, previous similar practices, no hospitals in nearest places and suffering from general illnesses were noted in both the cities (Figure 3(a); Table 3).
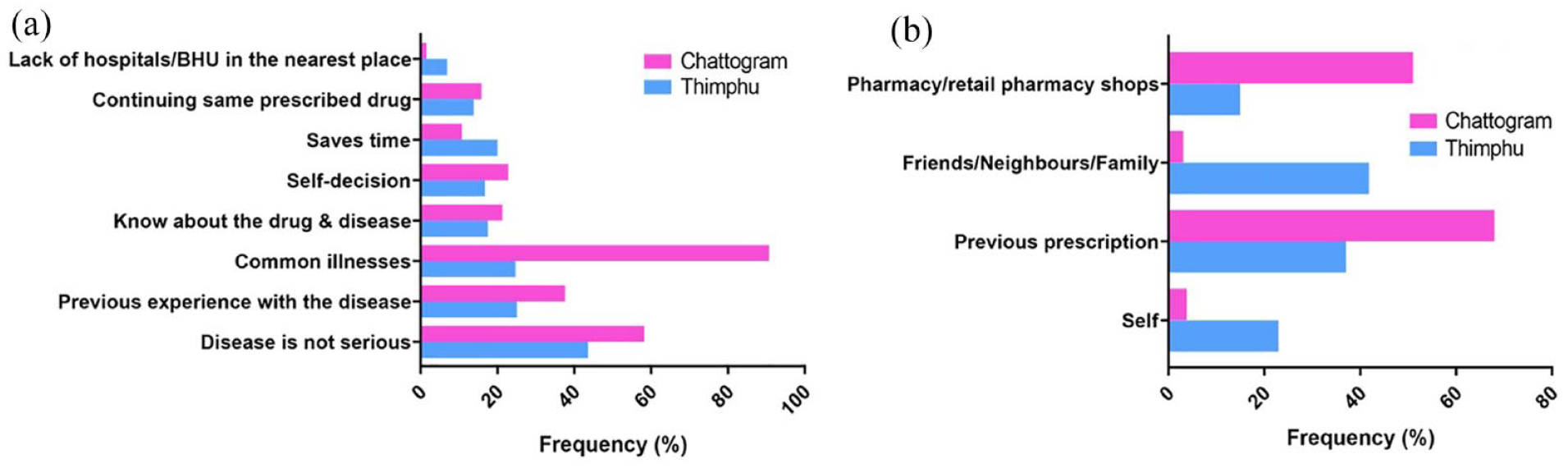
(a) Major factors behind self-medication in Thimphu and Chattogram, (b) Source of information on self-medication.
Possible reasons and sources of information of self-medication.
NS: non-significant.
The majority of the participants in Thimphu considered family, friends and neighbours (41.8%) as their primary sources of information on self-medicated drugs however, people of Chattogram received information from old prescriptions of doctors (68.0%) and local pharmacies (51.0%) (Figure 3(b); Table 3).
Knowledge on self-medication practice
In comparison to Chattogram, Thimphu had a higher tendency to use leftover medicines from previous uses (Table 4). The tendency to complete the full course of the drug used for self-medication basis was also higher in Bhutan than in Chattogram. Knowledge of drug resistance, and other side effects were significantly higher among participants in Bhutan and then in Chattogram (Table 4). Those who self-medicated in Thimphu are more aware of the side effects of the drug (Table 4).
Self-medication related knowledge.

NS: non-significant.
Factors affecting self-medication factors in Thimphu and Chattogram
Younger age was found to be a significant determinant of self-medication among participants of Thimphu in bivariate model, but this finding was not significant when adjusted for other variables (Table 5). Students were more likely to do self-medication compared to other occupation, however, this finding was only significant in bi-variate analysis among participants in Chattogram, Bangladesh. Having a general illness was a significant predictor of self-medication in both Thimphu (adjusted OR = 7.8, 95% CI: 3.3–18.4) and Chattogram (Adjusted OR = 2.0, 95% CI: 1.4–2.8). However, in Chattogram, previous knowledge about antibiotic was significant predictor of self-medication practices (Adjusted OR = 1.5, 95% CI: 1.1–2.2).
Logistic regression determining the factors affecting self-medication in Thimphu and Chattogram.
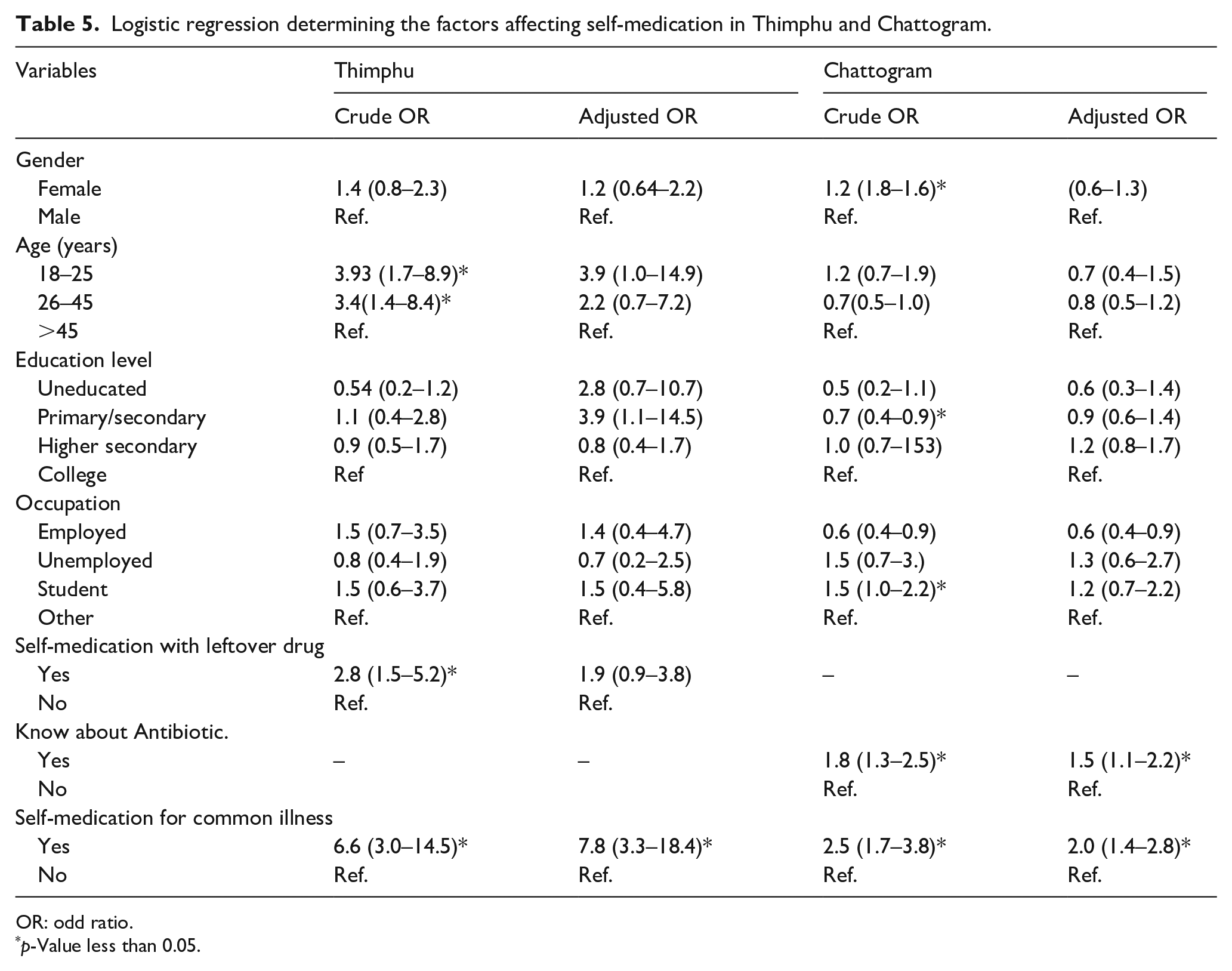
OR: odd ratio.
p-Value less than 0.05.
Discussion
Self-medication is quite common in many parts of the world; however, it varies substantially across the countries.8,23–25 Substantially high prevalence of self-medication was found in this study, especially in Thimphu, Bhutan, which is similar to several other cities in South Asia, such as Islamabad, Pakistan (61.2%), Pokhara valley, Nepal (59.0%).25,26 Some other cities in South Asia, such as Delhi, Karachi had a high rates of self-medication as well.14,27 This variation may be due to differences in educational background, socioeconomic status and accessibility, affordability and quality of the health care systems.
Eye infection and fever were most reported diseases and respiratory diseases, and skin diseases were the two least reported illnesses to use self-medication in Bhutan. In Chattogram, self-medication was mostly reported for skin diseases and diarrhoea. The level of gastric problem in Chattogram city was almost three times higher than in Thimphu city. Being a coastal city, dry fish is a very common food for most of the Chattogram people. 28 In addition, the popularity of various types of junk food has also increased in Chattogram in recent days. Overeating of Junk food or dry fish can be a reason for high gastric problem. Although, infection from Heliobacter Pylori was reported very high in Bhutan only a small fraction of them suffered from gastric complications. 29 Less dependency on processed food and healthy lifestyle could be a reason for less gastric complications in Thimphu, despite high prevalence of Heliobacter Pylori infection. Antipyretics (such as Panadol and Paracetamol), drugs for cough/runny nose and pain killers (Paracetamol, Panadine, Aspirin and Brufen) were the mostly used medication that denoted a usage by more than half of the studied population of Thimphu, although in Chattogram it was relatively low. Among the self-medicated drugs used in Chattogram city, Antihistamine type drugs used most. In recent years, air pollution in Chattogram city has reached an intolerable level which could be a reason behind high dust allergy and use of antihistamine. Increased air pollution has induced enhanced sales of over-the-counter antihistamines in Gothenburg and Malmö city of Sweden. 30 Eating habits and environmental differences might explain the difference between the disease prevalence and the medication practices in these two cities.
Aligned to our findings, other studies have reported that self-medications were common for ailment of general minor diseases like cough and cold, headache, gastric problems and fever.31,32 Likewise, top three common reasons for self-medication in Chattogram and Thimphu reported in this study were- lack of seriousness of disease, common illness and previous experience with the diseases, which is compatible with many other studies.19,31 The participants of Thimphu mentioned the most common source of information for self-medication as family and friends followed by previous prescriptions; this is comparable with previously conducted studies.33–35 On the contrary in Chattogram, previous prescriptions and local pharmacies were the most common source of information as found in many other studies.8,33,36,37 With the implementation of the Medicines Act of the Kingdom of Bhutan 2003, only licenced pharmacists are qualified to open a new pharmacy, which is likely to result in a shortage of professionals for community pharmacies and could explain why people in Thimphu rely less on their neighbourhood pharmacy. 38
The knowledge of self-medication was better in Thimphu, meaning participants thought that it was not good to self-medicate. 39 However, among those who are aware of the side effects of the drug, the tendency to self-medicate in Chattogram was significantly lower than in Thimphu. It was acknowledged by multiple participants of our study sample belonging to Chattogram that the use of prescription medicine without consulting a physician is clinically inadvisable; as well as using previously prescribed medications to treat recurring symptoms. The study participants of Chattogram city, who are aware of completing the course of antibiotics, do not usually take the medicine on their own. These findings of this study create evidence for the policy makers and intervention programme targeting awareness raising on self-medication targeting pharmacists, general public and also pharmacy students.
Limitations
The study used a cross-sectional survey design, the information reported may suffer from recall bias; however, self-medication usage by the respondents was to the best knowledge and believes of the respondents. Non-probability sampling used for recruitment of study subjects in both the cities may limit the study findings to be generalizable outside the study population. Sample sizes used in two cities were dissimilar because sample sizes were calculated separately using locally available estimates. Thus, the study findings may not be fairly comparable and generalizable between two countries without considering contextual factors including disease prevalence, level of knowledge and other socio-demographic factors.
Conclusion
Self-medication of both antibiotic and non-antibiotic medicines was common in both Thimphu and Chattogram. The study findings will be useful for the government, medical professionals, pharmacists and other stakeholders to undertake further policies and interventions address the situation. At a national level, monitoring of selling prescription medications without a prescription in pharmacies should be strengthened. Community based intervention programmes should be strengthened to raise awareness on side-effects and consequences of self-medication among general population. Further studies should be conducted using more rigorous methodologies to generate further evidence on especially antibiotic self-medication and in both Chattogram and Thimphu to inform health professionals and policymakers for better practices and policies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.