
Abstract
Background:
Alzheimer’s disease/dementia (AD) prevalence is of concern globally and in Canada owing to the rapidly aging population and increase in life expectancy. This study explored: (1) trends in the overall prevalence of self-reported AD/dementia by sex, age groups, educational levels, and geographic areas in Canada from 1994 to 2014, and (2) assessed what the observed trends mean in the context of the aging Canadian population and the health care system.
Design and methods:
This cross-sectional study used Canadian national survey data. Data for this study were from two Canadian national health surveys (National Population Health Survey and the Canadian Community Health Survey), between 1994 and 2014. After age-sex standardization, trends in the prevalence of self-reported Alzheimer’s disease/dementia were tracked over time. The two cross-sectional surveys used similar diagnostic criteria over the years.
Results:
The overall prevalence of Alzheimer’s disease/dementia increased from 0.14 in 1994 to 0.80 in 2014 representing a 0.66-point increase over the 20 years. Alzheimer’s disease/dementia prevalence increased with age across all years but was more pronounced after age 80. Men 65+ years, those with lower education, and Canadians living in Central Canada had an increased prevalence.
Conclusions:
The overall prevalence of Alzheimer’s disease/dementia in the community increased over time. This study highlights the importance of establishing effective community-based prevention strategies that focus on minimizing risk and optimizing protection as well as health system capacity strengthening and preparation for long-term care including increased demand for neurologists’ services, increased associated disability, psychosocial difficulties, rising costs, and caregiver burden.
Introduction
Alzheimer’s disease/dementia (AD) is one of the most common types of dementia and neurological conditions. In 2017, 40 to 50 million people were living with and impacted by AD/dementia and related dementias globally. 1 By 2050, the global prevalence of dementia including AD/dementia is expected to quadruple and 1 in 85 people is projected to be living with the disease. 2 In Canada, 614,000 people were living with dementia in 2018 with an estimated 25,000 people diagnosed each year. The number of people with dementia in Canada has been projected to almost double to 937,000 by 2031.3,4 The economic burden on the Canadian health system is tremendous. In 2011, the total economic burden of care for dementia was approximately $33 billion. This cost is projected to increase to $293 billion by 2040. 4 The number of older persons with dementia living in the community is expected to steadily rise, exacerbated by a projected shortage of long-term care beds. 5
The risk of developing dementia appears to be modified by a combination of demographic, lifestyle, and medical factors. Diseases such as hypertension and diabetes contribute to cardiovascular and cerebrovascular diseases. 2 Individuals with obesity and cardiovascular and cerebrovascular diseases are at higher risk for dementia and AD/dementia. 6 Obesity has been linked with changes in the structure of the brain, resulting in cognitive decline, dementia, and AD/dementia. 7
Notwithstanding these risks, dementia is expected to decrease because there has been a significant decline in the incidence of stroke in recent decades. In Canada, improved treatments of heart disease, hypertension, and stroke have resulted in decreased mortality from these diseases. 8 One study identified an increasing prevalence but a decreasing incidence of AD/dementia in Saskatchewan. 9 There is also evidence to suggest that the prevalence of dementia and AD/dementia is decreasing in younger cohorts and that these trends are likely to occur across developed countries.10,11 On the other hand, there may be more individuals, especially in the older population with an increased risk of dementia due to advances in medical interventions that contribute to an improvement in survival after stroke, or increased prevalence of underlying vascular disease despite not presenting with stroke or its effects. 2
Formal education and more wealth have been identified as protective against the risk of dementia. 12 Many years of formal education are associated with a reduced risk of dementia including AD/dementia. Over time, there has been an increase in the level of education among older adults impacting brain development and function and better health behaviors. The general health advantages of having more education and social opportunities may have influenced the prevalence of AD/dementia. 12
A diagnosis of Alzheimer’s disease/dementia means cognitive impairment, dependency, caregiver burden, and premature death. 13 Despite the depth of the impact of AD/dementia on individuals and caregivers, Canadian studies focusing specifically on the trends of AD/dementia are lacking. Studies on the epidemiology of dementia generally provide estimates of overall dementia and are not specific to causes such as AD/dementia.14,15 Also, some studies have shown that AD/dementia is declining in the younger age cohorts and ballooning in the oldest old age categories, with prevalence projections focusing on those in the highest age categories, otherwise called the oldest old. This may lead to appropriating health care interventions to only a select group of people to the neglect of others who also may need to be targeted. Updated information on the trends of dementia specifically due to AD/dementia is needed in Canada if we are to ensure that adequate and appropriate resources are mobilized to deal with the needs of those with this condition and their families who are most times severely impacted. Such studies can also inform prevention strategies and approaches to management.
The objectives of this study are to: (1) describe the trends in the overall prevalence of self-reported AD/dementia among men and women in different age groups, educational levels, and geographic areas in Canada from 1994 to 2014, and (2) assess what the observed trends mean in the context of the aging Canadian population and the health care system.
Methods
Study sample and data sources
Our study used merged data from two sets of Statistics Canada’s national health surveys over 20 years from 1994 to 2014, namely Canadian National Population Health Surveys (n = 17,276) and Canadian Community Health Surveys (n = 65,000). 16 The Canadian Community Health Survey (CCHS) replaced the National Population Health Survey (NPHS) and has been taking place on a continuing basis since 2000. 17 Both the NPHS and CCHS allow for proxy responses (information provided on behalf of others). These types of responses represented less than 10% of the total responses for all years of the surveys utilized in this study. We examined data from the 10 provinces and the three territories of Canada: Newfoundland and the Labrador (NL), New Brunswick (NB), Nova Scotia (NS), Prince Edwards Islands (PEI), Quebec (QC), Ontario (ON), Manitoba (MB), Saskatchewan (SK), Alberta (AB), British Colombia (BC) and Nunavut (NU), Yukon (YT), and North West Territories (NT).
All these surveys were conducted among respondents aged 12+ but excluded those who were living in long-term custodial facilities, full-time members of the Canadian Armed Forces, living on First Nation reserves, or civilian residents on military bases. This study analyzed data from both the publicly accessible Statistics Canada’s Public Use Micro Data Files (PUMF) and the Master Files.
Survey items
In all surveys between 1994 and 2014, the questionnaires were similar and covered content areas of lifestyle, reported health, healthcare utilization, emotional health, household characteristics, and demographic characteristics. The question of Alzheimer’s disease/dementia in the two data sets was: “Do you have Alzheimer’s disease/other dementia diagnosed by a health professional?” Respondents aged 45 years and over with Alzheimer’s disease/dementia were included in this analysis. In some instances, variable categories for provinces and territories, and educational levels were collapsed to preserve the confidentiality of data. Alzheimer’s disease/dementia prevalence estimates were generated from 1994 to 2014. A survey weighting factor based on age groups, sex, marital status, educational levels, and provincial differences is supplied by Statistics Canada. Population estimates were calculated using the weighting variable.16,17 A written informed consent was granted by participants during the primary data collection process by Statistics Canada. Therefore, it was not required for this study as it involved analysis of anonymized secondary survey data that contained no personal identifiers.
Study variables
AD/dementia prevalence was analyzed by age (45–64, 65–79, and 80+), and sex (male vs female) to account for differences in age and sex. We categorized respondents according to their highest level of education such as “less than secondary,” “secondary graduation,” “some post-secondary,” and post-secondary graduation”. We further categorized respondents into the four regions of Canada based on their province of residence. To allow ease of comparison across all 20 years, as well as graphical presentation, and maintenance of confidentiality of individual data, the provinces and territories were categorized into four regions: Eastern Canada (NL, NB, NS, PEI); Western Canada (MB, SK, AB, and BC); Central Canada (QC and ON) and Territories (NU, YT, and NT).
Statistical analyses
The analyses of this study involved estimating frequencies and prevalence of AD/dementia by sex, age group, region of residence, and educational level for each study population from 1994 to 2014. Data analysis of the CCHS Master Files was conducted under the confidentiality restrictions of the SKY-RDC at the University of Saskatchewan. Population frequencies were estimated using the Statistics Canada survey-specific sampling weights. This was followed using direct standardization to estimate prevalence to account for changes in the demographic structure of the population and population-weighted estimates over time. Standardization was performed based on the population size and age and sex distributions in 2001 to facilitate a comparison of frequencies over time. 18 We treated AD/dementia values recorded as, “not stated,” “don’t know,” “not applicable,” and “refusal” as missing values and excluded them from subsequent analyses.
AD/dementia prevalence was generated to reflect the age–sex groupings for each year included in the study. Stratified analyses were performed according to age groups, sex, region of residence, and educational level to identify trends in Alzheimer’s/dementia prevalence over time. Study results are presented in both tabular and graphic forms. All analysis was conducted using STATA 14.
Results
Trends in overall Alzheimer’s disease/dementia prevalence in Canada
The overall prevalence of Alzheimer’s disease/dementia increased from 1994 to 2014. There was a steady increase in prevalence from 1994 to 2001, with a significant rise in prevalence in 2003, followed by a decline in 2005 and 2010 and again in 2014 (Figure 1). Over the period 1994–2014, the highest prevalence rates were recorded from 2011 to 2013 with the highest standardized prevalence (1.06%) reported in 2013 (Table 1 and Figure 1). In 2014, Alzheimer’s/dementia prevalence at the endpoint (0.80%) remained the same as it was at the midpoint in 2007 (Table 1). Table 1 indicates that the prevalence of Alzheimer’s/dementia increased between the periods 1994 and 2013, from 0.14% to 1.06%. This represented an increase of 0.92% points.
Adjusted prevalence of Alzheimer’s disease/dementia from 1994 to 2014.

Midpoint.

The overall prevalence of Alzheimer’s disease/dementia in the Canadian health survey population stratified by age, over the period 1994–2014.
According to Figure 1, the Alzheimer’s/dementia prevalence dipped below expected estimates from 1996 to 2008 and surpassed the expected estimates between 1999 and 2001. The period 2001 and 2012 saw an expected incline in overall AD/dementia prevalence (Figure 1). Though there was a plateau in overall AD/dementia prevalence between 1998 and 2001, the overall prevalence of AD/dementia among Canadians 45–64 years of age was at an all-time high, with the steady increase in trend for that period reflected in the 65–79 and 80+ age categories. Males accounted for the highest increase in overall AD/dementia prevalence between 1994 and 2014 (Figure 1 and Table 2).
Trends in the prevalence of Alzheimer’s disease/dementia diagnosed by a physician in Canadian health surveys over the period 1994–2014.

Total prevalence for men and women, women, and men, standardized according to the age distribution in 2001.
Percentage point.
Sex differences in the prevalence of Alzheimer’s disease/dementia
Figure 2 demonstrates that for the period 1994–2001, Alzheimer’s disease/dementia prevalence was higher in females than in males, followed by a lower AD/dementia prevalence in females than males in 2003, 2007, 2009–2011, and 2014. Female AD/dementia prevalence surpassed male AD/dementia prevalence in 2005, 2008, and 2013. We observed that for the entire period, 1994–2014, males experienced a higher increase in AD/dementia prevalence than females, though in later years (2012 and 2013) the increase is much greater for females than for males. For both sexes, AD/dementia prevalence was slightly less than expected between 1996 and 1998 and higher than expected for males between 1998 and 2001. The female prevalence of AD/dementia was slightly lower than expected between 2012 and 2014 (Figure 2).

The prevalence of Alzheimer’s disease/dementia in Canada, by sex over the period 1994–2014.
Age differences in the prevalence of Alzheimer’s disease/dementia
According to Figure 3, AD/dementia prevalence is highest among men and women in the 80+ age category followed by the 65–79 age category, and lowest in the 45–64 age category. Increases in AD/dementia prevalence were most evident among men and women in the 80+ age category when compared to the younger age categories, 45–64 and 65–79. While there is a noticeable increase in AD/dementia prevalence among men and women in the 80+ age category for the period, 1994–2014, the increases in prevalence in AD/dementia prevalence are slightly lower for men and women in the 45–64 and 65–79 age categories (Figure 3).
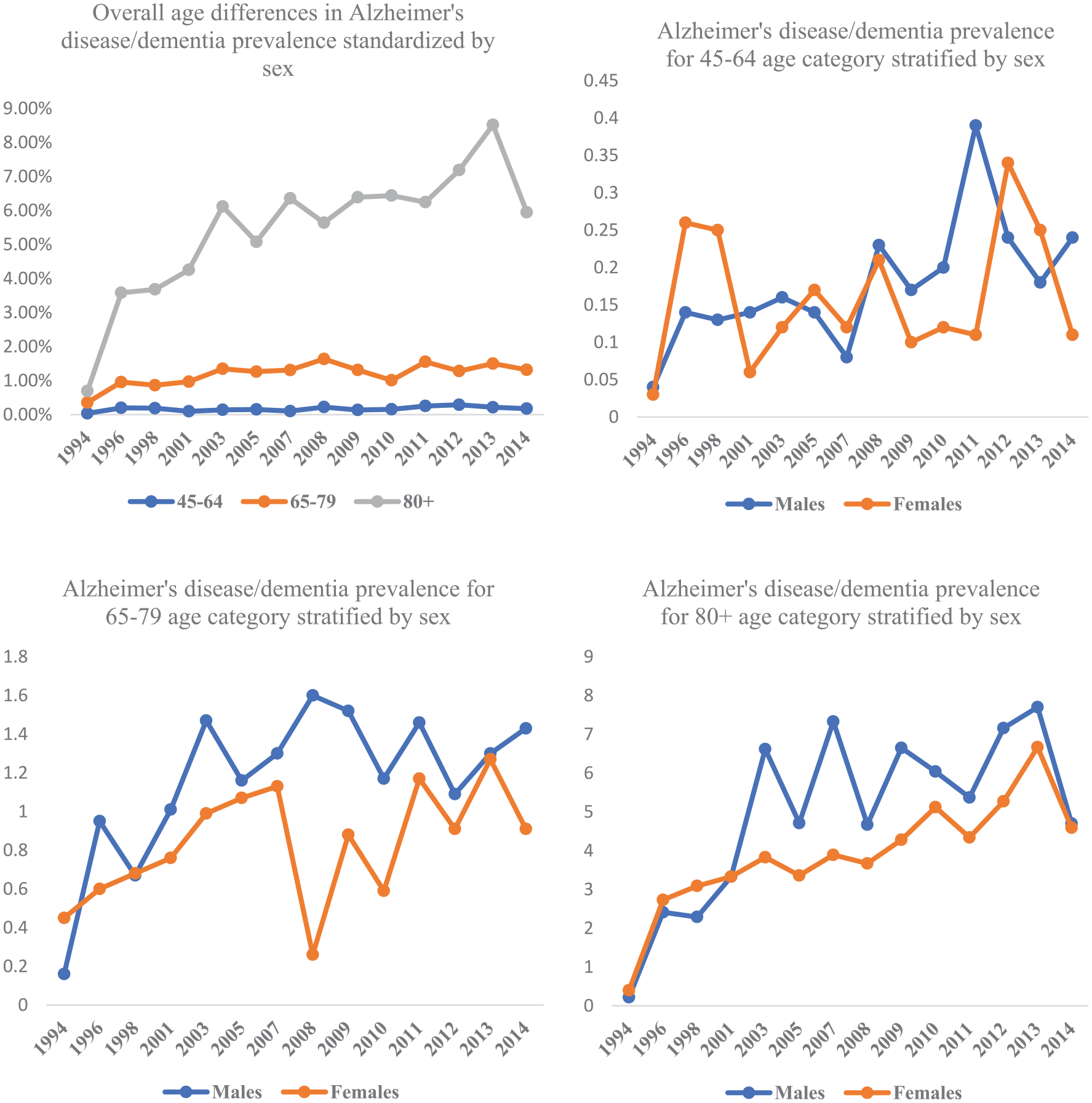
The prevalence of Alzheimer’s disease/dementia among age groups stratified by sex in Canada, 1994–2014.
The highest prevalence for each of the sexes was recorded in 2013 and the 80+ age category. Additionally, in the 65–79 age category, there was a marked increase in AD/dementia prevalence in males (1.27%) compared to females (0.46%), with increases in prevalence from 1994 to 2014 being higher in males among all age categories (Table 2). As shown in Figure 3, there was a decline in AD/dementia prevalence in 2005 which was attributable to the decline of AD/dementia in all age categories of men in that year. While there was a marked decline in AD/dementia prevalence among women in the 65–79 age category in 2008, there was a converse incline in AD/dementia prevalence among females in the 45–64 age category with a small decrease in the prevalence of AD/dementia among women in the 80+ age category for that same year. There does not appear to be a significant difference in the prevalence of AD/dementia between males and females in the 45 and 64 age category, except during the period between 2008 and 2012 when the prevalence of AD/dementia in men was higher than that of women.
Geographic differences in the prevalence of Alzheimer’s disease/dementia
We did not observe a significant geographic difference in the prevalence of AD/dementia. Figure 4 shows that AD/dementia prevalence across all 10 provinces and territories increased over time and the derived estimates are a good predictor of the expected prevalence of AD/dementia. On average, there was a 0.44% increase in prevalence across the country over the period 1994–2014 with no change in prevalence for the territories over time, and Eastern, Central, and Western Canada reported significant above-average increases in the prevalence of 0.45%, 0.71%, and 0.60% respectively over time. After 1994, the lowest recorded prevalence among the regions of residence in Canada was recorded as 0.46% in Central Canada.
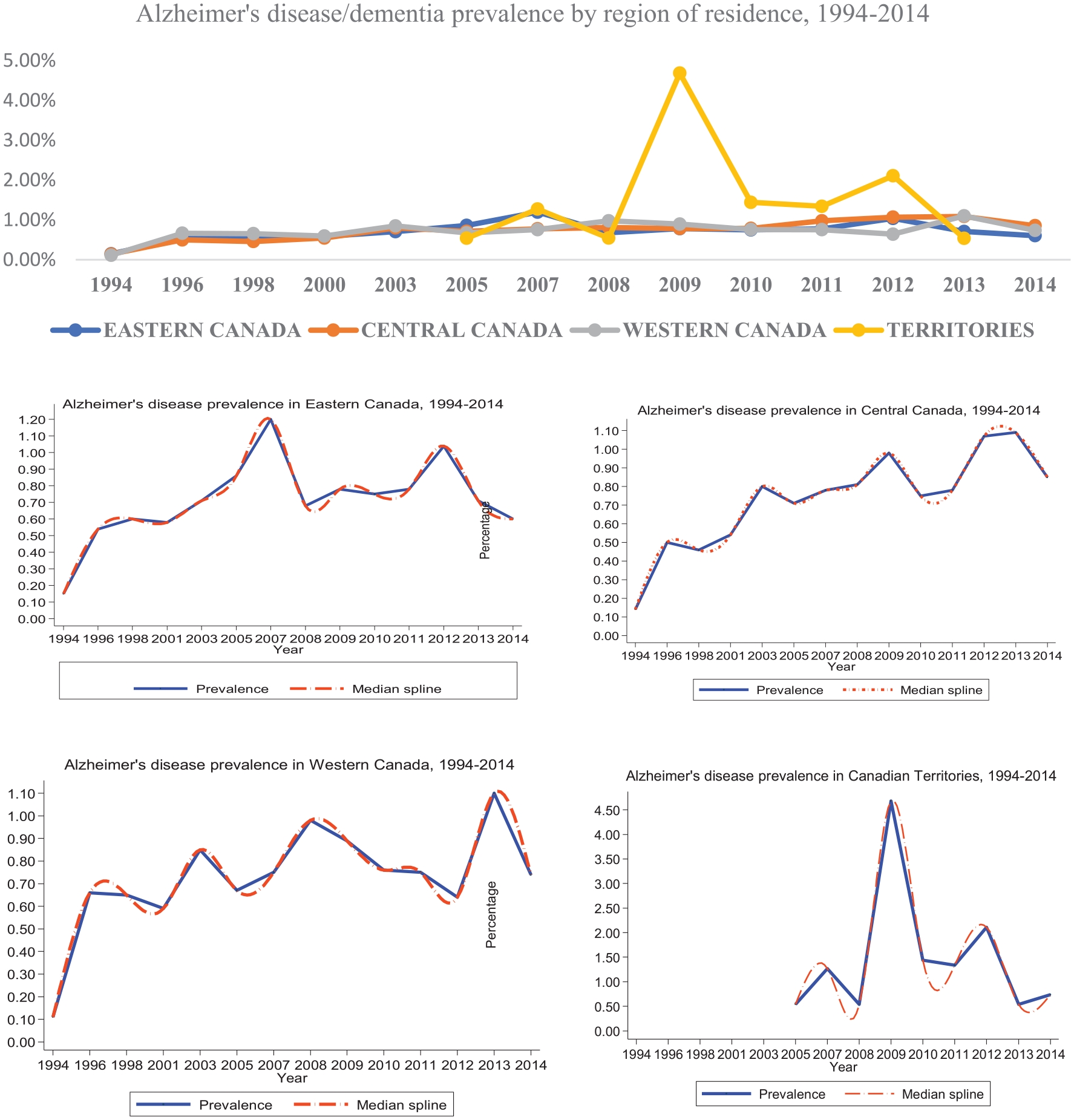
The prevalence of Alzheimer’s disease/dementia according to region of residence in Canada, 1994–2014.
There was a sharp increase in prevalence from 0.15% in Eastern Canada to 0.86% in 2005 and 1.20% in 2007 followed by a sharp decrease to 0.68% in 2008 and a leveled increase from that point to 2012 when there was a marked increase (1.04%) in AD/dementia prevalence, followed by a decline resulting in a prevalence of 0.60% in 2014. This reflected a 0.45% increase in AD/dementia prevalence in Eastern Canada from 1994 to 2014.
Central Canada recorded a 0.71% increase in prevalence over time, from 0.14% in 1994 to 0.85% in 2014, reflecting the highest increase in prevalence among the regions of residence in Canada. Central Canada also recorded the steadiest increases in prevalence between 2005 and 2013, reflecting marked inclines in 2008 and 2011 and a sharp decline in 2014.
Western Canada reflected the second-highest overall increase in prevalence from 0.11% in 1994 to 0.74% in 2014, accounting for a 0.60% overall increase in prevalence for that region. The highest prevalence recorded in Western Canada was 1.10% in 2013. There were other sharp inclines in 1996, 2003, and 2008. Apart from 1994, the lowest prevalence recorded in Western Canada was 0.59% in 2001.
The trend in AD/dementia prevalence observed in the territories is similar in undulation to that observed in Eastern Canada. The territories had the highest prevalence of AD/dementia since the number of people living in that region of Canada is small compared to that of other provinces and regions in Canada. Figure 4 demonstrates that though there was a marked increase from 0.54% in 2005 to 4.68% in 2009, this was followed by a steady decline to 0.54% in 2013 resulting in no real change in the overall prevalence of AD/dementia in the territories over the period for which data was available.
Educational differences in the prevalence of Alzheimer’s disease/dementia
We observed educational differences in AD/dementia prevalence over time. The average all-time increase in prevalence by education was 0.74%. Figure 5 shows that the highest number of prevalence estimates >1.00% was recorded in those with the lowest level of education, that is, those who had less than secondary education. Those in the category of less than secondary education also recorded an above-average increase in the prevalence of 1.22% over the period 1994–2014. Though the overall increase in prevalence was higher in those who had completed secondary education (0.70%) than in those with some post-secondary education (0.52%), yearly prevalence increases were higher among those who had some post-secondary education in 1994, 1996, 2001, 2008, 2009, 2010, and 2012.

The prevalence of Alzheimer’s disease/dementia according to level of education in Canada, 1994–2014.
There was little difference between the overall increase in prevalence between those who graduated post-secondary and those who had some post-secondary education. Additionally, those who reported post-secondary graduation reported a steadier increase in prevalence compared to those who reported some post-secondary education, who had more significant shifts in prevalence increases over time, suggesting a more protective relationship between the completion of higher levels of education and AD/dementia than mere exposure to higher education.
Discussion
There are not many studies that have examined national trends in AD/dementia prevalence in Canada over time. Other studies focused on a single province, a subgroup in the population, or all dementias, or predicted overall change in prevalence from a single point in time to some future time decades later.3,9,19 –21 While these studies examined the prevalence, they did not look at annual trends over time or by strata within the population. More studies focusing on trends in AD/dementia and dementia prevalence were also conducted internationally.2,22 –26 It is difficult to compare the results of such studies due to the variation of dementias included, characteristics of the study populations including strata, age, and sex standardization, and differences in the period or country studied.27,28
Notwithstanding, previous studies reported similar findings to our study. In general, our findings that the prevalence of AD dementia showed substantial variation between 1994 and 2014, but no secular trend is in keeping with recent results. 26 We found that the prevalence of AD/dementia recorded an overall 0.66-point increase between 1994 and 2014, and a 5.12-point increase in individuals 65+ years of age, in that same period. One study which also focused on age and sex standardized prevalence estimates for AD/dementia using Ontario data found that the prevalence over time increased by 18.2% in individuals 66+ years of age. 19 This finding corroborated what was found in a Japanese study of the prevalence of AD/dementia. 25 The increase in the prevalence of AD/dementia over time may be attributable to the continued increase in the size of the older population, growing awareness of the disease 2 , and earlier diagnosis of cognitive deficits. 29 Our study showed small increases in prevalence year over year, but bigger increases over time, signifying smaller increases in the incidence of AD/dementia, and declining mortality, resulting in more people living longer with the disease. 30 Improved mortality among those at risk for AD/dementia may be caused by improved survival rates for strokes and cardiovascular diseases, largely due to more public health promotion activities targeted to nutrition and other lifestyle factors, leading to earlier identification and treatment of lifestyle-related diseases (e.g. diabetes and hypertension), greater control of serum lipid levels, and decreases in cigarette smoking.2,31
We observed that the prevalence of AD/dementia increased with age in both men and women across all years but increased significantly after age 80. This is consistent with the findings from previous studies,25,27,32,33 which is in keeping with the expectation that, over time, there will be a greater number of the elderly living in the community and with AD/dementia.5,29 While the increase in the prevalence of AD/dementia was consistent with age in both males and females, our study found that over time, there was a greater increase in prevalence among men than women. This finding is contradictory to some studies which report that AD/dementia prevalence is greater among women than men.25,34–36 On the other hand, the more recent Canadian study with a similar methodology 19 supported our finding that although prevalence rates were highest among women, the increase in the rate over time was greater among men. This higher prevalence in men may be an artifact of survey methodology which excluded those living in institutions.16,17 Women are more likely to live in long-term care facilities after a confirmation of AD/dementia as opposed to men who spend more time living in their communities after AD/dementia diagnosis. 37 On the other hand, neurodegeneration, and the development of clinical symptoms significantly contributing to mortality are more severe and progress faster in women than in men,38 –41 resulting in fewer women with AD/dementia living in the community.
We did not observe a significant geographic difference in the prevalence of AD/dementia throughout the years. However, there was variation in the level of AD/dementia prevalence increase across all provinces, over time. Few trend studies highlighting geographic differences have been published in Canada. It is therefore difficult to make adequate comparisons. Some researchers suggest that, if regional variations in Alzheimer’s disease/dementia exist, they exist for reasons other than lack of standardization of rates or differences in diagnostic protocols across the country. 42 Lack of significant geographic variations in AD/dementia prevalence year over a year may be because of population homogeneity in the risks and duration of AD/dementia across the country as well as similarities in preventive approaches and cultural factors influencing the etiology and expected course of AD/dementia. On the other hand, the variations in geographic prevalence increases of AD/dementia in this study over time might be explained by differences in genetic, environmental risk, and protective factors that may exist across provinces. Similar results have been reported earlier regarding other chronic diseases.43 –45
Our study found that prevalence increases were less among those who had attained higher levels of education and increased in those with lower levels of education. This is consistent with data in the literature that indicates that low educational assessment is a risk factor for AD/dementia while high educational attainment is protective.12,46 One of the rare analyses of Alzheimer’s disease/dementia trends by education, found similar trends in AD/dementia, indicating that those with less than secondary education had greater increases in AD/dementia than secondary graduates who in turn had greater increases in AD/dementia than post-secondary graduates. 47 Our study found a slightly higher prevalence of AD/dementia among those who completed post-secondary education compared to those with some post-secondary education. This finding could be explained by the protective association between higher education levels and longer life expectancy found in another study. 48 In that study, the researchers explained that individuals with higher education tend to live longer in general and with AD/dementia; which is consistent with the slightly higher prevalence of AD/dementia observed in those with post-secondary graduation compared to those with some post-secondary exposure. Those with higher levels of education and wealth are more likely to intentionally seek information and improve health behaviors, leading to a reduction in risk factors for AD/dementia related to lifestyle factors such as cigarette smoking, nutrition, and physical activity.47,49 On the other hand, those in the older age categories may have lower levels of education associated with cognitive decline attendant with AD/dementia, 50 accounting for higher increases in the prevalence of AD/dementia among the 80+ year groups in our study. This higher prevalence of AD/dementia among individuals 80+ indicates that as persons live longer with AD/dementia, there may be an increased need for long-term care whether in the community or in facilities when the disease progresses beyond the ability of caregivers (mostly spouses of similar age) to provide the relevant care required by AD/dementia patients.
Strengths of this study include a consistent definition of AD/dementia cases across years, the use of nationally representative surveys of the Canadian population over 20 years with relatively high participation rates. Another strength is that our study supports the findings of similar studies in other jurisdictions. This study impacts the dearth of trend studies on Canadian data by updating information on AD/dementia prevalence within several strata of the Canadian population and is a good source of information for the development of targeted public health and community-based approaches to AD/dementia.
A major limitation of our study is that the surveys used did not include respondents living in institutions including health care facilities and nursing homes. Besides, data were lacking for the territories for most years. This study may have resulted in an over or under estimation of AD/dementia prevalence, due to underdiagnoses of AD/dementia in the community and variation in participants in the surveys over the years as well as the fact that those diagnosed with AD/dementia are more likely to be living in institutions.
Conclusion
The prevalence of AD/dementia has increased steadily over the past 20 years in the general population of middle-aged and older Canadians. The increasing trend seemed to be observed across all strata of the population (age, sex, education, and region of residence) and mostly among men aged 65 or older, those with lower levels of educational attainment, and those living in Central Canada, despite a lack of consistent pattern. Future projections of the prevalence of AD/dementia in the Canadian population should include data on individuals living in institutions. The focus should also be given to the cultural and behavioral drivers of the etiology of the disease, reflective of the diversity of the Canadian population.
Given, the high life expectancy and projected growth of the elderly population, our study underlines the importance of establishing effective community-based prevention strategies for AD/dementia. It also underscores the need for health system capacity strengthening and preparation for increasing challenges associated with long-term care of AD/dementia including rising costs, caregiver burden, and increased demand for neurologists’ services. Additionally, public health prevention strategies that focus on minimizing risk and optimizing protection are needed to mitigate against the steady increases in the prevalence of AD/dementia in the community.
Footnotes
Acknowledgements
TC-R is grateful to the School of Public Health, University of Saskatchewan for its financial assistance throughout her studies. The authors thank the Saskatchewan Research Data Centre for granting us access to their confidential data.
Author contributions
TCR, BC, CD conceptualized the study. TCR conducted the formal analysis, visualizations, interpreted the results, and undertook the writing of the original draft. TCR, BC, CD provided ideas and thoughts for discussion. BC and CD revised the manuscript for important intellectual content and supported TCR in writing—reviewing and editing. The content and views expressed in this article are those of the authors and do not necessarily reflect those of Statistics Canada.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was not required for this study since it was a secondary analysis of a series of national health surveys already conducted by Statistics Canada. Written informed consent was obtained from all respondents, as well as ethics review approval for the original study before it started. The Canadian Community Health Surveys and the Canadian National Population Health Surveys were conducted by Statistics Canada.
Significance for public health
Alzheimer’s disease/dementia (AD) prevalence is of concern globally and in Canada owing to the rapidly aging population and increase in life expectancy. Given that the “baby boom” cohort has contributed significantly to Canada’s population aging, accurate estimates of Canadians with Alzheimer’s disease/dementia are crucial in the ongoing evaluation and resulting in continuous quality improvement of healthcare services for this vulnerable population. Such knowledge will contribute to the Canadian health system’s preparation of and strengthening of services to adequately provide for and meet the needs of the constantly increasing aging population. This study highlights the importance of establishing effective community-based prevention strategies that focus on minimizing risk and optimizing protection as well as health system capacity strengthening and preparation for long-term care including increased demand for neurologists’ services, increased associated disability, psychosocial difficulties, rising costs, and caregiver burden.
Data availability statement
The data that support the findings of this study are from both the Public Use Microdata Files (PUMF) and the Master Files of the National Population Health Survey and the Canadian Community Health Surveys. Access to the National Population Health Survey cross-sectional data is available to bona fide researchers through institutions participating in the Statistics Canada Data Liberation Initiative (DLI) including university libraries throughout Canada—see https://www.statcan.gc.ca/eng/dli/dli. Access can also be arranged directly through DLI inquiries: ![]() ).The views expressed in this paper do not represent the views of Statistics Canada.
).The views expressed in this paper do not represent the views of Statistics Canada.