
Abstract
Recent developments in artificial intelligence (AI) and machine learning raise the possibility of screening and early diagnosis for neurodegenerative diseases, using 3D scans of the retina. The eventual value of such screening will depend not only on scientific metrics such as specificity and sensitivity but, critically, also on public attitudes and uptake. Differential screening rates for various screening programmes in England indicate that multiple factors influence uptake. In this narrative literature review, some of these potential factors are explored in relation to predicting uptake of an early screening tool for neurodegenerative diseases using AI. These include: awareness of the disease, perceived risk, social influence, the use of AI, previous screening experience, socioeconomic status, health literacy, uncontrollable mortality risk, and demographic factors. The review finds the strongest and most consistent predictors to be ethnicity, social influence, the use of AI, and previous screening experience. Furthermore, it is likely that factors also interact to predict the uptake of such a tool. However, further experimental work is needed both to validate these predictions and explore interactions between the significant predictors.
Keywords
Introduction
Neurodegenerative diseases are a major and growing cause of disability. For example, the number of people diagnosed with Parkinson’s in the UK is expected to almost double between 2018 and 2065, 1 with an even faster predicted increase in Alzheimer’s. 2 Currently in Parkinson’s for example, most of the dopaminergic neurones and some essential functioning of the brain have already been lost before diagnosis, 3 indicating that earlier diagnosis is crucial in beginning effective treatment. The retina is part of the central nervous system, directly visible from the outside, and can now be imaged non-invasively in near-microscopic detail by optical coherence tomography (OCT), a relatively inexpensive method that is increasingly available to detect eye disease in high-street opticians. Mounting evidence suggests that neurodegenerative diseases are associated with changes in retinal structure long before physical symptoms occur, 4 offering the possibility of early diagnosis via retinal imaging. However, these changes are subtle and barely detectable by humans, requiring considerable training and experience to detect. Advances in artificial intelligence (AI) and machine learning offer a possibility for earlier diagnosis, through training AI algorithms on large datasets to recognise these subtle changes. Therefore, this raises the possibility that people attending a routine eye test could be screened to detect neurodegenerative diseases very early in the disease process.
Alongside the practical question as to how such screening would be implemented is the critical question of whether the public would accept such screening. Since the technology described above offers the potential that such a screening tool may be developed, it is important to explore and understand these issues before it is approved for use. Potentially, if public acceptance is very low, screening might not be appropriate at all. More realistically, an exploration into the factors that influence acceptance may reveal concerns which can be addressed by appropriate action, such as better engagement with particular communities. This literature review will explore the potential influencing factors using existing screening initiatives as a guide.
Predictive factors for AI-enabled screening
It is important to acknowledge that much of what may be said about the likelihood of screening uptake for neurodegenerative diseases depends on the analysis of past screening uptake behaviour. However, as the number of screening programmes in the UK is small and uptake varies vastly, this analysis must be supplemented by analysis of public health studies exploring the predictors of other preventative health behaviours such as vaccination. Thus, in the absence of a validated screening tool to explore predictors through the collection of primary data, the possible predictors of AI-enabled screening for neurodegenerative diseases may only be explored through consideration of a wide range of literature. The possible predictive factors discussed in this review fall into three main groups:
a) Properties of the disease itself and early diagnosis of it (e.g. awareness, perceived benefit of early diagnosis, perceived risk and susceptibility).
b) Properties of the screening procedure (e.g. perceived accuracy, inconvenience, pain, embarrassment and time).
c) Properties of the individual (e.g. their perceived level of vulnerability, perceived control over their own life, trust of health authorities or authority in general, previous medical experiences).
Clearly, several of these could apply and also interact. For example, a negative experience with a particular screening method (a) might mean that method is met with resistance when encountered again (b). In this review, we will assess the available evidence relating to each of these groups in turn, in the context of AI-enabled screening for neurodegenerative disease via OCT imaging. It is important to note that given the interactions aforementioned, the grouping will necessarily be somewhat arbitrary.
The remaining discussion of this review identifies several factors which might influence take-up of screening for neurodegenerative diseases if this became possible in future, based on existing literature of health screening. Namely, these are the influence of participants’ age, sex/gender, perceived mortality risk, source of the diagnosis (AI vs human) and the stated benefits of early diagnosis of, and personal proximity to neurodegenerative disease.
Properties of the disease itself and its early diagnosis
Multiple studies have found that being affected by a particular disease vicariously, through the diagnosis of a family member, predicts uptake of early screening tools. For example, relatives are more likely to attend mammography,5,6 cervical6–8 and colorectal9,10 cancer screening, and lack of family history has been cited as a barrier to attendance. 11 A further relevant finding is that most relatives of those with Parkinson’s would accept genetic testing if offered, 12 despite the relatively low genetic risk. 13 There are several reasons why being affected by a neurodegenerative disease might predict uptake of an early screening tool.
Increased understanding of neurodegenerative diseases and benefits of early diagnosis
One possibility is that relatives are more accepting of early diagnostic methods because they have increased awareness of the illness, which subsequently predicts uptake. Lack of awareness of colorectal cancer 14 in comparison to other, more highly publicised cancers 15 may help to explain the observation that uptake and coverage for cervical and breast cancer in those eligible lies between 70% and 75% in England,16,17 whilst uptake of bowel screening is far lower at 57.7%. 17 However, an alternate suggestion is the relatively high time investment compared to other screening types, as the screening via faecal occult blood test requires submission of three samples. Indeed, implementation of the faecal immunochemical test (FIT) test 7 which requires one sample increases uptake by 8.5%. 6 Nonetheless, uptake still does not reach that of cervical, breast, or diabetic eye screening, retaining the possibility that a lack of awareness is the largest determinant of this decreased uptake.
Indeed, lack of knowledge around why it is important to attend screening and the available treatment options for the disease being screened for has been identified as one of the main barriers to diabetic eye, 18 colorectal, 14 and breast5,19 screening and increased perception of seriousness was one of the main predictors of breast and cervical screening in the US. 6 Additionally, social media campaigns have been demonstrated to significantly increase knowledge, 20 intention 21 and subsequent screening attendance by 12.9%. 22 Other successful knowledge-based interventions include an intervention comparing the discomfort of cervical screening to the potential consequences of not attending screening, which increased attendance by 15%, 23 and an intervention of diabetes education, which significantly increased attendance for diabetic eye screening. 24 However, many campaigns include other elements such as providing social support 20 and information about the procedure, 22 thus it is difficult to tease their effects apart. Also, the success of interventions to increase awareness may be dependent on there being benefits to early diagnosis.25,26 Although lifestyle changes 27 or medication 28 may be effective for some, there is currently no cure or definitive effective treatment for neurodegenerative diseases such as Parkinson’s. Therefore, the perceived benefits of early diagnosis are likely to better predict screening for neurodegenerative diseases than awareness alone.
Perceived risk of neurodegenerative disease
Being related or close to someone with a neurodegenerative disease may increase its salience and therefore perceived risk for the disease; additionally, the former might induce perception of increased genetic risk. However, the evidence on perceived risk as a predictor of screening is inconsistent, as a meta-analysis of 18 longitudinal studies found that perceived susceptibility to an illness showed a minimal overall correlation of −0.06 with preventative health behaviours, and perceived benefit of the behaviour emerged as a much stronger predictor. 29 This may be explicable by the finding that the relationship between perceived risk and cervical screening was mediated by cancer worry. 30 Since high cancer worry is rare even in high risk populations, 31 the relationship is only detectable in large samples. As relatives of those with Alzheimer’s report high worry towards developing the disease,32,33 this may drive a relationship between perceived risk and screening uptake for neurodegenerative diseases.
It is important to note, though, that perceived risk does not necessarily reflect actual risk. Although in relatively older women (age 40–86; 312 women) for osteoporosis, breast cancer and heart disease perceived risk has been shown to decrease with age, actual risk for these diseases increases with age. 34 This decline in perceived risk might explain the greater likelihood of younger women (aged 35–50; 581 women) versus older women (50 and over) to attend recommended mammography screening. 35
Social influence
Social influence, through wider sources such as the media and healthcare providers, is a well-established predictor of screening uptake. Discussion with and encouragement from not only relatives,10,36 but also physicians10,34,37,38 and wider social groups10,36,39 have been shown to strongly predict colorectal, 10 breast34,37,39 and prostate36,38 cancer screening. It is likely that physicians, specifically primary healthcare providers, exert the largest influence on screening attendance; for example, screening for colorectal cancer in England increased by 6% when endorsed by a letter from a local GP and by a further 11% when the letter was signed by the GP. 40 Further, a review and meta-analysis of 69 interventions found a modest but consistent effect of a GP’s signature on invitation letters. 41 The consistent trust in physicians and subsequent influence in patient’s screening decisions has led to the conclusion that their relationship is the most important predictor of screening attendance. 37
Social influence may also represent the mechanism between the relationship between family history and enthusiasm towards screening, since family history is a significant predictor of discussion around screening. 42 However, it is most likely that these factors also act independently, as there is evidence that the effect of discussion with friends, family and healthcare providers on screening interacts with age. Whilst younger women were found to rely on these sources for breast cancer screening, middle aged women were more likely to utilise mass media. 43 Interestingly, an intervention study of African American women found that whilst age, marital status, discussing with friends, and believing early detection led to a cure were all positive predictors of mammography attendance, family history of breast cancer was no longer a significant predictor. 39 However, discussion with friends and family did not mediate the relationship between family history and prostate cancer screening, whilst number of acquaintances with prostate cancer did. 36 As all participants were African American, the influence of number of acquaintances may depend on ethnicity, which will be further discussed as a predictive factor below.
In summary, history of disease and discussions with friends and family are proposed to predict higher uptake of screening for neurodegenerative diseases, due to an increased perceived risk mediated by worry, and social interaction, respectively. Additionally, perceived benefits of screening and endorsement from a local GP are likely to be independent predictors.
Properties of the screening procedure
AI versus human agent
A number of studies have found that a human healthcare provider is generally preferred over AI,44,45 demonstrated across a range of prevention, treatment and diagnosis scenarios. 44 Moreover, this preference is most prominent for decision making within healthcare, including diagnosis. 46 Mainly, AI is only accepted for these purposes providing a physician is present to supervise or for a second check,47,48 indicating that the public do not support the unsupervised use of AI for screening and diagnosis. 47 Studies have found different reasonings for this decreased trust in diagnosis, 49 such as perceptions that AI cares less than a human doctor, 50 a perceived lack of control over AI being used for diagnosis, 49 and perception of lower accuracy. 51 However, even if the accuracy of AI were proven to be as accurate as physicians’, participants still felt more confident in a human doctor over AI. 52 Alternatively, a preference for a human doctor was found to be mediated by the view that AI does not account for the uniqueness of each patient and their health. 44
However, this preference runs deeper than conscious reasoning. A comparison of explicit and implicit attitudes towards AI found that whilst only 6% reported a negative attitude to AI, 77% showed a negative implicit attitude on the implicit associations test (IAT). 53 This test measured sub-conscious biases to find that most participants more readily conflated AI with ‘bad’ rather than ‘good’, compared to humans. Additionally, a study involving fMRI found that whilst participants reported preferring AI when the conversation was personalised rather than generic, the areas of the brain associated with prosociality were only activated when engaging in the same conversation with a human doctor. 54 This selectiveness towards feeling a social and trusting connection indicates an inbuilt preference towards humans as an evolutionary mechanism. 54
While the tendency to distrust AI is general, a number of other factors may interact with it. Evidence for the influence of demographic factors such as age and sex/gender is mixed,52,55 and may be dependent on other factors such as country. 55 Additional predictors of acceptance towards AI include education, 48 direct previous experience with AI,46,53 and personal history 52 and severity 46 of the disease the AI aims to diagnose. It is likely that the use of AI will tend to lower the acceptance of screening for neurodegenerative diseases, although this may change as public awareness of and experience with AI becomes more widespread.
Experience of screening using OCT
Although no AI algorithms for diagnosing neurodegenerative disease from OCT images have yet been approved for use in the UK, OCT is already used to diagnose ophthalmic diseases such as glaucoma,56,57 diabetic retinopathy 58 and age-related macular degeneration.58,59 A relevant finding is, therefore, that whilst there are multiple factors that predict previous screening behaviour, only previous screening behaviour remains a significant predictor of current screening.60,61 Furthermore, a study of 2657 women found that important predictors of initial breast cancer screening such as family history and proximity to someone with breast cancer were no longer significant in predicting attendance for the second and third time. 62
One explanation is that attending screening eliminates any worries or fear around the screening procedure. In support, familiarity with the screening procedure is a firm predictor of mammography screening 5 and campaigns that aim to provide information about the procedure have successfully improved screening attendance. 17 A beneficial feature of OCT imaging is that it is painless, convenient and involves no bodily exposure. Screening for eye health in diabetic patients is similar to the procedure of OCT imaging and shows a much higher uptake than other screening programmes in the UK, at 82.7%. 17 Indeed, beliefs that diabetic eye disease could be seen with an eye examination was a significant, positive predictor of self-reported adherence to screening. Furthermore, pain, convenience and bodily exposure have all been demonstrated to predict screening uptake.63–67 Therefore, previous experience with OCT should eliminate any fears around pain or embarrassment.
Home sampling for cervical and colorectal cancer greatly increases uptake, 41 potentially indicating that factors such as embarrassment were the main barriers. However, having the home sampling kit delivered rather than needing to collect it from a GP increases uptake still further.11,14,41,68 This suggests that in fact it is the convenience of home screening which is the major advantage. Despite this, it remains reasonable to conclude that previous experience of OCT scanning within an optometrist or optician would predict a high uptake of screening tool for neurodegenerative diseases that utilise OCT, due to the consistent predictor of past screening behaviour.
Properties of the individual
Socioeconomic status and uncontrollable mortality risk
One consistent finding in the literature is that those of lower socioeconomic status (SES) are more likely to: suffer from adverse health outcomes such as obesity (in women 69 ), engage less in healthy behaviours and more in harmful health behaviours, 70 and have a lower life expectancy. 71 For example, average life expectancy for men in the UK was found to range from 73 for those in very unskilled manual occupations, compared to over 80 for those in the highest professional roles. 72 For each intermediate occupational class, there is a step decrease in life expectancy, 72 suggesting an underlying gradient 73 rather than a ‘cliff edge’ effect, 74 wherein there is a sudden decrease in life expectancy below a certain SES threshold. More specifically, one review of inequalities due to SES noted that the differences also exist in preventative healthcare and can sometimes be substantial. 75 For example, on the rollout of screening for colon cancer in the UK, there was a 26% difference in uptake between those at the bottom fifth and top fifth SES, 76 despite the existence of free universal healthcare in since 1948. 77 Many studies have found a similar relation between some measure of SES and probability of some protective health behaviour – for example, between women’s occupation and flu vaccination, 78 education and cervical screening, 79 and area SES and both follow-up diagnostic tests 80 and eye tests 81 – although the effect size is rarely as substantial as for colon cancer. 76 Furthermore, this effect is also present across other developed countries in Europe,82,83 and is especially linked to cancer screening.82,83 Considering the most important driver of the relationship between SES and preventative health, education remained an independent predictor of cervical screening even when income, class and occupation were added into the model. 79 Overall, a review of the effect of education concludes that it is at least as strong a predictor as income, and that the two interact. 84
One possible reason for the link between education and screening is that highly educated people have higher health literacy, that is are better able to comprehend health information and thus make informed decisions about their health. 85 Although a review of 10 articles of mostly self-reported cancer screening found relatively inconsistent findings, 86 a longitudinal study with over 3000 participants found a 10% difference in attendance for colorectal cancer screening between those with acceptable versus with limited health literacy, even when controlling for age and gender. 87 Furthermore, in a sample of 2668 adults, health literacy mediated the relationships between education and: flu vaccination, dental check-ups and mammography screening. 88 Although participants were over 65 and all variables were measured cross-sectionally, this does indicate a mechanism for the strong relationship between education and preventative health behaviour including screening.
However, those of lower SES also experience higher exposure to environmental risks such as air pollution,89,90 poor housing quality,89,91 and infections such as COVID-19, 92 a finding that differences in health literacy does not account for. Whilst stress and a lack of resources 73 have been suggested as the link between adverse environment and investment in preventative health, an underlying evolutionary mechanism is posited by the uncontrollable mortality risk hypothesis. 93 The hypothesis states that when an individual is faced with a number of threats to mortality that are out of their control- as is the case in those of low SES- they will invest less in behaviours within their control. This is because if an individual’s environment threatens the longevity of their life, there is little point in investing energy and resources into preventative health behaviours. In a series of experiments, Pepper and Nettle 94 demonstrate that manipulating the perceived controllability of life expectancy significantly predicts whether a fruit or chocolate prize is chosen, irrespective of whether participants were primed with long or short life spans. This indicates the effect is due to the uncontrollable aspect rather than a general mortality threat. Moreover, in an online study of 600 North Americans, Pepper and Nettle 95 found uncontrollable mortality risk to fully mediate the relationship between subjective SES and health investment.
Since the uncontrollable mortality risk hypothesis posits that lack of control results in prioritisation of short-term outcomes over long-term, it makes sense that it would apply to preventative health behaviours including screening. Indeed, actual 96 and perceived 97 mortality risk significantly predict health screening behaviour and interest in it, 96 in studies where the influence of controllability was not investigated. Also, health optimism was found to interact with mortality salience, such that women high in health optimism were significantly more likely to intend to engage in breast self-examination when primed with a mortality salience cue than women who were not. 98 Although this study 98 purportedly investigated health optimism, the scale items related to an individual’s ability to control their health outcomes and thus were more reflective of controllable mortality risk. Unlike optimism, which is viewed as a trait because it is relatively stable over time, 99 uncontrollable mortality risk is dependent on the environment and changes in response to cues. 94 The relationship between perceived controllability of risk and preventative health behaviours for COVID-19 reveals complexities of the interaction, as fear related to the COVID-19 pandemic was found to interact with perceived control over it, so that in those of low perceived control, fear increased engagement in preventative health behaviours both generally and relating to the pandemic, whereas for those of high perceived control, increased fear decreased engagement in preventative health behaviours and had little effect on COVID-19 preventative health behaviours. 100 This finding may appear to contradict the mortality risk hypothesis, however the included scale measured perceived control over contracting and being ill with COVID-19, rather than mortality. In fact, there are no existing studies on COVID-19 that have specifically addressed uncontrollable mortality risk. Thus, it is reasonable to predict that low SES and perceived uncontrollable mortality risk will negatively predict AI-enabled screening for neurodegenerative disease via OCT imaging.
Given the heterogeneity of findings related to demographic factors and preventative health behaviours, findings for sex/gender, age and ethnicity are next presented in table format, summarising the directions of their predictions in screening for neurodegenerative disease.
Age
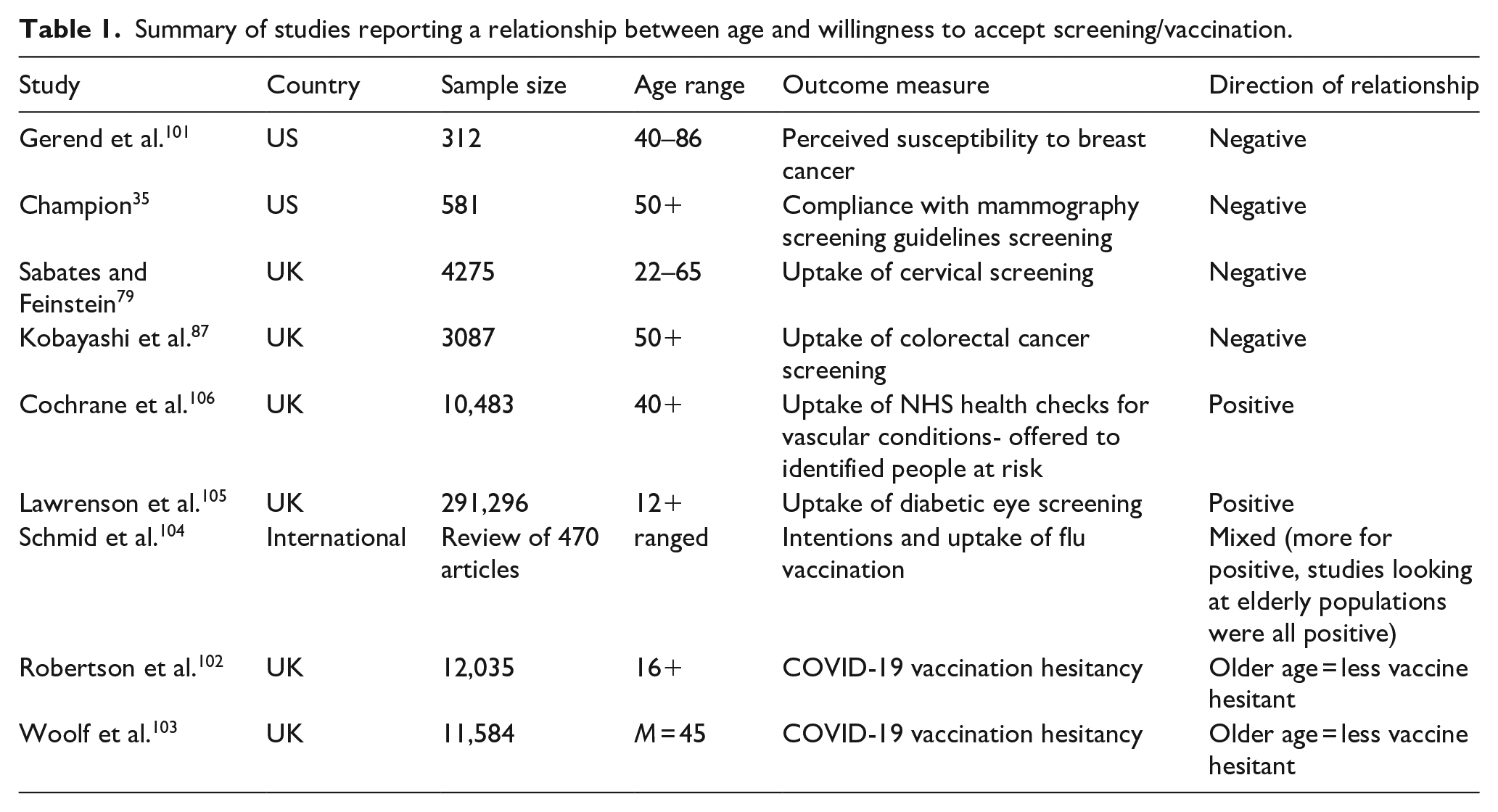
As shown in Table 1, the relationship between age and health behaviour depends on the health behaviour. Age negatively predicts cancer screening35,79,87,101 but positively predicts vaccination,102,103 especially in older populations 104 or for COVID-19,102,103 uptake of screening for eye conditions relating to eye health 105 and attendance of NHS health checks. 106 A large international review of flu vaccination intentions and behaviour found the prediction from age to be highly inconsistent, 104 although the review was international and so these polarised findings may be due to differences in vaccination initiatives and incentives. Additionally, age may also interact with factors such as SES 35 to predict screening.
Summary of studies reporting a relationship between age and willingness to accept screening/vaccination.
Sex/gender
It is important to note that the difference in UK screening uptake of colorectal cancer and cervical and breast cancer may be due to a sex/gender difference, namely that women are more likely to attend screening. However, the global review by Schmid et al. 104 found polarised results for the relationship between sex and flu vaccination, with very few studies finding no significant differences; possibly due to publication bias. Namely, the authors concluded that gender was a key predictor of flu vaccination in elderly, healthcare professional and general populations, but for those with chronic diseases. Being female was more frequently cited as a barrier, although many studies also cited it as a facilitator. Conversely, there is consistent evidence that being male predicts COVID-19 vaccination in both US 107 and UK102,103,107 samples. Men are 41% more likely to intend to receive the vaccine on average, 108 an effect which is fully mediated by perception of others as intending to be vaccinated, perceived control over vaccination, and less anticipation of negative feelings such as fear. 109 For other preventative healthcare, large UK studies found females to be more likely to attend colorectal screening,87,110 males to have a higher uptake of NHS health checks for those at risk of vascular diseases, 106 and no effect of gender on the uptake of free eye examinations. 111 As shown in Table 2, the effect of sex is largely dependent on the type of preventative healthcare, and thus it is uncertain whether or how sex might affect screening for neurodegenerative diseases.
Summary of studies reporting a relationship between sex/gender and willingness to accept screening.

Ethnicity
Ethnicity as a predictor of preventative health behaviours is more consistent (Table 3). In Western countries, Black, Asian and other ethnic minority participants are less likely than White participants to attend flu vaccination,88,104 prostate cancer 112 and colorectal cancer 112 screening. The same pattern is observed for cervical screening in the UK,79,113 even after controlling for SES. 113 One literature review concluded that ethnicity is an independent predictor of preventative health behaviours, and therefore should not be collapsed into an overarching variable of SES. 112 In the US and UK, participants who are an ethnicity other than White are also more hesitant towards COVID-19 vaccination than White participants,102,103,107,114 but this only translates to reduced attendance in the US and not the UK. 107 Hesitancy is highest in Black participants but is also increased in Asian and Hispanic participants.102,107 Breast cancer screening is not predicted by ethnicity in the US 88 and UK, 113 but is in Canada, 115 although the review of studies in Canada does not quantify this effect. As the effect of ethnicity is not accounted for by SES, a potential alternative explanation is health literacy. For example, as for the relationship with education, health literacy was found to mediate the relationship between ethnicity and flu vaccination, but not for mammography screening or dental check-ups. 88 Indeed, COVID-19 vaccine hesitancy was found to partly be caused by a lack of knowledge, 107 indicating health literacy to be a mediator of ethnicity for vaccines, but not screening. The lack of ethnicity diversity in vaccine study samples and lack of trust have also been cited as causes of COVID-19 vaccine hesitancy. 103 In the case of screening, distrust may be particularly acute when healthcare is carried out by AI, given the longstanding built in biases in AI towards ethnic majorities due to sampling bias. 116 By nature, ethnic minorities are less represented when building AI algorithms, so the AI becomes less accurate for them. Previous examples have found schizophrenia to be over diagnosed, 117 and prediabetes and diabetes to be underdiagnosed 118 in ethnic minorities. Provided people of ethnic minorities are aware of these previous issues, this may lead to distrust and hesitance towards screening using AI. In summary, those of Black ethnicity are the least likely to take part in all preventative care aside from mammography, for reasons such as distrust which is arguably justified given that non-White people still experience discrimination within healthcare,119,120 resulting in poorer treatment of ethnic minorities. 120
Summary of studies reporting a relationship between ethnicity and willingness to accept screening and vaccination.
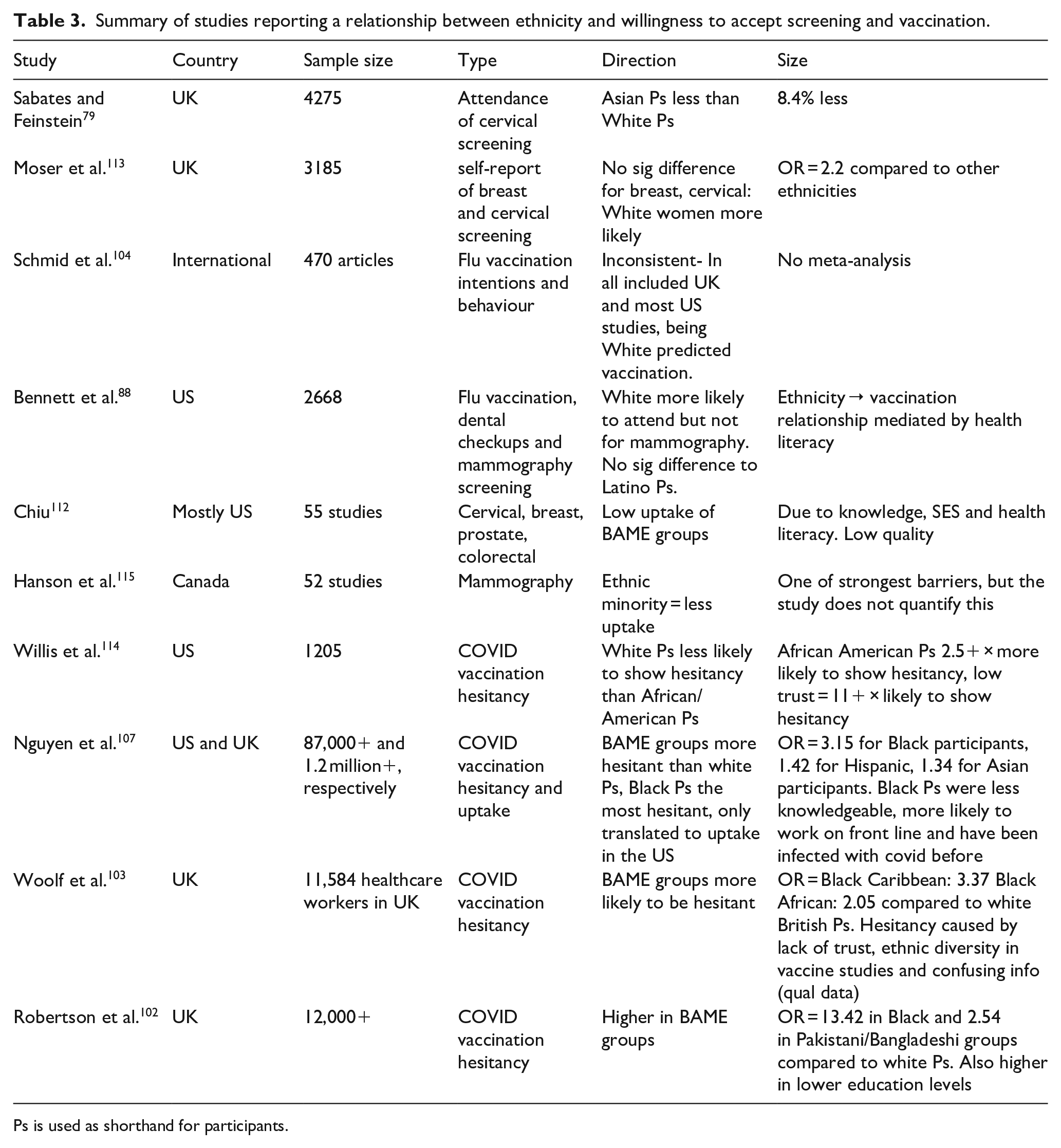
Ps is used as shorthand for participants.
Conclusion
From the findings of this literature review, the most important positive predictors of the acceptability and uptake of AI-enabled screening for neurodegenerative disease via OCT imaging, in the UK, are likely to be:
1) Knowing someone/possessing a relative with a neurodegenerative disease (mediated by social influence).
2) Perceived risk (mediated by worry).
3) Perceived benefits of screening.
4) The use of a human agent rather than AI.
5) Previous experience of receiving an OCT retinal scan.
6) Education (mediated by health literacy).
7) High SES (mediated by uncontrollable mortality risk).
8) Being an ethnic majority (i.e. White in the UK) compared to an ethnic minority.
The above factors are not an exhaustive list, but represent those for which the evidence discussed above is most consistent. Future qualitative and quantitative research would benefit from specifically exploring the acceptability of AI-enabled screening for neurodegenerative disease via OCT imaging. This literature review provides a basis to explore the above factors in relation to uptake of such a tool.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ‘This report is independent research funded by the National Institute for Health Research and NHSX (Artificial Intelligence, “OCTAHEDRON : Optical Coherence Tomography Automated Heuristics for Early Diagnosis via Retina in Ophthalmology and Neurology”, AI_AWARD01976).
Significance for public health
This study highlights the importance of investigating the factors that determine uptake of a new screening tool alongside the development of the tool itself. Further research around the potential influencing factors named in this study will help inform interventions to increase uptake when screening for neurodegenerative diseases using OCT and artificial intelligence becomes available. Furthermore, this narrative review provides valuable insights for predicting health screening behaviour in general, and how predictors might change depending on the individual, the disease that is being screened for, and the nature of the screening procedure.