
Abstract
Background:
One of the impacts in anatomic laryngeal and phariyngeal changes after total laryngectomy (TL) is oropharyngeal dysphagia (OPD). The detection of neopharyngeal residue as a sign of OPD can be performed by videofluoroscopy (VFS) and flexible endoscopic evaluation of swallowing (FEES). The availability of these tools in rural areas is still limited, thus the treatment of OPD is not maximal. There is a need for a more practical tool, including the modified swallowing outcomes after laryngectomy (SOAL) questionnaire.
Methods:
This was an analytic observational diagnostic study with a cross-sectional approach. Samples were obtained in Otorhinolaryngology Oncology Clinic and Outpatient Clinic of Dr. Soetomo General Academic Hospital, Surabaya, Indonesia, who filled SOAL modified questionnaire followed by FEES. Samples were obtained within 3 months from 10 May to 10 August 2021. The number of samples obtained through simple random sampling was 16 post-TL patients from a total population of 17 patients who met the inclusion and exclusion criteria. The conformity test between modified SOAL questionnaire and FEES was analyzed using McNemar comparison test and Kappa association test.
Results:
McNemar test showed no significant difference between both assessment tools (p > 0.05), and the Kappa test showed an association between both tools (p < 0.05). The results of this study stated that there was conformity between modified SOAL questionnaire and FEES in patients after TL in all types of food bolus had Kappa score of >0.81, showing a reliable association between these tools. Kappa test also showed that out of all three types of boluses, the soft bolus had the highest conformity with a Kappa score of 0.875, followed by thick bolus with 0.839, and watery bolus with 0.818.
Conclusion:
There was a conformity between the results of the modified SOAL questionnaire and FEES in head and neck surgery patients after TL.
Keywords
Introduction
Neopharynx formed after total laryngectomy (TL) affects the stage of swallowing due to changes in the anatomy and physiology of the larynx after TL surgery. Post-TL oropharyngeal dysphagia (OPD) is more common, characterized by the presence of neopharyngeal residues. 1 The diagnosis of OPD is established by videofluoroscopy (VFS) and Flexible Endoscopic Evaluation of Swallowing (FEES).2,3 The availability of these two tools is still very limited in some areas which may cause the management of OPD not to be optimal, so an effective and practical tool which is easier to work with is needed. One such tool is the Swallowing Outcomes After Laryngectomy (SOAL) questionnaire which contains 17 questions regarding swallowing disorders in post-TL patients.4,5
In recent years, many studies have used questionnaires as an easier tool in evaluating dysphagia in post-TL patients.4–6 This study used a SOAL questionnaire which had been modified into 13 question items related to swallowing disorders in post-TL patients, which has been adjusted per item, then the results of the modified questionnaire score was be compared with the FEES examination available at Dr Soetomo Hospital, Surabaya, Indonesia. Several studies explain that the advantage of VFS examination is that it can assess the swallowing process in real time at each swallowing phase, while FEES is better at assessing neopharyngeal residues in pharyngeal phase.2,3
The incidence of oropharyngeal dysphagia after TL had not been widely reported in studies. Post-TL patients often complain of changes in the consistency of food and the feeling of food residue in the throat.1,2 This seems to have not received special attention and until now the relationship between pharyngeal residues and OPD in post-TL otolaryngological patients is not known with certainty. The purpose of this study was to explain the conformity between the modified SOAL and FEES questionnaires in post-TL otolaryngological patients.
Design and methods
This study was an analytical observational diagnostic test with a cross sectional approach. Samples were taken at the Otorhinolaryngology Oncology Clinic and Outpatient Clinic, Broncho-Esophagology Division, of Dr. Soetomo Hospital, Surabaya, Indonesia, as the site to fill out the modified SOAL questionnaire, which was then followed by a FEES examination. Sampling was carried out for 3 months starting from May 10 to August 10, 2021 by simple random sampling. The sample size as many as 16 patients was taken by simple random sampling who had met the inclusion and exclusion criteria with no sample declared to have resigned or dropped out.
The modified SOAL questionnaire contains 13 question items. The assessment of the modified SOAL questionnaire has a 3-point response scale, that is, “no” = 0, “a little” = 1 and “a lot” = 2. The total score ranges from 0 to 26 with a higher score indicating that there are larger reported problems. The questionnaire rating scales are light, moderate, and severe whose values (cut-off points) were determined from the results of this study. The assessment of neopharyngeal residue with FEES used Farneti score pharyngeal residue scale. The rating scale for the number of consecutive swallows on the same bolus is 1 = swallowing once; 2 = swallowing twice; 3 = three times; 4 = four times; and 5 = swallowing five times or more. The examination used three boluses with the order of administration being used as follows: first with watery bolus, then thick bolus and finally soft bolus.
The filling of the modified SOAL questionnaire and FEES was done on the same day. The patient received a modified SOAL questionnaire sheet and an explanation of how to fill out the questionnaire from the researcher. The filling of the questionnaire was accompanied by the researcher and the collection of the questionnaires was carried out on the same day. The FEES examination was carried out by a otorhinolaryngology broncho-esophagology consultant at the Otorhinolaryngology Oncology Clinic and the Outpatient Clinic.
Data obtained in the study were presented in tabular form and analyzed statistically. The search for cut-off point from the modified SOAL questionnaire was analyzed using the Receiver Operating Characteristic (ROC) curve. The conformity of the modified SOAL questionnaire with FEES was analyzed using a comparison test (McNemar test) and association test (Kappa test). This research was approved by the Health Research Ethics Committee of Dr. Soetomo Hospital, Surabaya (no. 0193/KEPK/V2021).
Results
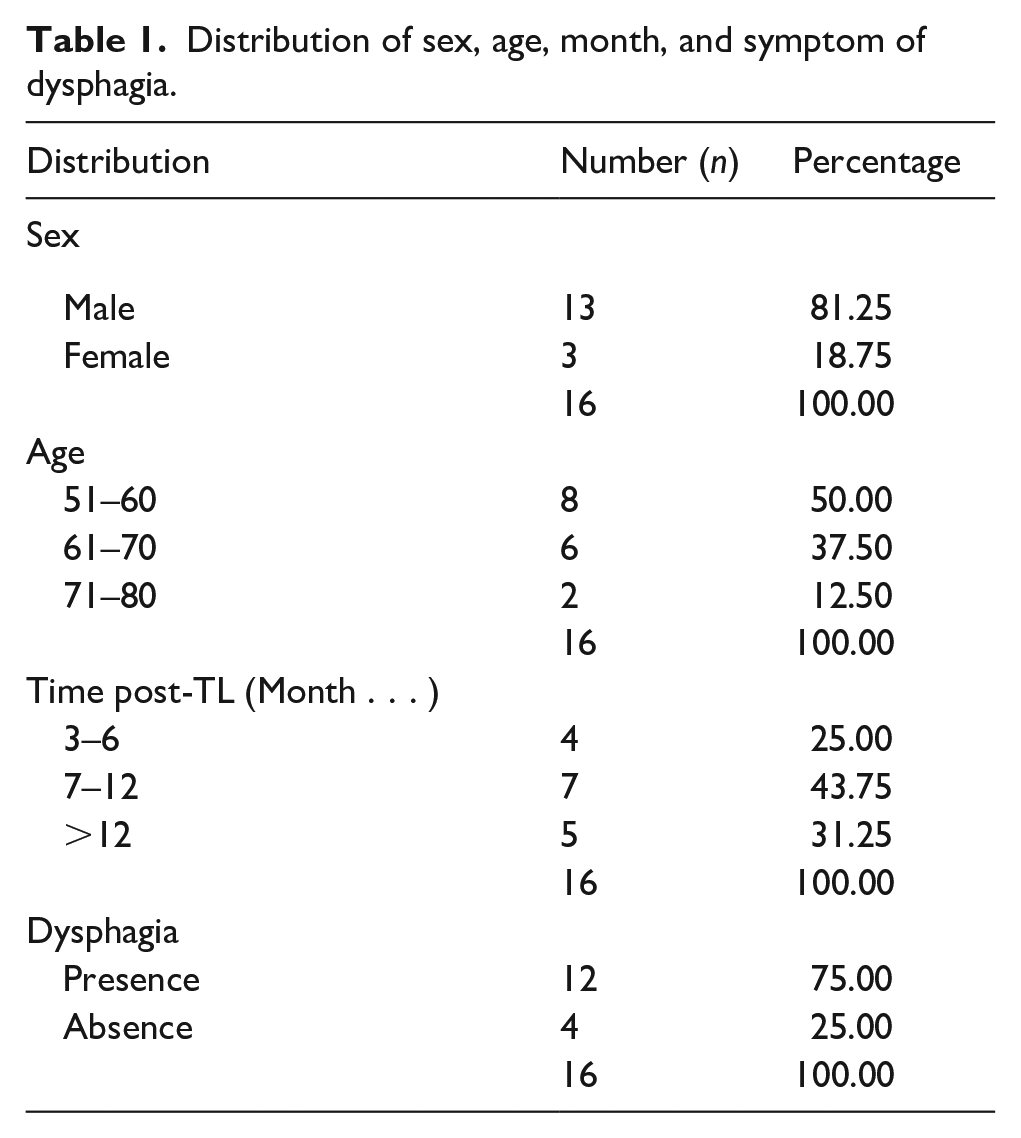
Basic data in this study consisted of sex, age, length of time after TL (in month), and symptom of dysphagia. The number of male samples was higher than female samples, where the male patients were 13 (81.25%) and female samples 3 (18.75%). The largest age group was between 51 and 60 years, consisting of eight patients (50.00%). The distribution of post-TL length of time was between 7 and 12 months in seven patients (43.75%), >12 months in five patients (31.25%) and 3–6 months in four patients (25.00%). Dysphagia was found in the majority of post-TL patients, which was in as many as 12 patients (75.00%), while four patients (25.00%) did not show post-TL dysphagia (Table 1).
Distribution of sex, age, month, and symptom of dysphagia.
Neopharyngeal residual assessment with a good Farneti score was found in nine patients (56.25%) with watery bolus, followed by thick bolus in three patients (18.75%), and soft bolus in two patients (12.50%). The highest moderate Farneti score was found in seven patients (43.75%) with thick bolus, followed by soft bolus in six patients (37.50%), and watery bolus in five patients (31.25%). The poor Farneti scores were found in eight patients (50.00%) with soft bolus, followed by thick bolus in six patients (37.50%), and watery bolus in two patients (12.50%) (Table 2).
Distribution of three-bolus neopharyngeal residues with Farneti score.

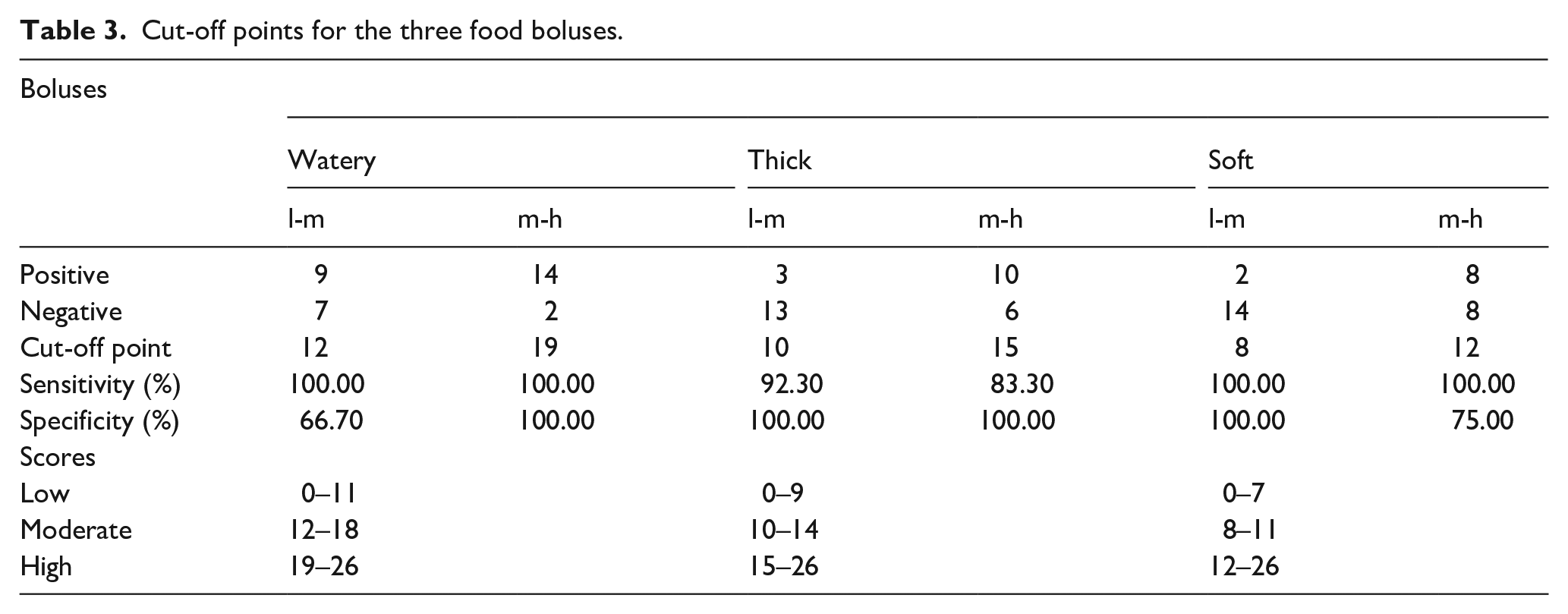
The modified questionnaire scores of three types of food boluses based on the cut-off point indicated that the watery bolus had low degree 0–11, moderate 12–18, and high 19–26. Thick bolus of low degree 0–9, moderate 10–14, and high 15–26, while soft bolus of low degree 0–7, moderate 8–11, and high 12–26 (Table 3).
Cut-off points for the three food boluses.
McNemar’s comparative test on all types of food boluses showed no difference between the results of the examination tool (p > 0.05). Kappa association test showed that there was an association between the results of the examination tool (p < 0.05). This showed that there was conformity between the modified SOAL questionnaire and FEES in post-TL patients on all types of food boluses with Kappa values >0.81, with the strength of conformity between the two tools being very good. The Kappa test of the three food boluses with the highest conformity was the soft bolus with Kappa value of 0.875, followed by thick bolus with Kappa value of 0.839, and watery bolus with Kappa value of 0.818 (Table 4).
Average Kappa values of the three food boluses.

Good: ≤2 swallows, moderate: 3–4 swallows, poor: ≥5 swallows.
Discussion
The sex distribution in this study showed that the male samples consisted of 13 patients (81.25%), higher than female patients, which consisted of three patients (18.75%). This was in accordance with the study of Balaji et al. who reported that of the 67 patients who underwent TL from June 2015 to November 2017, male patients were found to be 63 patients (94%) more than female patients who were only four patients (6%). 7 The higher incidence in males than females was due to smoking habits and higher alcohol consumption in males. Most patients in this study belonged to the age group 51–60 years, consisting of eight patients (50.00%), followed by the age group 61–70 years as many as six patients (37.50%) and 71–80 years as many as two patients (12.50%). This was in accordance with Johnson’s research which reported an increase in the incidence of KL at the age above 50 years, starting from the fifth to seventh decades of life. 8
In this study, the longest time after undergoing TL surgery ranged from 7 to 12 months, namely in 7 patients (43.75%), >12 in 5 patients (31.25%) and 3–6 months in 4 patients (25.00%). This finding was in accordance with the theory that the difference in the swallowing process in the early postoperative month of TL can be influenced by the wound healing process which will later determine the function of the remaining anatomical structures after undergoing TL. The ability of the pharyngoesophageal segment to enlarge and coupled with force from the base of the tongue will have an effect on the length of time the pharyngoesophageal segment remains open. It will also determine the ease with which the patient swallows various food consistency. These factors ultimately lead to an increase in neopharyngeal residue, which in turn will increase the time of swallowing, swallowing frequency, prolonged eating and social pressure during eating. The function of the pharyngoesophageal segment in the early post-TL months compared to 12 months post-TL also showed differences in function, with improvement occurring over time.9,10
Symptom of dysphagia were found in the majority of post-TL patients in this study, which was in 12 patients (75.00%), while four patients (25.00%) did not show dysphagia. In this study, most of the post-TL patients complained of swallowing difficulty or dysphagia and there were only four patients who did not have dysphagia with postoperative TL of >12 months. These four patients had no symptoms, but FEES examination revealed positive residual findings. This finding was in agreement with the study by Maclean et al. who reported that some patients after laryngeal removal also often did not have swallowing symptoms because they had adjusted their daily diet to the ability to swallow, although FEES examination still showed the presence of the residue. 10 The reduction in the remaining laryngeal and pharyngeal sensitivity post-TL is also highly variable and can differ from patient to patient in relations to the stage of the cancer before the surgery, the area of the organ removed in the surgery, and the technique used.7,11–13
The findings of FEES in this study showed that neopharyngeal residues with good Farneti score were found in nine patients (56.25%) with watery bolus, followed by thick bolus in three patients (18.75%), and a soft solid bolus in two patients (12.50%). The moderate Farneti score was found mostly in seven patients (43.75%) with thick bolus, followed by soft bolus in six patients (37.50%), and watery bolus in five patients (31.25%). Poor Farneti scores were found in eight patients (50.00%) with soft bolus, followed by thick bolus in six patients (37.50%), and watery bolus in two patients (12.50%). These results were in accordance with the results of the study of Coffey et al. which reported the findings of residues in several anatomical areas with different consistency and showed that solid soft bolus residues were the most common, followed by thick bolus, and lastly, the watery bolus. 13 FEES examination revealed solid soft bolus residues in as much as 96% of the upper esophagus and neopharynx, whereas watery residues were only 23.30% of the neopharynx.13–15
The cut-off point of the watery bolus with moderate degree was 12 with a sensitivity of 100.00% and specificity of 66.70% and the high degree was 19 with a sensitivity of 100.00% and a specificity of 100.00%. The cut-off point of thick bolus with moderate degree was 10 with a sensitivity of 92.30% and specificity of 100.00% and the high degree was 15 with a sensitivity of 83.30% and a specificity of 100.00%. The cut-off point for soft bolus with moderate degree was eight with sensitivity of 100.00% and specificity of 100.00% and the high degree was 12 with a sensitivity of 100.00% and a specificity of 75.00%.
Determination of the cut-off point in this study aimed to find the scoring of the modified SOAL questionnaire in classifying patients whether they were classified as having mild, moderate, or severe swallowing disorders. Previous research by Govender et al. did not yet have a cut-off point from the SOAL questionnaire. The cut-off point score is expected to make it easier for doctors to screen the swallowing disorders and determine the severity of dysphagia, whether mild, moderate, or severe.
The modified SOAL questionnaire scores from three types of food boluses in this study were watery boluses of low degree 0–11, moderate 12–18, and high 19–26. Thick bolus scores of low degree 0–9, moderate 10–14, and high 15–26 while soft bolus scores of low degree 0–7, moderate 8–11, and high 12–26. This was in accordance with Govender et al. who reported the results of SOAL questionnaire scores ranged from 0 to 34, where higher scores indicated that the reported problems were worse. Patients with no adverse findings on MBS would have a predicted SOAL score of 5, whereas patients with all adverse findings on all boluses would have a predicted score of 34. Govender et al. reported that further research is needed to determine swallowing function in post-TL patients, whether they are mild, moderate, or severe.
Three different SO-AL modified questionnaire scores from each type of food bolus in this study consisted of three degrees of dysphagia, that is, mild, moderate, and severe. This study proved the hypothesis that there was conformity between the modified SOAL questionnaire and FEES in post-TL otolaryngological patients. Kappa value >0.81 indicated the strength of the conformity between these two tools was very good. The statistical test of all types of food boluses using the McNemar comparison test showed no difference between the results of these examination tools (p > 0.05), and the Kappa association test showed that there was an association between the results of these tools (p < 0.05). Based on the Kappa test of the three food boluses, the highest conformity was found in the soft bolus with Kappa value of 0.875, followed by thick bolus of 0.839, and a watery bolus of 0.818.
These findings were in accordance with the findings of Lee et al., who showed that SOAL was a sensitive and validated measurement tool to evaluate changes occurring in post-TL swallowing process, especially in patients undergoing long-term follow-up care. The SOAL questionnaire may become a simple and accessible screening tool to identify swallowing problems during long-term postoperative care.4–6 Govender et al., tested the psychometric properties of SOAL scale in a representative sample of post-TL patients and provided strong evidence of its internal consistency and validity.
A study by Maclean et al., also reported that postoperative TL patients often revealed residues in the neopharynx, mostly soft boluses. Watery boluses tend to flow to a lower area and follow the direction of gravity downwards, whereas denser boluses often clump together and form a residue. 12 Queija et al., also reported that from 28 study samples, 15 were post-TL patients who showed that 64.22% had pharyngeal residue on soft bolus administration and also reported restrictions on oral consumption of soft solid foods in 8 (28.5%). 16 Viscous fluids have a slower transit rate as they pass through the oropharyngeal stage of swallowing.17–20
The three food boluses in this study showed that bolus with high conformity was the soft bolus with a Kappa value of 0.875. This was consistent with the theory that the expected optimal outcome for swallowing in post-TL otolaryngological patients is the ability to swallow soft boluses.17,18 The results of this study also proved that the modified SOAL questionnaire can be used as a screening tool to assess the presence of OPD in post-TL. Studies comparing the modified SOAL and FEES questionnaires have not been reported, but there has been a theory and a previous study by Govender et al. who found that the SOAL questionnaire is a sensitive, validated tool and can be used as a screening tool in diagnosing dysphagia.4–6
The limitation of this study was that, due to the implementation of community activity restrictions to suppress the increasing rate of Covid-19 virus positivity, the visit of post-TL patients to the hospital reduced and limited so that the research population was limited. The population in this study was limited by 3 months so that the results of this study can only be generalized within the 3 months of the study. Further research needs to be done with a wider population, not limited by time and place, so that the results can be generalized more widely. Further research can be conducted to analyze the determinant factors that influence the occurrence of dysphagia in post-TL patients more deeply.
Conclusion
There is a conformity between modified SOAL and FEES questionnaires in post-TL otolaryngological patients. The modified SOAL questionnaire can be used as a diagnostic or screening tool to detect OPD and as a reference in treating OPD in post-TL otolaryngological patients if FEES is not available in the hospital.
Footnotes
Acknowledgements
The authors would like to express our highest gratitude to the Faculty of Medicine, Airlangga University, Surabaya for encouraging interdisciplinary research collaborations and providing academic and practical support for this work.
Contribution
Conceptualization: Rista Rahayu Rarasati, Sri Herawati Juniati, Muhtarum Yusuf. Data curation: Rista Rahayu Rarasati. Formal analysis: Rista Rahayu Rarasati, Sri Herawati Juniati. Methodology: Rista Rahayu Rarasati, Muhtarum Yusuf. Project administration: Rista Rahayu Rarasati. Writing – original draft: Sri Herawati Juniati, Muhtarum Yusuf. Writing – review & editing: Sri Herawati Juniati, Muhtarum Yusuf.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study had met the ethical clearance procedure before the conducting of the study at Soetomo Hospital, Surabaya, with ethical clearance number 0193/KEPK/V2021.
Patient consent for publication
Not applicable
Informed consent
The manuscript does not contain any individual person’s data in any form.
Significance for public health
The availability of these tools in rural areas is still limited, thus the treatment of OPD is not maximal. There is a need for a more practical tool, including the modified swallowing outcomes after laryngectomy (SOAL) questionnaire. The incidence of oropharyngeal dysphagia after TL had not been widely reported in studies. Post-TL patients often complain of changes in the consistency of food and the feeling of food residue in the throat. This seems to have not received special attention and until now the relationship between pharyngeal residues and OPD in post-TL otolaryngological patients is not known with certainty. The purpose of this study was to explain the conformity between the modified SOAL and FEES questionnaires in post-TL otolaryngological patients.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.