
Abstract
Background:
The study was designed to compare parametric and Cox regression survival models. It was also aimed at determining risk factors of death due to HIV/AIDS.
Design and methods:
The models were fitted to time from ART initiation to death due to HIV/AIDS while using data that was collected from 6670 patients records who registered for ART from 2007 to 2012 at Ntcheu district hospital in Malawi. The best fitting model was used to determine risk factors of death due to HIV/AIDS.
Results:
The exponential and Gompertz model competed very well with the Cox regression. Patients in WHO clinical stage 4 (HR = 1.69, p-value <0.001) and males (HR = 1.74, p-value <0.001) were associated with increased hazard of death than those in WHO clinical stage 3 and females. Patients with high body mass index (HR = 0.82, p-value <0.001) were associated with lower hazard of death than those with lower body mass index.
Conclusions:
Parametric models may perform as good as the Cox regression and the plausibility of all models needs to be investigated to use the correct model for accurate inferences. Furthermore, strategies to limit deaths due to HIV/AIDS should initiate ART early before WHO clinical stage 4 and males should receive special attention. The strategies should also aim at improving the body mass index of patients.
Introduction
The world has been greatly hit with high prevalence of human immune deficiency virus/acquired immune deficiency syndrome (HIV/AIDS), more especially in developing countries such as those in the sub-Saharan Africa. 1 The disease has claimed lives of many people. The World Health Organization (WHO) estimated that 38 million people were living with HIV/AIDS globally, with 1.7 million new infections in 2019. 2 The African continent remains heavily affected region in the global HIV epidemic with 25.7 million people living with HIV/AIDS out of the world total of 38 million as of 2019 and the southern Africa has been greatly affected.2,3 Meanwhile, the world new HIV infections and deaths have been decreasing since the onset of the epidemic. For example, in 2017, approximately 1.8 million new HIV infections occurred, compared to 3.4 million in 1996 and approximately 940,000 people died from the disease world-wide in 2017, compared to 1.9 million in 2004. 4 The decrease has been due to the introduction of antiretroviral therapy (ART) which reduces the viral load of a person with HIV to undetectable levels and which also reduces the risk of transmitting the virus to uninfected persons. A joint report from the United Nations (UN) program on HIV/AIDS, WHO, and United Nations International Children Emergency Fund (UNICEF) on HIV/AIDS treatment, 5 indicated a huge acceleration in the rollout and uptake of antiretroviral therapy since 2011. A record of 23.3 million people living with HIV were accessing treatment in 2018 compared to 13.0 million in 2013. 6
The prevalence of HIV/AIDS for adults in Malawi as of 2017 was 10.4% with about 38,000 newly diagnosed cases. 7 In Ntcheu district, the prevalence of HIV/AIDS in 2014 was 14.8%. 8 The HIV/AIDS prevalence in Malawi has decreased from 11.8% in 2004 to 10.4% in 2017. Similarly, in Ntcheu district, it has decreased from 22% 9 to 14.8%. The decline in HIV prevalence has been attributed to introduction of antiretroviral therapy. The Malawi government started giving free antiretroviral therapy in public sectors in 2004 and a total of 10,761 patients were on ART. 10 The Malawian government in 2011 received funding from the president’s emergency plan for AIDS relief (PEPFAR) through USAID for essential HIV/AIDS programs and services. The funding assisted to register significantly large number of HIV infected patients for ART by the end of 2011. It had been indicated that by 31 March, 2012, 347,983 (73%) HIV/AIDS infected patients were on ART. 11 This was an improvement compared to 2004 HIV/AIDS infected people who were registered on ART.
A common theme in HIV/AIDS care and support is the prognosis of the disease. Particularly, it is common to analyze time-to-event, where the event may be “death,” “CD4 immune recovery,” or “attrition after initiating ART.” More often, the question of interest is finding the median time to an event or the determinants of time to an event. Researchers commonly apply the semi-parametric Cox regression to address these questions. The advantage of Cox regression over parametric survival models is that it does not assume any distribution about the survival times, except, the proportionality of hazard functions over time. Nevertheless, Cox regression has some shortfalls over the parametric models. First, it is in efficient in case of long observation time and that there is usually violation of distribution free assumption. 12 In addition, Cox regression assumes a constant hazard over time which is frequently violated. 12 Furthermore, survival and cumulative hazard functions in Cox regression are stepwise and it is reasonable to think that they are smooth. 13 A number of studies comparing Cox regression and parametric survival models have been conducted and they have shown parametric models outperforming Cox regression.12,14–17 This study aimed at comparing the performance of parametric and Cox regression survival models. The study would also determine risk factors of death in HIV patients on ART. The study would be confirmatory on both the comparison of parametric and Cox regression survival models and risk factors of death.
Design and methods
Study area
The data used in this study came from the study that was conducted at Ntcheu district hospital in Malawi. Malawi is one of the countries from the sub-Saharan Africa and is divided into three regions, namely, South, Central, and North. Ntcheu district is located in the central region and it has a population size of 471,589. 18 The district hospital had 269 beds and there were 37 health centers of which 15 were private at the time of this study. The hospital started providing free ART in 2005. However, out of these 37 health centers, five were not providing ART due to the fact that they had no trained staff such as medical assistants and nurses. In addition to this, the district did not have enough qualified personnel to administer HIV/AIDS tests. Ntcheu district had registered 11,340 HIV/AIDS infected patients since 2005 and all of them were on ART. 11
Study design and data collection
The study design was a retrospective cohort study where a total of 6670 patients were followed from 2007 to 2012. The sample size depended on the patients’ records available within the study period, 2007–2012 and hence forth, sample size calculation was not necessary. Data was collected from medical records of patients who were registered for ART from 1 January, 2007 to 31 December, 2012 at Ntcheu district hospital which were electronically stored in Baobab health trust touch screen computers. The data was collected from the patients’ records by hospital officers, namely, one surveillance assistant, two data entry clerics, HIV/AIDS counselor, and the ART clinical nurse. The clinical nurse assisted in tracking down the quarterly data from ART supervision monitoring check list from 1 January, 2007 to 31 December 2012, to ensure that the data taken reflected what had been stored electronically.
Inclusion and exclusion criteria
Although ART program at Ntcheu hospital started in 2005, the study did not look at patients from 2005 to 2006, considering that the patients’ records within this time frame had been tampered with and hence were not reliable. Furthermore, the patients included were 15 years and above since information for patients younger than 15 years was not available.
Data variables
The response variable in the study was time from initiation of ART to death due to HIV/AIDS. Failure was defined as death due to HIV/AIDS. Individuals who died of other causes where considered as censored according to the standard analytical approach, otherwise, competing risk analysis methods would be employed. 19 Variables such as age (in years), body mass index (BMI) (kg/m2), occupation (non-worker/worker), WHO clinical stage (stage 3/stage 4), CD4 (initiated at ≤250 cells/µL/initiated at >250 cells/µL), and sex (female/male) were considered as independent variables. Age and body mass index were continuous variables. The inclusion of the mentioned independent variables was based on the previous research.20–24
Statistical analysis
First, descriptive analyses in terms of frequency tabulation, numerical summaries, and basic statistical inference procedures in form of Kaplan-Meier curves and Log-rank test were performed. Kaplan-Meier curves were used to compare survival of HIV/AIDS patients graphically between groups while the Log-rank test was used to determine whether there was significant difference in survival between groups.
Multiple variable parametric survival and semi-parametric Cox proportional hazard models as described by Kleinbaum and Klein
25
were then fitted. The Cox proportional hazard model is specified as
Model comparison was by the R2, Brier score and the Cox-Snell residuals plots. Furthermore, the correlation coefficient between the observed and predicted survival probabilities was also used to select the best model. The observed survival probabilities were based on Kaplan-Meier survival estimates. A model with a smaller Brier score and a high R2 and correlation between observed and fitted survival probabilities was considered as the best model in terms of fit and prediction. A Cox-Snell residuals plot with most of the points falling on the 45° line, corresponded to a better fitting model. The global test of the proportional hazard assumption of the Cox regression was also done to check its validity. The use of Akaike information criterion (AIC) and Bayesian information criterion (BIC) was not possible in this study as the AIC and BIC for parametric models is based on full likelihood while AIC and BIC for Cox regression is based on partial likelihood and hence they were not comparable. Statistical analyses were performed in stata version 14 (StataCorp, College Station, TX, USA) and R.
Ethical consideration
Ethical approval was not sought for the present study because the study used secondary data and that the data was analyzed anonymously without using patients’ names. Permission to use the data was granted by the District Health Officer for Ntcheu district.
Results
The tabulation of categorical variables showed that for the 6670 HIV/AIDS patients that were studied from 2007 to 2012, 482 (7.2%) had died, 1558 (23.4%) were transferred out, 1466 (22%) defaulted, and 3161 (47.4%) were found to be alive and on ART. The frequency tabulation analysis also revealed that more females, 4527 (67.9%), were registered during the period as compared to their male counterparts, 2143 (32.1%). The numerical summaries for continuous parameters (Table 1), show that the mean survival time for the patients was 18.37 years. The average age of patients was 37.89 years.
Numerical summaries of HIV/AIDS patients taking ART at Ntcheu district hospital in Malawi, 2007–2012.

SD: standard deviation.
Figure 1 presents Kaplan-Meier curves showing the probability of survival of HIV/AIDS patients taking ART over time at Ntcheu district hospital after initiation of ART. The results from Kaplan-Meier survival curves have shown that females have a better survival as compared to males, as evidenced from the survival curve for females being positioned above that of males (Figure 1(a)). It can also been observed that patients who were initiated ART at WHO clinical stage 3, had a better survival as compared to those who were initiated at WHO clinical stage 4 (Figure 1(b)). Furthermore, HIV/AIDS patients who were not working, had a better survival as compared to those who were working (Figure 1(c)). HIV/AIDS patients who were initiated ART at CD4 ≤ 250 cells/µL, showed better survival as compared to those initiated at CD4 count >250 cells/µL (Figure 1(d)).
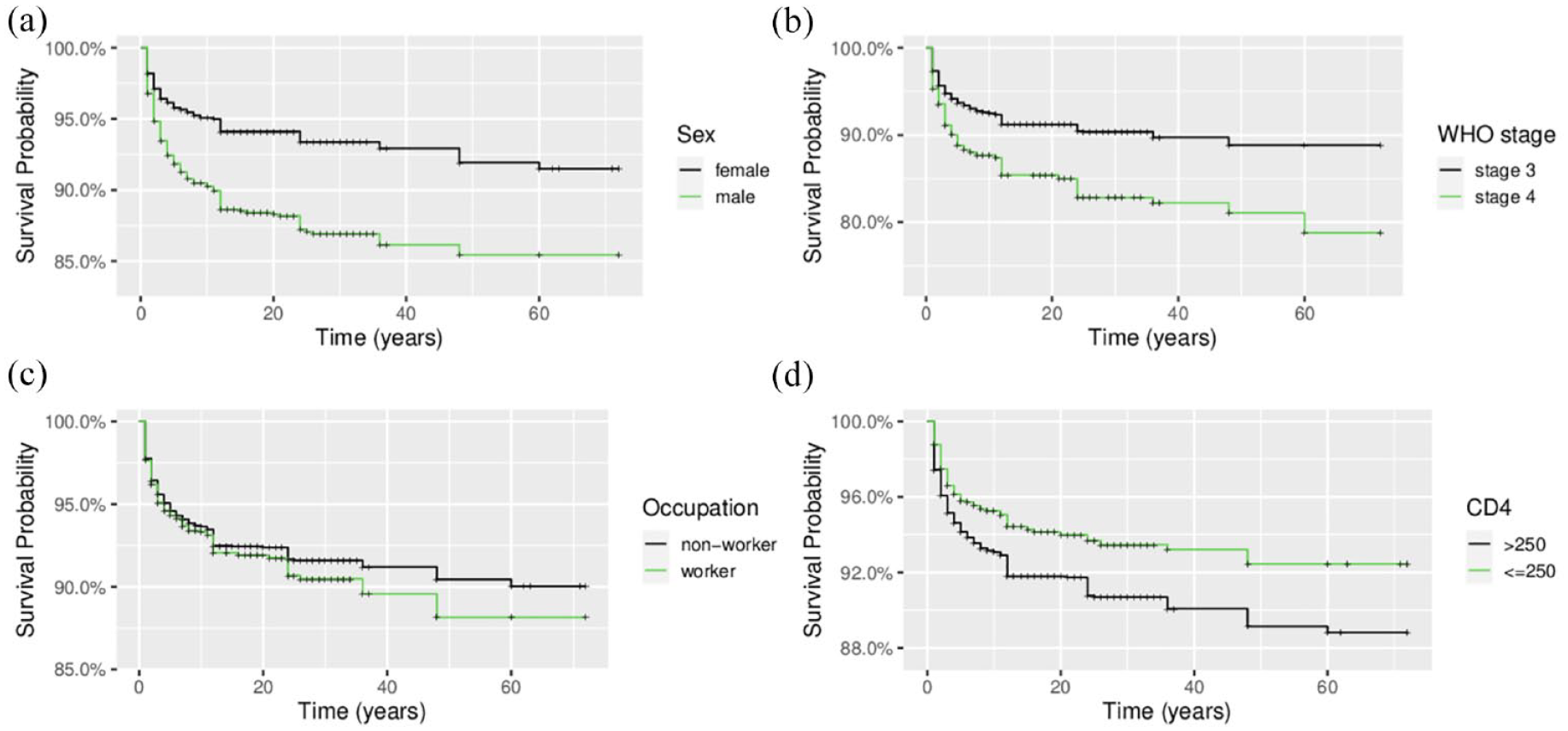
Kaplan-Meier survival curves comparing groups: (a) sex, (b) WHO clinical stages, (c) occupation, and (d) CD4 count.
Table 2 presents tests of significance in terms of equality of survival functions between groups using log-rank test. The results of the log-rank test show a significant difference in the survival of patients for the sex groups with a p-value of less than 0.001. WHO clinical stage 3 and 4 and CD4 count groups have also indicated significant difference in the survival of patients taking ART with a p-value of less than 0.001. However, occupation is found to be statistically insignificant as its p-value is 0.25 which is greater than 0.05. Therefore, there is insufficient evidence of a difference in the survival of patients between working and non-working patients taking ART Ntcheu district hospital in Malawi.
Log-rank test of equality of survival functions.

Before presenting results of the multiple variable survival model, the best fitting model is first selected using R2, Brier score, correlation between observed and fitted survival probabilities, and the Cox-Snell residuals plots. Table 3 presents correlation coefficient between the observed and the fitted survival probabilities, R2, and Brier score. The exponential model is seen to be the best model, since it has the highest R2 and correlation coefficient between the observed and predicted survival probabilities. The exponential model has also the smallest Brier score. The other good model is the Gompertz based on correlation of observed and predicted values and R2 (Table 3) and its Cox-Snell residuals plot (Figure 2(c)), where most of the points are close to 45° line. The Cox regression does not fare well based on Brier score and correlation between observed and predicted survival probabilities (Table 3), but may still be considered as just as good from the fact that it has a good R2 and that its Cox-Snell residuals plot (Figure 2(f)), has most of the points close to 45° line. Furthermore, its proportional hazard assumption is not violated (X2 = 3.29, p-value = 0.77).
Correlation, R2, and Brier score from the fitted models.


Cox-Snell residuals plots to check model goodness of fit: (a) exponential, (b) Weibull, (c) Gompertz, (d) log-logistic, (e) log-normal, and (f) Cox.
The results of multiple variable exponential survival model (Table 4) indicate that body mass index (HR = 0.82, p-value <0.001), WHO clinical stage 4 (HR = 1.69, p-value <0.001), and sex (HR = 1.74, p-value <0.001), significantly influence survival of HIV/AIDS patients. Age, occupation, and CD4 count are insignificant. From Table 4, the hazard ratio of males is greater than one, which means, males have an increased hazard of death than females. The hazard ratio of body mass index is less than one, which means, larger body mass is associated with reduced hazard of death compared to lower body mass. WHO clinical stage 4 hazard ratio of 1.69, means that the hazard of death for patients in WHO stage 4 is 69% higher than those in WHO clinical stage 3.
Multiple variable exponential model.

CI: confidence interval; HR: Hazard ratio; _: reference category.
Discussion
The study aimed at comparing survival models on the survival of HIV/AIDS infected patients at Ntcheu district hospital in Malawi. Five parametric models including the popular semi-parametric Cox regression were fitted to the data and compared. The results showed that parametric models may fit the data better than the popular Cox regression model as the exponential and Gompertz model fitted the data well, competing with the Cox regression. The Cox regression was just as good, particularly from the fact that its proportional hazard assumption was not violated, in addition to having a fairly good R2 and a close to 45° Cox-Snell residuals plot. The different measures of model fit are usually based on certain assumptions and how well the model fitted values suit the observed. For example, the Brier score and the correlation coefficient between the observed and predicted values, measure the closeness of the predicted and the observed values. The R2 measures how well the independent variables explain the outcome. The Cox regression did not perform well on prediction since it had the highest Brier score and smaller correlation between expected and observed values. The poor performance of the Cox regression on predicting survival probabilities is expected because Cox regression is not good at predicting absolute risk or survival as the base line hazard is not estimated. 27 Cox regression is mainly used for prognostic purposes, that is, describing correlation of the independent variables and the outcome through the use of the estimated hazard ratios. In practice, it is recommended that Cox regression is fitted in combination with some parametric models as a means of validating results from Cox regression.
Based on the results from exponential model, it is found that men have a higher risk of death than females. This is in agreement with previous research.23,28 However, other previous studies found the opposite, where females had poor survival than males. 29 According to Akbari et al. 28 the observed males’ poor survival than females may be explained by the fact they come to the hospital with advanced disease due to delayed access of medical care. Furthermore, males tend to not comply with medical treatment given to them. 24 Other previous studies have reported the same that late reporting by men for health care and treatment causes them to experience a higher risk of death than their women counterparts.30,31
The findings from this study also show that WHO clinical stage 4 is a significant predictor of HIV/AIDS related mortality. It is observed from the study that most of HIV/AIDS patients in Ntcheu district who were dying, were the ones who developed diseases like Kaposi sarcoma (skin cancer), bacterial pneumonia, and wasting syndrome (severe malnutrition), among others. These complications are what define WHO clinical stage 4.
32
This finding from the study is consistent with previous studies.33,34 Other studies though, have shown that WHO clinical stage 4 is not associated with mortality,
35
and in this case, the insignificant effect of WHO clinical stage 4 on HIV related mortality is assumed to be attributed to the fact that the majority of patients usually may have good ART adherence and may start early at WHO clinical stage 1 and 2. The study has also shown that HIV/AIDS patients with body mass index >16 kg/m2 are associated with decreased hazard of death. Other previous studies found similar results, where patients with body mass index <16 kg/m2 at ART initiation, had a mortality rate double that of patients with body mass index ≥
The limitation in this study was that data had missing information. For example, a good number of patients had their CD4 cell count not recorded. Furthermore, it was very difficult to trace the patients who were transferred out as to whether they were alive or not, or were still on ART or had defaulted. Their outcomes after the study were not known. The study has only looked at HIV/AIDS patients of 15 years of age and above and there was no information for HIV/AIDS patients below 15 years of age on their survival. In addition, calculation and justification of the selected sample size for the study was not done, that is, it was based on the available samples in the defined study period. Furthermore, some independent variables such as education status, marital status, and ART adherence were not taken into account due to the absence of information on patients registers. Regardless of these weaknesses, the study results are consistent with previous research and hence still usable.
Conclusions
The study aimed at comparing parametric survival models with the popular semi-parametric Cox regression among HIV/AIDS infected patients receiving ART at Ntcheu district hospital in Malawi. The exponential and Gompertz model fitted the data better based on correlation of observed and fitted survival probabilities. The Cox regression was just as good based on the Cox-Snell residuals plot and the validity of proportional hazard assumption. Thus, plausibility of all models needs to be investigated so as to use the correct model for accurate inferences. WHO clinical stage 4 and male sex were significantly associated with increased hazard of death, while increased body mass index was found to be significantly associated with decreased hazard of death. Strategies to reduce deaths due to HIV/AIDS, should aim at starting ART early before patients progress to WHO clinical stage 4 and special attention should be paid to men. Furthermore, nutritional interventions should aim at improving the body mass index of HIV/AIDS patients so as to limit deaths due to HIV/AIDS.
Footnotes
Acknowledgements
We thank the Malawi Ministry of Health through the Ntcheu District Health Officer for allowing us to use the data from the patients’ health registers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because the study used secondary data and that the data was analyzed anonymously without using patients’ names. Permission to use the data was granted by the District Health Officer of Ntcheu district.