
Abstract
Background:
Due to the high prevalence of hepatic steatosis (HS), the aim of the study is to verify the frequency of HS incidentally detected in chest computed tomography (CT) imaging in our population affected by SARS-CoV-2 and to investigate its association with the severity of the infection and outcome in terms of hospitalization.
Design and methods:
We retrospectively analyzed 500 patients with flu syndrome and clinically suspected of having Sars-CoV-2 infection who underwent unenhanced chest CT and have positive RT-PCR tests for Sars-CoV-2 RNA. Two radiologists both with >5 years of thoracic imaging experience, evaluated the images in consensus, without knowing the RT-PCR results. Liver density was measured by a region of interest (ROI), using a liver attenuation value ≤40 Hounsfield units (HU).
Results:
On 480 patients, 23.1% (111/480) had an incidental findings of HS on chest CT. The steatosis group, included 83 (74.7%) males and 28 (25.3%) females. Patients with HS were more likely to be hospitalized in the intensive care unit (ICU). On univariate analysis, there is a correlation between probability to be intubate (access in the ICU) and HS: patients with HS are twice as likely to be intubated (OR 2.04, CI 95% 1.11–3.73).
Conclusion:
Chest CT is an important diagnostic tool for COVID-19 and can provide information about the prognosis of the disease. HS can easily be detected on chest CT taken for the diagnosis of the COVID-19 disease, is an important sign for a poor prognosis and possible predictor of admission in ICU.
Introduction
Coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) first appeared in Wuhan, China in December 2019. The World Health Organization declared it pandemic in March 2020.1–3 SARS-CoV-2 is typically associated with fever, dry cough, anosmia, fatigue, headache and can progress to respiratory failure. 4 The prevalence of abdominal pain, diarrhea, nausea, and vomiting is about 17%, and these manifestations are more frequent in hospitalized patients.5,6 Risk factors associated with major incidence of severe illness and mortality among patients with severe COVID-19 are cardiovascular diseases, type 2 diabetes mellitus (DM), hypertension (HT), chronic obstructive pulmonary disease (COPD), obesity and metabolic syndrome.7–11 About 30% of the population is affected by fatty liver disease and metabolic dysfunction (including HS and overweight)12–15 and patients with type 2 DM and obesity, have higher risk for Metabolic Associated Fatty Liver Disease (MAFLD). Patients with MAFLD frequently have elevated abnormal liver tests at admission to discharge and longer viral shedding time. 16 A recent systematic review concludes that MAFLD is associated with a higher risk of symptomatic, and severe COVID-19. 17 A meta-analysis has confirmed that MAFLD increased the risk of disease progression among patients with COVID-19. 18 Non-enhanced CT, has a key role in the management of COVID-19,19,20 as has been shown in our previous study about correlation between chest CT accuracy and RT-PCR. 21 It is also an accurate non-invasive method for quantifying the liver fat. 22 Due to the high prevalence of HS and its relationship with many disorders associated with higher risk of COVID-19 infection, the aim of the study is to verify the frequency of HS incidentally detected in chest CT imaging in our population affected by SARS-CoV-2 and to investigate its association with the severity of the infection and outcome in terms of hospitalization.
Design and methods
Patient population and study design
This retrospective study was approved by the Institute Research Medical Ethics Committee at AOU Maggiore della Carità, Novara, Italy; protocol number CE 123/20.
We analyzed a cohort of 500 patients from March 7th to April 28th 2020 and from October 15th 2020 to February 19th 2021. Were included patients clinically suspected for Sars-CoV-2 infection (with temperature >37.5°C, cough, dyspnea) who underwent RT-PCR test for Sars-CoV-2 RNA and unenhanced chest CT.
CT acquisition technique and images analysis
CT examinations were performed in the emergency department (ED) CT room, in supine position, during single full inspiratory breath hold on a 128-slice CT (Philips Ingenuity Core, Philips Healthcare, Netherlands). Tube voltage: 120 kV; tube current modulation: 226 mAs; spiral pitch factor: 1.08; collimation width 0.625, matrix 512 (mediastinal window) and 768 (lung window). Images were reconstructed with a slice thickness of 1 mm.
Images were evaluated by two radiologists both with >5 years of experience in thoracic and abdominal imaging, who were blindly to RT-PCR results, clinical and laboratory data. STR/ACR/RSNA consensus statement 20 was employed for lung CT images and the radiographic features include: ground-glass opacities (GGOs), consolidation, crazy paving, reversed halo-sign, bilateral distribution, lymphadenopathy, pleural or pericardial effusion, according by Chung et al. 23 (Figure 1).

Chest CT images of patients with COVID-19 pneumonia (coronal view), with bilateral patchy areas of GGO.
For this study, liver density was measured by the HU of a 90 mm2 circular ROI in four different areas of both lobes, each separated by the hepatic veins, avoiding vessels, biliary tree or focal lesions and using a liver attenuation value ≤40 HU (Figure 2).

Demonstration of ROI positioning and measurement—with an area of approximately 90 mm2—in the right and left liver lobes.
Clinical data
Parameters as respiration frequency (FR), blood pressure, oxygen saturation (SpO2) and blood tests as white blood cell count (WBC), lymphocyte count (LC), platelet count (PLT), lactate dehydrogenase (LDH), alanine aminotransferase (ALT), and blood glucose (BG) were recorded. Significant comorbidities were verified for each patient: HT, DM, coronary artery disease, COPD, non-COPD lung disease, neurological disorders, neoplastic diseases, chronic kidney disease (CKD), hepatic failure. Whether the patients were hospitalized or deferred for home treatment was documented. When hospitalization was necessary, invasive or non-invasive high-flow ventilation use in the ICU or hospitalization on a general ward with non-invasive low-flow ventilation was recorded. Date of the discharge or of the demise were recorded.
Statistical analysis
All analyses were performed with the use of STATA, version 15.0.
Continuous variables were reported as mean ± standard deviation; categorical variables were expressed as counts and percentages. The distribution of continuous variables within the groups was evaluated by the unpaired t-test (two groups) or by the analysis of variance (ANOVA) model with Bonferroni’s correction (more than two groups). Chi-squared tests or Fisher’s exact test were used to compare categorical variables, as appropriate. Each variable predictive of the outcome was analyzed with univariate logistic regression. The variables selected (p < 0.10) by every univariate analysis were entered into a logistic regression model with the use of a forward stepwise elimination algorithm (terms with p > 0.05 were eligible for removal). A two-sided alpha of <0.05 was considered statistically significant.
Results
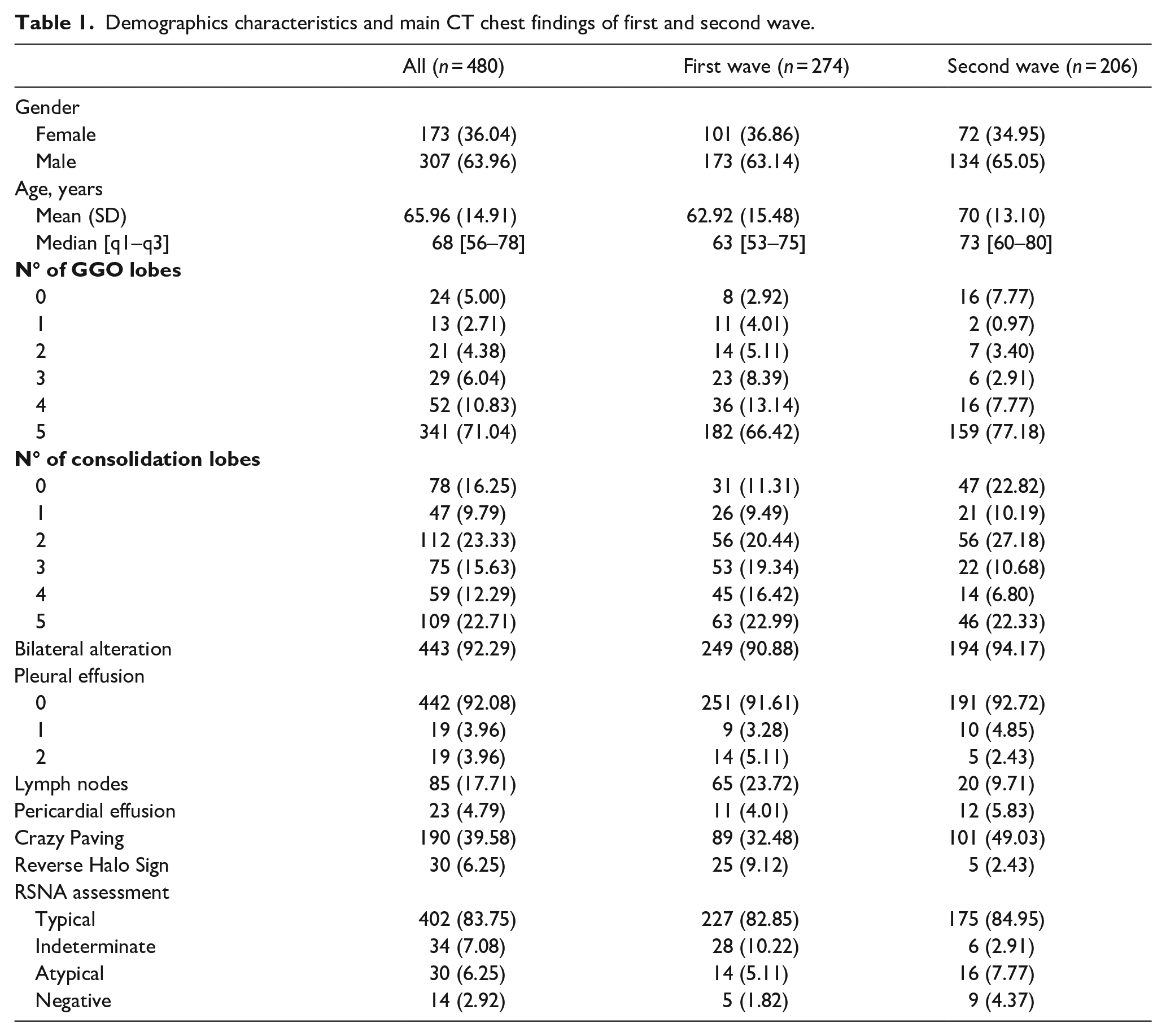
Our original population included 500 patients who underwent chest CT in our ED due to suspected COVID-19 and had a positive RT-PCR. Twenty patients were excluded because of severe motion artifacts. A total of 480 patients, recorded from April to March 2020 (first wave) and from October 2020 to February 2021 (second wave), were available for analysis. The mean age of the study population was 65.9 years ± 14.9, and 307 (64%) were male and 101 (36%) were females. The first wave included 173 (64%) males and 101 (36%) females, for a total of 274. The mean age population was 62.9 years (±15.4). The second wave included 134 (65%) males and 72 (35%) females, for a total of 206. The mean age population was 70 years (±13.1) (Table 1). Chest CT findings were reported in Table 1. In first and second wave, the main findings were GGOs in five lung lobes (66.4% [182/274] and 77.1% [159/206] respectively) and bilateral lung injury (90.8% [249/274] and 94.1% [194/206] respectively). 402/480 (82%) patients of study population had a “typical appearance,” based on STR/ACR/RSNA consensus statement (82.8% [227/274] and 84.9% [175/206]) in the first and second wave, respectively. In this population, 11% (53/480) was admitted in the ICU. On 480 patients, 23.1% (111/480) had an incidental findings of HS on chest CT. The steatosis group, included 83 (74.7%) males and 28 (25.3%) females. The mean age population was 70 years (±56.8). The no-steatosis group included 224 (60.7%) males and 145 (39.3%) females, for a total of 369. The mean age population was 66.9 years (±15.6). An analysis of this groups, showed a statistically significant difference (p = 0.006) between males and females. In particular, males were more likely to have HS. On chest CT findings was found a statistically significant difference, in particular for GGOs (p = 0.007): patients with HS had a major number of lung lobes with GGOs findings and “typical appearance,” based on STR/ACR/RSNA consensus statement (p = 0.003) (Table 2). An analysis of the different comorbidities between the two groups was performed. The most common comorbidities were HT, which affected 46.6% of study participants (47.7% and 46.3% respectively for steatosis and no steatosis group) and DM (17% of total patients, 22.5% and 15.4% for steatosis and no steatosis group) but no statistically relevant difference was found for the two population (Table 3). The clinical data recorded were categorized in Table 4: the analysis has demonstrated a significant different between the two groups for the sPO2 that is most under threshold (p = 0.006) and higher respiratory rate (p = 0.015) in the steatosis group. Regarding the required level of treatment, there was a significant difference: patients with HS were more likely to be hospitalized in the ICU. On univariate analysis, there is a correlation between probability to be intubate (access in the ICU) and HS: in this case, patients with HS are twice as likely to be intubated (OR 2.04, CI 95% 1.11–3.73); however, on multivariate analysis considering continues variable as sex, age and comorbidities, HS has no statistical relevance: probably may have reached significance in a larger cohort. The male population has twice as likely to be intubated (OR 2.4 CI 95% 1.16–4.95), with statistical relevance.
Demographics characteristics and main CT chest findings of first and second wave.
Demographics characteristics and main CT chest findings of no-steatosis and steatosis groups.

Data are patients with percentage in parentheses. Age is mean ± standard deviation. Time interval is shown as median.
RSNA: Radiological Society of North America.
Analysis of comorbidities between no-steatosis and steatosis groups.
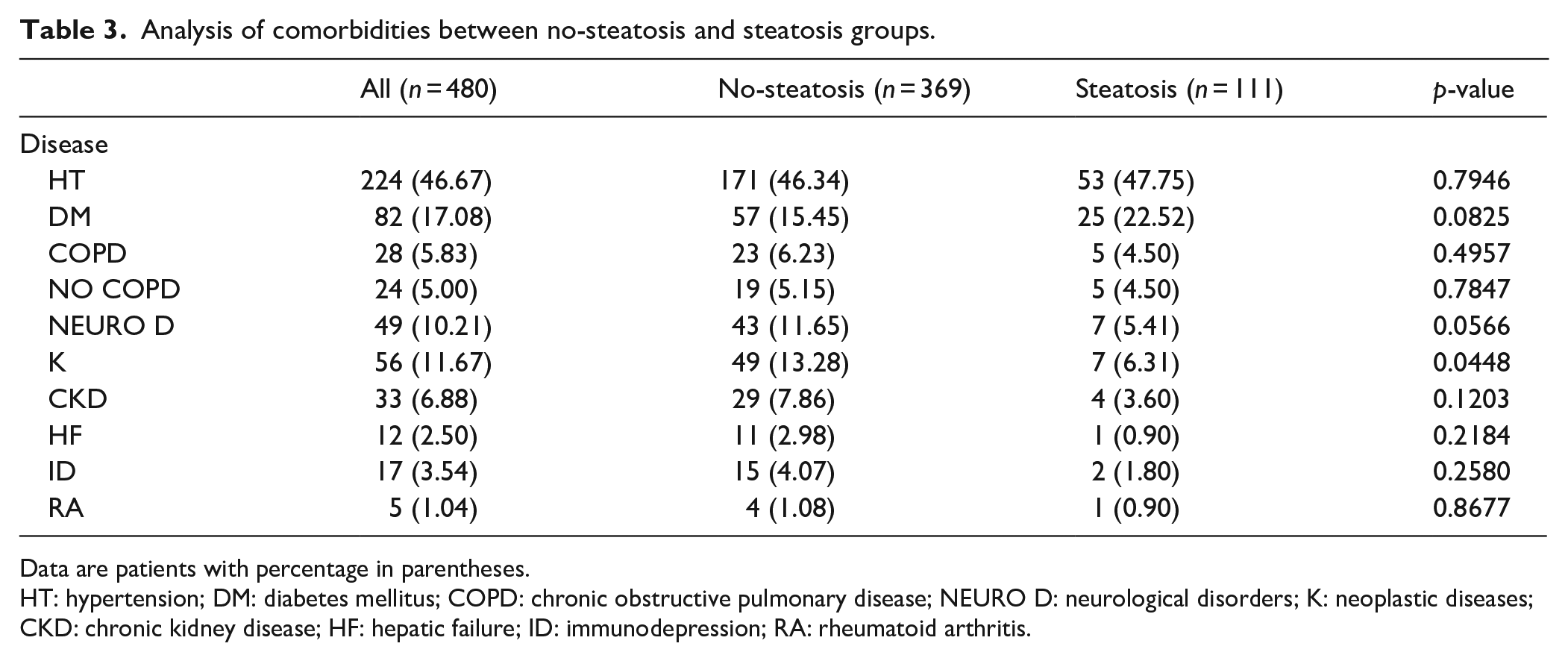
Data are patients with percentage in parentheses.
HT: hypertension; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; NEURO D: neurological disorders; K: neoplastic diseases; CKD: chronic kidney disease; HF: hepatic failure; ID: immunodepression; RA: rheumatoid arthritis.
Analysis of clinical data between no-steatosis and steatosis groups.

Data are patients with percentage in parentheses.
WBC: white blood cell count; NC: neutrophil count; LC: lymphocyte count; PLTs: platelet count; LDH: lactate dehydrogenase; AST: aspartate aminotransferase; ALT: alanine aminotransferase; BG: blood glucose; SBP systolic blood pressure; DBP: diastolic blood pressure; SpO2: oxygen saturation; RF: respiration frequency.
Conclusions
This study suggests a possible association of incidental HS on CT and SARS-CoV-2 infection, with a higher frequency of this liver disorder among male patients. In our demographic analysis we found a predominance of males with COVID-19 in both groups (steatosis and no steatosis). This corroborates with the profile found in a study published in Wuhan, China, were 56% of the cases were male individuals. 24 It is hypothesized that the adipose tissue may amplify the pro-inflammatory response to viral infection owing to different mechanisms.25,26 The incidence of liver injury in COVID-19 patients ranges from 14% to 53% and in severe cases have a significantly higher rate. 27 Our results showed a relationship between pulmonary findings and fatty liver. Thus the important relation between HS and metabolic syndrome, our results are in keeping with other prior analysis. Patients with a body mass index (BMI) ≥35 have a greater risk for hospital admission in the acute care. 28 In another study, patients with MAFLD have an increased likelihood of severe forms of COVID-19. 29 Also Medeiros et al., 30 in our retrospective analysis found significantly higher prevalence of HS among COVID-19 positive individuals and they used CT for diagnoses of HS. Severe imaging findings were found in patients with liver injury and it was significantly higher in the ICU patients than in the non-ICU patients.31,32 The progression to severe disease and worse outcomes in COVID-19 was higher in patients with NAFLD.33,34 Zhou et al. found that the risk of severe COVID-19 increases fourfold by the coexistence of metabolic associated fatty liver disease. 35 In our analysis the males reveal a major risk of admission in the ICU. These data are also confirmatory of a previous study by Percivale et al. 36 were females required a lower rate of admission to the ICU, and were more likely to be immediately deferred home after ED access. Pre-existing comorbidities are described as additional risks to progression of COVID-19 37 : in the current study, they not contributed to ICU admissions. An increased number of affected lobes, and diffuse infiltrations in the form of consolidation were detected in steatosis and no-steatosis group, thus corroborates that HS was significantly higher among the ICU patients. In according with Saudi et al. concluded that liver density was significantly lower in the ICU patients. The prevalence of severe disease was higher in the patients with HS than in the non-steatotic group (odds ratio [OR] 3.815, 95% confidence interval [CI] 1.97–7.37, p < 0.001). 38
Our study has several limitations. We have not assessed important variables (obesity, weight, height, body mass index, lipid profile), not available in our patient’s cohort (evaluated in ED); therefore, we could not establish correlations between such variables and HS. While previous studies have assessed the relationship between obesity and hospitalization or mortality due to COVID-19, we evaluated only the association between diagnosis of COVID-19 and presence of HS: further studies should be designed to answer if an association exists between HS and mortality. No liver histology was available to compare with CT findings, once CT sensitivity rises to 93% for detecting steatosis involving greater than 33% of the liver, probably we can have a bias underestimating the diagnosis of mild steatosis. Another limitation is the retrospective nature of the study. Lastly, the CT scans of all patients could not be performed on the same symptomatic day because they presented autonomously to the ED, with the consequent impossibility to collect the time interval between the onset of the clinical signs and the chest CT in the majority of cases.
In conclusion, chest CT is an important diagnostic tool for COVID-19 and can provide information about the prognosis of the disease. HS can easily be detected on chest CT taken for the diagnosis of the COVID-19 disease, is an important sign for a poor prognosis and possible predictor of admission in ICU.
Footnotes
Abbreviation
HS: hepatic steatosis
CT: computed tomography
RT- PCR: Reverse transcriptase-polymerase chain reaction
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2
COVID-19: Coronavirus disease 2019
ROI: region of interest
HU: Hounsfield units
ICU: intensive care unit
OR: odds ratio
HT: hypertension
COPD: chronic obstructive pulmonary disease
DM: diabetes mellitus
MAFLD: metabolic fatty liver disease
NASH: nonalcoholic steatohepatitis
HCC: hepatocellular carcinoma
RNA: ribonucleic acid
ED: emergency department
kV: kilovolt
mAs: milli Ampere/sec
STR/ACR/RSNA: Radiological Society of North America
GGO: ground-glass opacities
FR: respiration frequency
SpO2: oxygen saturation
WBC: white blood cell count
LC: lymphocyte count
PLT: platelet count
LDH: lactate dehydrogenase
ALT: alanine aminotransferase
BG: blood glucose
CKD: chronic kidney disease
BMI: body mass index
Contribution
All authors have contributed significantly and that all authors agree with the content of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This retrospective study was approved by the Institute Research Medical Ethics Committee at AOU Maggiore della Carità, Novara, Italy; protocol number CE 123/20.
Patient consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from a legally authorized representatives for anonymized patient information to be published in this article.
Significance for public health
As soon as the Covid-19 epidemic struck the region of Piedmont in northern Italy we started collecting data about all the patients with suspected Sars-Cov-2 infection who performed a Chest CT in our institution.
In this paper, we aimed to evaluate the frequency of hepatic steatosis as incidentally detected in chest CT examinations of COVID-19 positive patients and the relations between steatosis and level of treatment required.
The subject overlaps with some previously published studies, validating them on a larger sample, showing a greater severity of Sars-cov2 disease in patients with occasional finding of hepatic steatosis on the chest CT and a correlation between steatosis and ICU admission.
We are convinced that the results obtained in this study can provide useful prognostic information in the management of patients affected by Covid-19, a central issue of Public Health.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.