
Abstract
Pre-eclampsia is one of the main causes of maternal mortality, premature birth and low birth weight in developing countries. In addition, this condition can lead to chronic diseases (including cardiovascular and renal diseases) in postpartum mothers. The purpose of this study was to review the effectiveness of psycho-educational counseling in pregnant women with preeclampsia. The methods of this study were using PRISMA guidelines, databases from Scopus, PubMed and ScienceDirect, were published 2016 until 2020, yielded 65 articles. The keywords were retrieved from Medical Subject Heading (Mesh). The results showed interventions were given during the treatment period ranges from cognitive-behavioral counseling group that received four 1.5-h counseling sessions and the solution-focused counseling that received three 1.5-h counseling sessions, which were held weekly. This systematic review concludes that improving prenatal empowerment and self-care enable mothers to experience fewer complications in this period of their life. Thus, psycho-educational provides an excellent opportunity for educating and counseling pregnant women to promote maternal and neonatal health and psychological well-being.
Introduction
Pre-eclampsia is one of the most common conditions in pregnancy that can occur in women with normal blood pressure or chronic hypertension from the 20th week of pregnancy. 1 It is estimated that around 76,000 women and 500,000 babies die each year due to high blood pressure disorders due to preeclampsia. 2 Studies have shown that pre-eclampsia is one of the main causes of maternal mortality, premature births and low birth weights in developing countries. 1 In addition, this condition can lead to chronic diseases (including cardiovascular and renal diseases) in mothers after childbirth. 2 Early diagnosis of the signs and symptoms of this condition can prevent many of its effects and complications. 3
Lifestyle counseling, to promote regular exercise and a healthy diet, is recommended as self-care therapy for reducing blood pressure (BP), especially pre-eclampsia. 4 Studies have shown that lack of knowledge and awareness about disease increases poor outcomes. 5 For example, in a study among patients with pre eclampsia, showed that early recognition of signs and symptoms of pre-eclampsia can improve health outcomes, such as premature delivery and neonatal mortality. Because they received the necessary care at the right time.6,7
Pregnant women with preeclampsia often present more health complaints compared to those with uncomplicated pregnancies, and they may suffer from both psychological and physical problems. 8 Taking care of women with risk factors for decreasing health as well as counseling and referring them to more advanced diagnosis and treatments can improve their quality of life and reduce maternal and fetal outcomes and mortality. 9 Considering the effects of anxiety on mother and fetus, especially in pregnant women with preeclampsia, this study aimed to review the effectiveness of psycho-educational counseling in pregnant women with preeclampsia. It is expected that the intervention will decrease anxiety levels in the sample and consequently improve pregnancy outcomes and the mothers’ quality of life.
Methods
Data resource
Fifteen studies were included in this systematic review. Scopus, PubMed, and Science Direct were used as online databases for the primary search strategy in order to identified articles. The full search strategy was adapted with using terms and medical subject headings (MeSH) combined with Boolean operators. The keywords used to search those journals were “pre-eclampsia” OR “preeclampsia” AND “counseling” OR “psycho-educational counseling” AND “maternal” OR “maternity.”
Study selection
The feasibility of the study was assessed using the PICOT (Population, Intervention, Comparation, Outcome, and Time) framework. The inclusion criteria were (i) patient diagnosed with preeclampsia (ii) patient who had symptoms such as hypertension (iii) types of study: randomized controlled trials (RCT), case control study, quasy experiment, only articles published in English were included (iv) publication years; 2016 until 2020 (v) main outcome: to investigate the effectiveness of individual psycho-educational counseling in pregnant women with preeclampsia.
Data extraction
The following information was extracted from 14 articles: information on demographics, study design, outcome measure, sample size, intervention, control, pre-post intervention mean, country and year of publication from each study. Information was collected on relevant outcome data and included number of participants.
Quality assessment
This systematic review followed a preferred reporting items for systematic reviews (PRISMA) 10 (Figure 1) guidelines for the stages of design and results.

Flow chart of the study selection.
Risk of Bias
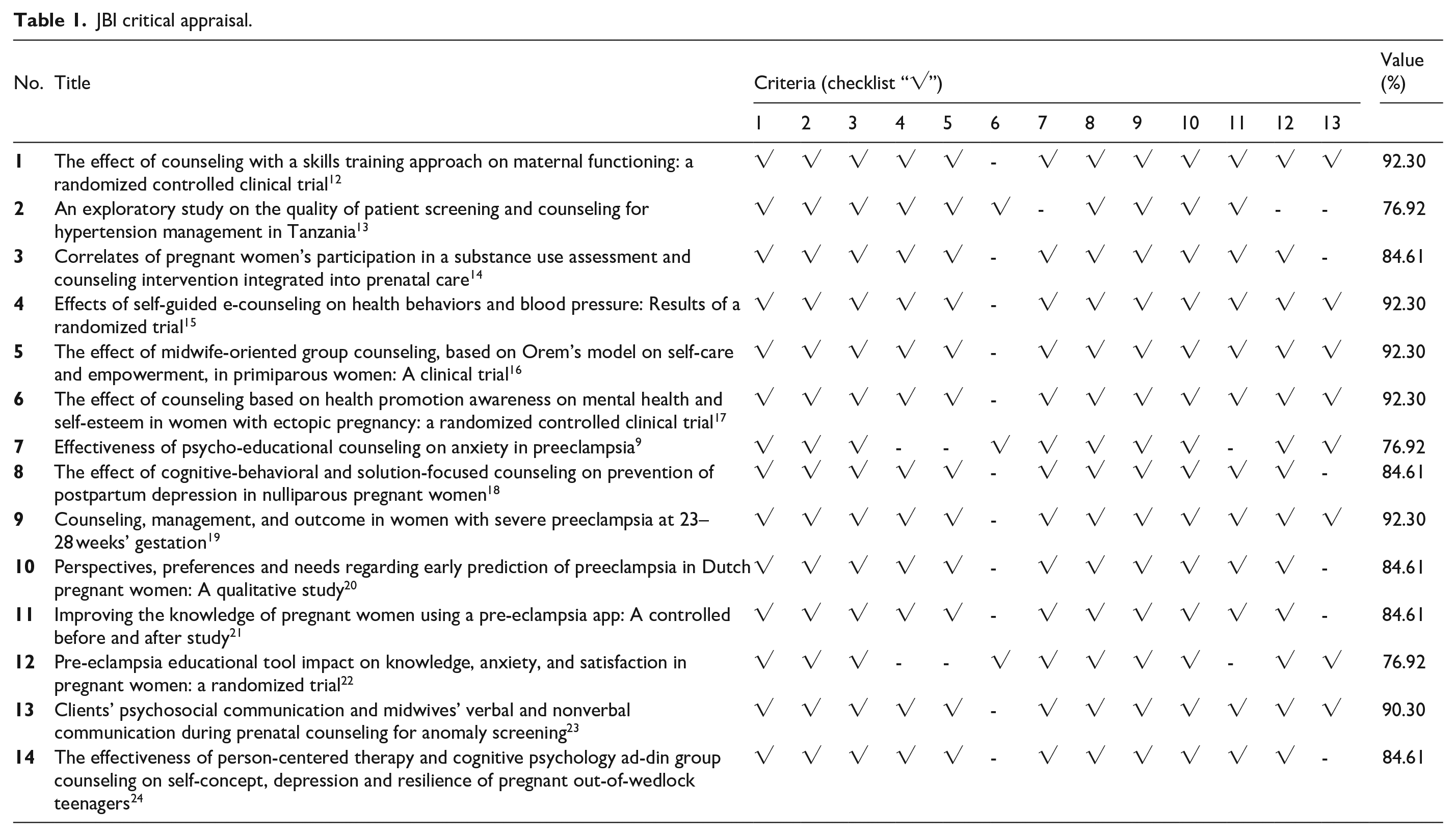
The risk of bias was measured using The JBI Critical Appraisal to assess the quality of each study. 11 Studies with RCT research designs were assessed using the JBI Critical Appraisal Checklist. The checklist consists of some questions with answers to “yes,” “no,” “unclear” and “not valid.” An assessment score that reaches a minimum of 50% then meets the critical appraisal with the cut-off point value agreed upon by the researcher. We did not include studies with scores below 50% to avoid bias in results and discussion. The JBI scores for each journal in this review >50% (Table 1).
JBI critical appraisal.
Related studies results (n = 14).

Results
Three steps strategy were used to the initial phase of literature search in three databases with the specified keywords then obtained a number of 65 articles. It is consisted of 21 articles from Scopus, 5 articles from PubMed and 39 articles from Science Direct. Second step were reviewed the abstract who retrieved for eligible criteria. We exclude some articles with PICOT framework. At the end of the process, we included 14 studies which is consist of eight studies were randomized controlled trial, one true experiment, four pilot study and the other one was a case control study (Table 2).
Population
Almost all population characteristic in the study included were patients who had symptoms such as pregnant women with preeclampsia, gestational age ≥20 weeks, and low risk pregnancy. The total sample in this study was 907 patients, with sample sizes varied from 8 to 186 patients. Demographic characteristics included maternal age, education level, occupation, number of pregnancies, number of deliveries, abortion, age of pregnant woman, intended pregnancy and emotional relationships with husband. Several studies explained that bio-demographic data from all participants showed differences in homogeneity and were not significant between the two groups in terms of age, weight, height and body mass index.
Intervention
The cognitive-behavioral counseling group received four 1.5-h counseling sessions and the solution-focused counseling received three 1.5-h counseling sessions, which were held weekly. The control group received no counseling and only routine pregnancy healthcare services were provided for them. The routine pregnancy care consists of prenatal care such as control of blood pressure, weight, fundal height measures, auscultation of fetal heart rate and laboratory test. The intervention groups also received the routine pregnancy healthcare services in addition to the designed interventions. At the start of the meetings, demographic, and obstetric history questionnaires were completed for the participants. The structure of interventions and counseling sessions were reviewed and approved by the supervisors of the study.
Discussion
Preeclampsia, as an emergency event that affects 1.2%–27% of pregnancies, is an important stressor in nulliparous as well as multiparous women. 9 The main purpose of this research was to review the effects of psycho- educational counseling in pregnant women with preeclampsia. The primary objective in the management of women with a history of preeclampsia is to reduce the risk factors for recurrence, therefore it is imperative that maternal health be optimized before conception. 19 In previous study had found ideally counseling of patients with a history of SPE should begin preconceptually; however, because late entry into prenatal care may occur, these recommendations can be given at the 6 weeks postpartum visit. Recommendations should include risk modification strategies to reduce SPE recurrence. 13 For example, preeclampsia is correlated with the severity of maternal hypertension, glycemic control, and obesity, so tight control of blood pressures along with lifestyle modifications should be attempted before conception.13,24 Early and frequent prenatal visits are imperative for successful pregnancy outcome in women with prior SPE, so we recommend that this should be emphasized during the counseling visits.17,19 Other study evaluated the effectiveness of a self-guided e-counseling program (REACH) designed to promote self-care behavior for hypertension management 15 The results of that study showed the REACH e-counseling protocol was effective in improving daily steps relative to control at 12-month follow-up.15,17
Other study found women with preeclampsia showed that cognitive- behavioral therapy, health education and mental nursing could significantly reduce the level of anxiety. 12 Relaxation training decreased the anxiety of pregnant women significantly, which is consistent with the present study. 9 The contents of psycho-educational counseling in this research were designed in such a way as to enhance the level of knowledge of pregnant women about the pathophysiology of their acute problem, to familiarize them with the therapeutic services offered, to reassure them about their own health and fetal health as well as to provide pre eclampsia becomes rarely complicated, to train problem-solving skills as well as anxiety management techniques, and patient’s appropriate justification to the problem. 22 The above mentioned acquired abilities and positive attitudes may reduce the level of anxiety and promote maternal mental health during pregnancy. 18 The positive effect of counseling on anxiety and depression has been reported in other studies. The present findings agree with the results of studies such as ones by Hasani et al. 17 examined the impact of supportive counseling on the 280 women who were diagnosed with abortion in China and reported that counseling had a significant impact on women’s mental health for 6 weeks and 3 months after the abortion. In the study of Abazarnejad et al. 9 who studied the effect of counseling on the anxiety level of 100 women with spontaneous abortions in Tehran reported that although the rate of anxiety over time in both groups was significantly decreased, 3 months after the intervention, women in the intervention group experienced less amount of anxiety.
One of the domains of maternal functioning is (maternal) psychological well-being. Given that drug interventions may come with unwanted side effects, and potentially stigma, non-pharmacological psychological interventions aimed at skill-building may be particularly useful; the Skills Training Approach fits this description. Based on the obtained results, and the results of several other studies, it can be concluded that counseling and skills training interventions, have the potential to play an important role in maternal functional improvement after delivery. 19 Therefore, we may have the ability to mitigate many mother and infant difficulties by enhancing maternal functioning through counseling with the skills training approach.9,18 Other study found counseling with STA (Skills Training Approach) resulted in improved maternal functioning in all domains. Mothers have vital and often multidimensional roles including spouse, mother, daughter, worker, and citizen. 17 As a result, they are faced with complex challenges, including infant feeding difficulties and sleep deprivation and require additional support in order to function optimally. 9
Conclusions
Improved prenatal empowerment and self-care enables mothers from experiencing fewer complications in this period of their life. Thus, educating and counseling is needed to promote maternal and neonatal health and psychological well-being
Footnotes
Acknowledgements
The author would like to thankful to the Faculty of Nursing, Universitas Airlangga for providing the opportunity to present this study.
Author contributions
The authors contributed equally. Conception and design:
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Universitas NU Surabaya, Surabaya, East Java, Indonesia.
Clinical trials
The study is not involved any clinical trial.
Significance for Public Health
Pregnant women with preeclampsia often present more health complaints compared to those with uncomplicated pregnancies, and they may suffer from both psychological and physical problems. Psycho-educational counseling in pregnant women with preeclampsia is needed to take care and improve their psychological and physical health. Psycho-educational counseling is included in prevention level of public health.