
Abstract
Objective:
To understand the interaction of multimorbidity and functional limitations in determining health-care utilization and survival in older adults.
Methods:
Olmsted County, Minnesota, residents aged 60–89 years in 2005 were categorized into four cohorts based on the presence or absence of multimorbidity (≥3 chronic conditions from a list of 18) and functional limitations (≥1 limitation in an activity of daily living from a list of 9), and were followed through December 31, 2016. Andersen–Gill and Cox regression estimated hazard ratios (HRs) for emergency department (ED) visits, hospitalizations, and death using persons with neither multimorbidity nor functional limitations as the reference (interaction analyses).
Results:
Among 13,145 persons, 34% had neither multimorbidity nor functional limitations, 44% had multimorbidity only, 4% had functional limitations only, and 18% had both. Over a median follow-up of 11 years, 5906 ED visits, 2654 hospitalizations, and 4559 deaths occurred. Synergistic interactions on an additive scale of multimorbidity and functional limitations were observed for all outcomes; however, the magnitude of the interactions decreased with advancing age. The HR (95% confidence interval) for death among persons with both multimorbidity and functional limitations was 5.34 (4.40–6.47) at age 60–69, 4.16 (3.59–4.83) at age 70–79, and 2.86 (2.45–3.35) at age 80–89 years.
Conclusion:
The risk of ED visits, hospitalizations, and death among persons with both multimorbidity and functional limitations is greater than additive. The magnitude of the interaction was strongest for the youngest age group, highlighting the importance of interventions to prevent and effectively manage multimorbidity and functional limitations early in life.
Keywords
Introduction
The number of persons aged 65 years and older in the United States is projected to increase twofold by the year 2050, representing 20% of the total population. 1 As a result of the aging population, along with advancements in life-prolonging medical care, an increased number of persons with multimorbidity and complex medical needs are expected, together with increased health-care utilization and expenditures. 1 –3 In the United States, 1% of adults account for more than 20% of health-care expenditures, and the top 5% of spenders account for 50% of all health-care expenditures. 4,5 The vast majority of high-cost patients have three or more chronic conditions, and nearly half of patients in the top 5% of annual medical expenditures have at least three chronic conditions as well as functional limitations. 6 Thus, an inevitable result of the aging population and advances in medical care is an increasing number of complex, high-cost patients who will contribute to escalating medical costs.
The population of complex, high-need patients is diverse, and there are different definitions of complex needs in the literature. 7,8 The Commonwealth Fund defines persons with high needs as those who have both multimorbidity (having three or more chronic diseases) and functional limitations (limitation in at least one basic or instrumental activity of daily living (ADL) affecting their ability to care for themselves or to perform routine daily tasks). 6 In the Medical Expenditure Panel Survey, the persons who meet the definition of high need 6 experienced higher rates of emergency department (ED) visits and hospitalizations, higher health-care spending, and higher out-of-pocket costs than those with multimorbidity but without functional limitations. 6 Therefore, we hypothesized that multimorbidity and functional limitations may have different underlying mechanisms, and that having both imparts a larger risk of adverse health outcomes than expected (synergistic interaction).
With increasing numbers of older, high-need patients, it is imperative to better understand the outcomes of high-need patients. However, only few data sets in the United States and worldwide contain information on patient-reported outcomes assessing functional limitations. As such, studies utilizing administrative claims data or electronic health records data are unable to provide this information. Therefore, the aim of our study was to describe the interaction of multimorbidity with functional limitations on health outcomes, including ED visits, hospitalizations, and death, in a large population of older adults.
Methods
Study population
This study was conducted using the Rochester Epidemiology Project (REP) medical records-linkage system. 9 –12 The REP captures all health-care information from the few providers who deliver most of the health care to the residents of Olmsted County, Minnesota, allowing virtually complete capture of residents’ health-care utilization and outcomes. Importantly, demographic characteristics of Olmsted County, Minnesota, are representative of the state of Minnesota and the Upper Midwest region of the United States, and age- and sex-specific mortality rates in Olmsted County are similar to national data, supporting the generalizability of findings from this population. 10 For the current study, we examined the 2005 residents of Olmsted County, Minnesota, aged 60–89 years who were alive as of January 1, 2006 (n = 16,267). We further restricted our sample to persons with available data on ADLs between 2004 and 2005 (n = 13,145; 81% of the total population). This study was approved by the Mayo Clinic and Olmsted Medical Center Institutional Review Boards.
Assessment of multimorbidity and ADLs
We retrieved diagnostic codes for 20 chronic conditions defined by the US Department of Health and Human Services as important for studies of multimorbidity. 13,14 However, less than 1% of the population had autism, hepatitis, or human immunodeficiency virus, so these conditions were excluded. Anxiety was added to the list, resulting in a total of 18 chronic conditions. The diagnostic codes used to define the 18 chronic conditions are provided in Supplementary Table 1. To reduce the possibility for false-positive or rule-out diagnoses, we required two occurrences of a code (either the same diagnostic code or two different diagnostic codes within the same code set) separated by more than 30 days and occurring between 2000 and 2005. Multimorbidity was defined as having 3 or more of the 18 chronic conditions.
We ascertained difficulty with at least one ADL using a questionnaire that was administered on at least a yearly basis to persons seen at one of the institutions that participates in the REP (Mayo Clinic). A total of nine ADLs, including both basic and instrumental ADLs, were ascertained by asking the person to select all of the activities which they had difficulty performing on their own from a list (see Table 1). For example, a person could have selected needing help with housekeeping or with climbing stairs. Only persons with at least one questionnaire between 2004 and 2005 were included, and when persons had multiple questionnaires available, we used the most complete questionnaire that was closest to January 1, 2006. Functional limitations was defined as reporting difficulty with one or more of the nine ADLs.
Demographic characteristics and chronic conditions in four cohorts defined by functional limitation and multimorbidity status.a

ADLs: activities of daily living.
a Values are presented as median (25th, 75th percentile) or N (%).
Using the framework from the Commonwealth Fund to identify high-need patients, 6 persons were categorized into four discrete cohorts based on the presence or absence of multimorbidity and functional limitations: (1) neither multimorbidity nor functional limitations, (2) multimorbidity but no functional limitations, (3) no multimorbidity but functional limitations, and (4) both multimorbidity and functional limitations.
Outcomes ascertainment
Hospitalizations and ED visits for any cause, and deaths from any cause were obtained from January 1, 2006 through December 31, 2016 from the REP. In-hospital transfers or transfers between hospitals were combined into a single encounter and were counted as a single hospitalization. However, ED visits that resulted in a hospitalization were counted as both an ED visit and a hospitalization.
Statistical analysis
For each of the four cohorts, demographic characteristics were reported as median (25th, 75th percentile) or number (percent), and the proportion of persons with each of the 18 comorbidities was also reported. Follow-up began on January 1, 2006 and continued until death, last clinical encounter, or December 31, 2016, whichever came first. Persons were stratified by decade of age on January 1, 2005 (60–69, 70–79, and 80–89 years), and the rates of each outcome per 1000 person-years were calculated, counting multiple events per person for ED visits and hospitalizations. For ED visits and hospitalizations, the mean cumulative functions over follow-up for the four cohorts were plotted using a nonparametric estimator. 15 The basis for this function is that each person can be represented by a stepwise curve of cumulative number of ED visits or hospitalizations over follow-up; thus, this function is appropriate to use when there may be multiple recurrent events per person. The mean cumulative function is the pointwise average of all the individual cumulative measurement curves. In addition, Kaplan–Meier plots were constructed to visualize survival over follow-up for the four cohorts. The mean cumulative function and Kaplan–Meier plots are crude representations of differences between groups, and were not adjusted for differences in patient characteristics between the four cohorts.
Andersen–Gill modeling, which allows for multiple repeated outcome events, was used to estimate hazard ratios (HRs) of ED visits and hospitalizations, while Cox proportional hazards regression was used to estimate HRs for death. Persons with neither multimorbidity nor functional limitations served as the reference group for the Andersen–Gill and Cox models. The HRs were adjusted for age (to account for residual confounding), sex, race (White, Black, Asian, other), ethnicity (Hispanic, non-Hispanic), education (less than high school, high school or some college, college or advanced degree), and marital status (married or living together, non-married). Additive interactions between multimorbidity and functional limitations were tested using the relative risk due to the interaction (RERI) statistic as described by Li and Chambless. 16 The RERI is calculated as HR12 − HR1 − HR2 + 1, where HR12 is the HR for those with both multimorbidity and functional limitations versus those with neither, HR1 is the HR for those with multimorbidity only versus those with neither, and HR2 is the HR for those with functional limitations only versus those with neither multimorbidity nor functional limitations. This statistic tested whether the observed joint effects of multimorbidity and functional limitations on each outcome were greater than expected assuming independence. Analyses were performed using SAS statistical software, version 9.4 (SAS Institute Inc., Cary, North Carolina, USA).
Results
A total of 13,145 Olmsted County residents aged 60–89 in 2005 had available ADL data and were included in the analyses (81% of the population enumerated by the REP). Persons included in the analyses were slightly older (median age 71 vs. 68; p < 0.001), more likely to be female (56% vs. 51%; p < 0.001), more highly educated (34% vs. 26% with a college or advanced degree; p < 0.001), had a higher prevalence of all of the 18 individual chronic conditions, and a higher number of chronic conditions (median number of chronic conditions 3 vs. 2; p < 0.001) compared to persons excluded.
The baseline characteristics of the four cohorts are shown in Table 1. The cohorts differed in demographic characteristics and in types of chronic conditions. Of the 13,145 persons in our study, 2323 (18%) had both functional limitations and multimorbidity. These persons were the oldest of the four cohorts, and were most similar to persons with functional limitations but no multimorbidity regarding sex, education level, and marital status. The majority of persons with both multimorbidity and functional limitations had between 3 and 7 chronic conditions (3, 18%; 4, 22%; 5, 18%; 6, 16%; and 7, 12%) and difficulty with 1 (40%), 2 (25%), or 3 (13%) ADLs. More than half of these persons had hypertension (85%), hyperlipidemia (67%), and arthritis (53%), and the most frequently reported ADL limitations were with climbing stairs (69%), walking (46%), and housekeeping (41%) (Table 1).
Over a median follow-up of 11 years, a total of 4559 deaths, 2654 hospitalizations, and 5906 ED visits occurred. The lowest survival and highest cumulative number of hospitalizations and ED visits were observed for persons with both multimorbidity and functional limitations, followed by persons with functional limitations only, multimorbidity only, and neither (who experienced the best survival and the lowest risk of ED visits and hospitalizations) (Figures 1 and 2). The median number of hospitalizations per person was 1 for persons aged 60–69 at baseline, 2 for persons aged 70–79, and 3 for persons aged 80–89 at baseline. The median number of ED visits per person was 2 for persons aged 60–69 and 4 for persons aged 70–79 and 80–89. Within each decade of age, the rates of death, hospitalizations, and ED visits were highest among persons with both functional limitations and multimorbidity (Table 2). As expected, the oldest persons had the highest rates of all outcomes, and persons aged 80–89 with functional limitations and multimorbidity had rates of 5.16 per 1000 person-years for death, 6.60 per 1000 person-years for hospitalizations, and 7.03 per 1000 person-years for ED visits.

Kaplan–Meier survival curves in four cohorts defined by functional limitation and multimorbidity status.

Mean cumulative hazard function curve for hospitalizations (top panel) and ED visits (bottom panel) in four cohorts defined by functional limitation and multimorbidity status. ED: emergency department.
Association of functional limitations and multimorbidity with death, hospitalizations, and ED visits.

MM: multimorbidity; FL: functional limitations; ED: emergency department; HR: hazard ratio; CI: confidence interval.
a Rates are presented per 1000 person-years.
b HRs were adjusted for age, sex, race, ethnicity, education, and marital status.
c p Values indicate the p value for the additive interaction.
After adjustment for age, sex, race, ethnicity, marital status, and education, the highest risks of death, hospitalization, and ED visits were observed in persons with both multimorbidity and functional limitations (Table 2, Figure 3). Persons with functional limitations only experienced higher risks of death than persons with multimorbidity only. However, for hospitalization and ED visits, similar associations were observed for persons with multimorbidity only and functional limitations only.
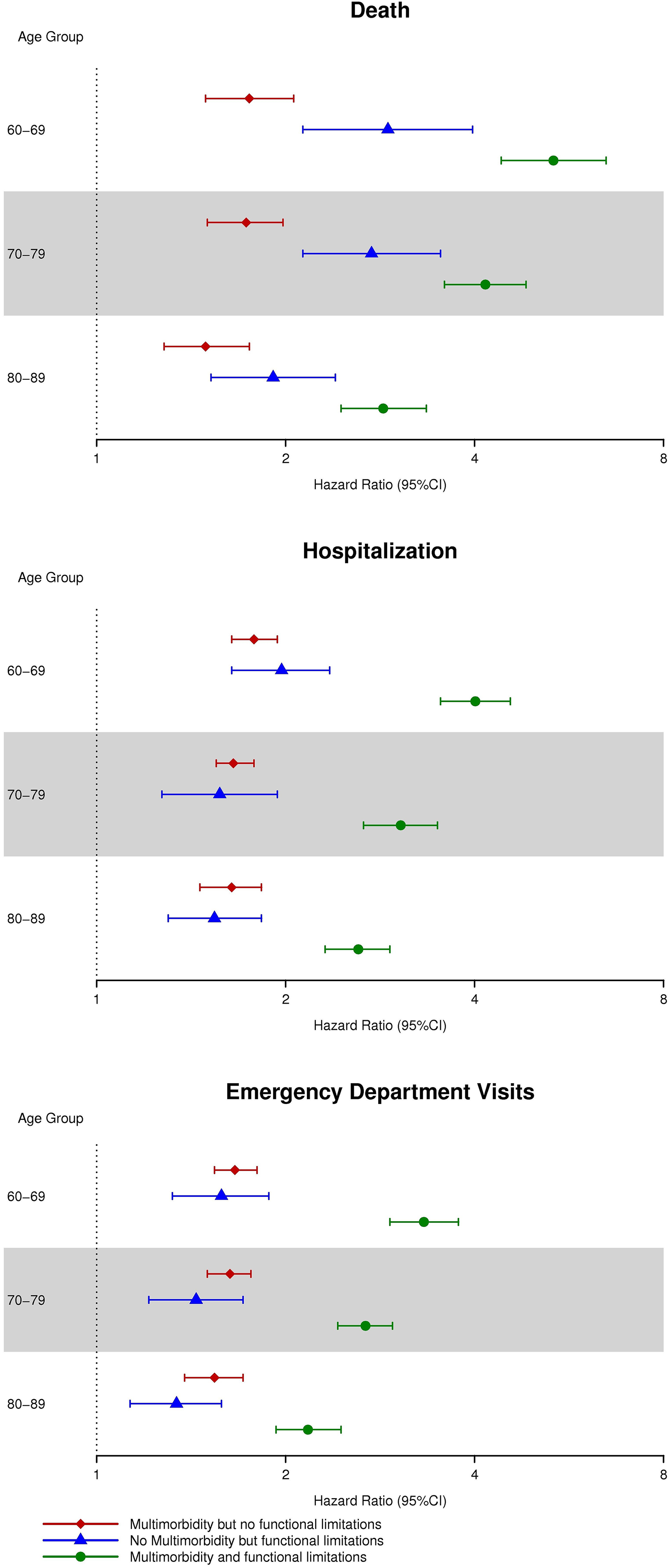
HRs (95% CIs) for death (top panel), hospitalization (middle panel), and ED visits (bottom panel) in four cohorts defined by functional limitation and multimorbidity status. The HRs for death were estimated from a Cox proportional hazards regression model, whereas the HRs for hospitalizations and ED visits were estimated using Andersen–Gill models. HRs were adjusted for age, sex, race, ethnicity, education, and marital status. The cohort of persons with neither multimorbidity nor functional limitations served as the referent cohort. CI: confidence interval.
Interactions between multimorbidity and functional limitations were tested on the additive scale for each outcome, and a synergistic effect of multimorbidity and functional limitations was observed for all outcomes. For death, the interaction was highly significant for persons aged 60–69 (p < 0.01) and borderline significant for persons aged 70–79 (p = 0.06) and 80–89 (p = 0.04). For hospitalizations and ED visits, the interactions between multimorbidity and functional limitations were highly significant for all age groups (p < 0.01). These findings suggest that the impact of both multimorbidity and functional limitations on outcomes is greater than would be expected assuming additivity of effects. Furthermore, for each outcome, a similar pattern of association was observed for each age group; however, the magnitude of the interactions was strongest in the youngest age group and attenuated with increasing age. For example, the HR (95% confidence interval) for death among persons with both functional limitations and multimorbidity was 5.34 (4.40–6.47) for persons aged 60–69, 4.16 (3.59–4.83) for persons aged 70–79, and 2.86 (2.45–3.35) for persons aged 80–89.
Discussion
In this large population of older adults, we observed an increased risk of ED visits, hospitalizations, and death among high-need patients (defined as persons with both multimorbidity and functional limitations). Few persons had functional limitations without multimorbidity, but these persons tended to have higher rates of death than persons with multimorbidity alone. For all outcomes, synergistic effects of multimorbidity and functional limitations were observed on an additive scale, whereby persons with both multimorbidity and functional limitations experienced greater-than-expected risks assuming additivity of effects. The patterns of association were similar for all age groups; however, the magnitude of the interaction was strongest for the youngest age group and attenuated with increasing age.
Persons with both multimorbidity and functional limitations experienced the poorest health-care outcomes, and multimorbidity and functional limitations acted synergistically for each outcome. Individually, both multimorbidity 17 –19 and functional limitations 20,21 have been shown to contribute to poor outcomes, including hospitalizations and death. Furthermore, frailty, which is a distinct clinical entity but overlaps with both multimorbidity and functional limitations, 22 is associated with increased risks of hospitalizations, ED visits, and death. 23 –27
In the Medical Expenditure Panel Survey, persons with both functional limitations and multimorbidity experienced higher rates of ED visits and hospitalizations compared to persons with multimorbidity alone, and compared to the total adult population; however, outcomes among persons with functional limitations only were not reported. 6 In another study of persons with heart failure, those with both non-cardiovascular multimorbidity and functional limitations experienced the greatest risk of ED visits and hospitalization; however, those with functional limitations alone and those with both multimorbidity and functional limitations experienced similar mortality. 28 However, to our knowledge, our study is the first to specifically examine interactions of multimorbidity and functional limitations on adverse health outcomes and test whether having both imparts a larger risk of outcomes than expected. In the general population of older adults, we observed a synergistic effect of multimorbidity and functional limitations for all outcomes and found that patients who have both multimorbidity and functional limitations had the highest risk of ED visits, hospitalizations, and death. The interactions were more extreme for ED visits and hospitalizations and less extreme for death. Interestingly, we observed that persons with functional limitations alone had a higher risk of death than persons with multimorbidity alone, which suggests that the risk of death is driven more by functional limitations than multimorbidity. By contrast, similar risks of ED visits and hospitalizations were observed for persons with multimorbidity alone and with functional limitations alone. Finally, for all outcomes, the magnitude of the interactions was strongest in the youngest age group and attenuated with increasing age. It has been postulated that aging results in a chronic dysregulation of multiple organ systems, and that multimorbidity is a landmark of loss of resilience and homeostasis. 29 Therefore, it can be hypothesized that having mutlimorbidity and functional limitations at younger ages is associated with accelerated aging, and results in poorer outcomes compared to persons who develop multimorbidity and functional limitations later in life. At advanced ages (e.g. 80–89 years), age itself is the major predictor of adverse health outcomes regardless of the number of chronic conditions or the number of functional limitations.
Implications of our findings
Because nearly half of the persons in the top 5% of annual medical expenditures have at least one functional limitation along with multimorbidity, 6 and this top 5% accounts for 50% of the annual health-care spending in the United States, 4,5 it is imperative to identify interventions to improve the care and outcomes for these high-need patients. Although nearly 90% of high-need patients in the United States report that they have a treatment plan, 30 the needs of these patients may extend beyond clinical needs alone. Thus, to improve the outcomes of these high-need patients, a shift to more broadly address the patients’ functional, social, and behavioral needs through social and community services in addition to traditional treatment plans may be required. 2,8 Furthermore, our results support the need for interventions to prevent the onset of multimorbidity and functional limitations at all ages, but particularly at younger ages.
Limitations and strengths
Our study has limitations that deserve mention. First, we relied on electronic ascertainment of chronic conditions, and because we did not validate the diagnoses, some patients may have been misclassified. However, we required two occurrences of a code (either the same diagnostic code or two different diagnostic codes within the same code set) separated by more than 30 days to minimize misclassification. We expect that any misclassification would not differ systematically between cohorts, and thus would not substantially affect our estimates. Second, we excluded patients who did not have available information on ADLs, which was nearly 20% of the population. The patients with missing ADL information tended to be younger and had fewer chronic conditions than those included in the analyses, and their exclusion could have biased our results. However, we expect that our results are most likely biased toward the null, and thus the estimates presented in our paper may be conservative. Third, the proportion of persons in our cohort with multimorbidity and functional limitations would have differed if we had used different cutoff points. For example, we used a list of 18 chronic conditions to define multimorbidity, and fewer patients would have been considered to have multimorbidity if a smaller number of chronic conditions had been used. Fourth, we did not consider severity of conditions or treatment for conditions when defining multimorbidity. Fifth, persons may have accumulated chronic conditions and functional limitations during follow-up, but we did not account for these intervening events in our results. Finally, our population was primarily White, and thus our results may not be generalizable to other populations with different racial or ethnic characteristics. However, comparison of the REP population to Census data revealed that this population is representative of the population of the Upper Midwest and of a large segment of the entire US population. 10
Our study also has several strengths, including the large sample size and the comprehensive capture of all health-care visits and outcomes in the population through the resources of the REP. 9 –12 In addition, the large data set allowed us to stratify patients into four cohorts and to study both individual and joint effects of multimorbidity and functional limitations on several adverse health outcomes. This design allowed us to show that functional limitations are more strongly associated with poor outcomes than multimorbidity.
Conclusion
In older adults, the risk of ED visits, hospitalizations, and death was highest among persons with both multimorbidity and functional limitations, underscoring the importance of incorporating both multimorbidity and functional limitations when stratifying patients to predict risk. Furthermore, although multimorbidity and functional limitations act synergistically on these outcomes, the magnitude of the interactions attenuated with increasing age. Therefore, interventions to prevent the onset of multimorbidity and functional limitations are warranted at all ages, but will be most impactful at younger ages.
Supplemental material
Supplementary_Table - Multimorbidity, functional limitations, and outcomes: Interactions in a population-based cohort of older adults
Supplementary_Table for Multimorbidity, functional limitations, and outcomes: Interactions in a population-based cohort of older adults by Alanna M Chamberlain, Lila J Finney Rutten, Debra J Jacobson, Chun Fan, Patrick M Wilson, Walter A Rocca, Véronique L Roger and Jennifer L St Sauver in Journal of Comorbidity
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, the National Institute on Aging (R01 AG052425), and was made possible using the resources of the Rochester Epidemiology Project, which is supported by the National Institute on Aging of the National Institutes of Health under Award Number R01 AG034676.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.