
Abstract
Background:
Multimorbidity is the co-occurrence of two or more diseases in the same individual. One method to identify this condition at an early stage is the use of specific markers for various combinations of morbidities. Nonetheless, evidence related to physiological markers in multimorbidity is limited.
Objective:
The aim was to perform a systematic review to identify physiological markers associated with multimorbidity.
Design:
Articles available on PubMed, Register of Controlled Trials, Academic Search Premier, CINAHL, Scopus, SocINDEX, Web of Science, LILACS, and SciELO, from their inception to May 2018, were systematically searched and reviewed. The project was registered in PROSPERO under the number CRD42017055522.
Results:
The systematic search identified 922 papers. After evaluation, 18 articles were included in the full review reporting at least one physiological marker in coexisting diseases or which are strongly associated with the presence of multimorbidity in the future. Only five of these studies examined multimorbidity in general, identifying five physiological markers associated with multimorbidity, namely, dehydroepiandrosterone sulfate (DHEAS), interleukin 6 (IL-6), C-reactive protein (CRP), lipoprotein (Lp), and cystatin C (Cyst-C).
Conclusions:
There is a paucity of studies related to physiological markers in multimorbidity. DHEAS, IL-6, CRP, Lp, and Cyst-C could be the initial focus for further investigation of physiological markers related to multimorbidity.
Introduction
Multimorbidity is the co-occurrence of two or more diseases in the same individual, which are often associated with each other. 1,2 It is more common in elderly, 3 and it affects one in five adults and two-thirds of the elderly. 4,5 Multimorbidity is more prevalent in groups from lower socioeconomic status. 4 Although studies about multimorbidity have recently begun, evidence has already shown that it leads to a decrease in quality of life, 6 functional decline, 7 and an increased risk of mortality, 8 in addition to difficulty to manage it adequately. Early diagnosis and management of multimorbidity may be important factors to minimize serious consequences. One method to identify this condition at an early stage is the use of specific physiological and molecular markers for various combinations of morbidities. 9
Some attempts have been made to identify physiological markers associated with multimorbidity. Reviews have evaluated markers that are associated with pairs of diseases. For example, high levels of B-type natriuretic peptide are commonly associated with dyspnea and have prognostic value in the acute coronary syndromes, such as myocardial infarction, diastolic dysfunction, and atrial fibrillation in congestive heart failure patients. 10 Cancer patients frequently have obesity and diabetes as comorbidity conditions. Current studies show that microRNAs such as miR-9 may serve as novel biomarkers and molecular targets for cancer therapy in patients with comorbidity conditions. 11
Recently, other alternatives have been attempted to improve early detection of multimorbidity. Alemi et al. developed the multimorbidity index to account for the prognosis of patients with multiple diagnoses. The authors have reported that physiological markers may help not only in the prevention of certain conditions and comorbidities but also in the possibility of early diagnosis and treatment, increasing the chances of survival of patients and decreasing health expenditures. 12,13
Using simple blood tests in hospital and/or outpatient laboratories may be an easy-to-access alternative for the population to detect specific physiological markers for a set of diseases. As there are few studies evaluating markers related to multiple concomitant diseases, the aim of this article is to perform a systematic review to identify physiological markers associated with multimorbidity.
Materials and methods
The search was conducted in the following electronic databases: MEDLINE (via PubMed), Register of Controlled Trials (Cochrane CENTRAL), Academic Search Premier, CINAHL, Scopus, SocINDEX, Web of Science, LILACS, and SciELO. The search was conducted in the first semester of 2018 and included all articles from the beginning of the bases until May 2018. Manuscripts written in the following languages were included, English, Portuguese, or Spanish. The Medical Subject Headings (MeSH) terms and their synonyms were used to search the terms in all fields. The search strategy used in PubMed is shown in Table 1.
Literature search strategy used for the PubMed database.

The systematic review was reported according to the PRISMA statement and the AMSTAR 2. 14,15 According to PICOS principles, 14 we consider the following criteria: P means any patient who presented multimorbidity; I means patients with multimorbidity (who have two or more coexisting diseases); C stands for patients who have none or one disease; O means any physiological or molecular marker; and S stands for the study design, mainly observational/epidemiological studies.
Observational studies, which evaluated molecular, physiological, or genetic markers related to different multimorbidity, were selected. The inclusion criteria were studies reporting specific markers to a condition of at least two concomitant diseases. The exclusion criteria were papers that did not specify the marker or were related to one specific disease; studies evaluating seasonal or allergic diseases, general markers of oxidative stress, or markers of resting metabolic rate; and reviews or papers in a language other than English, Spanish, or Portuguese. Full texts of the selected articles after screening the titles and abstracts were assessed, and data were extracted using predetermined formats. The extracted data included author(s) and year of the publication, type of the study, sample, morbidities, and the evaluated biomarkers.
Two independent researchers (GDF and JAS) performed the literature search, screening titles and abstracts, full-paper reviews, study quality assessment, and data extraction. Disagreements were referred to a third author.
The project was registered in PROSPERO under number CRD42017055522.
Results
The search identified 922 papers. We found seven duplicate studies and another 775 were excluded as they did not include the outcome of interest. Thereafter, 140 papers were screened to title and abstract selection, and 37 papers were selected for full-text evaluation. Nineteen papers were excluded for the following reasons: languages other than English, Spanish, or Portuguese; literature review, case study, or incomplete data. In the end, 18 papers reporting at least one physiological marker with coexisting diseases were included in the systematic review (Figure 1).
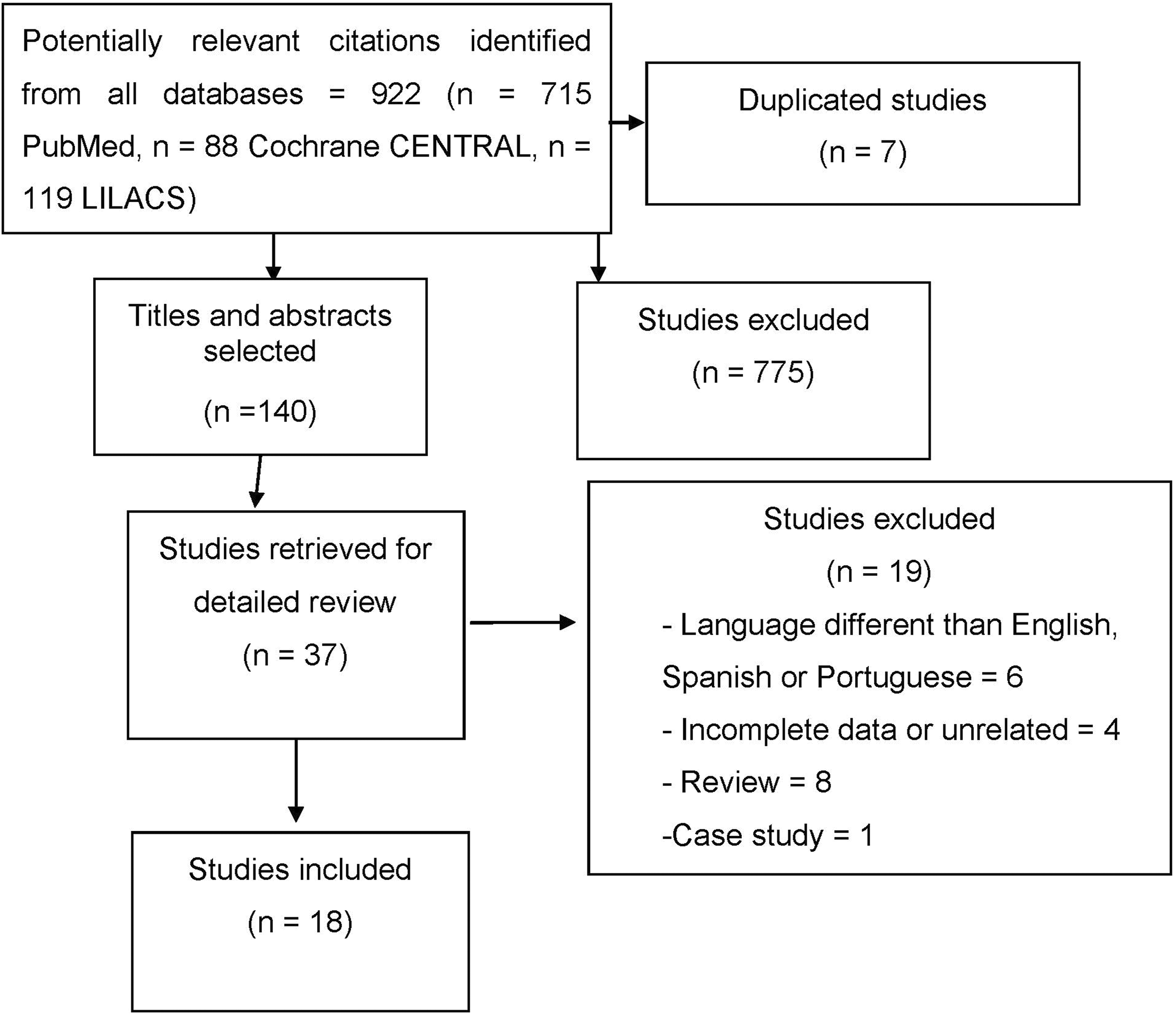
The flow diagram of studies included in the review.
Tables 2 and 3 show the characteristics of the included studies.
Characteristics of the included studies that analyzed multimorbidity.

IL-6: interleukin 6; DHEAS: dehydroepiandrosterone sulfate; IQR: interquartile range; CRP: C-reactive protein; Lp: lipoprotein; Cyst-C: cystatin C levels; OR: odds ratio; CI: confidence interval.
Characteristics of the included studies that analyzed at least two coexisting diseases (comorbidities).
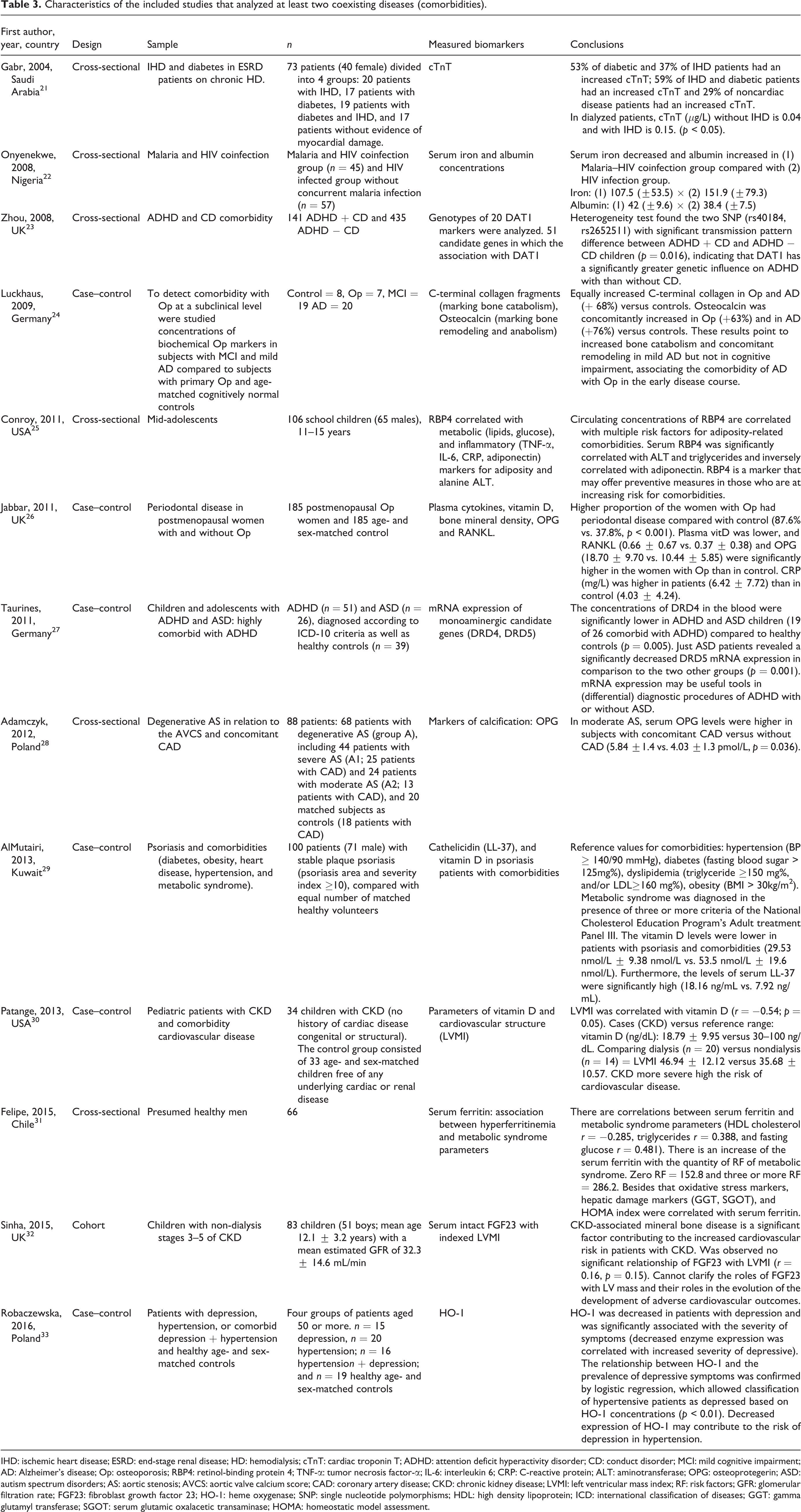
IHD: ischemic heart disease; ESRD: end-stage renal disease; HD: hemodialysis; cTnT: cardiac troponin T; ADHD: attention deficit hyperactivity disorder; CD: conduct disorder; MCI: mild cognitive impairment; AD: Alzheimer’s disease; Op: osteoporosis; RBP4: retinol-binding protein 4; TNF-α: tumor necrosis factor-α; IL-6: interleukin 6; CRP: C-reactive protein; ALT: aminotransferase; OPG: osteoprotegerin; ASD: autism spectrum disorders; AS: aortic stenosis; AVCS: aortic valve calcium score; CAD: coronary artery disease; CKD: chronic kidney disease; LVMI: left ventricular mass index; RF: risk factors; GFR: glomerular filtration rate; FGF23: fibroblast growth factor 23; HO-1: heme oxygenase; SNP: single nucleotide polymorphisms; HDL: high density lipoprotein; ICD: international classification of diseases; GGT: gamma glutamyl transferase; SGOT: serum glutamic oxalacetic transaminase; HOMA: homeostatic model assessment.
In relation to disease conditions, the studies are heterogeneous, and only five evaluated multimorbidity in a more widespread construct (Table 2). Although only five studies dealt exclusively with multimorbidity in general, our search selected some studies, which associated markers for specific comorbidities. We only considered papers evaluating at least two of the following diseases related to different markers: three studies related renal and cardiovascular disease, two studies with behavioral diseases, two with bone diseases associated with periodontal diseases and Alzheimer, one study related to depression and hypertension, one related to different cardiac conditions, one related to psoriasis and metabolic comorbidities, one study about infectious diseases, and two studies with healthy people that evaluated markers predicting multimorbidity (Table 3).
Discussion
This article aims to review the literature to identify physiological markers associated with patterns of multimorbidity. Based on the systematic search, we found 18 studies from 2004 to 2017, which evaluated physiological markers related to different concomitant diseases or which are strongly associated with the presence of multimorbidity in the future.
No randomized clinical trials (RCTs) were found in the search strategy, most part of the studies carried out observational analyses, and none cited a methodology including blind review. Nevertheless, from the 18 included studies, 15 presented a control group for comparability: patients who had only one of the morbidities of the study 16–24,27,28,30,33 or without morbidity (matched according to sex and age). 19,26,29 Although all included papers assessed association between at least two different morbidities, only five assessed specifically markers for multimorbidity in general regardless of the disease. The three studies, which did not present control groups, were related to correlation between variables, which may increase the risk of comorbidities. 25,31,32 In general, even considering that the included papers are not RCT or long follow-up periods, the presence of a control group in most studies can be used to assist with a more thorough data analysis. Nevertheless, suggestions are put forward as the results are not conclusive, because the aim is to observe cross-sectional data. The quality evaluation of the studies followed the parameters of the Newcastle–Ottawa scale. 34
Physiological markers and multimorbidity
Only five studies evaluated multimorbidity in general. The results cross-sectional data show that the elevated interleukin 6 (IL-6) and lower dehydroepiandrosterone sulfate (DHEAS) are associated with a greater burden of multimorbidity and suggest that investing in these markers may be an alternative for earlier detection and target interventions aimed at reducing multimorbidity. 16 Although high levels of serum cytokines such as IL-6 and tumor necrosis factor α (TNF-α) are considered risk factors for several chronic diseases, the second study emphasizes that these markers are not available in the majority of clinical laboratories. Therefore, other markers should be studied, such as C-reactive protein (CRP), lipoprotein (Lp), and cystatin C (Cyst-C) levels. People in the group of those with zero or one disease showed normal levels for the markers, as the number of chronic diseases increased the percentage of a person with a normal value of the markers decreased, showing that they are markers which can also be considered for detection of multimorbidity. 17 Three other studies also suggested CRP as a possible marker for multimorbidity, associating the increase of its concentration with two or more chronic conditions. 18–20 These data should be analyzed with caution, because cross-sectional and longitudinal studies have limitations to identify cause or consequence.
Physiological markers, patterns of multimorbidity, and specific combinations of diseases
In relation to the studies described in Table 3, combinations of pairs of diseases were normally controlled by individuals with only one of the associated diseases, thus observing the pattern of specific markers between groups. Three studies related renal and cardiovascular diseases. In ischemic heart disease (IHD) and diabetes in end-stage renal disease (ESRD) patients, it was observed that cardiac troponin T (cTnT) was increased in IHD and diabetic patients compared to control and isolated diseases, suggesting that increased cTnT appears to be the most specific biochemical marker to predict subclinical myocardial damage in ESRD patients. 21 It is suggested that chronic kidney disease severely increases the risk of cardiovascular disease 30 ; however, it does not seem to be associated with mineral bone disease. 32
Two studies analyzed attention deficit hyperactivity disorder (ADHD) and conduct disorder (CD) comorbidity. The genetic heterogeneity showed that variations in the dopamine active transporter 1 (DAT1) gene confer significantly different risks to ADHD children to either have or not have CD. 23 These data corroborate with Gizer who showed co-occurrence among psychiatric disorders and that the candidate gene studies of psychological disorders are involved in monoaminergic function (DAT1) giving the relevance of these neurotransmitter systems to brain–behavior relations. 35 Taurines et al. also related monoaminergic genes to comorbidities with autism spectrum disorders. 27
One study reported different cardiac conditions and concluded that the presence of coronary artery disease in moderate aortic stenosis was associated with increased serum osteoprotegerin (OPG) levels, suggesting the effect of atherosclerosis on early valve calcification. 28 Moreover, one study evaluated depression and hypertension and showed that decreased expression of heme oxygenase may contribute to the risk of comorbidity of depression in hypertension cases. 33
Two studies reported osteoporosis with comorbidities. It is clear that in Alzheimer’s disease there is an increase in bone catabolism, associating the comorbidity of Alzheimer’s disease with osteoporosis in the early disease course detected at the level of biochemical blood markers, such as C-terminal collagen fragments and osteocalcin. 24 Other comorbidity is periodontal disease, which is more common in women with osteoporosis and is associated with lower vitamin D and higher concentrations of RANKL and OPG. 26
Psoriasis and comorbidities (diabetes, obesity, heart disease, hypertension, and metabolic syndrome) can be evaluated with cathelicidin (LL-37) and vitamin D. Vitamin D levels were lower in patients with psoriasis and comorbidities, but serum LL-37 levels were significantly elevated. 29 Furthermore, one study analyzed the coinfection of malaria and HIV compared to HIV-infected individuals without concurrent malaria infection and showed that serum iron and albumin concentrations were indicators related with malaria infection in HIV-infected subjects. 22
Two studies with healthy people evaluating markers that predict multimorbidity were included. In adolescents, the establishment of retinol-binding protein 4 as a marker may offer health-care providers a tool to begin aggressive preventive measures in those who are at increasing risk for adiposity-related comorbidities but have not yet been afflicted by them. 25 In healthy men, significant correlations were found between serum ferritin concentration and metabolic syndrome parameters. 31
Related findings
A birth cohort study aimed at assessing the association of obesity with physiological markers at 22 years of age, showing direct association for IL-6 and CRP and an inverse association for adiponectin, suggesting early care for this population at risk. 36 A meta-analysis of prospective studies suggests the association of IL-6 and CRP with type 2 diabetes risk (relative risk of 1.31 per 1 log pg/mL increment in IL-6 levels and of 1.26 per 1 log mg/L increment in CRP levels). 37
Therefore, a systematic review has shown the elevation of the concentrations of pro-inflammatory cytokines (IL-6, TNF-α) in metabolic syndrome, suggesting that the measurement of these biomarkers may aid in the detection of these disorders, 38 and agrees with findings from the past decade that have already indicated that laboratory-measured pro-inflammatory markers are needed to target specific treatment in the metabolic syndrome. 39
Limitations
As limitations of this study, the included papers were cross-sectional analyses; however, it is not clear whether the marker is a cause or a consequence related to different pairs of diseases. In addition, only five studies are performed with nonspecific concomitant diseases, showing the existing gap in the literature. Therefore, more studies controlling confounding variables and monitoring different conditions are needed to find markers that allow the prevention or early treatment of different multimorbidity.
Conclusions
This study was important for grouping physiological markers associated with different types of comorbidities to facilitate early diagnosis and intervention in these patients. Nonetheless, there is a paucity of studies related to physiological markers and multimorbidity. In the initial efforts, despite cross-sectional analyses, DHEAS, IL-6, CRP, Lp, and Cyst-C seem to be the choices for further investigation regarding the effects of physiological markers related to multimorbidity.
Footnotes
Authors’ note
All authors have read and agreed the Statement for Authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Medical Sciences, Faculty of Health Sciences, University of Beira Interior.