
Abstract
Cancer patients are at heightened risk for infections due to immunosuppression, often leading to excessive or inappropriate antimicrobial use. An antimicrobial stewardship program (ASP) is essential to optimize therapy, but its implementation in oncology remains challenging and underexplored. Thus, a scoping review was conducted using Arksey and O’Malley’s framework and the Preferred Reporting Items for Systematic Review and Meta-analyses extension for Scoping Reviews (PRISMA-ScR) guidelines, with an aim to map existing evidence on ASP implementation in oncology settings, focusing on types of interventions, outcomes, and barriers. Searches across PubMed, Scopus, and Web of Science (until July 2024) identified studies on ASP in cancer patients. All original research evaluating stewardship interventions in oncology settings was included. Fifty-six studies from 18 countries were included, comprising diverse study designs and intervention types. Most interventions demonstrated improved antimicrobial appropriateness and reduced usage. Diagnostic interventions, including procalcitonin (PCT) and rapid diagnostics, facilitated targeted therapy. Therapeutic strategies such as de-escalation and prospective audit and feedback (PAF) effectively reduced broad-spectrum antibiotic use. Barriers included limited training, resources, and diagnostic infrastructure. ASP in oncology settings is feasible and beneficial, especially in improving antimicrobial use. Broader adoption requires overcoming systemic barriers, standardizing interventions, and strengthening multidisciplinary collaboration.
Introduction
Antimicrobial resistance (AMR) is directly responsible for approximately 1.27 million deaths globally and is associated with up to 4.95 million deaths worldwide. 1 If current trends continue, it could result in 10 million deaths per year by 2050, surpassing cancer as a leading cause of death. 1 There is a significant regional variability in resistance patterns driven by inadequate surveillance, inappropriate antimicrobial use, and poor infection control practices.2,3 Cancer patients are particularly vulnerable due to their immunocompromised state from both the disease and its treatment, placing them at increased risk for infections caused by multidrug-resistant organisms.4,5
Antimicrobial stewardship programs (ASPs) are evidence-based initiatives designed to optimize antibiotic use, reduce AMR, and improve patient outcomes.6,7 In cancer care, these programs face unique challenges due to higher disease severity, diagnostic uncertainties, and the complexity of managing infections in immunocompromised patients.8,9 The high propensity of antimicrobial use in such a setting further increases the risk of AMR. Also, in patients with cancer, AMR is likely to have a high impact on outcomes. Despite their potential to reduce healthcare-associated infections, improve antimicrobial efficacy, and lower costs, the adaptation of ASP to oncology settings remains limited, particularly in low- and middle-income countries.10,11 Thus, we conducted a scoping review to gauge the evidence of ASP in an oncology setting, which might help healthcare practitioners develop an effective strategy to counteract AMR.
The scoping review was chosen over a systematic review as the research question of the current review is broad and does not aim for a quantitative synthesis, making it a comprehensive mapping study in the field of ASPs in oncology. Further, the heterogeneity among the included studies in terms of their study design, ASPs intervention types, and outcomes points toward the suitability of a scoping review, which can address the diversity among these studies without restricting the robust evidence synthesis.
Materials and Methods
The Arksey and O’Malley methodological framework for conducting this scoping review is followed. 12 Further, the Preferred Reporting Items for Systematic Review and Meta-analyses extension for Scoping Reviews (PRISMA-ScR) checklist was used to develop the manuscript. 13 Although a protocol was developed before conducting this review, the protocol was not registered in International Prospective Register of Systematic Reviews (PROSPERO), as scoping reviews are not eligible for registration in PROSPERO.
Research Question
What is the current landscape of antimicrobial stewardship (AMS) interventions in oncology settings, and how do they impact antimicrobial use, resistance patterns, and clinical outcomes in cancer patients?
Search Strategy to Identify Relevant Studies
A comprehensive electronic search was performed across Scopus, PubMed, and Web of Science. The following search string was used using keywords from population, concept and context: ((cancer* OR onco* OR malignan* OR carcino*) AND (“formulary restriction” OR “Defined Daily Dose (DDD)” OR “antimicrobial cycling” OR “dose optimization” OR “Days of Therapy (DOT)” OR “de-escalation” OR “timeout” OR “PAF” OR steward* OR “AMS” OR “antimicrobial stewardship” OR “antibiotic stewardship”)). The search included all studies up to 24th July 2024. Rayyan.ai software was used to import and manage the articles. 14
Eligibility Criteria and Study Selection
The scoping review included all original research articles in the English language (e.g., randomized controlled trials, observational studies, cohort studies) that described AMS interventions and their outcomes in cancer wards. Articles were excluded if they were unrelated to AMS or were related to out-of-hospital care.
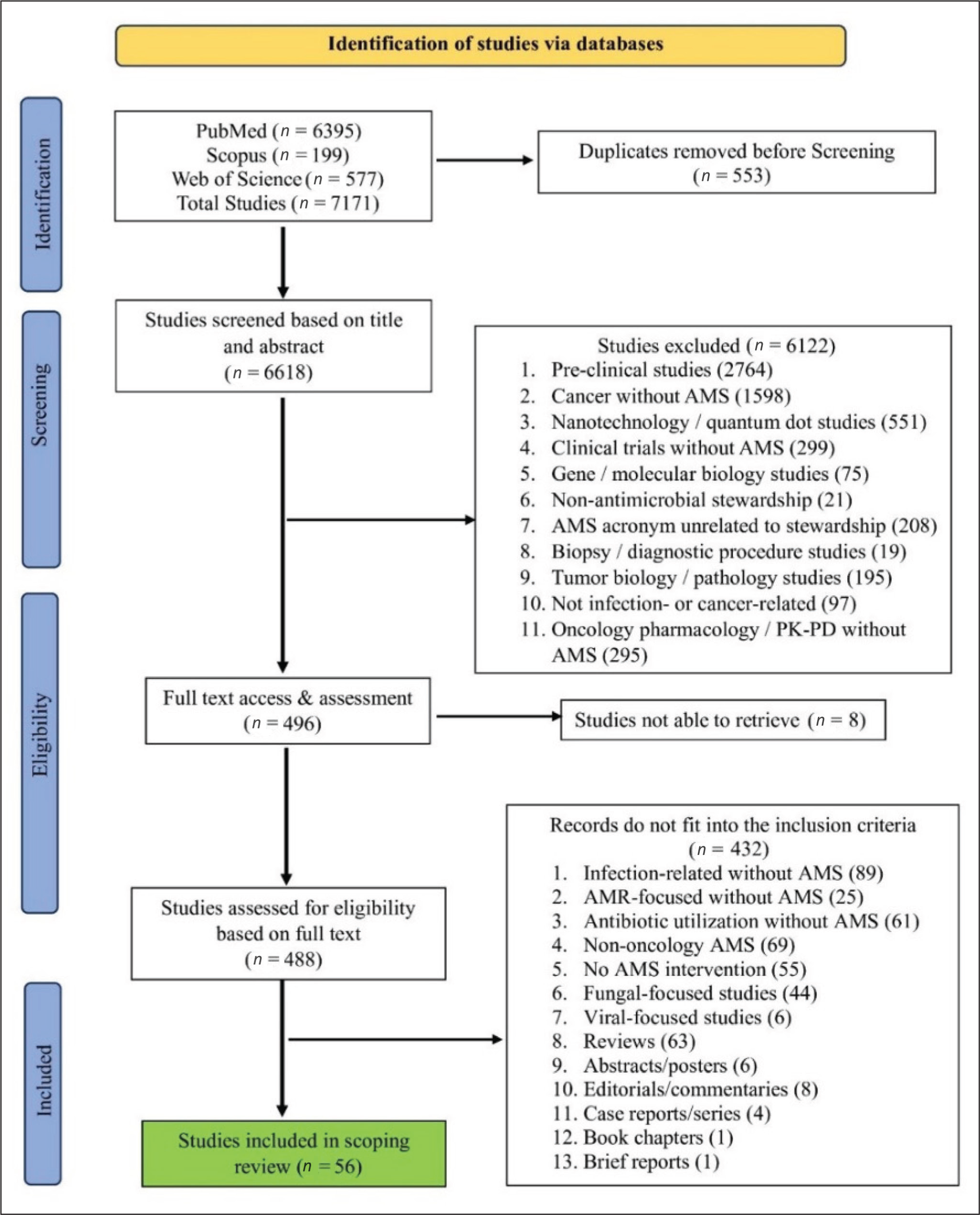
All duplicate records were removed. Further, all the remaining articles were screened for eligibility based on the titles and abstracts by two independent authors (DA and NG). The third author (MV) resolved any disagreements during the screening. Later, potentially relevant articles were read in full independently by two authors (DA and NG), with the selection of screened articles blinded through Rayyan. If there were conflicting opinions about the inclusion or exclusion of articles, consensus was reached with discussion among all authors. The research team discussed the exact definition of best practice and which elements should be included. The PRISMA diagram for identifying literature has been illustrated in Figure 1.
PRISMA-ScR Flow Chart Detailing the Identification, Screening, Eligibility, and Inclusion of Studies.
Data Charting and Extraction Process
The data extraction was carried out by the two independent authors (DA and NG), and any disagreements were resolved by a third author (MV). The data was charted and extracted from eligible articles using a predesigned form and entered into Microsoft Excel. The following details were extracted: Authors, country, year of publication, study settings, population, study design, sample size, and key findings related to ASP.
Summarizing and Reporting the Result
The knowledge, attitude, and practice (KAP) of ASP among healthcare professionals in oncology on ASP and AMR were tabulated. We also summarized the impact of various diagnostic/therapeutic interventions in cancer settings on mortality, clinical cure, antimicrobial use, resistance, adherence, and Clostridioides difficile infection (CDI). The quality or risk of bias assessment was not performed for the included studies in this review, as the review was solely focused on mapping the evidence rather than evaluating the effectiveness of ASP interventions.
Results
Selection of Sources of Evidence
Out of 7,171 articles identified via search, a total of 553 duplicates were removed before screening. Thus, 6,618 articles were eligible for title and abstract screening, of which 6,122 were removed based on the eligibility criteria. The remaining 496 were considered for full text review, of which eight articles were not able to be retrieved, and 432 articles did not meet the inclusion criteria. Thus, a total of 56 articles were reviewed to generate the evidence. The details on included and excluded articles have been depicted in Figure 1.
Characteristics and Results of the Source of Evidence
The 56 studies in this review explore various aspects of AMS in cancer patients, categorized into KAP (n = 12), diagnostic interventions (n = 8), and therapeutic interventions (n = 34). Additionally, one study explored the impact of antimicrobial allergy labeling on overall antimicrobial prescription. 15 It was found that those with an allergy label had higher antimicrobial use. 15 Another study by Sasaki et al. showed that an AMS pharmacist may have a role in the reduction of postoperative surgical site infections. 16
These studies span 18 countries, with the majority conducted in North America (n = 22), followed by Asia (n = 21), Europe (n = 6), Australia (n = 3), South America (n = 2), and Africa (n = 2). Most were single-center studies (n = 48), with eight multi-center studies. The study designs included in this review consisted of randomized controlled trials (n = 2), non-randomized controlled trials (n = 17), and observational studies (n = 37).
Assessment of KAP Related to ASP
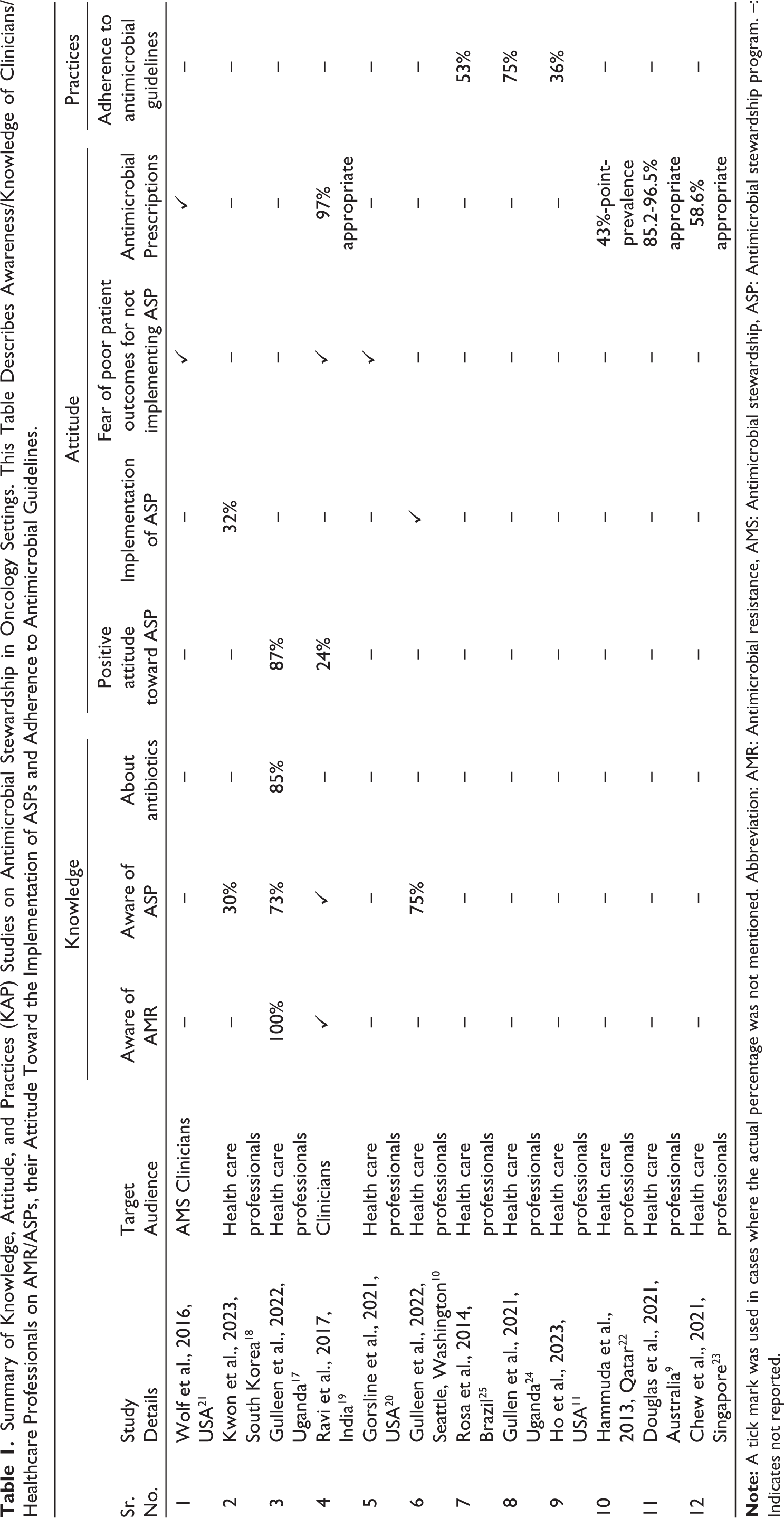
Twelve studies examined ASP-related KAP (Table 1) in healthcare professionals. The knowledge about antibiotics and their importance was very high among healthcare professionals (85%–100%). 17 However, the awareness of ASP was low, ranging from 30% to 75%.10,17,18 Positive attitudes toward ASP varied from 24% to 87%, whereas the implementation of ASP is 32%.10,17–19 Three studies expressed concern about poor patient outcomes from a lack of ASP implementation.19–21 In a point-prevalence survey on oncology patients, 43% were on antimicrobials. 22 In three studies, appropriate antibiotic prescribing patterns varied from 58.6% to 97%.9,19,23 The adherence to antimicrobial guidelines ranged from 36% to 75%.11,24,25 Common barriers to ASP implementation included a lack of knowledge, poor communication, limited resources, insufficient training, and difficulties obtaining blood cultures.17,21
Summary of Knowledge, Attitude, and Practices (KAP) Studies on Antimicrobial Stewardship in Oncology Settings. This Table Describes Awareness/Knowledge of Clinicians/ Healthcare Professionals on AMR/ASPs, their Attitude Toward the Implementation of ASPs and Adherence to Antimicrobial Guidelines.
Diagnostic-driven Interventions
Table 2 summarizes eight studies on diagnostic interventions in cancer patients. These studies used various diagnostic tests, including improved blood culture collection, procalcitonin (PCT) testing, multiplex polymerase chain reaction assay (PCR) panels, and rapid antimicrobial susceptibility testing as tools for ASP.26–33 Increasing blood culture volume improved etiological diagnosis, while rapid bacterial tests helped detect infections faster and guide better treatment.26,27,30,32,33 Diagnostic improvements also contributed to reduced antibiotic use, shorter treatment durations, and increased optimal antibiotic selection.27–31,33 Some studies reported no significant changes in mortality outcomes.26,27,30–32
Outcomes Associated with Diagnostic-based Antimicrobial Stewardship Interventions in Cancer Patients. This Table Represents the Impact of Diagnostic Stewardship Interventions on Antimicrobial Use, Clinical Impact, and Mortality Across the Studies.

Abbreviations: ANC: Absolute neutrophil count, AST: Antimicrobial susceptibility testing, CoNS: Coagulase-negative staphylococci, FN: Febrile neutropenia, HM: Hematologic malignancies, PCR: Polymerase chain reaction, ST: Solid tumor, TTP: Time-to-positivity, VRE: Vancomycin-resistant Enterococcus.
Therapeutic Interventions
The studies summarized in Table 3 evaluated outcomes associated with AMS interventions targeting specific antimicrobials mainly among patients with hematologic malignancies (HM) with febrile neutropenia (FN). These interventions focused on reducing the use of broad-spectrum agents such as carbapenems, vancomycin, gentamicin, and fluoroquinolones.7,34–42 Two studies focused on cycling cefepime/amikacin and piperacillin–tazobactam (TZP), while one study assessed antimicrobial timeouts for carbapenems and antibiotics against methicillin-resistant Staphylococcus aureus.8,43,44 A consistent trend across studies was a reduction in the use of targeted antimicrobials.7,8,35–42,44 Some studies reported a decrease in vancomycin-resistant Enterococcus (VRE) incidence and CDI rates.8,37,38 However, changes in mortality were inconsistently reported.7,34
Outcomes Associated with Antimicrobial Stewardship Therapeutic Interventions Targeting Particular Antimicrobials in Cancer Patients. This Table Represents the Impact of Reducing or Optimizing High-risk Antimicrobials on Mortality, Clinical Cure, Antimicrobial Use, and Clostridioides Difficile Infection (CDI) Across the Studies.

Abbreviations: FN: Febrile neutropenia, HM: Hematologic malignancies, MRSA: Methicillin-resistant Staphylococcus aureus, TZP: Piperacillin–tazobactam, ST: Solid tumor, VRE: Vancomycin-resistant Enterococcus, CDI: Clostridioides difficile infection.
The various ASP therapeutic interventions depicted in Table 4 generally led to improvements in antimicrobial use among patients with cancer, HM, and FN. Most studies focused on comprehensive strategies encompassing the best practices of ASP.45–55 Some studies focused on targeted strategies such as prospective audit and feedback (PAF), 6 de-escalation of antibiotics,56–62 withholding antibiotics in viral infections,63, and educational programs. 64 ASP best practices and PAF were often associated with reduced inappropriate antibiotic use, better acceptance of recommendations, and decreased resistance.6,45–55 De-escalation strategies helped to reduce the use of broad-spectrum antibiotics and decreased the duration of antibiotics without increasing mortality or affecting clinical outcomes.56–62 Withholding antibiotics in viral infections led to shorter treatment duration, and educational efforts also showed benefits in reducing antimicrobial use and reducing mortality.63,64
Outcomes Associated with General Antimicrobial Stewardship Therapeutic Interventions in Cancer Patients. This Table Represents the Impact of the Implementation of ASP Best Practices, PAF, De-escalation Strategies, Withholding Antibiotics, and Educational Interventions on Antimicrobial Utilization, Clinical Outcomes, Mortality and Decreased Clostridioides Difficile Infection (CDI) Across the Studies.

Abbreviations: ASP: Antimicrobial stewardship program, FN: Febrile neutropenia, HM: Hematologic malignancies, PAF: Prospective audit and feedback, CDI: Clostridioides difficile Infection.
Discussion
This scoping review aimed to map the existing literature on AMS in oncology settings, providing insights into three major domains: KAP, diagnostic-driven, and therapeutic interventions. ASP in oncology encounters numerous challenges, including the complexity of infections, underlying disease conditions, and concerns about patient outcomes. Hence, understanding these aspects is essential for improving stewardship efforts. Although the concept of ASP is not yet well established in oncology practice, KAP studies have shown that healthcare professionals are aware of the significance of AMR and generally exhibit a positive attitude toward ASP implementation.17,18 Adherence to antimicrobial guidelines is a key component of effective AMS. Variability in adherence suggests that while some settings have well-established stewardship programs, others may lack standardized protocols or sufficient training in appropriate antimicrobial prescribing.11,24,25 Fear of poor patient outcomes, particularly in critical cases, is the main reason for not implementing ASP, which often leads to unnecessary antimicrobial use.19–21 This highlights the need for more support and reassurance through training. The variability in prescribing patterns reflects differences in available resources, institutional policies, and access to clinical guidelines.9,19,23 Barriers such as limited knowledge, resources, and education hinder ASP implementation, especially in low-resource settings.17–19,21 Thus, addressing barriers and initiating training programs is essential to enhance awareness of ASP.
Cancer patients often receive extensive antibiotic treatment and face numerous complications. Diagnostic stewardship is key in supporting de-escalation strategies, and result-based recommendations are increasingly adopted in clinical practice. 30 However, several barriers hinder effective diagnostic stewardship, including limited resources, a shortage of dedicated microbiology staff, poor communication among physicians, and delays in following up on results.27,33 Implementing diagnostic strategies tailored to each institution’s specific needs can significantly improve the quality of care. Several diagnostic measures have guided antimicrobial therapy, including rapid commercial tests, biomarkers such as PCT, and blood cultures.26–33 The availability of a 24-hour microbiology laboratory is essential for providing timely results, enabling prompt review of empirical broad-spectrum antibiotic use. This, in turn, helps reduce both financial burdens and the risk of antibiotic-related toxicity. 32 In the studies, rapid pathogen identification through advanced techniques significantly reduced reporting time, aiding targeted antibiotic therapy.27,30,33 Blood cultures are crucial for establishing definitive evidence of infection in neutropenic patients. Obtaining cultures before initiating antibiotics improves diagnostic accuracy. Additionally, the volume of blood collected significantly influences the reliability of the results. Biomarker-guided therapies can support early de-escalation of antibiotics. PCT is beneficial in this context: A PCT level below 0.5 µg/L suggests that antibiotics can be discontinued, while a level below 0.25 µg/L indicates that a bacterial infection is unlikely. 31 These test-based recommendations are generally well accepted. The absolute neutrophil count is another cost-effective and rapid tool, commonly used in patients with HM. 29
Therapeutic interventions targeting particular antibiotics such as carbapenems, vancomycin, or other non-carbapenems can help reduce overall antibiotic use and, in the long-term, lower the risk of developing AMR.7,34–42 In some studies, targeted antimicrobial is replaced with alternative antibiotics with a narrower spectrum, such as TZP, and cephalosporins.7,34,39 These substitution strategies aim to preserve the efficacy of last-line antibiotics, reduce selection pressure for multidrug-resistant organisms, and maintain clinical outcomes. However, sometimes these strategies can have unintended effects and increase CDI rates. 39 Regular audits and close surveillance are essential to detect and address these issues early.
Across most studies, ASP demonstrated positive impacts, especially in reducing inappropriate antimicrobial use.45–47,49–55 Two studies showed a reduction in overall mortality.51,54 While one study reported a decrease in Staphylococcus aureus-specific mortality, indicating targeted effectiveness in high-risk infections. 50 Although personalized ASPs are less frequently studied, they may offer enhanced clinical outcomes. 48 PAF and preauthorization are evidence-based interventions and two core elements of ASPs. PAF deals with the review of antimicrobials and their recommendations, whereas preauthorization deals with the approval for the use of antimicrobials. Thus, PAF helps to improve clinical outcomes, reduce hospital stays, and combat AMR. 65 Barriers to achieving a high acceptance rate could be patient-related, time constraints, or physicians’ resistance. Pharmacist-led ASPs are more effective due to their expertise in pharmacotherapy, timely provided interventions, and strong interdisciplinary collaborations. 51
De-escalation strategies, which involve narrowing empirical therapy based on culture results and laboratory findings, have been associated with reduced antibiotic use and duration.56–62 Key approaches include switching from intravenous to oral therapy, from combination therapy to monotherapy, and from broad-spectrum to narrow-spectrum antibiotics.58,60–62 As a result, several studies have reported an overall shorter duration of antibiotics.57,59,62 Notably, two studies also observed a reduction in mortality, which is a positive finding, especially given that many studies have not demonstrated a significant change in mortality following the implementation of ASP strategies.56,57 Withholding antibiotics in cases of confirmed viral infections can promote optimized antibiotic use without compromising patient safety. 63 Education-focused interventions resulted in a decrease in inappropriate antibiotic use. 64 These results may contribute to lower resistance over time. ASPs help improve antibiotic prescribing, but their impact on AMR may take time and is often influenced by local epidemiology and infection control measures. Regular educational sessions are essential to build trust and strengthen collaboration between physicians and the ASP team.
Low and Middle-Income Countries (LMICs) represent about 57% of new cancer patients and 65% of deaths among cancer patients. 66 Similarly, LMICs, particularly sub-Saharan Africa and South Asia, contribute to the higher AMR-associated deaths. The risk of death due to fatal infection increases nearly three times among cancer patients compared to non-cancer patients. Further, about 50% death among cancer patients (solid as well as HM) are attributed to the role of infection. 67 Although there is a lack of epidemiological data/evidence on death among cancer patients due to AMR, the contribution of LMIC to mortality among cancer patients and mortality due to AMR highlights the possible overlap between these two domains. 68 There are several barriers associated with the implementation of ASPs in LMICs, such as a lack of human resources/leadership, physician workload/time constraint, lack of funds, lack of diagnostic or laboratory support, lack of awareness/knowledge, and conflict between healthcare professionals/prescribers. However, these barriers can be overcome by establishing a core ASPs committee with well-qualified leadership, adopting guideline-oriented antimicrobial practices, and strengthening the rapid microbial diagnosis, well-structured prescribing hierarchy, access to electronic health records and antibiogram, and well-planned reserved antibiotic list, among other measures. 69 Thus, there is a need for strengthening the healthcare ecosystem, implementation of ASPs in oncology settings, and a change in the policy and education to combat AMR in LMICs.
The studies included in this review highlight the implications of a wide variety of diagnostic and therapeutic interventions, demonstrating their impact on antimicrobial use, mortality among cancer patients, overall clinical outcomes, and incidence of CDI. Antimicrobial utilization was measured using diverse metrics such as DDD, DOT, proportion of appropriate prescriptions, or frequency of prescriptions, resulting in variation in the reported estimates of antimicrobial use. Mortality outcomes were reported inconsistently, often as 30-day mortality, with some studies indicating increases or decreases and with varying follow-up durations. Clinical impact was assessed through measures such as changes in clinical cure rates, incidence of resistant organisms (including VRE), and CDI rates. In addition to outcome variability, substantial methodological heterogeneity was observed across studies, including differences in study design (retrospective, prospective, quasi-experimental, and before-and-after), sample sizes, and risk adjustment approaches. The type, intensity, and components of AMS interventions also varied considerably, particularly in implementation strategies, multidisciplinary involvement, audit and feedback, and diagnostic stewardship practices. Geographical heterogeneity further contributed to variability, as studies were conducted across diverse countries and healthcare settings with differences in infrastructure, baseline resistance patterns, diagnostic capacity, stewardship resources, prescribing guidelines, cancer epidemiology, patient case-mix, and institutional antimicrobial policies. Overall, the clinical, methodological, and geographical heterogeneity precluded quantitative synthesis. Therefore, a qualitative evidence synthesis was undertaken to provide a context-sensitive interpretation of the findings.
Although the current review mapped the importance of KAP and necessary interventions to practice ASP in the oncology setting, the review has various limitations, such as restricting to English language studies, which may have introduced bias. However, no relevant non-English studies were identified. Also, excluding gray literature likely omitted insights from underrepresented regions and non-academic settings. The lack of standardized definitions for AMS interventions complicated impact evaluation, and most studies focused on short-term outcomes, leaving long-term effectiveness unclear. Although the prospective registration of the scoping review in the Open Science Framework is encouraged, it is not a mandatory requirement. Thus, this review is limited by its registration in a public repository. Similarly, the risk of bias of critically appraised articles was not assessed. Future studies should focus on implementing AMS in high-risk settings, engaging multidisciplinary teams, and integrating infection control measures. Multicentric studies are essential for comprehensive insights into local epidemiological resistance patterns and best practices.
Conclusion
AMS has demonstrated potential benefits across various settings. However, its implementation in high-risk populations such as cancer patients remains challenging. The immunocompromised state of these patients increases their susceptibility to infections, often resulting in the overuse or irrational use of antibiotics. Despite these challenges, ASP has demonstrated benefits, including improved patient outcomes and decreased length of stay. Thus, strengthening AMS efforts in oncology is critical for optimizing therapy, curbing AMR, and enhancing patient care.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Not applicable.
Authors’ Contribution
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. All the authors are eligible to be author as per the International Committee of Medical Journal Editors (ICMJE) requirements/guidelines.
Availability of Data and Materials
All data generated or analyzed during this study are included in this article and its supplementary information files. Further, the data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not involve experiments on animals or human subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Use of Artificial Intelligence-assisted Tools:
The authors declare that they have not used artificial intelligence (AI)-tools for writing and editing of the manuscript, and no images were manipulated using AI.
List of Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.