
Abstract
The loss of teeth is always challenging for the patients. It is not only a functional loss but also a psychological and social loss. But with the advent of dental implants, this clinical situation can be dealt with tactfully. In an edentulous arch, prosthetic rehabilitation by all on 6 implants require accurate placement of implants for a successful result. A computer-guided surgical stent can be advantageous over arbitrary placement of implants and can overcome the difficulties associated with arbitrary placement. Using the cone beam computed tomography of the patient, virtual planning of implant is done. The exact implant angulations can be visualized to achieve the best possible esthetics and occlusion. This information is then converted to fabricate a stent using three-dimensional printing. Using this stent, a flapless surgical implant placement can be done which will reduce the post-operative trauma. This case report describes a case of a patient having an edentulous mandibular arch. The prosthetic rehabilitation of the mandibular arch was done by flapless surgical placement of six implants using a computer-guided surgical stent.
Introduction
In the past, the implant procedure was planned on the basis of the available bone on a radiograph that may lead to improper positioning and angulation of implant that cannot be corrected by prosthetics. This might create a problem in esthetic and function because of lateral forces transmitted to implant. 1 With the advancement in computer-guided surgical techniques, it has become possible to improve implant positioning, prevent injuries to important anatomical structures such as mandibular nerve, improve functional and aesthetic outcome of the prosthesis, and reduce operative time and post-operative discomfort. 2 , 3
The conventional method of pre-operative planning includes the radiographic assessment of the available bone by periapical and panoramic radiographs. After the introduction of cone beam computed tomography (CBCT), the accuracy of implant placement has increased as it provides a three-dimensional (3D) view of anatomical structures. Various implant planning software packages were developed and used to virtually plan implant positions. Along with the development of computer-aided design and computer-aided manufacturing (CAD/CAM) technology, it has become possible to replicate this virtually planned position in patient. 4
In computer-guided surgery, first CBCT is acquired followed by the virtual placement of implant with the aid of software, and surgical stent is then fabricated by 3D printing to replicate this virtually planned position in patient. This surgical stent has sleeves that correspond to the diameter of drills or implant. 1 The surgical stent is tooth supported, mucosa supported, or bone supported. The tooth-supported stent is more accurate than mucosa- supported stent. 5 , 6 Flapless surgery can be performed using a computer-guided surgical stent. Advantages of flapless surgery include less traumatic surgery, reduction in post-operative complications, preservation of soft tissues, etc. 7
Various studies have been done to check the reliability of computer-guided surgery. Schneider et al. 8 in 2009 conducted a systematic review to check the accuracy and clinical outcome of the computer-guided surgical template-based implant surgery. The accuracy of the surgical guide was checked by measuring the deviation between virtually planned implants and actually placed implants using CBCT. He concluded that the survival rate of the implants placed using the computer-guided surgical stent was 91% to 100%, and the deviation from virtually planned to actually placed implants was measured. In this systematic review, the mean values of deviation at the entry point and at the apex were 1.07 mm and 1.63 mm respectively. 8
So many studies have been conducted for measuring the accuracy of computer-guided surgery. In 2010, 2013, and 2014, Pettersson et al., Vieira et al., and Beretta et al. in their studies checked the accuracy of the computer-guided template-based implant placement respectively and concluded that implants placed using the computer-guided surgical stents were more accurate than those placed using the conventional method. 9 - 11
Thus, the use of computer-guided surgical stent has better advantages over nonguided surgeries because it will reduce postoperative surgical complications and the most optimum position of implants will be achieved for future prosthetic work. 12 In the present case report, implant surgery for edentulous mandible using a computer-guided surgical stent has been described.
Preoperative View

Preoperative OPG

CBCT Image

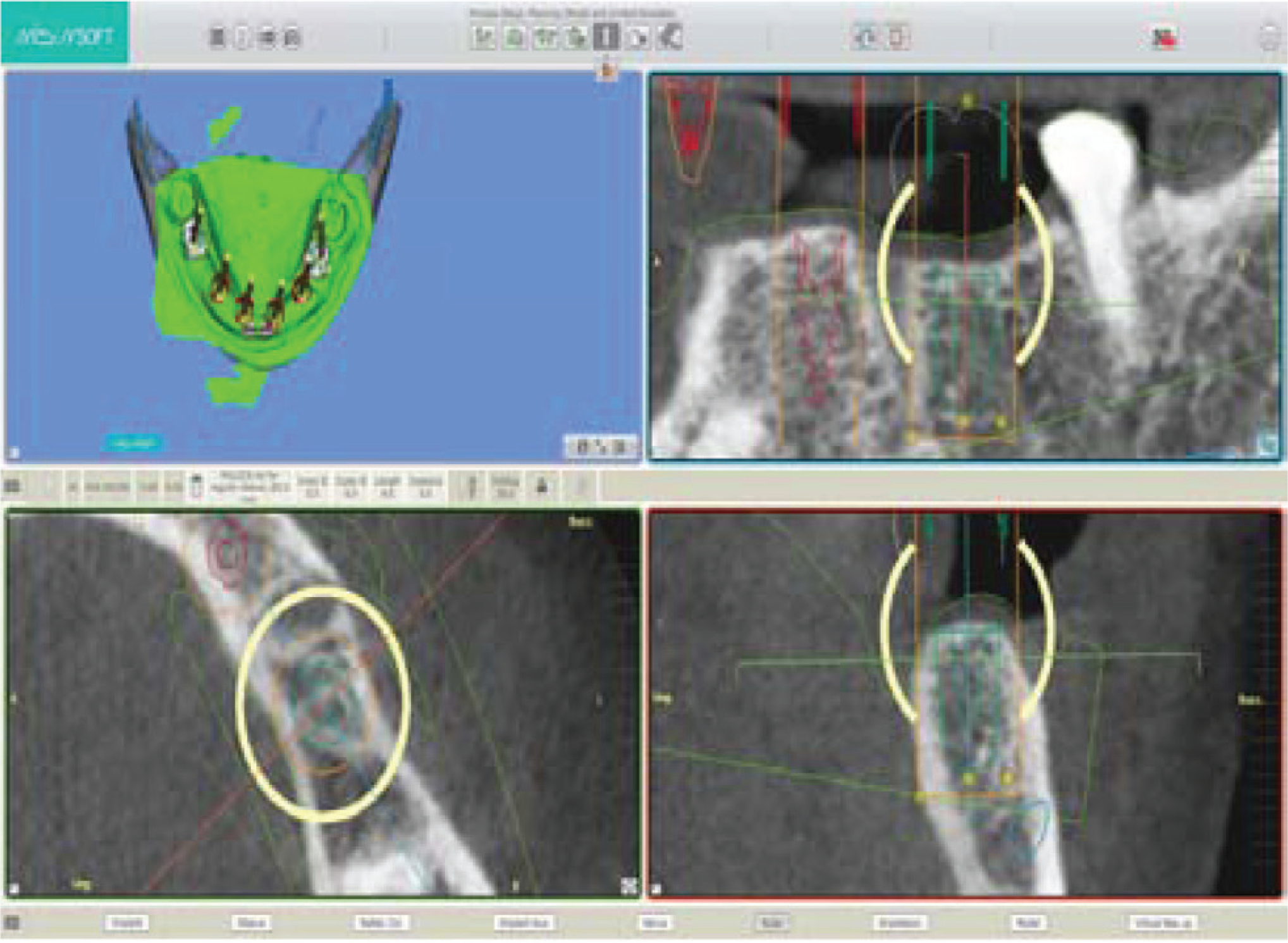
Virtual Implant Planning of 36 Regions for Computer-Guided Stent in Software
Computer-Guided Surgical Stent

MIS SEVEN Implant Kit for Computer-guided Implant Placement

Stabilization of Stent by Fixation Screws

Osteotomy Procedure

Case Report
A 50-year-old female patient came to the Department of Prosthodontics with the complaint of difficulty in chewing because of the loss of teeth. The examination of patient showed that in the mandibular arch only the second molars were present in both the quadrants. In the maxillary arch, all teeth were present (Figure 1). After radiographic and clinical examinations (Figure 2), implant-supported fixed prosthesis in the mandibular arch was planned. The patient was informed about the treatment plan, and her consent was taken before the start of any procedures. Preoperative investigations of the patient were done that included the blood profile (hemoglobin, complete blood (cell) count, bleeding time, clotting time, random blood sugar), and cone beam computed tomography (CBCT; Figure 3). The blood reports of the patient were within the normal range.
A mandibular conventional partial trial denture was fabricated, which was verified in the patient. This trial denture along with the mounted cast and CBCT data was sent to the lab for the fabrication of the computer-guided surgical stent. With the help of MIS MSOFT software, using the patient’s CBCT data, the virtual placement of implants was carried out (Figure 4). Sizes and location of the implants were determined based on the available data. Implants of 3.75 × 11.5 mm2 size were planned in the 31,35,42,44 regions, and those of 5 × 8 mm2 size were planned in the 36, 46 regions. Once the correct position and angulation of the implants were achieved, the computer-aided design of the surgical stent was made. This design was used to get the 3D print of the surgical stent with sleeves and stabilization screws. The 3D printed stent was tooth and bone supported (Figure 5).
Using this computer-guided surgical stent, flapless implant surgery was carried out. The implant system used in this case was MIS SEVEN (Figure 6). After giving local anesthesia, the surgical stent was fixed and stabilized with the help of fixation screws (Figure 7). Osteotomy was performed through the sleeves of the surgical stent and the implants were placed through the sleeves (Figure 8). After the placement of the implants, gingival formers were placed. Figures 9 and 10 show the postoperative clinical and radiographic views, and Figure 11 shows 4-month postoperative view.
After 4 months, the prosthetic phase was carried out. An open tray impression was taken with a polyether impression material for the fabrication of the master cast (Figure 12). On the master cast, a verification jig was made using the light cure acrylic resin. The jig trial was done in patient’s mouth (Figure 13). Facebow record and jaw relation were recorded and mounted on an articulator (Hanau™ Wide-Vue, Louisville, KY, USA). A metal framework was made on the master cast and this framework was then tried (Figure 14). The final PFM crowns were checked in centric and eccentric movements. All the deflective contacts were removed and prosthesis was cemented over the abutments with zinc phosphate cement (Figures 15 and 16). The follow-up of the patient was done after 1 week and the patient was kept on a regular 3-month recall appointment. Figure 17 shows the 1-month follow-up.
Postoperative Clinical View

Postoperative OPG

Healing After 4 Months

Open Tray Impression with Polyether Impression Material

Trial of Verification Jig

Metal Trial

Final PFM Restoration

Postoperative View

1-Month Follow-up

Discussion
Accurate selection of implant position is an important factor for the successful functional and aesthetic requirement of the resultant prosthesis. The accurate position is also required for the optimum osseointegration as the implant should be covered by the bone completely. The implant should not damage the important anatomical structures such as mandibular nerve, mental foramen, and maxillary sinus. 13
Since the advancement in the radiographic 3D imaging technique, implant planning software, and CAD/CAM technique, it became possible to place the implant in the same manner as it used to be planned. The trend in implant dentistry today is mainly toward the rapid and simplified procedure and immediate loading of the implants. The concept of flapless surgery was then introduced to simplify immediate loading of prefabricated prosthesis and enhance the healing. The flapless surgical procedure has advantages of enhancing postoperative healing, less traumatic surgical procedure, and less damage to soft tissues. 4
The accuracy of implant placement using the computer-guided surgical stent has been checked by several authors in their studies. The conclusions of different authors suggest that the accuracy of implant placement and the survival rate of implants are much higher than those done through the conventional method. 2 , 4 , 5 , 8 , 10 The accuracy of the surgery requires the stabilization of the stent during surgery. For the teeth-supported computer-guided stent in a partially edentulous arch, accuracy is more compared with mucosa supported in a completely edentulous arch. 5 , 6 , 10
Several advantages of computer-guided stent-based implant placement include the preservation of soft tissues, optimum utilization of available hard tissues, less invasive surgical procedure, performing flapless surgery, and immediate loading of the implants. Some disadvantages of this procedure include the inability of a surgeon to visualize anatomic structure, osseous thermal damage because of obstructed external irrigation, and misplacement of implant relative to depth and angulation. 6 , 10 , 11
Conclusion
With the advancement in technology, the use of digital imaging and CAD/CAM technology in computer-guided implant surgery will enhance the functional and aesthetic requirement of the final prosthesis. Compared with conventional implantation techniques, the use of the computer-guided surgical stent will result in improved precision in terms of position, angulation, and depth of implant placement. The use of the computer-guided surgical stent for flapless implant placement has several advantages over the conventional method such as the optimum utilization of the available bone, placement of implant in the right position, enhancement of the healing process, less traumatic surgery, preservation of soft tissues, and immediate loading of the implants.