
Abstract
Aims and Objectives:
The oral microbial flora is highly complex and diverse with obligate anaerobic bacteria as the predominant component. Most of these are not yet cultivated/difficult to cultivate due to technical limitations. In this study, we aim to detect two novel oral bacterial species Dialister invisus and Olsenella uli by simplified and economical procedure of polymerase chain reaction (PCR) and study their association with primary and persistent endodontic infections.
Material and Methods:
The study involved 60 patients that included 30 patients of primary endodontic infections and 30 with persistent endodontic infections. The sample collection from the root canal was performed by universally accepted protocol by using sterile paper points. The deoxyribonucleic acid (DNA) extraction was done, followed by PCR with species specific primers. We made several changes to the protocol mentioned by original authors. We adopted a one-step protocol for amplification of bacterial DNA, omitting the 16SrDNA amplification step with universal primers.
Results:
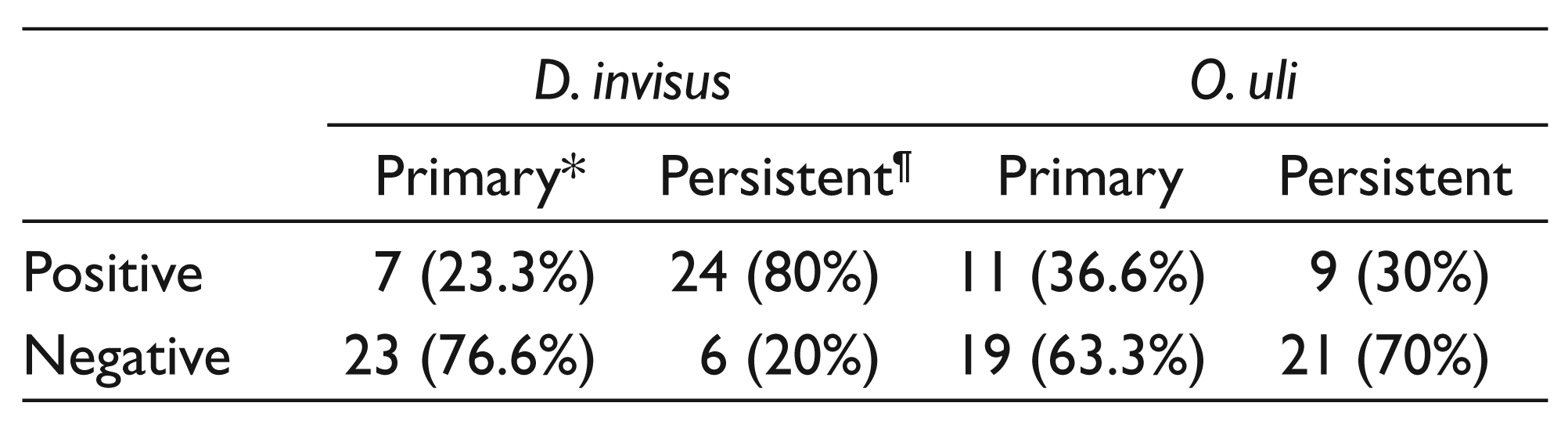
It was seen that 7 (23.3 %) samples in primary endodontic infection group and 24 (80 %) samples in persistent endodontic infection group were positive for D. invisus. On the other hand, 11 (36.6 %) patients of primary endodontic infection showed positivity for O. uli in comparison to 9 (30 %) of persistent endodontic infection.
Conclusion:
The results from the present study showed efficient amplification of both O. uli and D. invisus in a single-step PCR. Hence, we conclude that the modified protocol used here with taq polymerase enzyme offers a faster and cheaper alternative to nested PCR without compromising the quality of amplification process.
Introduction
The oral microbial flora is highly complex and diverse with obligate anaerobic bacteria as the predominant component. 1 The oral microbiome is made up of nearly 700 species, 2 but the recent estimation by some investigators have shown the number to be much higher, reaching approximately 1200 species. 3 Various studies have shown that nearly 50–60 percent of oral bacteria are yet to be cultivated and their presence in the oral cavity is deduced by using molecular techniques such as 16SrRNA sequencing and cloning.4–9
The physiological and pathogenic characteristics of most of these not yet cultivated/difficult to cultivate oral bacterial species is not known. It has been seen that many of these bacterial phylotypes are detected in periodontal and endodontic infections and dental caries. 10 Efforts are being made to cultivate these species in recent years. 11 In addition to 16SrRNA amplification and sequencing, checkerboard DNA–DNA hybridization also has been used to detect most of the microbes associated with endodontic infections.12–15 Studies have confirmed that bacterial diversity in endodontic samples detected by pyrosequencing is much greater than culture methods. 16 However, the involvement of these newly detected bacterial species in oral health and disease is not yet completely understood and needs to be studied.11,17
In this connection, we made an attempt to detect two novel oral bacterial species Dialister invisus and Olsenella uli by polymerase chain reaction (PCR) and study their association with primary and persistent endodontic infections. During the course of the study, we made several changes to the original protocol mentioned by Siqueira and Rocas. 18 The details of the procedure adopted are as follows.
Methods and Materials
The study was conducted over a period of 1 year that involved 60 patients that included 30 patients of primary endodontic infections (Group A) and 30 with persistent endodontic infections (Group B). Sample size was estimated based on the objective of detecting the differences in the proportions of microorganisms between the Groups A and B based on the results of the study obtained by Siqueira and Rocas. 18 The patients were in the age group of 18–40 years and belonged to both the sexes. Approval from the Institutional Review Board (Ref. No. 1046) was obtained before initiating the study. Informed written consent was obtained from each participant before enrollment in the study.
The sample collection from the root canal was performed by following universally accepted protocol. After isolating the tooth and sterilizing the area, the pulp chamber was accessed and fluid was sampled using three paper points, which was then placed in a vial containing Tris-EDTA buffer (TE buffer) and immediately transported to the laboratory. The deoxyribonucleic acid (DNA) was extracted from each sample using an in-house protocol with proteinase K. Briefly, the vials with paper points were centrifuged, the pellet was washed twice with TE buffer, treated first with 50 µl of lysis buffer I (1% Triton X-100, Tris-HCL pH 8.0 10 mM, and EDTA 1 mM), incubated for 5 minutes, followed by addition of 50 µl of lysis buffer II (Tris-HCl pH 8.0 50 mM, KCL 50 mM, MgCl2 2.5 mM, Tween-20 0.45%, and Nonidet P-40 0.45%), and 10 µl of proteinase K (100 µg/ml). The vials were then incubated in a water bath at 60°C for 2 hours followed by boiling for 10 minutes. DNA was then precipitated with 3 M sodium acetate and alcohol, reconstituted in 100 µl of water and stored at –20°C till use.
Initially, original nested PCR protocol devised by Siqueira and Rocas 18 was followed with universal DNA amplification of the extracted DNA in the first step followed by bacterium specific amplification in the second step. The only changes made were the use of Taq DNA polymerase in the master mix instead of Tth DNA polymerase enzyme in both the steps of amplification.
The positivity rate for both D. invisus and O. uli in both groups was very high with this protocol bordering around 90 per cent. Hence, it was decided to make several changes in the protocol. In the modified procedure, we adopted a one-step protocol for amplification of bacterial DNA, omitting the 16SrDNA amplification step with universal primers. The amplification was performed in a 25 µl reaction volume containing 2X Ampliqon Red master mix (Tris-HCl pH 8.5, (NH4)2SO4, 3 mM MgCl2, 0.2% Tween-20, 0.4 mM each dNTP, 0.2 units of ampliqon Taq DNA polymerase, and inert red dye and stabilizer), 12.5 pmole of each primer, and 5 µl of DNA extract.
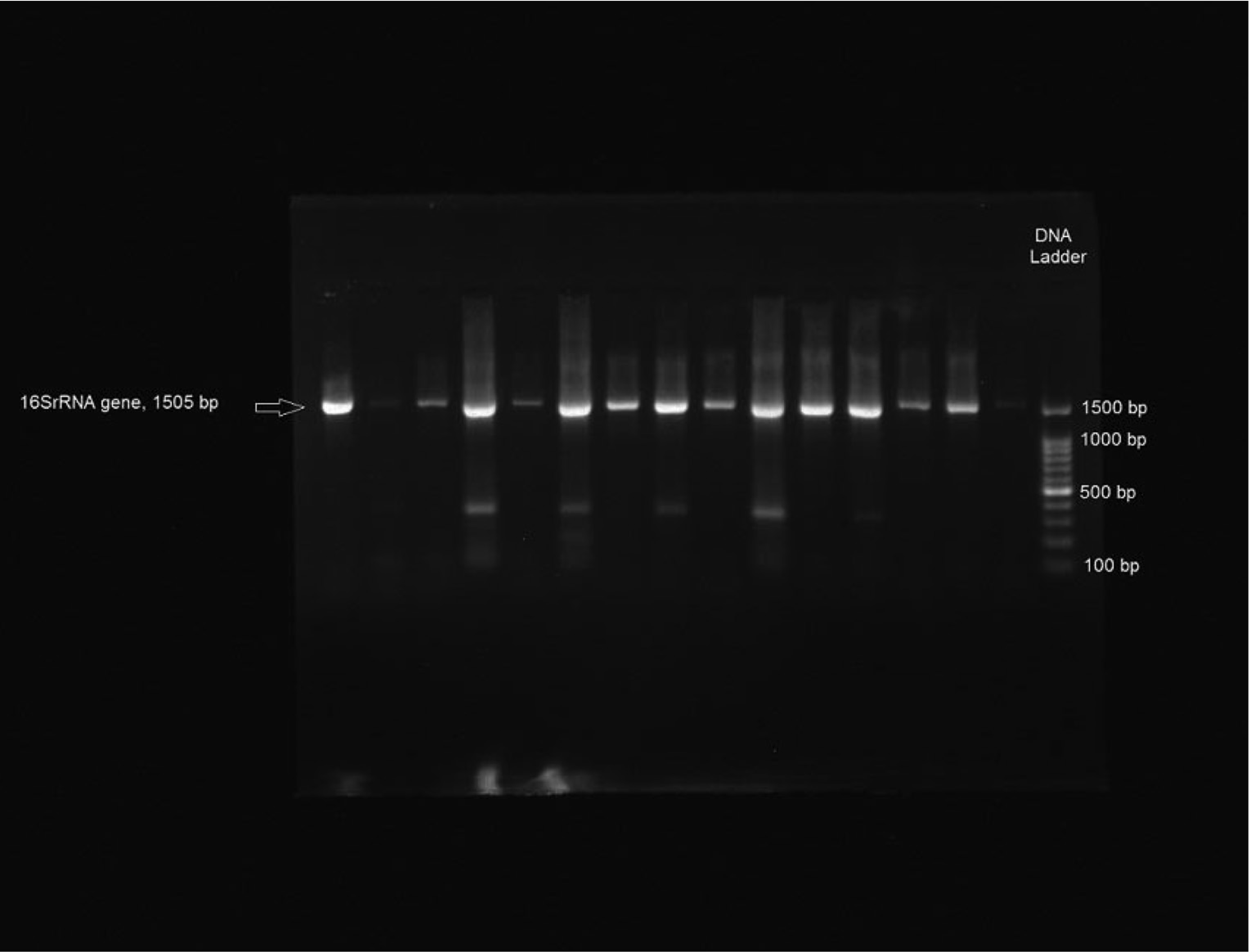
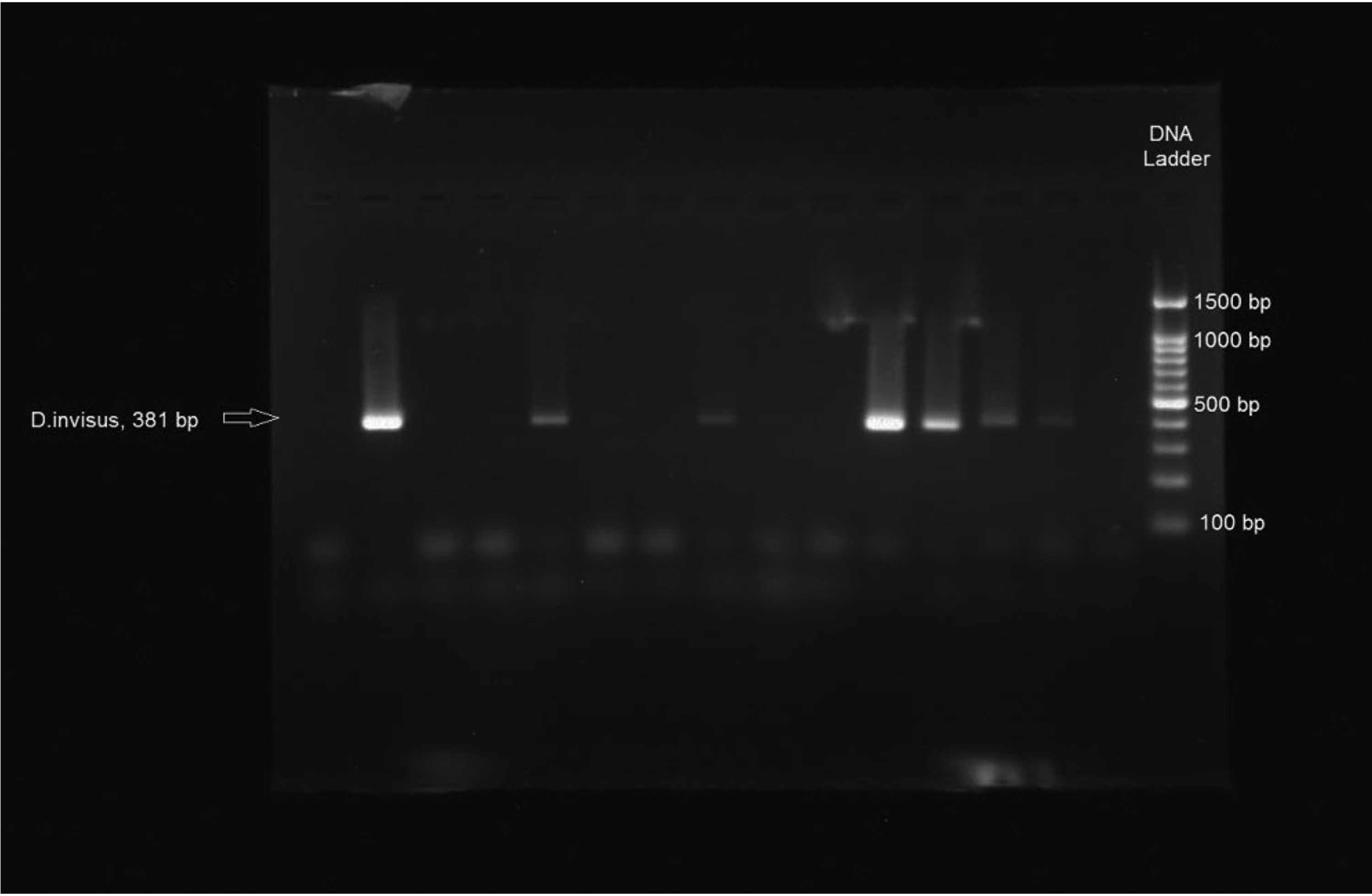
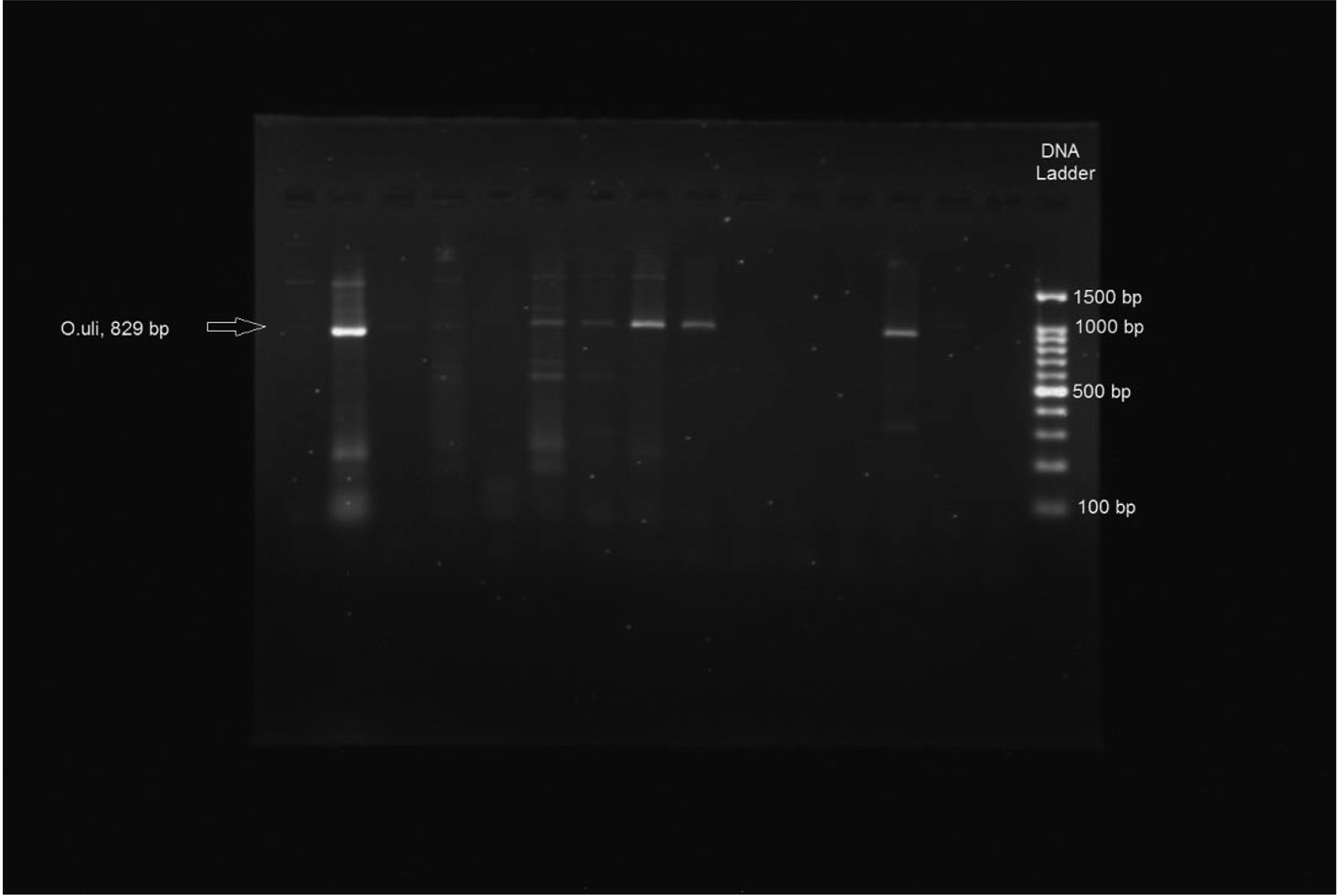
The PCR temperature profile for D. invisus included an initial denaturation step of 95°C for 5 minutes followed by 30 cycles each of denaturation at 95°C for 45 seconds, primer annealing at 68°C for 1 minute, extension at 72°C for 1 minute, and a final step of 72°C for 5 minutes. A similar temperature profile was used for O. uli except that an annealing temperature of 60°C was used for one minute. After amplification, the PCR products were separated by electrophoresis in 2 per cent agarose gel, which was stained with 0.5 µg/ml of ethidium bromide and viewed under UV transilluminator. A 100 bp DNA ladder was used as the molecular size standard. A band position of 381 bp for D. invisus and 829 bp for O. uli were considered positive.
Results
Initially, the original protocol optimized by Siqueira and Rocas 18 was used to detect the presence of D. invisus and O. uli in both primary and persistent endodontic infections. This included a two-step PCR process; first step being universal rRNA amplification (1505 bp region amplification using universal 16SrRNA primers) (Figure 1) followed by bacterium specific PCR with amplified DNA from the first round used as a template. However, using this method, it was seen that most of the samples studied from both the patient group showed high rate of positivity (13 out of 15) for both the bacteria studied. Even when the DNA template samples were diluted and tested with different concentrations of bacterium specific primers, the results remained the same.
This prompted us to change the protocol (as mentioned in the section titled Material and Methods) with single-step PCR amplification for both D. invisus and O. uli. After amplifying the bacterial DNA with the modified protocol, two different criteria were used to analyze the results. The absence of a band at specific location (381 bp for D. invisus and 829 bp for O. uli) was considered negative. The bands present at specific location were further allotted to three groups as bright, weak, and faint based on their intensity. Only the bright and weak bands at specific locations of 381 bp and 829 bp were considered to be indicative of the presence of D. invisus and O. uli, respectively. Very faint bands even though present at specific sites were considered negative (Figures 2 and 3).
Based on these criteria, it could be seen that 7 (23.3 per cent) samples in primary endodontic infection group and 24 (80 per cent) samples in persistent endodontic infection group were positive for D. invisus. On the other hand, 11 (36.6 per cent) patients of primary endodontic infection showed positivity for O. uli in comparison to 9 (30 per cent) of persistent endodontic infection (Table 1).
Discussion
A significant number of anaerobic bacteria from the oral cavity remain not yet cultivated or are difficult to cultivate. Their presence in various oral niches has been deduced by using molecular techniques such as 16SrRNA gene cloning and sequencing.19–22 Recently, efforts are being made to cultivate these bacteria by using novel techniques so that their role in oral health and disease could be better understood. Some of these bacteria include members of the genera Prevotella, Synegistes, Filifactor, Dialister, and Olsenella among others. 23 We selected O. uli and D. invisus for the present study because they have recently been cultivated and characterized,23–26 and efforts are being made to understand their role in oral infections. In addition, these two bacteria have been investigated recently by investigators in various endodontic infections and have been found to occur more frequently than many other novel bacteria.18,27–30
Apart from studying the prevalence of O. uli and D. invisus in primary and persistent infections, the major thrust of the present investigation was in technical aspects of the PCR methodology used. During the course of the investigation, several changes were made to the protocol followed by original workers. 18 In the present study, DNA extraction was performed by using an in-house protocol using proteinase K and extracted DNA was purified with alcohol and sodium acetate. We believe this would be much purer form of DNA and can be stored for a long time under freezing conditions when compared to the DNA extracted by boiling samples in distilled water, wherein DNA gets degraded in a short time. 31 The second major change was use of taq polymerase enzyme in a single-step PCR instead of nested PCR with Tth DNA polymerase. Tth DNA polymerase is a highly processive thermostable enzyme which is more commonly used in reverse transcriptase PCR, because it possesses good reverse transcriptase activity. In conventional PCR, its use is confined to making long PCR products. Otherwise, it has similar properties as that of taq polymerase including fidelity and lack of proofreading activity, but is expensive. 32 This enzyme was used in nested PCR probably because the size of the amplified products of first PCR involving 16srRNA universal primers was 1505 bp. In the present study, since PCR involved only one-step amplification with species specific primers and the size of the amplicons also was not long, we believe, the use of taq polymerase enzyme could be justified. In addition, adequate changes were made in the cycling parameters to suit the processivity of taq polymerase enzyme in the protocol here.
Detection of D. invisus and O. uli in Primary and Persistent Endodontic Infection
The results from the present study showed efficient amplification of both bacteria tested. This is probably the first study from India to assess the prevalence of D. invisus and O. uli in oral infections. The data show a very high prevalence of D. invisus in persistent endodontic infections compared to the primary group (80 per cent vs 23.3 per cent); in contrast, the prevalence rate of O. uli was slightly higher in primary endodontic infections than the persistent group (36.6 per cent vs 30 per cent). These results are somewhat different than other studies, where the prevalence rate is much lower in persistent infections in comparison to the primary group. 18
The major contribution of the study has been the designing of an economical and simplified protocol for detection of novel bacteria from oral infections. This approach also reduces the overall time needed for the whole procedure to just four hours. In addition, the other finding of the study includes detection of both D. invisus and O. uli in our subjects. The presence of D. invisus in very high percentage of persistent endodontic infection is an interesting finding and needs further exploration.
To summarize, we propose that the modified PCR technique mentioned here can be applied for the detection of novel bacterial phylotypes from oral infections. The occurrence of D. invisus and O. uli at a higher prevalence in our subjects with endodontic infection should be further explored by taking up more number of such studies with increased sampling size. The only limitation of the study was that no other technique was used for confirmation of the PCR results. We intend to compare several different molecular techniques with PCR in the ongoing studies to evaluate the specificity and sensitivity of each method in detection of novel oral bacterial phylotypes.
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
None.
Funding
None.