
Abstract
Objectives:
School dental screening and referral is a dental public health measure that helps children with oral health problems to come in contact with dental services. Recent studies have failed to demonstrate the effectiveness of school screening programs in stimulating dental attendance. The objective of the present study is to assess the effectiveness of school oral health screening in stimulating dental attendance and factors affecting dental attendance among female primary school children in Saudi Arabia.
Methodology:
A multistage cluster random sampling method was used in which the unit of randomization was the school. All children were given comprehensive oral health education followed by oral screening. Oral health referrals to visit dental clinic were given to children needing any dental treatment. The parents were contacted by telephone two months after oral health referral and information on child’s dental attendance and reasons for failing to attend dental clinics was collected according to predetermined set of questions and the data was subjected to statistical analysis.
Results:
A total of 1,035 female school children aged 6 to 12 years received oral health education at school followed by dental screening. Only 211 (23.8%) children attended dental clinics after receiving oral health referrals. The most important reason for not attending the dental clinic was difficulty for working parents to take time off (41.2%) followed by logistic problems (20.4%) and some parents thought dental treatment was not important since there was no pain (9.7%). The least perceived barriers were cost of dental treatment (3.6%), difficulty in taking leave from school (3%), and school exams (3%).
Conclusions:
School oral health screening and referrals have been found to be ineffective at stimulating dental attendance. Parental factors like ‘lack of time’ and ‘logistic problems’ for taking their child to the dentist were found to be major factors affecting dental attendance. Methods to improve parent’s awareness regarding oral health of children and alternative choices to ensure adequate dental care to vulnerable children needs to be explored.
Introduction
Good general health is not complete without good oral health. According to the World Health Organization (WHO), oral health is ‘a state of being free from mouth and facial pain, oral and throat cancer, oral infection and sores, periodontal (gum) disease, tooth decay, tooth loss, and other diseases and disorders that limit an individual’s capacity in biting, chewing, smiling, speaking, and psychosocial wellbeing.’ 1 Poor oral health has been directly linked with missing school time, loss of work hours and sometimes death in the case of oral cancers.2–4 Inequalities in oral health is continuing to increase, especially in developing countries.5–7 Government health policies are now focusing to reduce such inequalities in health.8–10
The common oral diseases like dental caries and periodontitis are multifactorial in origin and could be largely prevented.11,12 Unrecognized oral disease and postponed care might increase the severity of problem leading to pain, discomfort, and sometimes irreversible damage. 13 Chronic oral infections are now linked with systemic conditions and mortality rate.14,15 According to WHO, early detection of disease is crucial and lifesaving. A careful oral examination helps to identify not only oral diseases but also many general diseases including microbial infections, immune disorders, injuries, and cancers. 16 Public health screening is defined as ‘the presumptive identification of unrecognized disease or defect by the application of tests, examinations, or other procedures which can be applied rapidly.’ 17 Screening tests sort out apparently well persons who probably have a disease from those who probably do not. A screening test is not intended to be diagnostic. Persons with positive or suspicious findings must be referred to their physicians for diagnosis and necessary treatment.
School dental screening and referral is a dental public health measure that helps children with oral health problems to come in contact with dental services. For any screening program to be supported, strong evidence is required to demonstrate its effectiveness. Several studies conducted have found school dental screening and referral programs to be effective in stimulating attendance.18–20 There are laws in several states in the USA mandating dental screening of school-aged children before school entry. 21 More recent studies in the UK have failed to demonstrate the effectiveness of screening and formal criteria for referral process in increasing rates of follow-up care.22–24 Furthermore, a recent systematic review and meta-analysis of randomized controlled trials on the effectiveness of school-based dental screening confirms that there is no evidence to support or refute the clinical benefits or harms of dental screening. 25 This conflicting evidence raises financial and ethical concerns on continuing school dental screening programs. Thus, it becomes imperative to understand the factors responsible for poor dental attendance following a school dental screening program.
King Khalid University, College of Dentistry (KKUCOD), is one of the renowned dental institutions in Saudi Arabia providing dental care for nearly about two decades. Reflecting the institution’s mission of community service, it regularly conducts school outreach programs. Currently, there is no available research on effectiveness of school oral health screening in the Kingdom of Saudi Arabia. It is generally believed that females are more concerned about their oral health. A research on dental attendance pattern among children have found that girls had significantly more dental visits than boys. 26 Since the educational system in Saudi Arabia is exclusive for both genders and due to administrative restrictions, we decided to study them first. A similar research will be conducted in future to study and compare the male children counterparts. Therefore, the objective of the present study was to assess effectiveness of school oral health screening in stimulating dental attendance and factors affecting dental attendance among female primary school children in Saudi Arabia.
Methodology
The present cross-sectional survey was conducted among female primary-school-going children in Abha-Khamis, Saudi Arabia. The ethical clearance was obtained by the institutional review board of KKUCOD (SRC/ETH/ 2016–17/050).
A multistage cluster random sampling method was used in which the unit of randomization was the school. In the first stage, a list of all female primary schools in Abha and Khamis cities was obtained from the Ministry of Education, Saudi Arabia. KKUCOD where the present study was carried out is located in the city of Abha. The second city, that is, Khamis (which is 30 km away from the first), was included to find out whether distance of dental service and residence has a role in stimulating dental attendance after oral health referral. Two schools from each city were selected randomly and all children from the selected schools were considered for the study. An official permission for carrying out the study was obtained from all concerned school authorities. All children were given comprehensive oral health education followed by oral screening using WHO Oral Health Assessment Form, 2013 by trained examiners. 27 The outcome variables were measured dichotomously in terms of presence and absence of the condition. The inter-examiner agreement was found to be 100 percent. Oral health referrals to visit dental clinic at KKUCOD were given to children needing any dental treatment. The referral sheets carried a note for parents informing about the treatment required including contact details.
In the second stage, telephone numbers of respective parents were collected from school authorities. The parents were contacted by telephone two months after oral health referral from schools and information on child’s dental attendance and reasons for failing to attend dental clinics was collected according to predetermined set of questions. All parents were informed about the purpose of research and their consent for participation was obtained before asking questions. The information collected during the telephone call was simultaneously entered into the computer (MS Excel) for further statistical analysis.
Results
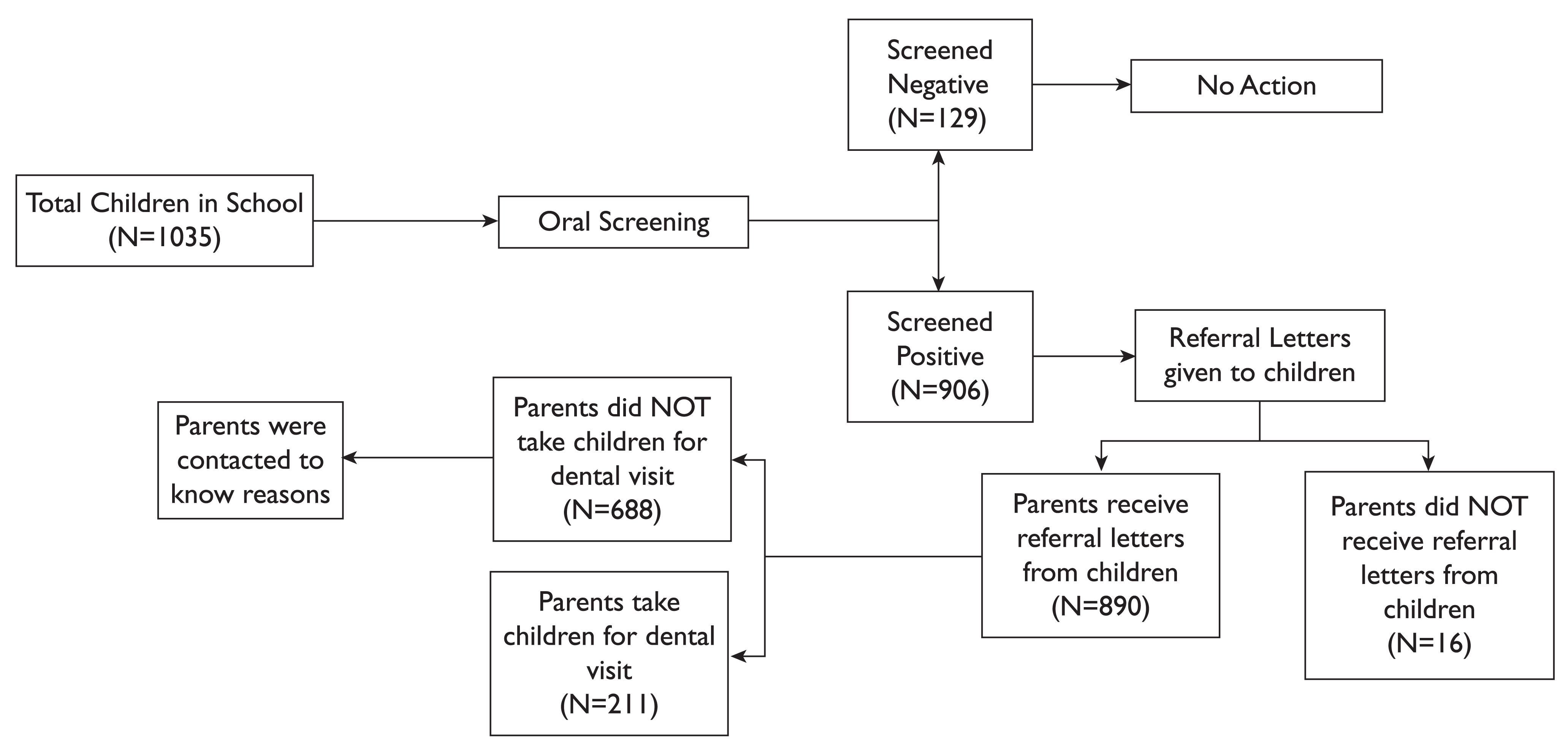
A total of 1,035 female school children aged 6 to 12 years received oral health education at school followed by dental screening. Out of total children screened, 906 children had positive oral health findings and received oral health referrals to outpatient dental clinics of KKUCOD. 16 parents said they did not receive any referral forms. A total of 890 parents agreed to participate in the study (Figure 1). Approximately equal number of children from short and long distance places (51.9% and 48.1% respectively) were given oral health referrals. Only 211 (23.8%) children attended dental clinics after receiving oral health referrals. The children visiting dental clinic from long distance places were higher than those visiting from short distance places (p < 0.05). However, the children who did not visit dental clinic were higher from short distance places than those from long distance places (p < 0.05; Table 1).
A Schema of School Dental Screening Process
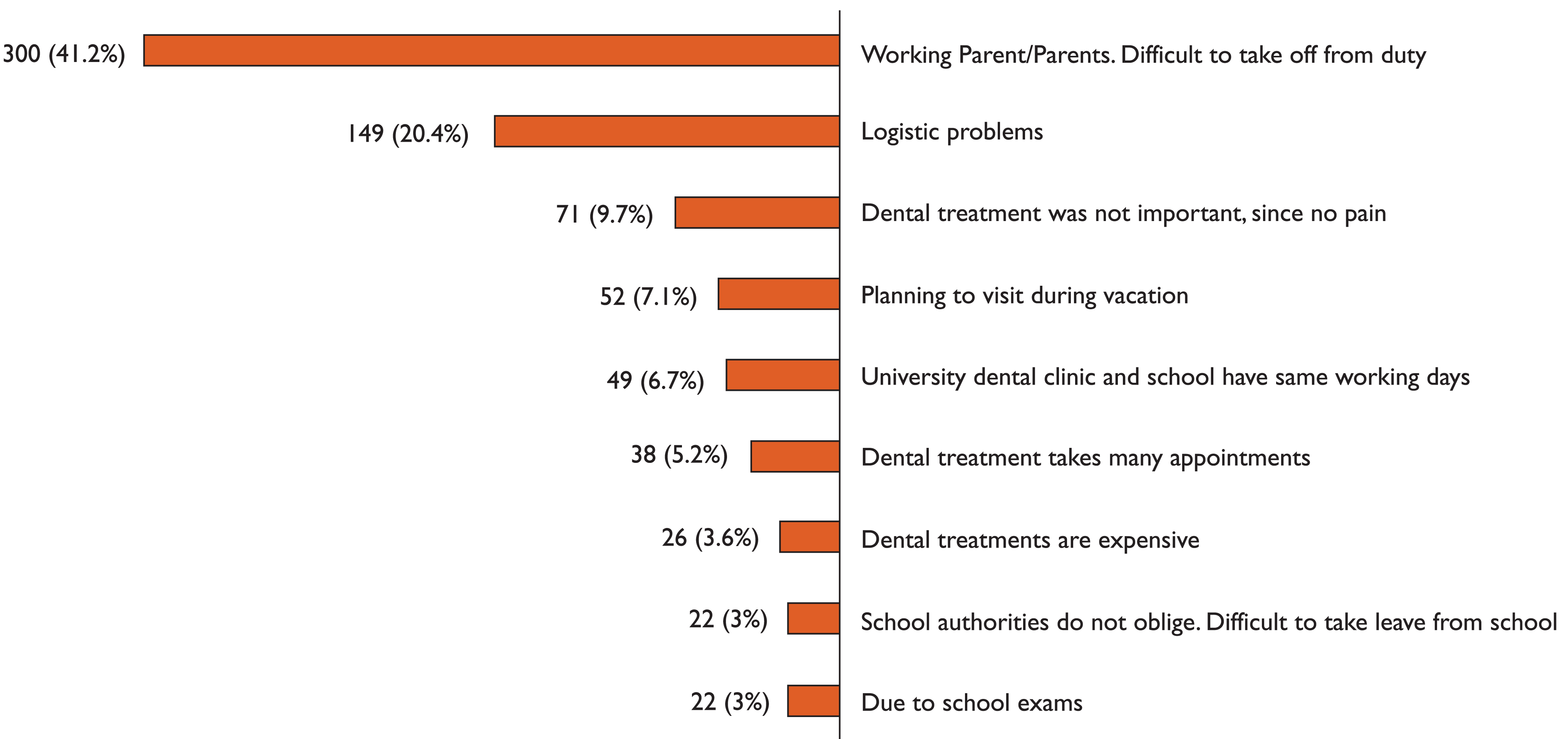
The most important reason for not attending the dental clinic was difficulty for working parents to take time off (41.2%) followed by logistic problems (20.4%) and some parents thought dental treatment was not important since there was no pain (9.7%). The least perceived barriers were cost of dental treatment (3.6%), difficulty in taking leave from school (3%), and school exams (3%) (Figure 2).
Discussion
This present study was conducted to determine the effectiveness of school oral health screening in stimulating dental attendance and factors affecting dental attendance among female primary school children in Saudi Arabia. The dental attendance in our study was found to be 23.8 per cent. Similar studies in the past have shown a high variation in dental attendance ranging from as low as 14 per cent to as high as 97 per cent where the target population were from a low socioeconomic status group.18,23 This high variation in results indicates that a multitude of factors are responsible in stimulating dental attendance.
In our study, the major factors for non-attendance were ‘lack of time’ (41.2%), that is, for parents of participants to take time off from duty and get their wards to dental clinic and ‘logistic problems’ (20.4%). Many other studies have found similar factors affecting dental attendance.28,29 Dental treatments require multiple appointments which could be another reason for parents reluctant in taking time off from duties. Some parents (6.7%) in our study said that reason for not attending dental clinic was overlap of working hours between parents, schools and dental clinics at KKUCOD. However, parents even failed to visit private dental practice which are operating at after school hours, in the present study. Majority (42.5%) of non-attendees in our study was from children residing close to KKUCOD dental clinics. Some cultural barriers in Saudi Arabia include logistic difficulties for non-working mothers, especially in absence of male family members or drivers.
Dental Attendance Following Referral from School Program

Usually, dental health is perceived to be of less priority than general health. Some parents in our study did not attend dental clinic since the child had no acute symptom like pain. Parent’s awareness and knowledge about their child’s oral health have shown to influence the parent’s compliance to dental visits for their children. 30 The cost of dental treatment was least perceived as a barrier in our study. Although dental services are provided for free at public health care facilities in Saudi Arabia, several studies elsewhere have confirmed the importance of financial barriers in utilization of dental services.31,32 Poor dental attendance in our study could be due to the fact that parents were not followed up immediately after dental screening at school. Researches have shown increased dental attendance by intensive follow up of non-respondents.19,33
Factors for non-attendance might not be relevant for the same population, for example, dental anxiety, cost of dental treatment, self-perception of dental need, educational level, lack of access to dental services, and so on could be important barriers in adult population, while for younger children their barriers to dental care will be affected by parental attitude and anxieties. The literature suggests that several factors are responsible for children not visiting the dentist and many of them have proven to be difficult to modify. 20 Many institutions in Saudi Arabia conduct regular school dental screening programs. A low dental attendance rate in our study raises ethical and financial concerns about continuing to provide ineffective screening programs. The concerned dental professionals and government policy makers will need to consider overcoming the possible barriers during planning school screening programs. Ideally, for any school dental screening program to be effective and reduce the burden of untreated dental disease in the population, all positive-screened children not only need to visit the dentist but also seek comprehensive treatment. Our study was restricted to finding the dental attendance rate after the school oral health referrals. A further study is required to explore the effectiveness of such screening programs with intensive follow up with parents and treatment status of the child.
Conclusions
School oral health screening and referrals have been found to be ineffective at stimulating dental attendance. Parental factors like ‘lack of time’ and ‘logistic problems’ for taking their child to the dentist were found to be major factors affecting dental attendance. Methods to improve parent’s awareness regarding oral health of children and alternative choices to ensure adequate dental care to vulnerable children needs to be explored.
Footnotes
Acknowledgements
The authors thank all children who participated, school authorities for allowing the study to be carried out and the parents of children for showing their perseverance towards this study.
Declaration of Conflicting Interest
None.
Funding
None.