
Abstract
Aims and Objectives:
Improving maternal knowledge plays a major role in developing good oral health habits and in preventing diseases like early childhood caries in their children. The present study is aimed to provide pregnant women with the anticipatory guidance and to evaluate its effect on promoting the knowledge and attitude of pregnant mothers regarding infant and toddler’s oral health care.
Material and Method:
In this interventional study, 600 pregnant women attending government hospital, Madurai, were divided into direct intervention, indirect intervention, and control groups. A self-reported questionnaire was completed before intervention. The anticipatory guidance was presented to the direct intervention group by PowerPoint and to the indirect group by pamphlets. Immediately after the intervention, the questionnaire was completed by intervention groups and two months later by all participants. Chi-square test was used for statistical analysis at a significance level of 0.05.
Results:
The change of scores in the knowledge and attitude of pregnant women had a significant difference in all the three groups. At the end of the study, a statistically significant difference (p < 0.05) was noted in the knowledge between the intervention and the control groups. The change in the attitude was not statistically significant.
Conclusion:
Anticipatory guidance led to change in the score of knowledge about infant and toddler’s oral health in intervention groups compared to control group. The direct presentation had superiority over indirect presentation in increasing knowledge about their oral health care. Dentists should do their utmost to educate parents especially the pregnant mothers on children’s oral health in a culturally and linguistically appropriate manner, as oral health literacy is, ultimately, a pathway to health equity.
Introduction
A child’s oral health begins in utero. Bacteria causing early childhood caries (ECC) are easily transmitted from parents/caregivers to child and when left untreated can lead to pain, infection, as well as difficulty in eating, speaking, and even learning.[1 These difficulties can have effect on cognitive development, school readiness, and self-esteem, thus reducing the child’s quality of life. The effects of ECC, including an increased risk of caries in the mixed and permanent dentition, often persist into adulthood.[2 In a society where mothers play a significant role in rearing their children, it is important to instill the education on anticipatory guidance regarding infant oral health care when they are expecting a baby.
Anticipatory guidance, as defined by Nowak and Casamassimo[3 is the “process of providing information about the children to their parents by alerting them to impending changes, teaching them their role in maximizing their children’s developmental potential, and identifying their children’s special needs.”
Most of the pregnant women get no instructions during their pregnancy regarding oral health; even though pregnancy is a phase of increased acceptance of instructions that should be used as an opportunity to introduce preventive programs.[4 Improving maternal knowledge plays a major role in preventing ECC and in developing good oral health habits in their children.[5 Therefore, the best time to start these informative programs is the prenatal period. Those parents who are expecting the birth of their child, especially their first, will welcome the preventive advice the most.[6
Few studies have explored the effects of oral health education on pregnant women.[6-8 The results of these studies indicate that the presentation of anticipatory guidance led to the increase in the knowledge about maternal, infant, and toddler’s oral health care. Cardenas and Damon evaluated the gain in knowledge of oral health after pregnant women were educated about it, and they reported an improvement in knowledge after a 10-minute presentation on dental anticipatory guidance immediately and after a month.[9
Keeping in mind the importance of measuring the knowledge and attitude of pregnant women related to infant and toddler's oral health care and lack of studies carried out on this issue in this particular population, the present study is aimed at providing pregnant women with an anticipatory guidance and evaluating its effect on promoting the knowledge and attitude of the pregnant mothers regarding infant and toddler's oral health care.
Materials and Methods
An interventional study was carried out among the pregnant women attending the government hospital, Thirumangalam, Madurai, to assess the effectiveness of the anticipatory guidance presentation on improving the knowledge and attitude of the pregnant women related to infant and toddler’s oral health care. The ethical clearance (BDSC/13-7-15) was obtained from the institutional review board, Best Dental Science College, Madurai. Informed consent was obtained from all the study subjects. The study population includes pregnant women attending government hospital, Thirumangalam, Madurai, during the months of May 2015–August 2015.
Pregnant women who have the ability to read and write in the local language were included in the study. The questionnaire was prepared in English and translated in the local language Tamil by a bilingual speaker. The questionnaire was tested for face validity by a panel of “experts” and modified in accordance with their recommendations to ensure comprehensive ability. A pilot study was carried out with 15 subjects in order to test items’ understandability and content validity. The internal consistency was assessed by Cronbach’s α. The results of the pilot study showed a good consistency with α values higher than 0.9.
Pregnant women attending the government hospital, Thirumangalam during the month of July 2015–August 2015 were randomly allocated to three groups. Separate sheets with specific code were put in envelopes, and each subject was asked to select one of it. They were then allocated to one of the groups, according to the codes written in the envelope. Data collection was done through self-reporting questionnaire. The questionnaire contained demographic data which included age, educational qualification, period of gestation, and gravida status.
The prepared questionnaire in Tamil was filled by all the participants. After completion of the questionnaire, the anticipatory guidance was prepared according to the baseline knowledge of the participants and was pretested before imparting it to the main study. The content of the guidance was prepared by the specialists in pediatric dentistry and gynecologist based on nurses’ guide to anticipatory oral health guidance for children.[10-17 The scoring criteria for the questions were done quantitatively based on an arbitrary scaling. The participants were grouped based on the number of questions answered correctly.
For the knowledge-based questions, the participants were grouped into three as:
0–7 questions—poor; 8–14 questions—good; and 9–22 questions—very good.
For the questions based on the attitude, the participants were grouped into three as:
0–1 question—poor; 2 questions—good; and 3–4 questions—very good.
The prepared guidance was then delivered to each member of the intervention groups. The guidance was presented face-to-face using a 15-minute PowerPoint presentation for the participants in the direct intervention group, whereas for the indirect intervention group, pamphlets were used. No intervention was given to the participants of the control group.
The members of the indirect intervention group were given enough time to read the pamphlets in the hospital before collecting them back. Shortly after the presentations, the same questionnaire was filled out by the participants in the intervention groups. After a waiting period of two months, all the participants (intervention and control groups) were asked to fill the same questionnaire. In accordance with the ethical guidelines, at the end of the study, the prepared pamphlets were given to all the participants of intervention and control groups and all questions asked were answered.
Data analysis was done using SPSS, version 20 software. Using this software, significance of difference between variables was calculated using Yate’s and Fisher’s chi-square tests. A p-value less than 0.05 is taken to denote significant relationship.
Results
A total of 600 pregnant women were included in this study; 590 women remained throughout the study. Sociodemographic data revealed that the mean age of the pregnant women was 24.06 in direct intervention group, 22.58 in indirect intervention group, and 24.09 in the control group. The age of the participants in the groups ranges from 19 to 33 years. In terms of education, 14.9 per cent (n = 89) of women are graduate or postgraduates; 11.7 per cent (n = 70) had intermediate/post high school diploma; 41.5 per cent (n = 249) women finished their high school certificate; 18.1 per cent (n = 108) women finished middle school certificate; and 13.9 per cent (n = 83) had primary school certificate. In terms of trimester of pregnancy, 17 per cent (n = 103) of the women were in their first trimester of pregnancy; 23.4 per cent (n = 140) in their second trimester; and 59.6 per cent (n = 357) of the pregnant women were in their third pregnancy. In terms of the gravida status, almost 51 per cent (n = 306) were having their first baby; 39.4 per cent (n = 236) women were in their second pregnancy; and only 9.6 per cent (n = 58) women were expecting their third baby.
Comparison of Knowledge Levels before Health Education and after Health Education in Pamphlet Group and PowerPoint Group
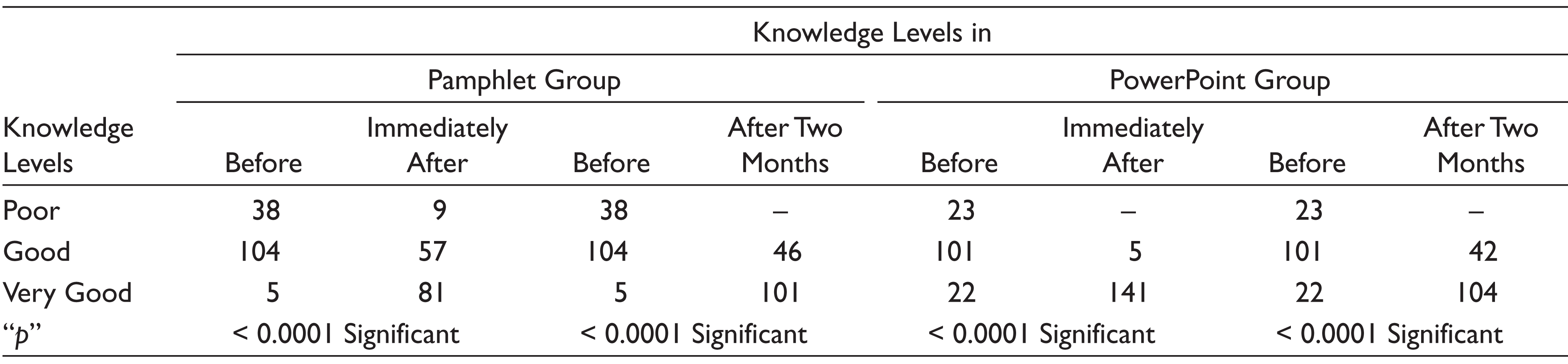
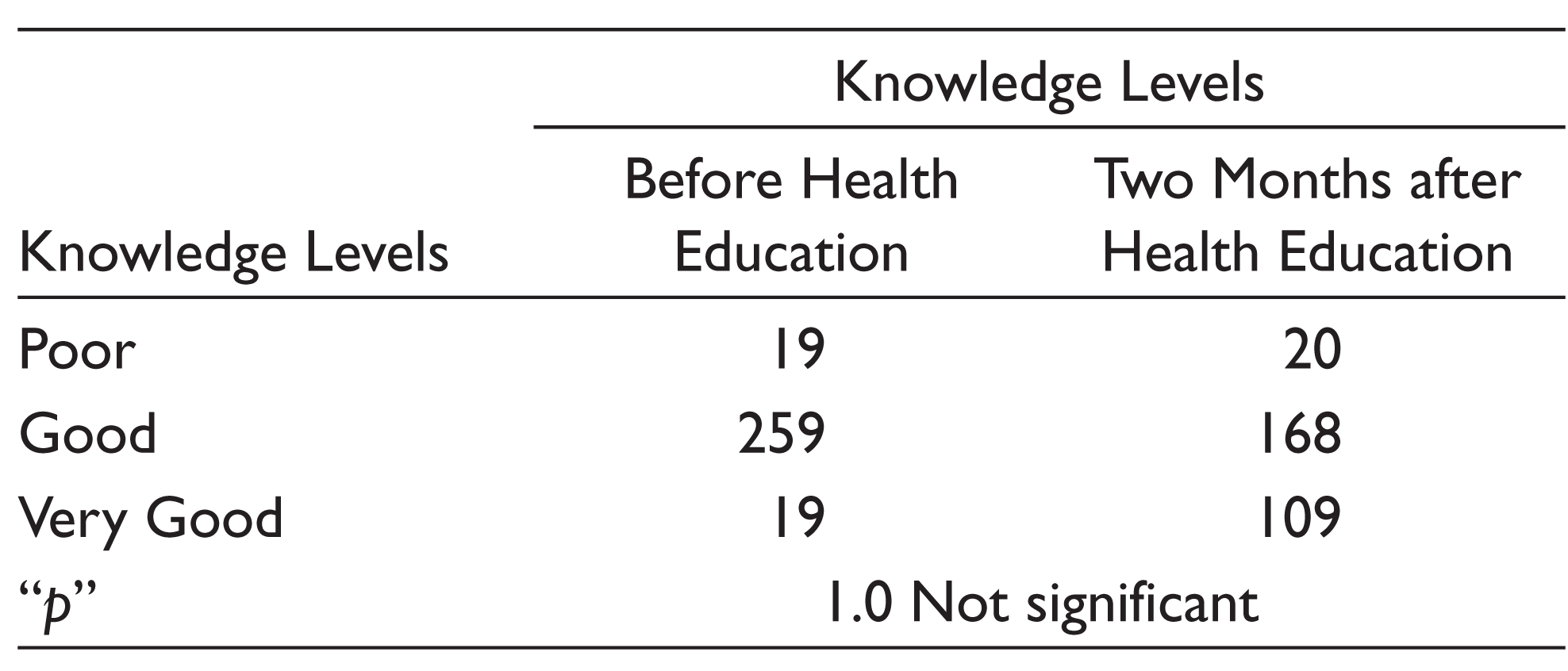
The knowledge level was compared before health education and after health education in the experimental groups (pamphlet and PowerPoint groups). The increase in the knowledge before and immediately after health education was statistically significant in both the experimental groups (p < 0.0001). The increase in the knowledge before and two months after health education was also statistically significant in both the experimental groups (p < 0.0001; Table 1). While comparing the knowledge levels before and two months after health education in the control group, there was an increase in the knowledge of the participants. But this increase in the knowledge was not statistically significant (p = 1.0; Table 2).
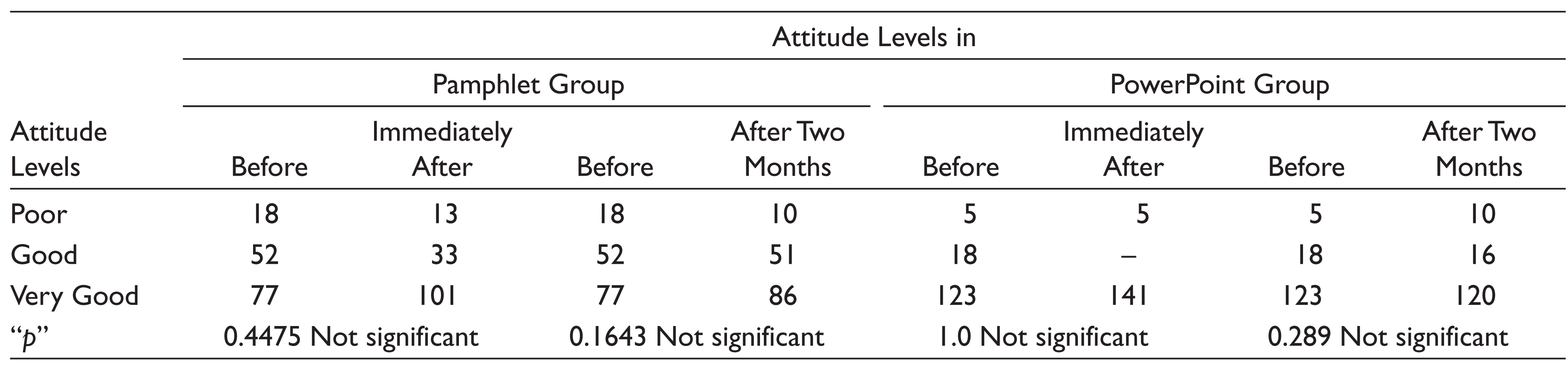
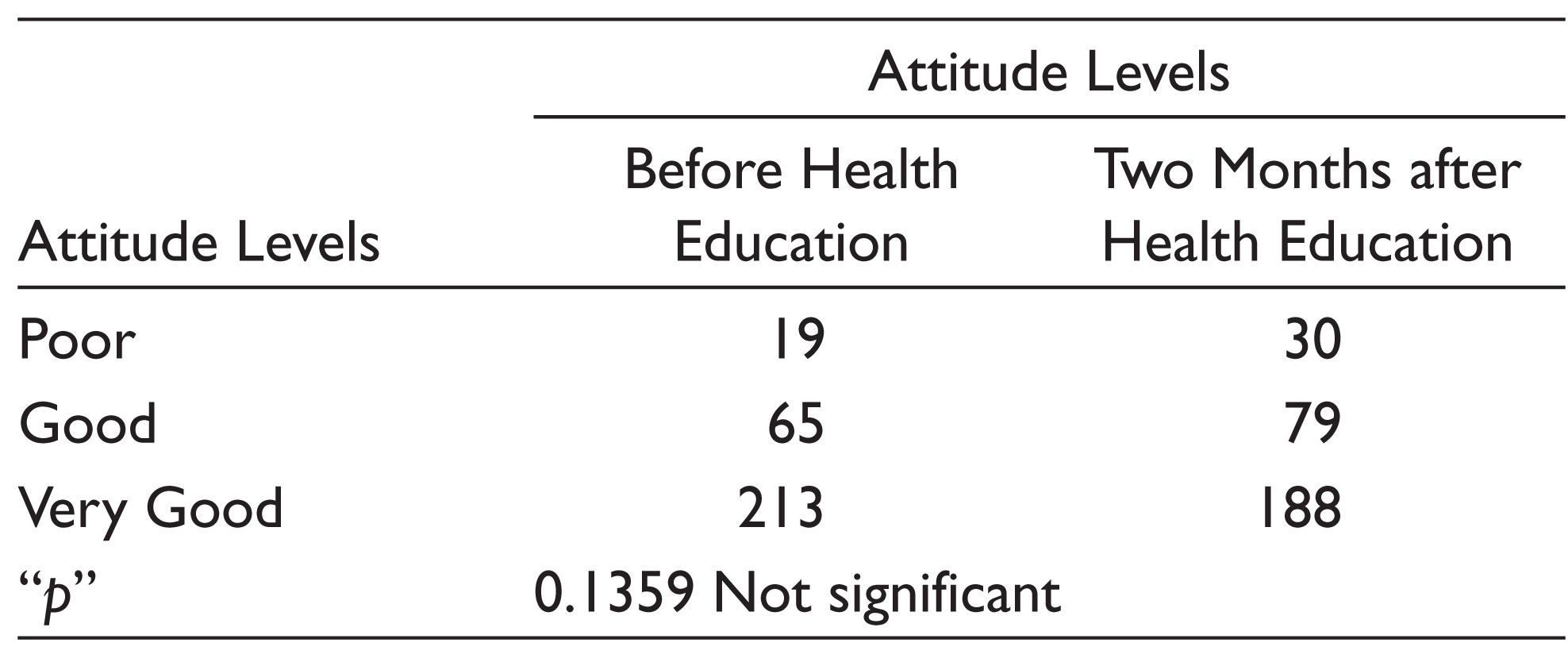
The attitude level was compared before health education and after health education in the experimental groups (pamphlet and PowerPoint groups). The increase in the attitude levels before and immediately after health education in the pamphlet group was not statistically significant (p > 0.05). The increase in the knowledge before and two months after health education was also not statistically significant in both the experimental groups (p > 0.05; Table 3). While comparing the attitude levels before and two months after health education in the control group, there was a decrease in the participants in the “very good” group. But this is not found to be statistically significant (p = 0.1359; Table 4).
Discussion
An intense early intervention using early preventive strategies starting during pregnancy proved to be efficient in preventing oral diseases.[7 Training pregnant mothers is one of the effective approaches to promote infant and toddler’s oral health care.[4 Pregnancy is an opportune time to provide health education as women (particularly primiparous women) are most receptive to and interested in receiving information, especially if it relates to the health of their infant.[18 Health education programs given to women during the prenatal period and the first years of children’s life may give a positive attitude to dental care and improve the oral health of the child.[19
Comparison of Knowledge Levels before Health Education and after Health Education in Control Group
The results of this study demonstrate that anticipatory guidance targeting pregnant women was effective in increasing the knowledge and attitudes of these pregnant women regarding infant and toddler’s oral health care. There was a significant increase in the knowledge levels between the experimental and control groups after the health education.
Comparison of Attitude Levels before Health Education and after Health Education in Pamphlets Group and PowerPoint Group
Comparison of Attitude Levels before Health Education and after Health Education in Control Group
Lin et al.,[8 in their study, observed improvement in the knowledge of oral health and positive tooth cleaning behaviors after a dental public health program, which is consistent with the results of our study. In the present research, a comparison of the results at the beginning and at the end showed a significant difference between the increase in the knowledge and attitude levels in the direct intervention group, which implies that the educational program was positively influential when given directly.
Cardenas and Damon,[9 in their study, offering anticipatory guidance through PowerPoint display, found out that the knowledge of the examined population about oral health advanced within four weeks, which is consistent with the findings of the present study. The direct and the indirect intervention groups were significantly different from one another and the control group, which particularly showed the positive influence of direct intervention in changing the knowledge of the pregnant women. In line with the findings of the present study, Bahri et al.[7 found a significant difference between scores of knowledge achieved by the control and the intervention groups at the end of their study.
There was no significant difference observed in the attitude between the intervention groups shortly after intervention and among the three groups at the end of the study. This was consistent with the study conducted by Ramazani et al.[5,6 On the contrary, Bahri et al.[7 reported a significant difference between scores of attitude achieved by the control and the intervention groups at the end of the study. This discrepancy might have originated from several contributing factors including sample size, type of intervention, and the education method. The change in the attitude in this study was not affected by the method of intervention. This inadequate change may be due to the short study period of two months. In other words, only longer time spans can properly show the effect of the education method on changed attitude scores.
In the present research, two education methods were employed by one person, and the materials taught were the same. The other strength of this study was allocating a control group to which intervention groups could be compared. Although the sampling was done randomly and each eligible pregnant woman attending the health center had equal chance to enter the study, the final results could not be generalized to the entire population of the pregnant women, because many of them might have chosen to visit other facilities, including private offices, which can probably influence individuals’ willingness to accept the training. Furthermore, unknown traits such as socioeconomic status, family income, and previous oral problems may have confounded the results. The other restriction was that 10 individuals were not accessible at the end. Nevertheless, our study can be regarded as one of the few studies examining education methods to deliver the guidance during pregnancy. Considering the restrictions, conducting a study to evaluate the long-term progress of changes in variables is suggested. In such a study, the effects of other education methods of oral health care can be examined.
Conclusion
Based on the results of the present study, presentation of the anticipatory guidance through direct and indirect methods led to the change in the knowledge and attitudes of pregnant women in a two-month period. In addition, direct presentation of this guidance was found to be more effective over the indirect presentation in increasing the knowledge of pregnant women.
Recommendations
This represents a low-cost intervention that was fully integrated into the functions of primary health centers.
This educational method could be applied to children of other ages.
Repeated reinforcement of the guidance is advisable over a shorter time span.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interest
We declare that there is no conflict of interest.
Funding
None.