
Abstract
Aims and Objectives:
To assess the effect of exposure to arsenic by drinking water and caries prevalence in children.
Material and Methods:
A total of 200 children between 10 to 14 years of age, 100 each from study village (Hutti, Raichur district, Karnataka) and control village (Sanduru, Bellary district, North Karnataka) were included in the study. Water samples from both the villages were analyzed for arsenic levels. Arsenic levels were determined in the hair and nail samples from the subjects to assess chronic arsenic exposure. Caries experience was measured by the DMFT/deft index and the severity of caries was measured by modified ICDAS-II index.
Results:
The mean concentration of arsenic in the study group was found to be 2.44 ppm in the hair samples and 2.72 ppm in the nail samples as compared to 0.12 ppm in both hair and nail samples in the control group. These values were statistically significant (p < 0.001). The mean DMFT score in the control group was 0.99 and in the study group was 2.45, which was statistically significant (p < 0.05) using SPSS version 21.
Conclusion:
Chronic arsenic exposure could be a possible cause for the increased caries experience in children in the study group.
Introduction
Arsenic is a rare crystal element that naturally occurs in all environmental media—earth crusts, sediments, soil, water, air, and living organisms. It has been used in various fields, such as, electronics, medicine, agriculture, livestock, industry, and metallurgy. 1 However, today it is ranked first amongst toxic agents, posing a significant threat to human health. 2 Chronic arsenic exposure, especially via the consumption of contaminated groundwater has farreaching consequences on human health. It affects fetal development, malignancies, and dermatological diseases. 3 Groundwater contaminated with arsenic has become a major public health concern worldwide, affecting 150 million people in more than 70 countries including Mexico, the USA, Taiwan, Mongolia, India, Chile, and Bangladesh. 4
In India, groundwater contamination of arsenic was first reported in four districts of West Bengal in the year 1983. 5 The earliest places with groundwater arsenic contamination in Karnataka were identified in the villages of Yadgir district in 2008. Since then, UNICEF and Government of Karnataka have discovered several villages with groundwater arsenic levels exceeding 10 μg/L (World Health Organization [WHO guideline value). 3 One such village is the Hutti village in Raichur district. There is a naturally occurring belt of metamorphic rock called the Hutti–Maski schist belt in this area that is rich in minerals like arsenopyrite. This belt has three active gold mines. These gold mines contribute to arsenic contamination of the groundwater. Arsenic is introduced into soil and groundwater during weathering of rocks and minerals followed by subsequent leaching and runoff. 6
Several studies have been done to find out the effect of arsenic on the general health of people. However, information on the effect of arsenic exposure on oral cavity is very limited. Hence, this study was carried out to study the effects of arsenic on caries experience in children of Hutti, a small village in the district of Raichur, North Karnataka.
Methods
A small village Hutti, Raichur district, North Karnataka was selected as the study village based on the UNICEF’s list of villages in Karnataka contaminated by arsenic. A control village, Sanduru, Bellary district, North Karnataka, that was not included in the UNICEF’s list of villages affected by arsenic contamination was selected based on the similarity of population and general demographic characteristics. This cross-sectional study was carried out between December 2015 and June 2016. Water samples were collected from both the villages for the analysis of arsenic content using atomic absorption spectrometry. A total of 200 children 3 between 10 to 14 years of age, 100 each from study and control villages were included in the study. Sample size determination criteria by the following formula for sample situation was:
where, Z = z score = 1.96, d = acceptable level of error = 0.10, p = the anticipated population affected by arsenic was set at 50% i.e. 0.5 because of available literature does not provide any estimation of the anticipated prevalence rate. Participation in the study was voluntary. Ethical clearance was obtained from the review board of the institution with the certificate no. ABSM/EC/5/2015 and written informed consent for the same was obtained from parents of the children. Information on the personal characteristics and drinking water source was gathered from the parents.
Children who were born and brought up in the respective villages were included in the study and children who had moved to the village in the last five years or children not having water from the common water source were excluded from the study.
Arsenic levels were also analyzed in the hair and nail samples of all the children using atomic absorption spectrometry and inductively coupled plasma optical emission spectrometry, respectively.
A single, skilled postgraduate student with the help of a mouth mirror and a probe carried out oral examination. Oral hygiene status was assessed using simplified oral hygiene index (OHI) by Greene and Vermillion, 1964. Caries experience of a child was recorded using the DMFT/deft index by Klein, Palmer, and Knutson in 1938 and modified by the WHO. A detailed assessment of the stage of caries lesion progression was done using the modified ICADS II.
Mann–Whitney U test was done to compare the arsenic levels in the hair and nail samples, oral hygiene scores, DMFT and deft scores, and the progression of dental caries (modified ICDAS-II scores) in both primary and permanent dentition between the children in the two groups.
Result
The level of arsenic found in groundwater of Hutti village was 90 μg/L, much higher than the WHO standard of 10 μg/L. Arsenic was not detected in the groundwater of Sanduru village. The fluoride levels in both the groups (Table 1) were within the permissible limits.
The mean concentration of arsenic in the study group was found to be 2.44 ppm in the hair samples and 2.72 ppm in the nail samples as compared to 0.12 ppm in both hair and nail samples in the control group. These values represent a statistically highly significant increase in arsenic levels in the study population (p < 0.001).
Oral Hygiene
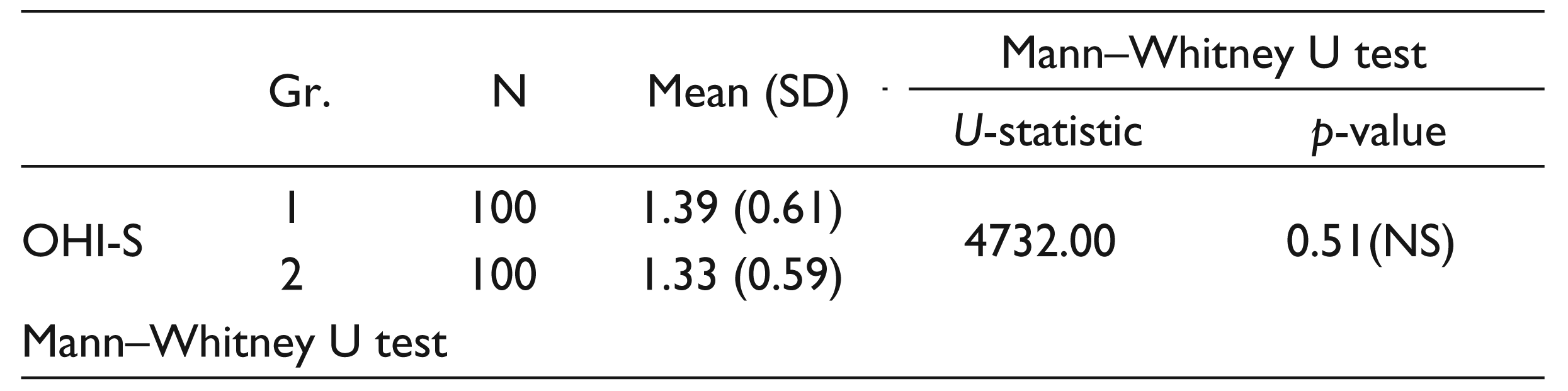
The oral hygiene of children in both study and control group was found to be fair. No statistical significance was found in the OHI-S scores in both the group.
Dental Caries
DMFT/deft
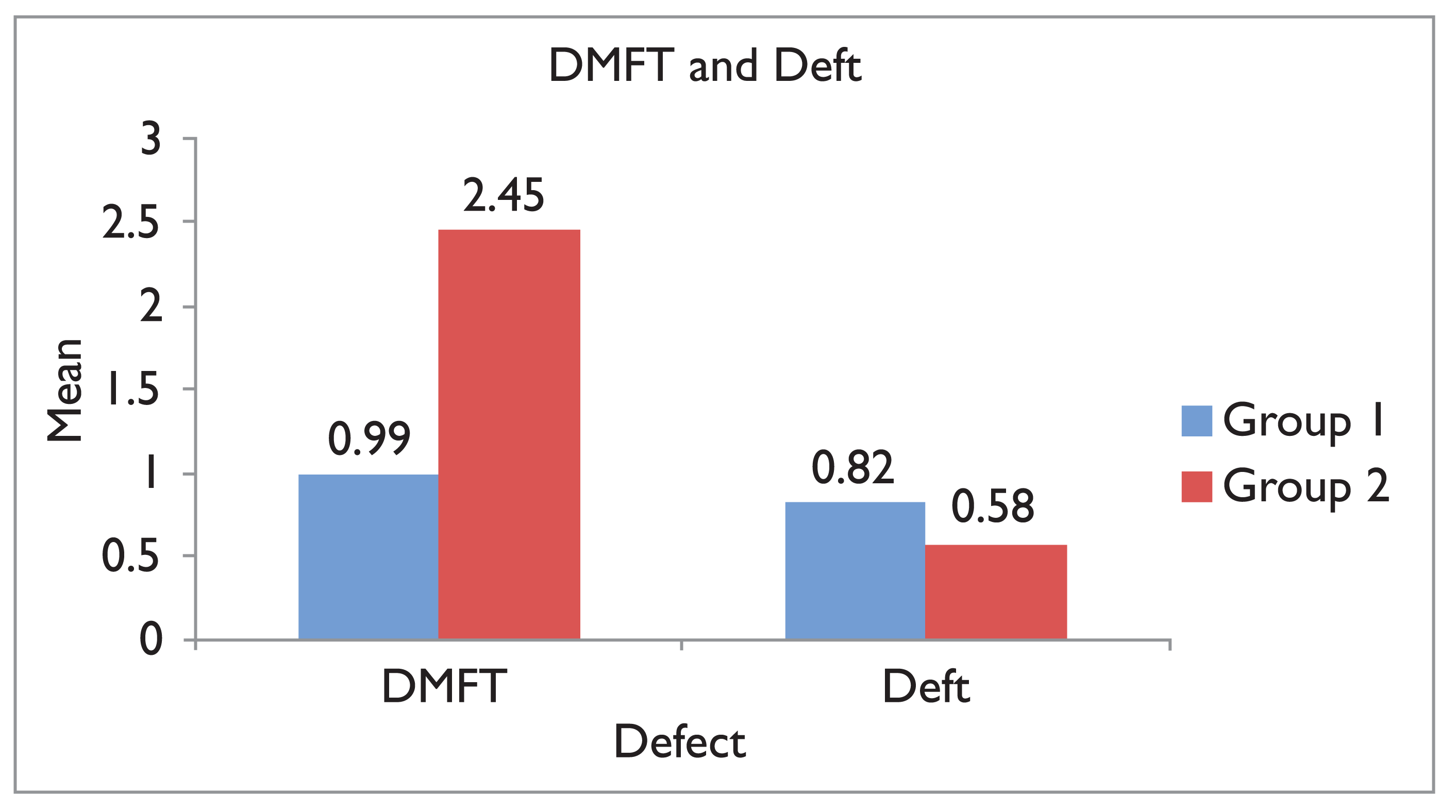
The mean DMFT score in the control group was 0.99 and in the study group was 2.45 which was statistically significant (p < 0.05). The deft scores were comparable between both the groups and were not statistically significant (Figure 1).
Modified ICDAS-II
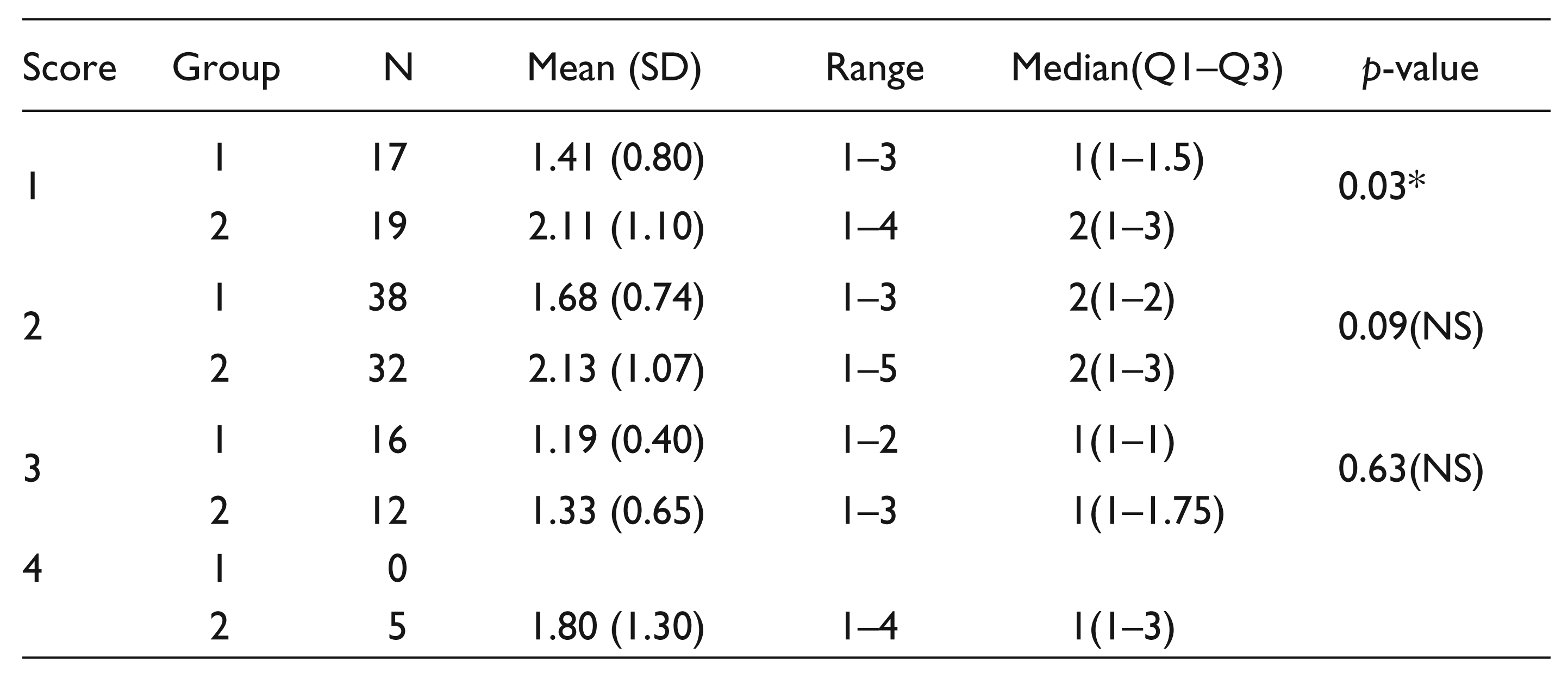
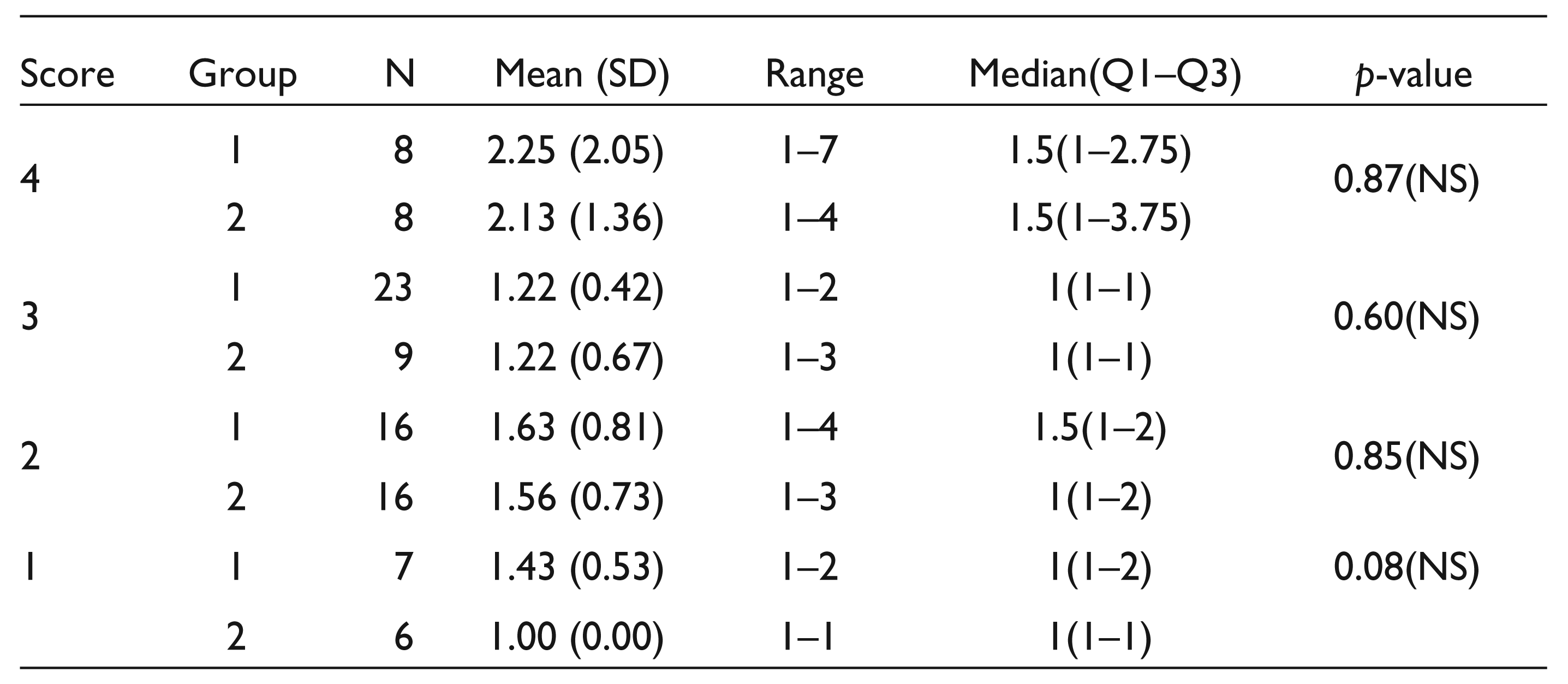
When the progression of caries was seen in the children in both study and control groups, it was found that in primary dentition, most commonly seen stage of caries was score 3 for the control group (23% of the subject) and score 2 for the study group (16% of the subjects). In permanent dentition, score 2 was seen most commonly in both control group (38% of subjects) and study group (32% of the subjects).
Mean permanent teeth with ICDAS score 1 was 1.41 (80) in the control group and 2.11 (1.10) in the study group. The median for the control group was 1(1–1.5) and for the study group was 2(1–3), which was statistically significant (Table 2). No other statistically significant results were found for other ICDAS-II scores for permanent and primary teeth.
OHI-S Scores of Children in Both the Groups
Permanent Dentition—Mean Teeth Affected in Each Score of Modified ICDAS-II
Primary Dentition—Mean Teeth Affected in Each Score of Modified ICDAS-II
No statistical difference was found in the progression of dental caries in primary dentition between the two groups (Table 3).
Discussion
Tooth decay is a major oral health problem in most of the countries, affecting 60–90% of school children. The role of trace elements in the development of tooth decay has been an area of study since the identification of fluoride’s protective effects. Like fluoride, other elements can modify the chemical and physical composition of the teeth, especially the surface layers of enamel. 7 Arsenic is of potential significance to the mineralized tissues because it is the next highest element to phosphorus in the periodic table. 8 Arsenic is known to replace phosphorus and localize in the bone. In rats, long-term exposure to arsenic in drinking water—at doses relevant to human exposure from drinking water—significantly altered bone microstructure and bone mineral density. 9
The objective of this study was to assess the effect of exposure to arsenic by drinking water and caries prevalence in children. Statistically, a significant difference in caries prevalence in study and control groups was observed. Contaminated drinking water is the main source of arsenic exposure in humans. 1 Groundwater level of arsenic in Hutti village was found to be 90 μg/L, much higher than the WHO standard. Hair and nails can be used as effective indicators for chronic arsenic exposure. Arsenic levels in the hair and nail samples of the study population were significantly higher than in the control population.
The US Environmental Protection Agency and WHO have set a standard of 10 μg/L (0.01 ppm) of arsenic level in drinking water. 1 In this study also, the groundwater level of arsenic in Hutti village was found to be 90 μg/L, which is much higher than the WHO standard, whereas in the village taken as control, the arsenic level in groundwater was negligible. Singh et al. found that the concentration of arsenic in water in contaminated areas is much higher than the maximum permissible level by the WHO standard. 10
In the present study, the mean concentration of arsenic in the study population was found to be 2.44 ppm in the hair samples and 2.72 ppm in the nail samples as compared to 0.12 ppm in both hair and nail samples in the control group. Normal concentration of arsenic generally ranges from 0.02 to 0.2 ppm in hair and 0.02 to 0.5 ppm in nails for individuals with no known exposure. 11 Mosaferi et al. found that the concentration of arsenic in hair can be used as a good measurement of chronic exposure. 12 The trivalent inorganic arsenic binds to the SH group of keratin present in hair and nails. 13 The elevated concentration of arsenic in the hair and nail samples of the study group could be due to the chronic arsenic exposure in the children residing in Hutti village.
The oral hygiene of children in both the study and control groups was fair and no significant difference was found between the oral hygiene scores of both the groups.
When the DMFT scores were compared in both the groups, the mean score in the study group was 2.45 as compared to 0.99 in the control group and it was statistically significant. No statistical difference was found between the deft scores of study and control groups. Progression of dental caries was checked by the modified ICDAS-II index. No significant difference was found in the progression of lesion in primary dentition between the two groups. However, statistically significant difference was found only in the initiation of dental caries in permanent dentition. Initial caries lesion in permanent teeth was higher in the children drinking water contaminated with arsenic as compared to the control group. However, in a study done in Bangladesh, Sunny et al. found that the prevalence of dental caries was less among children exposed to arsenic than the children not exposed to arsenic. 14 However, in an epidemiological survey done on children fed with milk contaminated with arsenic during their developmental stages in Japan, the DMFT rate was 97.57%, which was found to be much higher than average. 15 Similarly, Riyat et al. found slight increase in arsenic content in carious enamel as compared to healthy enamel. 16
Although there is no systematic review available about the effects of arsenic and prevalence of dental caries in children, this study contributes to the epidemiological evidence about the same. This study also measures the chronic arsenic exposure in each child by analyzing arsenic levels in their hair and nail samples. However, it was carried out on a smaller sample and more studies in a larger group of population are required to generalize the results and come to a definitive conclusion.
Conclusion
Prevalence of dental caries was significantly higher among the children in the study group. Arsenic could be a contributing factor in the initiation of caries seen in the children of the study group.
Future Research Directions
Observation should be carried out among a larger sample group. Determination of arsenic levels in teeth should be carried out. More studies should be carried out in various parts of India where the groundwater is contaminated with arsenic.
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
None.
Funding
None.