
Abstract
Background:
Neuromuscular diseases (NMDs) are heterogeneous disorders causing progressive motor decline, multisystem complications, and reduced quality of life. Sexual health, a key component of well-being, remains largely overlooked. This scoping review mapped and synthesized evidence on sexual dysfunction (SD) in adults with NMDs, focusing on prevalence, underlying mechanisms, and research gaps.
Methods:
A systematic search of PubMed, Cochrane Library, and Google Scholar (February–March 2025) identified studies reporting original data on SD in adults with genetically or clinically confirmed NMDs. Citation tracking complemented the search. Data were narratively synthesized following PRISMA-ScR guidelines.
Results:
Twenty-seven studies (1983–2024) including 2428 individuals met the inclusion criteria. Most were cross-sectional and questionnaire-based studies. SD was frequent but heterogeneous across conditions. In myotonic dystrophy, erectile dysfunction often related to hypogonadism; in Charcot-Marie-Tooth disease, higher disease severity correlated with altered desire and satisfaction in women; amyloid neuropathies showed autonomic-related erectile and ejaculatory dysfunction in men and multidimensional impairment in women; inflammatory myopathies revealed high SD prevalence in both sexes; amyotrophic lateral sclerosis involved intimacy loss mainly due to disability and psychosocial distress, despite preserved interest; myasthenia gravis displayed SD mainly associated with mental health conditions, X-linked spinal muscular atrophy showed predominantly endocrine-related SD.
Conclusion:
SD is common, multifactorial, and under-recognized in adults with NMDs. The available evidence remains limited by non-inclusive approaches to sexual orientation and intimacy, scarce physiological assessments, and substantial gaps regarding female sexual health, longitudinal data. Integrating sexual health assessment into routine care for people with NMDs should be prioritized.
Introduction
Neuromuscular diseases (NMDs) represent a heterogeneous group of inherited or acquired disorders affecting at least one element of the motor unit, leading to progressive loss of strength, mobility, and autonomy. 1 Management of NMDs is inherently multidisciplinary and typically involves both a medical team, responsible for diagnosis, disease monitoring, and treatment of systemic complications, and a rehabilitation team, usually coordinated by a physical and rehabilitation medicine physician (physiatrist), and including physiotherapists, occupational therapists, speech therapists, psychologists, and other allied health professionals, focused on functional abilities, participation, and quality of life. Clinical care has traditionally prioritized motor and cardiorespiratory complications, and sexual health, an integral aspect of physical, psychological, and social well-being, has received limited attention in both neuromuscular research and routine clinical practice.2,3
When disrupted, sexual function contributes to psychological distress, relationship difficulties, and reduced quality of life. 4 In individuals with chronic neurological or NMDs, sexual dysfunction (SD) may result from a complex interaction of physical limitations, altered genital innervation, fatigue, mood disorders, and hormonal imbalances. 5 Despite these vulnerabilities, sexual health remains insufficiently addressed in neuromuscular settings or in clinical guidelines.5,6
Given the paucity of the literature and the methodological heterogeneity, it was decided to perform a scoping review to map the extent, range, and nature of existing evidence and to identify any knowledge gaps. Such an approach is particularly suited for under-researched areas and exploratory questions. 7
This review aimed to: i) identify and characterize SD in adults with NMDs with particular attention to its prevalence and underlying mechanisms; ii) identify the assessment methods used; iii) highlight gaps to inform future research directions and clinical management options.
Methods
Protocol and registration
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols extension for scoping reviews (PRISMA-ScR). 8 The review protocol was developed a priori, revised in collaboration with members of the Institute of Myology (France), and retrospectively registered in the Open Science Framework on 12 August 2025 (DOI: 10.17605/OSF.IO/35B96). Although the registration occurred retrospectively, the methodological framework reported here reflects the planned process established prior to conducting the review.
Eligibility criteria
Studies were eligible if they included individuals with NMDs and reported data related to sexual function or dysfunction, regardless of whether sexuality was a primary or secondary outcome. Eligible designs encompassed cross-sectional, case-control, longitudinal, interventional, qualitative, and mixed-methods studies, as well as case reports, case series, reviews, and letters containing empirical data. Books, conference abstracts, and grey literature were also considered when accessible online.
Information sources
The literature search was conducted between February 28th, 2025, and March 18th, 2025, using the following electronic databases: PubMed, CENTRAL – Cochrane Central Register of Controlled Trials, Google Scholar. The final search results were exported into Rayyan® (Qatar Computing Research Institute). 9 Duplicates were automatically detected and removed prior to screening. No language filters were applied at the search stage, but only studies written in English or French were retained at the eligibility stage.
Search
The search strategy combined Medical Subject Headings (MeSH) and free-text terms related to both SF (e.g., “sexual behaviour”, “sexuality”, “libido”, “erectile dysfunction”, etc.) and neuromuscular diseases (e.g., “neuromuscular disorders”, “myotonic dystrophy”, “Charcot-Marie-Tooth”, etc.). Filters were applied to exclude animal studies and irrelevant comorbidities (e.g., diabetes, fibromyalgia, neurofibromatosis). The complete detailed search strategies for each database are provided in
Given that PubMed MeSH does not include a unified heading for all NMDs and many disease-specific studies may not be indexed under “neuromuscular disease,” a sensitivity analysis was conducted using disease-specific search terms. This extended search included terms for specific conditions (e.g., “myotonic dystrophy,” “Charcot-Marie-Tooth,” “amyotrophic lateral sclerosis,” “Kennedy disease,” “myasthenia gravis,” “inflammatory myopathy”) combined with sexual health terms.
Selection of sources of evidence
The selection process was conducted in two phases: i) title and abstract screening, ii) full-text screening for articles that appeared potentially eligible. Both phases were carried out independently by two reviewers (AE + MB) using Rayyan, an AI-powered online systematic review tool that facilitates blinded screening and conflict resolution. 9 In cases of disagreement, inclusion decisions were reached by consensus, and when necessary, a third reviewer (JYH) was consulted. In addition to the database searches, backward citation tracking was performed on all included full-text articles to identify additional relevant references not captured through initial search strategies. The full selection process is visually represented in the PRISMA flow diagram, detailing the number of records identified, screened, excluded (with reasons), and included in the final review.
Data charting process
Data were charted using a standardized extraction form developed by the review team in alignment with the review objectives. The form was piloted on a sample of five studies by two independent reviewers (AE + MB) to ensure consistency and was refined iteratively based on initial discrepancies.
For each included source, data were extracted in duplicate by two reviewers (AE + MB) using Microsoft Excel®. Disagreements were resolved through discussion, and a third reviewer (JYH) was consulted when needed. As no contact was made with study authors, all data were extracted from published material only.
Data items
Data extraction was performed using a standardized charting form including: bibliographic information (author, year, country), study design and population characteristics (sample size, age, sex distribution, NMDs subtype), sexual function assessment tools, and key findings related to SD. For reviews or meta-analyses, relevant primary data were extracted and cross-checked against the original studies to avoid duplication.
Critical appraisal of individual sources of evidence
We evaluated the methodological quality of each included study using the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence. 10 Each study was assigned a level of evidence ranging from 1 (highest) to 5 (lowest), reflecting its design and methodological soundness.
Synthesis of results
Data from the included sources were synthesized using a narrative and descriptive approach, consistent with the objectives of a scoping review. For each study, a methodological summary was prepared, detailing the study design, population characteristics, type of neuromuscular disease investigated, and assessment methods used. Key outcomes related to SD were extracted and summarized.
Results are presented in a combination of narrative text and structured tables to provide both an overall mapping of the literature and a focused overview of the main patterns observed by pathology.
Results
Selection of sources of evidence
A total of 975 records were identified through database searches (PubMed, Cochrane Library, and Google Scholar). The complete selection process, including numbers at each stage and reasons for exclusion, is illustrated in the PRISMA-ScR flow diagram (Figure 1).
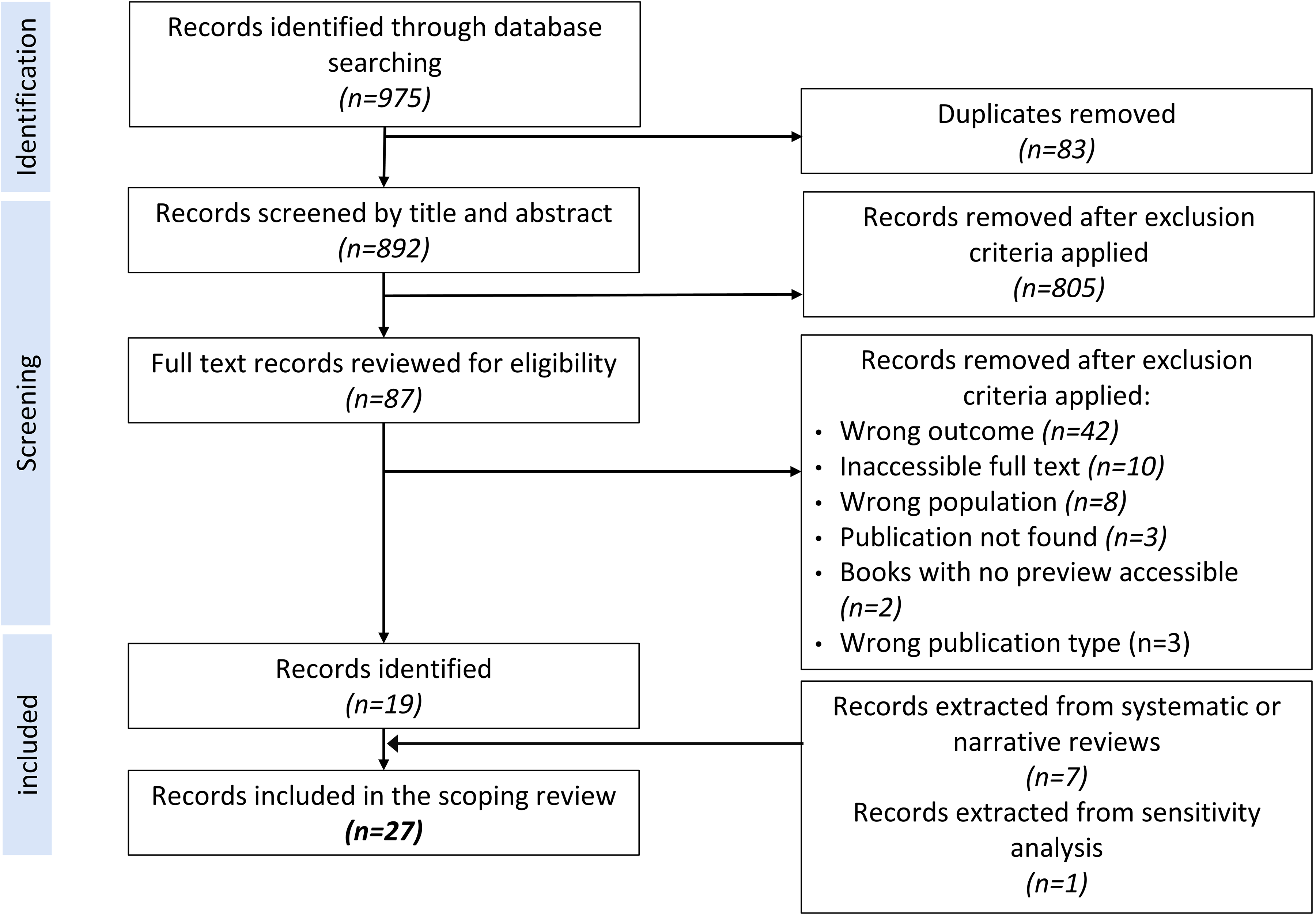
Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) flow diagram.
Characteristics of sources of evidence
A total of 27 articles published between 1983 and 2024 were included in the final review with 12 publications identified between 1983 and 2013 and 15 published since 2014. Of these, 19 were retrieved directly, 7 were extracted from systematic or narrative reviews,11–13 and 1 was identified using a sensitivity analysis 14 (Figure 1) encompassing data from 2428 individuals with various NMDs (Figure 2). The majority were observational studies, including cross-sectional designs (n = 20). Other sources included case series (n = 3), letters to the editor reporting original clinical observations (n = 2), one retrospective study and one patient report. Geographically, studies originated from Europe (n = 19), North America (n = 6), South America (n = 1), Asia (n = 1). Sample sizes varied widely, from single-case descriptions to multi-center studies including over 1180 participants.
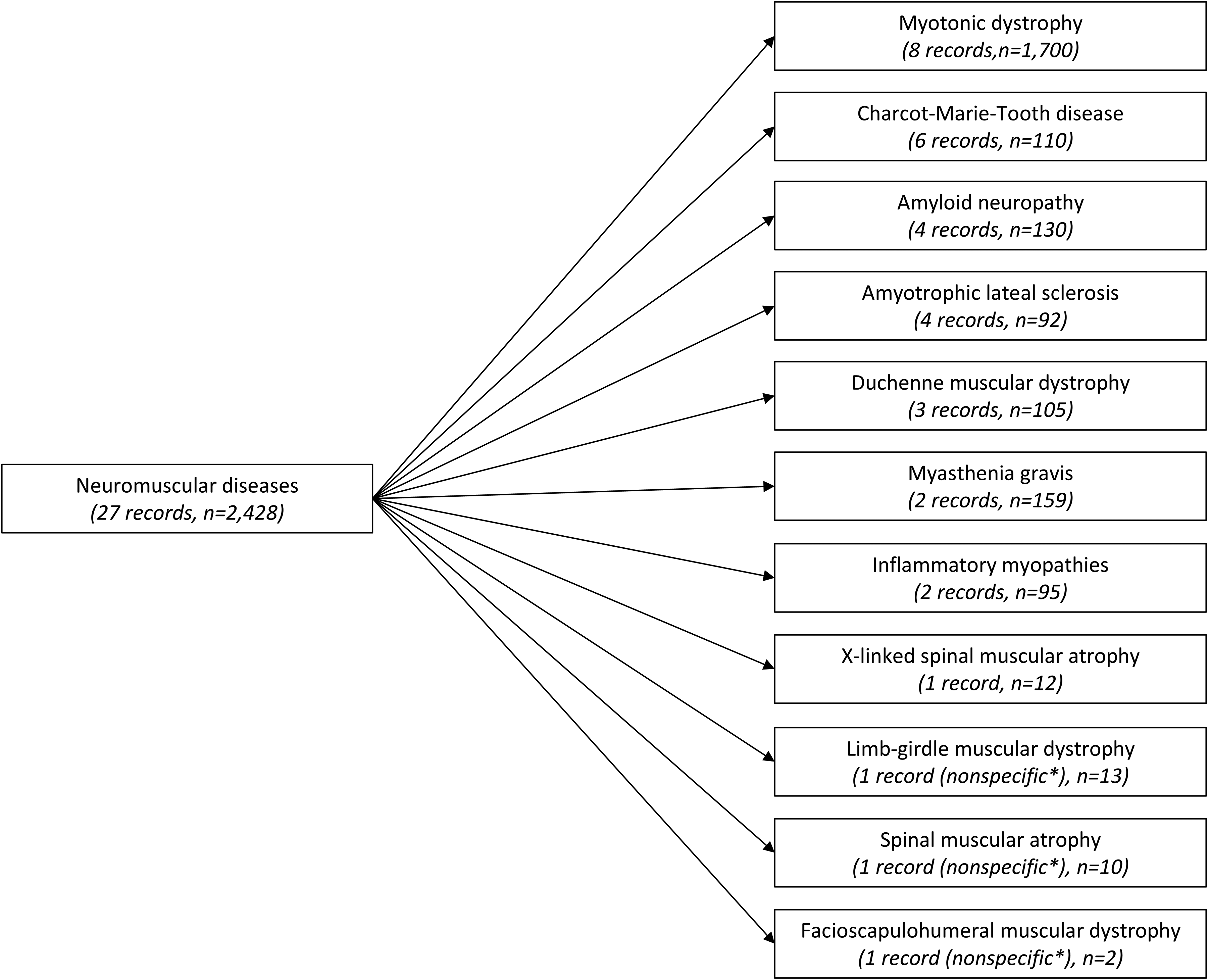
Overview of available studies and sample sizes on sexual dysfunction across neuromuscular disorders.
Across studies, SD outcomes were measured using a variety of approaches, including validated questionnaires (e.g., International Index of Erectile Function (IIEF), Female Sexual Function Index (FSFI), McCoy Female Sexuality Questionnaire (MFSQ)) and non-standardized clinical interviews. The heterogeneity of tools and definitions limited comparability across sources.
A detailed overview of each included source is provided in Table 1.
Characteristics of included studies.
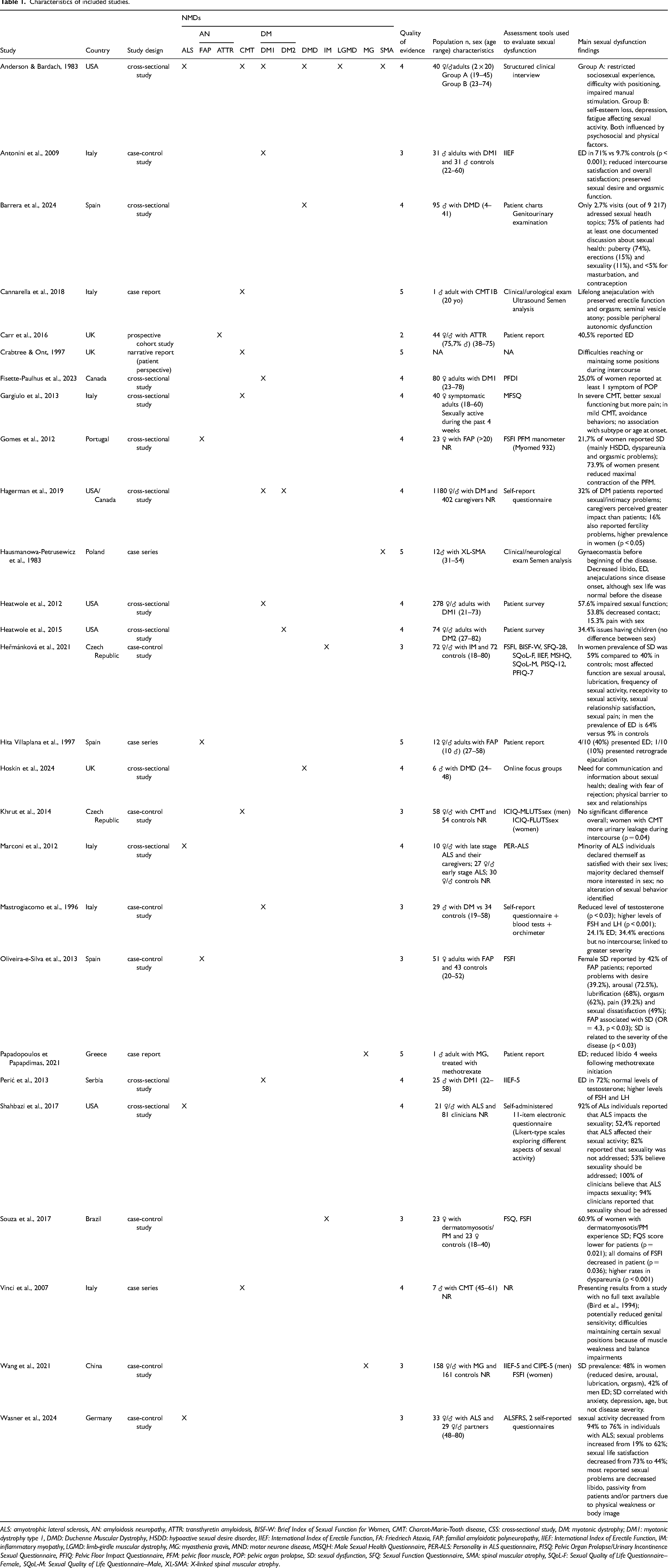
ALS: amyotrophic lateral sclerosis, AN: amyloidosis neuropathy, ATTR: transthyretin amyloidosis, BISF-W: Brief Index of Sexual Function for Women, CMT: Charcot-Marie-Tooth disease, CSS: cross-sectional study, DM: myotonic dystrophy; DM1: myotonic dystrophy type 1, DMD: Duchenne Muscular Dystrophy, HSDD: hypoactive sexual desire disorder, IIEF: International Index of Erectile Function, FA: Friedriech Ataxia, FAP: familial amyloidotic polyneuropathy, IIEF: International Index of Erectile Function, IM: inflammatory myopathy, LGMD: limb-girdle muscular dystrophy, MG: myasthenia gravis, MND: motor neurone disease, MSQH: Male Sexual Health Questionnaire, PER-ALS: Personality in ALS questionnaire, PISQ: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire, PFIQ: Pelvic Floor Impact Questionnaire, PFM: pelvic floor muscle, POP: pelvic organ prolapse, SD: sexual dysfunction, SFQ: Sexual Function Questionnaire, SMA: spinal muscular atrophy, SQoL-F: Sexual Quality of Life Questionnaire–Female, SQoL-M: Sexual Quality of Life Questionnaire–Male, XL-SMA: X-linked spinal muscular atrophy.
Quality of evidence
The methodological quality of included studies was assessed using the OCEBM Levels of Evidence (Table 1). Most studies (n = 21) were classified as Level 4, reflecting predominantly cross-sectional designs. Two case-control studies achieved Level 3b evidence. Case series and case reports (n = 5) were classified as Level 4–5. No randomized controlled trials or well-designed cohort studies specifically addressing SD in NMDs were identified.
Synthesis of results
Mixed neuromuscular cohorts
The seminal work of Anderson and Bardach 15 provided one of the rare insights into sexual activity among individuals with NMDs. The study highlights that early-onset and rapidly progressive forms of NMDs tend to severely impair psychosocial and psychosexual development in adulthood, often leading to limited or absent sociosexual experiences before the onset of major disabilities. In contrast, individuals with slowly progressive or late-onset NMDs are more affected by the emotional and psychological impact of the disease—such as low self-esteem, anxiety, and depression—than by physical limitations alone.
Across both groups, adapting to changes in physical and sexual functions was a source of significant distress. Physical complications commonly observed in NMDs—such as joint contractures, muscle weakness, and fatigue—interfere with mobility, positioning, genital stimulation, and intimacy. The shift in relationship dynamics, especially when one partner takes on a caregiving role, also emerged as a key factor affecting sexual satisfaction. Overall, the study emphasizes that both the timing of disease onset and the rate of progression play a critical role in shaping sexual experience and well-being, underscoring the need for more comprehensive and updated research in this area. Current knowledge is presented below by pathology.
Myotonic Dystrophy (DM) (8 records, n = 1,700, 955♀/ ♂742)
From 1983 to 2023, a total of 8 studies investigated SD among individuals with DM. Indeed, SD appears to be a frequent but under-recognized aspect of myotonic dystrophy type 1 (DM1) also known as Steinert's disease, with growing evidence supporting its multifactorial aetiology.
In men, erectile dysfunction (ED) is consistently reported as the most prevalent form of SD, with prevalence estimates ranging from 24% to over 72% depending on study design and assessment tool used.16–18 Several studies have linked ED to hormonal dysregulation, particularly hypogonadism of testicular origin involving Leydig cell dysfunction, as evidenced by low testosterone levels (p < 0.008), elevated luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations (p < 0.001).17,19 However, hormonal abnormalities alone do not fully account for the observed dysfunction, as some eugonadal individuals with DM1 also report ED, suggesting an interplay of neuromuscular degeneration, smooth muscle involvement, and psychological factors. 18
The sexual health of women with DM1 remains markedly understudied. To date, only one study 20 has investigated pelvic floor symptoms specifically in women with DM1. Although not focused on sexuality, it revealed that 25% of participants reported symptoms suggestive of pelvic organ prolapse, a condition known to affect sexual function through dyspareunia, reduced desire, and impaired arousal. However, due to a lack of direct assessment, no conclusions can be drawn regarding the prevalence or severity of SD in women with DM1.
Beyond isolated physiological mechanisms, SD in DM1 also appears to have a significant psychosocial impact. A large cohort study including 278 individuals with DM1 21 and 74 individuals with DM2 22 reported impaired sexual function and reduced sexual contact in more than half of individuals with DM, and concerns related to intimacy were frequently noted across both genders. 23
Charcot-Marie-Tooth Disease (CMT) (6 records, n = 110, 78♀/ ♂32)
Evidence from a small number of studies and case reports indicate that both men and women with CMT may experience various forms of SD. In men, reported manifestations could include ED24,25 and delayed ejaculation or anejaculation. 25 A case study documented lifelong anejaculation in a man with CMT1B, associated with seminal vesicle atony and autonomic imbalance. 26 However, another study reported no significant differences between individuals with CMT and controls regarding ED or ejaculatory function. 27
In women with Charcot–Marie–Tooth disease (CMT), a cross-sectional study using a validated sexuality questionnaire unexpectedly found that age was significantly and positively associated with global sexual functioning (p < 0.05), 28 indicating that older women reported higher sexual and relationship functioning, contrary to patterns observed in the general population. 29 Disease severity was also significantly related to sexual functioning after controlling for age (p < 0.01), with women with more severe symptoms showing higher scores compared with those with milder symptoms. 28 Higher scores among severely affected women reflected greater desire, arousal, orgasm, and sexual pleasure, although pain during intercourse was more frequent in this group (p < 0.05). 28 No significant differences were found according to CMT subtype (demyelinating vs. axonal; p > 0.3) or age of onset (p > 0.09). 28 Another study identified a higher frequency of urinary incontinence during sexual activity (p < 0.05), 27 but found no significant differences in other domains of sexual function compared to control subjects.
Amyloid Neuropathies (AN) (4 records, n = 130, 87 ♀/ ♂43)
SD is highly prevalent in AN, reflecting the prominent role of autonomic neuropathy in disease expression. In hereditary transthyretin amyloidosis, approximately 40% of men30,31 are affected, with higher prevalence in early-onset disease. 11 In men, ED is the most frequent SD manifestation, reported in about 40% of cases.30,31
In familial amyloid polyneuropathies (FAP), female SD is particularly well documented. Between 21.7% 32 and 42% 33 of women met diagnostic criteria for SD (defined by a FSFI score below 26.55/36). The most common symptoms were arousal disorders (up to 72.5%), lubrication difficulties (68%), orgasmic dysfunction (62–68%), hypoactive sexual desire (≈39%), and dyspareunia (≈39%).32,33 FAP was strongly associated with SD, even after controlling for age, marital status, education, physical exercise, medications potentially affecting sexual function, and the use of oral contraceptives (OR = 4.3, p < 0.03). 33 While asymptomatic women generally maintain normal sexual function, nearly half of symptomatic women experience SD, which becomes nearly universal in advanced disease stages. 32 Pelvic floor weakness, present in up to 74% of women with FAP, may further contribute to impaired arousal and orgasm. 32
Amyotrophic Lateral Sclerosis (ALS) (4 records, n = 92, 32♀/ ♂59)
From the literature, SD in ALS appears predominantly secondary, driven by physical disability, altered body image, and psychological factors rather than by primary neurogenic causes. Quantitative data show a marked decline in sexual interest, activity, and satisfaction after disease onset. In a large survey, 34 sexual interest decreased from 72% before the onset of the disease to 44% at time of survey, while the prevalence of SD rose from 19% to 62% (p < 0.001), with satisfaction negatively correlated with age (p = 0.008) and disease progression (p < 0.001). Partners showed similar trends (SD rising from 20% to 75%). Despite these impairments, some couples reported stable or improved intimacy. Men reported higher sexual interest than women both before ALS (p = 0.008) and at the time of the survey (p = 0.039), and youngest respondents exhibited highest interest (p = 0.034). Erectile and ejaculatory complaints were uncommon and typically predated ALS, reinforcing that secondary (not primary neurogenic) mechanisms predominate in this disease. 34
In questionnaires, individuals with ALS frequently emphasize non-coital activities such as cuddling and sensual touch (72.5%), highlighting adaptive forms of intimacy. 35 However, sexual health is rarely addressed in routine care: most individuals (82%) with ALS report never discussing sexuality with clinicians, and many health professionals feel unprepared to provide guidance, despite acknowledging its importance. 35
Duchenne Muscular Dystrophy (DMD) (3 records, n = 105♂)
Sexual health in DMD remains insufficiently addressed, despite being a significant concern for affected individuals. Clinical data indicate that discussions of sexuality are rare in routine care: in a large cohort of over 9000 outpatient visits, only 2.7% included documentation of sexual health topics, with puberty representing the dominant focus, while broader aspects such as body image, masturbation, contraception, or fertility were seldom addressed (≤5%). 36 When it is documented, sexual health is mainly addressed by endocrinologists, who were responsible for more than 80% of notes on sexual health topics, whereas other specialties such as adolescent medicine contributed more rarely. 36
Qualitative evidence (online focus group) from adult individuals with DMD reinforces this gap by highlighting lived challenges around intimacy and fertility. Men with DMD report major obstacles, including lack of accessible information, fear of rejection, low self-esteem, and physical limitations that sometimes necessitate assistance or the use of paid services to achieve intimacy. 37 Individuals with DMD also express ambivalence regarding reproductive health, particularly concerns about testosterone supplementation and uncertainties around parenthood. 37
Myasthenia Gravis (MG) (2 records, n = 159, 106♀/ ♂53)
A case-control study suggests a high prevalence, with nearly half of women reporting global impairments in sexual function, affecting desire, arousal, lubrication, and orgasmic capacity. 38 The incidence of SD was significantly higher in women with MG (N = 106) than healthy individuals (48.11% vs 22.64%, p < 0.001). 38 In men with MG (N = 52), ED is reported in more than 40% of cases (42.31% vs 32.08, ns), often accompanied by significant ejaculatory disturbances (p < 0.002) and reduced sexual satisfaction. 38
Importantly, SD in MG does not appear to correlate with the clinical severity of neuromuscular symptoms, suggesting that motor weakness alone cannot account for SD. Instead, strong associations have been observed with psychiatric comorbidities, particularly anxiety and depression (p < 0.001), pointing to psychosocial factors as major determinants of sexual health in this population. 38
In addition to intrinsic disease mechanisms, pharmacological factors may also play a role. A case report documented the occurrence of ED and decreased libido following methotrexate initiation, which resolved upon drug discontinuation, implicating methotrexate as a potential but underrecognized contributor to SD in MG. 39 Given that sexual side effects may go unnoticed unless actively explored, iatrogenic causes should be considered in clinical practice.
Idiopathic Inflammatory Myopathies (IIM) (2 records, n = 95, 84♀/ ♂11)
In IIM, SD is consistently reported with high prevalence. In dermatomyositis and polymyositis, more than 60% of women present some degree of SD, with marked reductions in sexual function scores across desire, arousal, lubrication, orgasm, and satisfaction (p < 0.05); dyspareunia is particularly frequent, affecting nearly two-thirds of patients versus less than 10% of healthy controls (p < 0.001). 40 Broader studies confirm that SD affects both sexes: women show significant impairments in FSFI and BISF-W domains (p < 0.01), especially arousal, lubrication, frequency, receptivity, satisfaction, and pain, while men more often report erectile and ejaculatory dysfunction, pelvic floor disorders, and reduced satisfaction. Overall, 59% of women with IIM meet diagnostic thresholds for SD compared with 40% of healthy controls (p < 0.05), and men (p < 0.05) and women (p < 0.001) with IIM exhibit lower sexual quality of life compared to healthy populations. 41
X-linked Spinal Muscular Atrophy (Xl-SMA) (1 record, n = 12♂)
Hausmanowa-Petrusewicz et al. 14 documented gonadal dysfunction as a consistent feature, with ED, reduced libido, testicular atrophy, and impaired spermatogenesis evidenced by elevated gonadotropins and reduced testosterone. These findings suggest a primary endocrine involvement of the hypothalamic–pituitary–gonadal axis. In this context, they are in line with more recent reports describing alterations in spermatogenesis in individuals with SMA. 42 Taken together, these observations indicate that SD in XL-SMA may involve mechanisms that differ from those observed in conditions such as ALS, where SD is predominantly related to physical disability and psychosocial factors.
Discussion
Summary of evidence
In this scoping review, SD emerges as a frequent but inconsistently conceptualized dimension of NMDs. Beyond its prevalence, the synthesis highlights marked heterogeneity in both underlying mechanisms and research approaches across conditions, reflecting the complexity of sexual health in NMDs.
The evidence base is heterogeneous in design (cross-sectional surveys, case-control studies, qualitative interviews, cohort descriptions, narrative reviews, and isolated case reports), relies chiefly on validated self-report questionnaires (e.g., FSFI, International Index of Erectile Function (IIEF/IIEF-5), Male Sexual Health Questionnaire (MSHQ)) and condition-specific questionnaires (e.g., Personality in Amyotrophic Lateral Sclerosis Questionnaire (PER-ALS)), and is characterized by modest samples, limited longitudinal data, and scarce interventional research.
Rather than a uniform phenomenon, SD appears to result from distinct and often overlapping pathways depending on the context of disease. Available evidence suggests that endocrine and autonomic mechanisms may play a prominent role in conditions such as DM, AN, and XL-SMA, whereas psychosocial factors, iatrogenic effects, and disability-related constraints seem to predominate in diseases such as ALS and MG. In IIM, pain and pelvic-floor dysfunction emerge as key contributors. This mechanistic diversity underscores that SD in NMDs cannot be adequately addressed through a single explanatory model or clinical approach.
The review also reveals a structural imbalance between the epidemiology of NMDs and research attention devoted to sexual health. While DM and CMT, among the most prevalent NMDs, 43 are relatively well represented in the literature on SD, several other common conditions remain unexplored in this domain. Notably, no disease-specific studies addressing SD were identified for chronic inflammatory demyelinating polyneuropathy (CIDP), inclusion body myositis (IBM), FSHD, or Becker muscular dystrophy (BMD), despite their relatively high prevalence. 43
In relation to the review objectives, the synthesis indicates: i) SD is common across entities but mechanistically heterogeneous from the scarce studies (autonomic in AN; endocrine/pelvic-floor and psychosocial in DM; psychosocial/iatrogenic in MG; disability/psychosocial in ALS; pain/pelvic-floor in IIM); ii) measurement relies almost exclusively on questionnaires, with minimal physiological or interventional corroboration; iii) research coverage is uneven, with notable blind spots (CIDP, IBM, LGMD, FSHD, …), a lack of longitudinal designs and limited investigation of sex differences in sexual functioning.
Limitations
Although a comprehensive search strategy was implemented across major databases and complemented by citation tracking, inclusion was restricted to English and French publications, which may have excluded relevant data in other languages. The broad scope and methodological heterogeneity of the included studies, ranging from case reports to cross-sectional surveys, prevented quantitative synthesis and limited comparability. In addition, many studies involved small sample sizes, which further constrain statistical power and limit the generalizability of findings to broader neuromuscular populations.
Most studies relied on self-reported, non–disease-specific questionnaires primarily focused on ED, with limited assessment of other domains such as desire, arousal, orgasm, or psychosocial correlates including relational satisfaction and body image. Several frequently used tools (e.g., FSFI, IIEF) assess experiences during the previous four weeks, which may not represent a typical period of sexual activity, especially in individuals with fluctuating health. Most research employed questionnaires grounded in androcentric and coitocentric models of sexuality centered on genital performance and penetrative intercourse and excluded individuals with severe motor impairments or those not engaging in partnered heterosexual activity. Consequently, individuals without penetrative sex, those engaging primarily in auto-erotic practices (e.g., masturbation), non-heterosexual persons, or individuals whose intimacy takes non-genital forms may be rendered invisible by the current measurement framework. In addition, social desirability bias may have influenced self-reported responses, leading to underreporting or overreporting of SD.
Female sexual health remains insufficiently explored. Broader determinants potentially influencing women's sexual health, such as hormonal fluctuations, reproductive history, or psychosocial transitions across life stages, were seldom addressed. While these factors were not specifically targeted in the search strategy, their limited representation highlights the need for more comprehensive and gender-sensitive approaches in future investigations. Most included studies originated from occidental and high-income countries, where sociocultural norms and healthcare structures may shape both the perception and reporting of sexual health issues.
Implications for practice and research
Sexual health should be recognized as a key component of holistic care in NMDs, requiring close collaboration between medical and rehabilitation teams. Rather than isolated diagnostic or technical interventions, sexual health management should be conceptualized as a structured rehabilitation process, beginning with education, normalization, and permission-giving, and progressing toward individualized assessment and intervention according to individual needs. This perspective is consistent with established multidisciplinary sexual rehabilitation frameworks developed for people with chronic disabling.44,45
Within the medical team (e.g., neurologists, internists, endocrinologists), responsibility primarily lies in identifying medical and iatrogenic contributors to SD, including pain, spasticity, endocrine abnormalities, fatigue, and medication-related effects. Medical clinicians also play a crucial role in initiating discussions about sexual health, legitimizing patient concerns, and ensuring appropriate referral when specialized care is needed. Physiatrists occupy a bridging position between medical and rehabilitation domains. While maintaining medical responsibility, they coordinate the rehabilitation process and integrate functional assessment and therapeutic strategies into the management of SD.
Within this coordinated framework, the broader rehabilitation team (e.g., physiotherapists, occupational therapists, psychologists, and other allied health professionals) is particularly well positioned to address the functional and psychosocial dimensions of sexual health in individuals with NMDs. Rehabilitation professionals routinely work on mobility, positioning, endurance, body awareness, and participation, all of which directly influence sexual activity and intimacy. Through their close and sustained contact with patients, they may also identify difficulties related to body image, self-esteem, role changes, and relational dynamics. Interventions may include practical adaptations such as positioning aids, 46 energy-conservation strategies, 47 pelvic-floor rehabilitation, and support for communication around intimacy.
Stepwise counseling models, such as the (EX-)PLISSIT framework, provide practical guidance for operationalizing this process, ranging from permission and limited information to specific suggestions and referral for intensive therapy when needed.48,49 Integrating such models into neuromuscular rehabilitation pathways may help clarify professional roles, improve continuity of care, and ensure that sexual health concerns are addressed in a systematic and patient-centered manner.
Despite its importance, most health professionals receive limited or no formal training in sexual medicine, which contributes to SD being infrequently addressed in routine practice. While it is not necessarily the role of physicians or other health professionals to manage SD directly, most sexual health concerns can initially be addressed within the multidisciplinary rehabilitation team. Referral to specialized professionals, such as sexologists, psychologists, or pelvic-health specialists, should be considered when difficulties persist, are complex, or exceed the scope of rehabilitation-based interventions. In the context of fertility or parenthood-related concerns, particularly for inherited NMDs, referral to genetic counseling may also be appropriate to support informed reproductive decision-making.
For individuals living with a NMD, SD can deeply affect intimacy, and emotional connection. Accessible, evidence-based education and partner-inclusive counseling are essential to help individuals and their partners redefine sexuality beyond performance or penetration, focusing instead on pleasure, communication, and mutual understanding. Encouraging open dialogue about sexual needs can also reduce isolation, improve relationship satisfaction, and enhance adherence to rehabilitation programs. Support groups and peer-based interventions may further help individuals normalize their experiences and exchange adaptive strategies within a safe, nonjudgmental space.
From a health system perspective, the case of DMD illustrates a broader systemic shortcoming: sexual health remains poorly documented and insufficiently prioritized in clinical practice, despite its major contribution to quality of life. Policy initiatives should promote the inclusion of sexual-health indicators in patient records, training modules for healthcare providers, and the integration of sexual rehabilitation within neuromuscular care networks.
For researchers, priorities include the establishment of longitudinal, open-enrolment cohorts encompassing a wide range of NMDs to ensure epidemiological representativeness and to better understand how SD evolves across disease trajectories. The validation of brief, disease-adapted tools for assessing sexual function and satisfaction is needed to facilitate inclusion of sexual health outcomes in both clinical and research settings. Mechanistic studies integrating endocrine, autonomic, and pelvic-floor assessments would help clarify the multifactorial origins of SD in NMDs, distinguishing physiological from psychosocial contributors. Pragmatic trials evaluating multidisciplinary sexual-rehabilitation interventions, including counseling, physical therapy, hormonal treatment, and assistive strategies, are also warranted to identify effective, scalable care models. Finally, dedicated research on women's sexual health is needed, particularly across key life stages such as adolescence and puberty, pregnancy, childbirth, the postpartum period, and menopause, all of which may influence sexual well-being and intimacy.
Conclusion
This scoping review provides the first comprehensive mapping of SD in NMDs, revealing that SD is common, multifactorial, and consistently under-recognized. The available evidence indicates that SD is reported in a wide range of NMDs and involves heterogeneous mechanisms, including endocrine, autonomic, neuromuscular, psychosocial, and iatrogenic factors, depending on the underlying pathology.
However, the review also highlights substantial disparities in the distribution and quality of available evidence. While relatively more data are available for DM, CMT, AN and ALS, no disease-specific studies addressing SD were identified for several common NMDs such as FSHD, CIDP, IBM, and BMD, underscoring important gaps in current knowledge.
Long considered taboo, research on sexual health in NMDs has begun to blossom in recent years. However, clinically, sexual health remains insufficiently assessed in neuromuscular practice, constituting a structural gap in holistic care. Developing interdisciplinary pathways, professional training, clinical guidelines and patient-centered educational resources would strengthen the translation of research into care, ensuring that sexual health is recognized as a core health domain and thereby potentially improving the quality of life and autonomy of individuals living with NMDs.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261434092 - Supplemental material for Sexual health in neuromuscular diseases: Neglected challenges revealed by a scoping review
Supplemental material, sj-docx-1-jnd-10.1177_22143602261434092 for Sexual health in neuromuscular diseases: Neglected challenges revealed by a scoping review by Audrey El kaïm, Marjorie Banos, Valérie Decostre, Simone Birnbaum, Jean-Yves Hogrel and Marcela Gargiulo in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank all the members of the Institute of Myology for their continuous support and their commitment to improving the understanding and management of neuromuscular diseases.
CRediT author statement
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received government funding managed by the French National Research Agency under the France 2030 program (reference ANR-23-BIOC-0003).
Declaration of competing interest
The authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of open AI
Language and grammar of this manuscript were reviewed and corrected using ChatGPT (version GPT-5, OpenAI, San Francisco, CA, USA), an AI language model. The authors are solely responsible for the scientific content and interpretations presented in this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.