
Abstract
Background:
Spinal muscular atrophy (SMA) is a genetic neuromuscular disease characterized by muscular atrophy and respiratory and bulbar dysfunction, especially in the most severe phenotypes (SMA type 0 and 1). Swallowing function remains understudied because assessment tools are often unavailable or poorly tolerated by young children. The Iowa Oral Performance Instrument (IOPI), that measures orofacial strength via a small air-filled bulb has recently been evaluated in SMA type 2 and 3 patients.
Objective:
The purpose of this study was to investigate muscle strength of several muscles used during the oral phase of swallowing using IOPI in SMA type 1 children treated with nusinersen compared to healthy controls. In addition, it sought to correlate labial and lingual pressures with known key predictors of phenotype severity (Children's Hospital Of Philadelphia Infant Test of Neuromuscular Disorders [CHOP INTEND], age at first symptoms, SMN2 copy number) and indicators of feeding-nutritional status (p-FOIS (Pediatric Functional Oral Intake Scale)).
Methods:
Combining results from four independent centers, we recruited 22 individuals with a confirmed genetic diagnosis of symptomatic SMA type 1. All patients had been treated with nusinersen for at least 2.5 years and had undergone at least one IOPI measurement at a median age of 5.4 years. IOPI data were compared to age- and gender-matched controls and published normative data when available.
Results:
Oral pressures were lower in patients than in typically developing children (lips: p < 0.01; tongue: p < 0.001). Weaker labial pressure was significantly correlated with younger age at disease onset (r = 0.66; p = 0.0053), older age at first nusinersen injection (r = -0.52; p = 0.0326), lower body mass index (r = 0.61; p = 0.0149), and worse motor performance as expressed by the CHOP INTEND score (r = 0.60; p = 0.0170). Weaker tongue pressure was significantly correlated with younger age at disease onset (r = 0.49; p = 0.0372) and lower p-FOIS (r = 0.526; p = 0.022).
Conclusions:
IOPI measurements objectively demonstrate orofacial weakness in this population compared with healthy controls and may serve as a biomarker to monitor the impact of comprehensive management, including disease-modifying therapies, on oral swallowing function in SMA type 1.
Keywords
Introduction
Spinal muscular atrophy (SMA) is caused by loss or mutation of the survival motor neuron 1 (SMN1) gene, resulting in the degeneration of alpha motor neurons in the anterior horn of the spinal cord. 1
Different SMA types (types 0 to 4) are recognized depending on the age at symptom onset and the motor function achieved. Phenotype severity is commonly inversely correlated with survival motor neuron 2 (SMN2) gene copy number, although not invariably. SMA type 1 is the most common type of SMA (60% of SMA diagnoses) and is characterized by symptom onset before 6 months of age. Symptoms include hypotonia secondary to muscle weakness and muscle wasting, especially in the proximal limb muscle. Without treatment, SMA type 1 patients never acquire the ability to sit up on their own, and the vast majority die within the first 2 years of life, making it the leading genetic cause of infant mortality. 2
Three disease-modifying therapies have been approved for the treatment of SMA: nusinersen, onasemnogene abeparvovec, and risdiplam. All three increase full-length SMN protein levels (i.e., the protein produced by SMN1) through different mechanisms and routes of administration, and have been shown to modify the disease course in terms of survival and motor improvement. Nusinersen, an antisense oligonucleotide administered intrathecally, and risdiplam, a small molecule administered orally, modify alternative splicing of SMN2 messenger ribonucleic acid, with increased production of functional SMN protein, 3 while onasemnogene abeparvovec is a one-time intravenous gene therapy that uses an adeno-associated viral vector type 9 containing the SMN1 gene. 4
Among the various comorbidities affecting SMA patients, bulbar dysfunction leading to feeding and swallowing difficulties is of particular relevance, especially in SMA type 1, and regular assessment of nutrition and swallowing function is part of the standard of care in these infants. The natural history of nutritional support needs for SMA type 1 patients is well documented.2,5 Initial symptoms, which are often fluctuating, include inadequate hydration, fatigue, sweating, increased respiratory rate, and frequent coughing during breastfeeding sessions that are shortened. All of these contribute to unsafe swallowing. 6 During the oral phase, SMA type 1 patients have difficulty sucking and managing their oral secretions. Previous studies have clearly shown that chewing difficulties, along with decreased tongue movements and food residues remaining in the oral cavity, are very common problems experienced by SMA type 1 and 2 patients during oral feeding. 7 During the pharyngeal phase, a combination of incomplete airway protection and swallowing weakness leads to an increased risk of inhalation pneumonia. A high incidence of gastroesophageal reflux has also been reported.
Swallowing function in SMA type 1 patients remains challenging to assess and limited in light of recent disease-modifying treatments. In young children, it is often evaluated based on the consequences of swallowing impairment, such as a possible cessation in weight and height growth or the occurrence of respiratory infections, especially after a pulmonary aspiration. Medical history can be completed using specific questionnaires, such as the Pediatric Functional Oral Intake Scale (p-FOIS) and the Oral and Swallowing Abilities Tool (OrSAT).6,8
Other more in-depth assessment modalities, such as magnetic resonance imaging (MRI) of the jaw, videofluoroscopic swallowing study (VFSS), and fiberoptic endoscopic evaluation of swallowing (FEES), allow for more direct observation of the anatomical structures involved in swallowing, but are much more invasive, more expensive and complex to organize.
Measuring the pressure exerted by intraoral and facial muscles using the Iowa Oral Performance Instrument (IOPI; IOPI Medical LLC, Washington, USA) provides quantitative and objective information on the oral phase of swallowing. The device measures pressure generated against a small air-filled bulb positioned either between the lips or between the tongue and the palate. The resulting pressure values reflect the functional capacity of the orofacial muscles involved. These muscles play a key role in the proper execution of phase I (oral phase) of swallowing.
In recent years, the IOPI has been validated in several neuromuscular diseases, and more recently SMA, especially SMA type 1, 2 and 3.7,9–11
In this context, the aims of this study are (1) to investigate muscle weakness of the lingual and labial pressures involved in the oral phase of swallowing in a cohort of SMA type 1 children treated with nusinersen compared to healthy controls (HC), (2) to correlate labial and lingual pressures with the main known predictors of severity of this phenotype (Children's Hospital Of Philadelphia Infant Test of Neuromuscular Disorders [CHOP INTEND], duration between first symptoms and treatment onset, and SMN2 copy number) and with indicators of nutritional status such as body mass index (BMI), p-FOIS and need for gastrostomy.
Materials and methods
Patients and study design
SMA cohort
Given the low prevalence of SMA (incidence of approximately 1 in 10,000 live births), this study combined the data collected in two prospective studies, conducted in Belgium and Italy, designed to assess swallowing function in SMA type 1 patients and approved by two distinct ethics committees. The Belgian study included the Hôpital universitaire des enfants reine Fabiola (HUDERF) in Brussels and the Universitair Ziekenhuis (UZ) in Ghent (HUDERF protocol P2022/191–B4062022000099; UZ protocol P2022 / 252- B408679560085), while the Italian study included the Department of neurorehabilitation of the University of Milan (Nemo Milan) and the Department of pediatric neurology of the Università Cattolica del Sacro Cuore of Rome (Nemo Rome) (Coordinator center protocol n. 290-2705220).
Measurements were performed between March 2020 and September 2023 in 22 SMA type 1 patients, aged 3 to 15.5 years, whose diagnosis was genetically confirmed. The inclusion criteria are having genetically confirmed type 1 SMA, being aged 3 to 16 years and being treated with nusinersen. Exclusion criteria included the presence of a respiratory infection at the time of registration, use of tracheostomy, and limitation in understanding instructions.
Informed consent was signed by the parents/caregivers.
Healthy control cohort
Data from HCs were collected as part of a previous study published in 2024 by Colot et al. 7 In this study, HCs were recruited in different school setting in the region of Brussels and Brabant Wallon in Belgium. Based on medical record interview with their parents, HCs did not present any significant comorbidities.
Experimental protocol
Patients underwent between one and five oral pressure measurements with the IOPI. The IOPI is a validated measure in patients with oropharyngeal muscular dystrophy and is currently being used in patients with myotonic dystrophies (TREAT-CDM study at the University of Virginia, USA; GUP19002 study, grant given to VS (“Verenigte samen”) from Telethon and the Italian Muscular Dystrophy Association). 9
The IOPI provides objective pressure measurement using an air-filled bulb. Pressure applied to the air-filled bulb is displayed by the device. After connecting the bulb, the unit is powered on, calibrated to zero, and set to record peak pressure. The bulb is positioned at the site of interest and reset between measurements.
This is a non-invasive measurement system to assess labial pressure (between the lips on the midline) and lingual pressure (between the anterior part of the tongue and the hard palate). For each location, the patient was asked to push three times during few seconds and the best of the three peak values was retained.12–14 Pressure is recorded in kilopascals (kPa).
During the measurements, the child sat with their back straight. The measurements were taken at least two hours after a meal. One examiner per center performed the measurements.
To correlate swallowing function with motor function, motor assessment was performed using the CHOP INTEND. This scale was originally validated to evaluate the ability of non-ambulatory SMA children and adults to perform specific movements. It consists of 16 items, most of which are scored from 0 to 4, with 0 corresponding to the absence of a response or the inability to perform the movement and 4 corresponding to the ability to perform the task completely. The maximum total score is 64. 15 Correlation was made between the CHOP INTEND value closest in time to the oral pressure measurements (duration <6 months).
Anthropometric data (height, weight, BMI) were collected for all patients, as well as the number of SMN2 copies, clinical information such as need for gastrostomy, presence of lingual atrophy (results only for 11 patients), lingual fasciculation (results only for 12 patients), age at disease onset, interval between first symptoms and first injection, motor function, and the p-FOIS. The p-FOIS is a 6-point feeding scale that categorizes an infant's feeding skills across a functional continuum (1 : No oral intake – 2 : Tube-dependent with minimal/inconsistent oral intake – 3: Tube supplements with consistent oral intake – 4: Total oral intake of a single consistency – 5: Total oral intake of a multiple consistencies requiring special preparation – 6: Total oral intake with no special). This scale has been easily used to assess swallowing in SMA type 1 patients treated with nusinersen 3 and can be used to monitor patients’ bulbar function and response to treatment.
Underweight was defined as a gender- and age-adjusted BMI <5th percentile, while overweight was defined as an age-adjusted BMI >85th percentile.9,16
Statistical plan
For each variable, the Shapiro-Wilk test and the Levene's test were used to evaluate normality of distribution and homogeneity of variance, respectively. Data were summarized using median and interquartile range for continuous variables and frequency and percentage for categorical and dichotomous variables.
Labial and tongue pressures, as measured by the IOPI, were compared between patients and HCs using the Mann-Whitney U test. Labial and tongue pressures in HCs were reported by one of the four participating centers (HUDERF) in a previous publication. 7 Reference values for both labial and tongue pressures were obtained from the cohort of HCs stratified by age group, and z-scores were calculated by comparing the SMA patients with the HCs within each age group.
The z-score values of the labial and tongue pressures that fell below the normal limits at the 95% confidence interval were defined as “abnormal” and were graphically represented by the Bland-Altman plot.
In patients, labial and tongue strengths were correlated with demographic characteristics, p-FOIS values and motor functional assessments using Spearman's correlation coefficient and Mann-Whitney U test, as appropriate.
All statistical tests were two-tailed, and a p-value <0.05 was considered statistically significant. All analyses were performed with SAS software version 9.3 (SAS Institute, Inc, Cary, NC, USA).
Results
SMA population characteristics
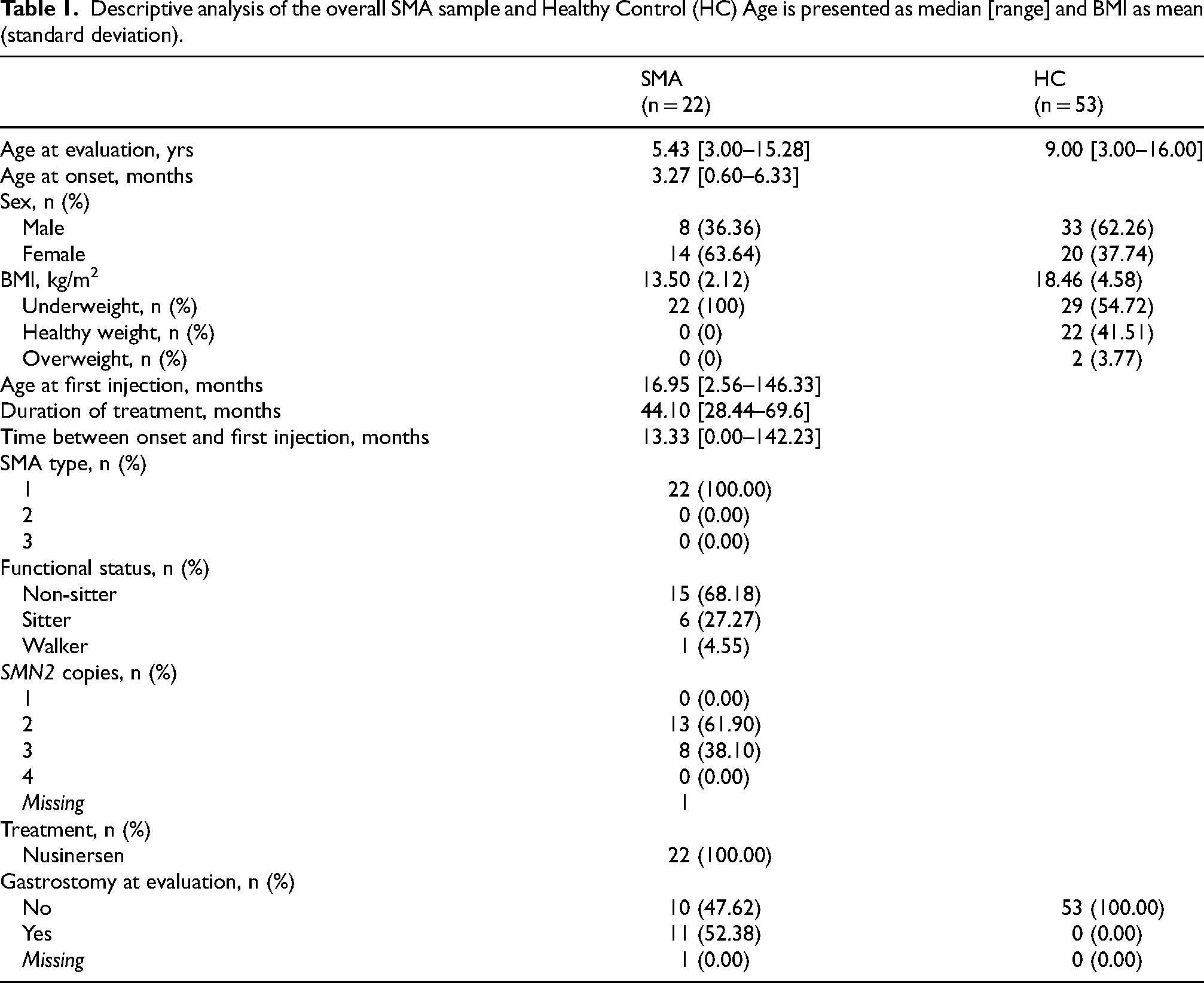
A total of 22 SMA type 1 patients were included. The median age at first assessment was 5.50 years (range 3.0–15.3). Demographic and clinical characteristics of both cohorts are summarized in Table 1. The median CHOP INTEND score was 44 (range 3–60). Of the 22 SMA patients, 91% (n = 10/11) had signs of lingual atrophy and 83% (n = 10/12) had fasciculations.
Descriptive analysis of the overall SMA sample and Healthy Control (HC) Age is presented as median [range] and BMI as mean (standard deviation).
Comparison of intraoral pressures between patients and healthy controls
Data from 53 HCs were collected from the original article for comparison. 10
A Mann-Whitney U test was conducted to compare oral pressure between SMA patients and HC. The results indicated a significant difference between the groups, Lip: U = 11, p < 0.001, r = 0.970 – Tongue: U = 13; p < 0.001, r = 0.967 with SMA patients having lower values than HC (mean lip SMA=6.93 ± 5.70 vs mean lip HC = 30.89 ± 9.23 – mean tongue SMA =6.93 ± 4.89 vs mean tongue HC = 46.8 ± 17.79) (Figure 1).
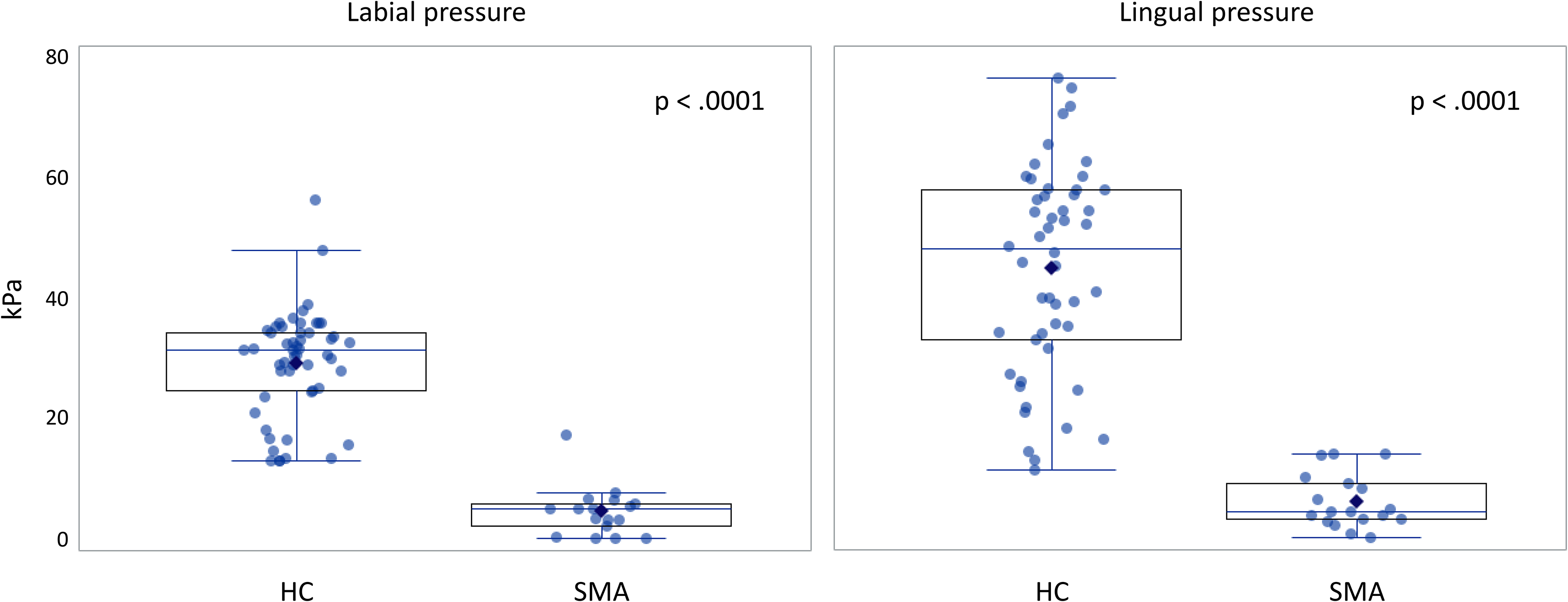
Comparison of labial and lingual pressure between SMA patients and healthy controls (HC).
When comparing the labial and lingual pressure z-scores of the patients to the age-matched HC population (Table 2), the labial and tongue pressures were below the normal range in 94% and 89% of the patients, respectively (Table 3).
Number of participants, mean and standard deviation of tongue and labial pressures of healthy control subjects stratified for age groups.
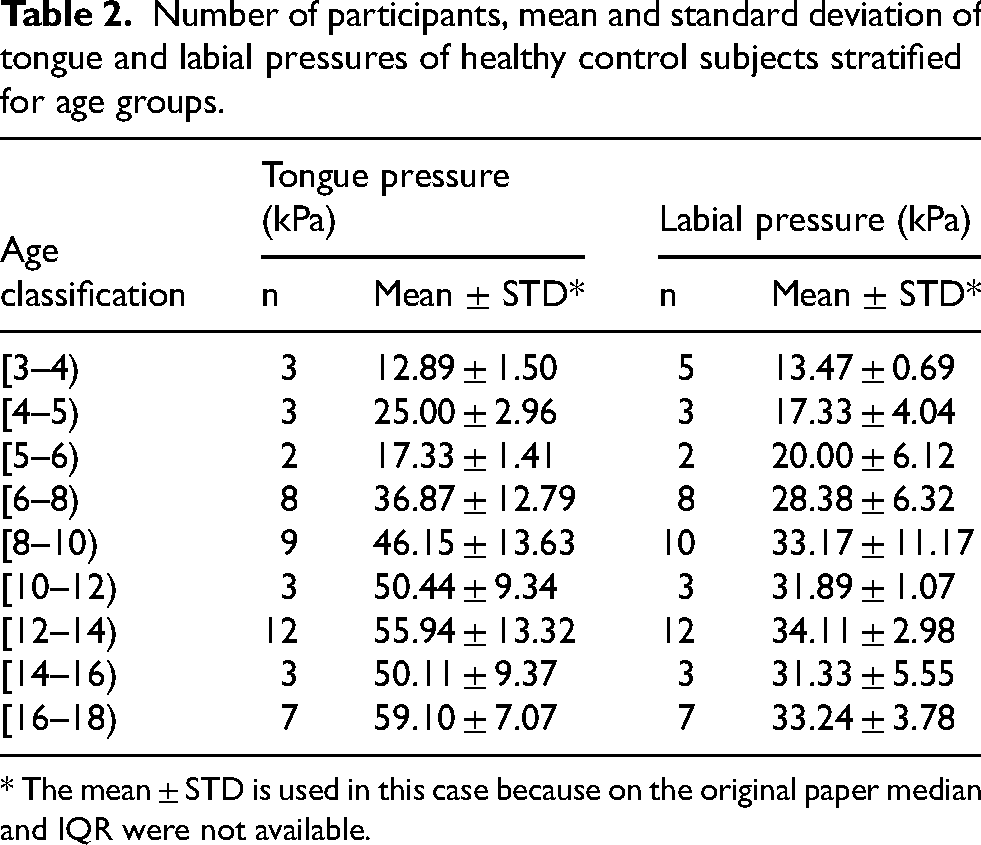
* The mean ± STD is used in this case because on the original paper median and IQR were not available.
Values of Lip and Tongue strength stratified by age in patients with SMA.
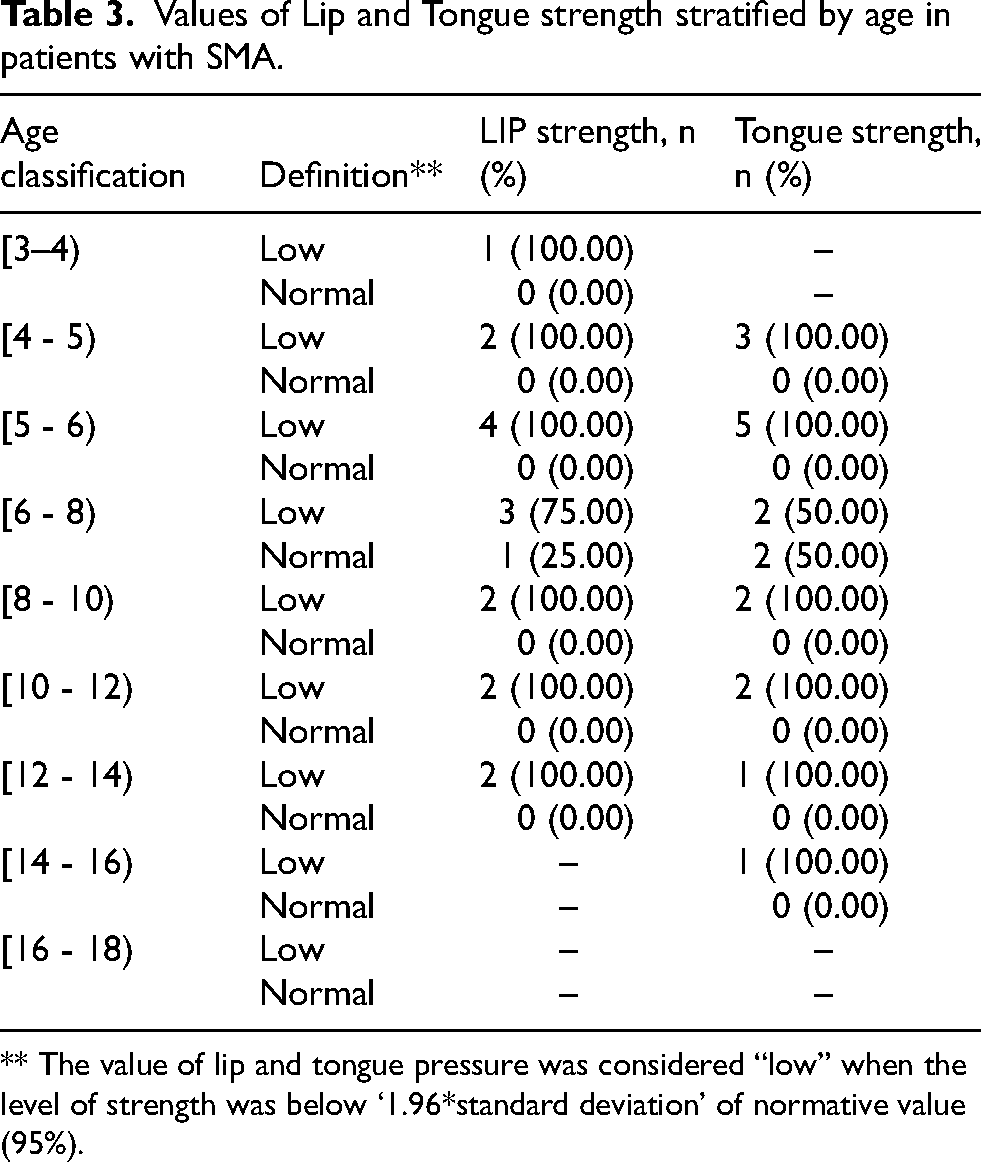
** The value of lip and tongue pressure was considered “low” when the level of strength was below ‘1.96*standard deviation’ of normative value (95%).
Associations between intraoral pressures and disease-related variables
A Spearman's rank-order correlation was conducted to assess the relationship between labial or tongue pressure and age at disease onset, age at disease-modifying treatment (DMT) initiation, treatment duration, age at IOPI evaluation, number of SMN2 copies, p-FOIS, BMI, gastrostomy and motor performance as expressed by the CHOP INTEND score.
Labial pressure vs age at disease onset
The analysis revealed a significant positive correlation, r = 0.66; p = 0.0053 indicating that the labial pressure is lower with younger age at disease onset.
Labial pressure vs age at DMT initiation
The analysis revealed a significant negative correlation, r = -0.52; p = 0.0326 indicating that the labial pressure is lower with older age at first nusinersen injection.
Labial pressure vs body mass index
The analysis revealed a significant positive correlation, r = 0.61; p = 0.0149 indicating that the labial pressure is lower with lower BMI.
Labial pressure vs CHOP INTEND scores
The analysis revealed a significant positive correlation, r = 0.60; p = 0.0170 indicating that the labial pressure is lower with worse motor performance as expressed by CHOP INTEND score (Figure 2(a)).
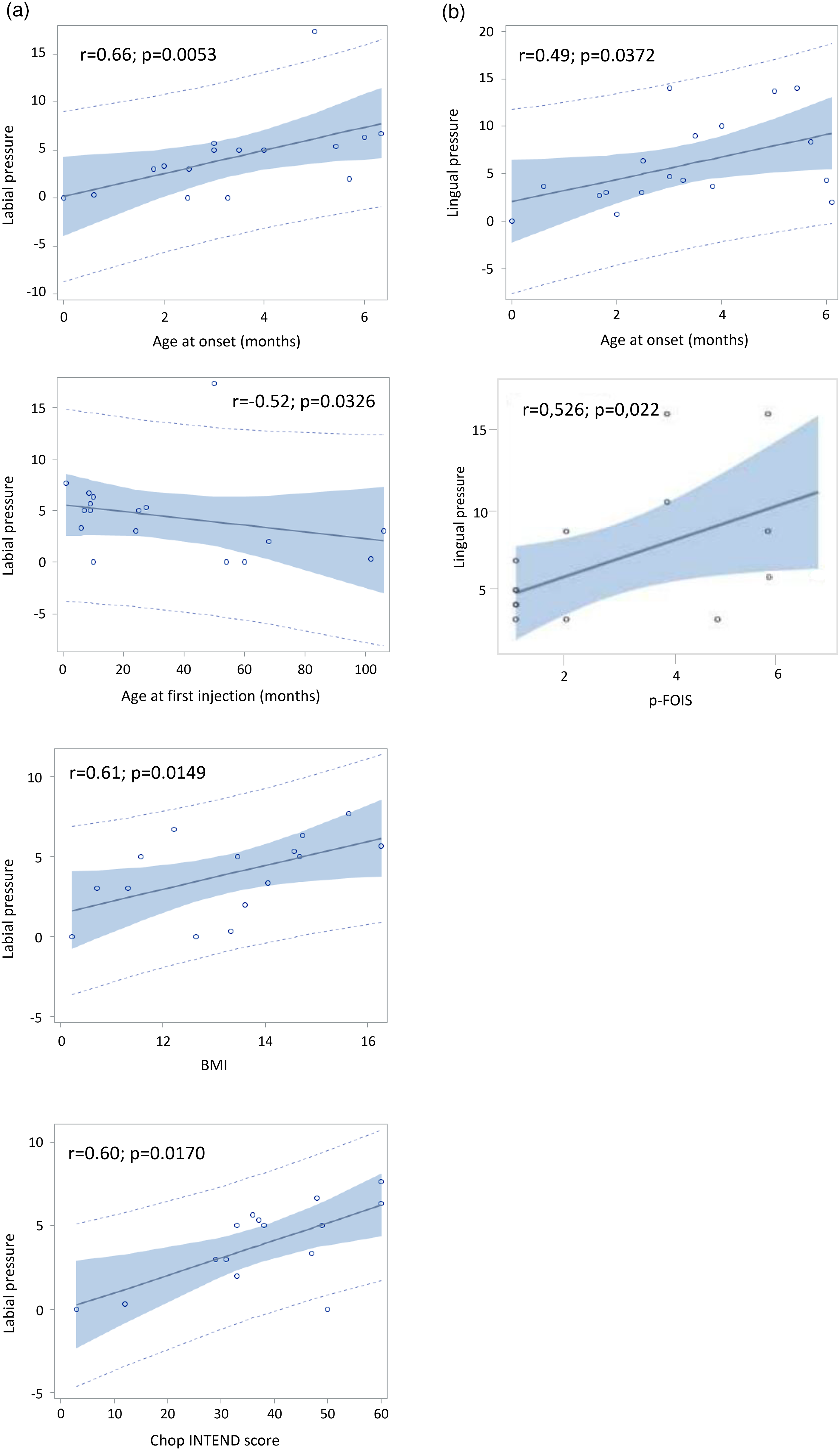
Significant correlations between intraoral pressures and clinical features and assessments (a) for labial pressure: age at disease onset, age at first nusinersen injection, BMI and motor performance as expressed by the CHOP INTEND score -b) for tongue pressure; age at disease onset, p-FOIS.
Labial pressure vs other variables
There was no significant relationship between labial pressure and treatment duration (p = 0.138), age at IOPI measurement (p = 0.050), p-FOIS (p = 0.350), SMN2 copy number (p = 0.241), presence or absence of gastrostomy (p = 0.053).
Tongue pressure vs age at disease onset
The analysis revealed a significant positive correlation, r = 0.49; p = 0.0372 indicating that the tongue pressure is lower with younger age at disease onset.
Tongue pressure vs p-FOIS values
The analysis revealed a significant positive correlation, r = 0.526; p = 0.022 indicating that the tongue pressure is lower with smaller p-FOIS values.
Tongue pressure vs other variables
There was no significant relationship between tongue pressure and age at DMT initiation (p = 0.922), treatment duration (p = 0.264), age at IOPI measurement (p = 0.484), BMI (p = 0.193), CHOP INTEND scores (p = 0.681), SMN2 copy number (p = 0.070), presence or absence of gastrostomy (p = 0.246) (Figure 2(b)).
Discussion
Direct assessment of swallowing in children with neuromuscular disorders, especially SMA type 1, remains complex and poorly reported in the literature. Most studies assess bulbar outcomes using functional swallowing measures, such as oral intake status and patient-reported outcomes. While clinically relevant, these measures have limited sensitivity because they depend on multiple personal and clinical factors rather than directly reflecting underlying bulbar integrity. Our study attempts to standardize physiological assessments of swallowing in type 1 SMA. By combining the results of two independent prospective studies conducted in geographically distinct populations, we have confirmed the relatively non-invasive, easy-to-use, and reliable nature of oral pressure measurement using the IOPI system in SMA type 1 patients. 9
This tool can be used in routine clinical assessment in children over 5 years of age because it is compact, easy to transport, and simple to use. In children under the age of 5, the assessment is more complicated due to their lack of cooperation.
As evidenced by the IOPI measurements, SMA type 1 patients displayed markedly reduced lingual and labial pressures compared to the normative data of age-matched children. Although there was considerable variability, our patient cohort consisted primarily of symptomatic patients whose median age at IOPI assessment and nusinersen treatment initiation was late, 82 months and 35 months, respectively. In a recent publication, we also demonstrated a negative correlation between IOPI-measured intraoral pressures and the Swallowing Function Assessment Questionnaire that assesses swallowing function in SMA patients. 7 Indeed, this study showed that low intraoral pressures were often consistent with subjective clinical data assessing the oral phase of swallowing in this population (e.g., chewing difficulty, weak sucking).
The decrease in pressure measured at two distinct anatomical sites is in line with previous reports of orobulbar muscle involvement and vulnerability of motor neurons in the brainstem, particularly in severe forms of SMA. 17
In SMA type 1 patients, the consequences of bulbar (lingual) motor neuron degeneration are manifested by a limited number of symptoms, in particular lingual fibrillation and progressive lingual atrophy, each of which was observed in more than 90% of the patients in our cohort, making these signs poorly discriminative in assessing swallowing function in this population. Unlike patients with ALS where atrophy and fibrillation of the tongue are very favorable and diagnostic of the bulbar presentation and generally have a worse prognosis.
Although facial diplegia as a presenting symptom of the disease has only been described in very severe neonatal forms (SMA type 0), and facial movements are generally considered to be initially preserved in the more classic form of SMA type 1, our results demonstrate the progressive occurrence of facial weakness in the majority of patients, most probably reflecting the progressive development of facial muscle damage and some form of facial amimia. 18 While facial weakness is rarely discussed in the literature, this study highlights its occurrence in SMA type 1. Consistent with these findings of facial muscle weakness, a significant reduction in the amplitude of the compound muscle action potential of the facial nerve and a concomitant reduction in motor unit size index values were observed in SMA type 2 and 3 patients compared to HCs. Moreover, the reduction was more pronounced in patients with more severe forms of SMA (type 2) compared to milder forms (type 3). 19
A recent MRI study of facial muscle volume in SMA type 2 and 3 patients revealed a reduction in muscle volume in the lateral pterygoid muscles, with relative sparing of the masseter, temporalis, medial pterygoid, anterior digastric, and geniohyoid muscles. Severe fatty atrophy of the lateral pterygoid muscles is notably implicated in the reduction of active Maximum Mouth Opening (aMMO), especially in severe SMA type 1 and 2 patients. 20 Jaw motion via aMMO was not consistently available across all patients included in the study. Future studies should investigate potential correlations between aMMO and tongue strength parameters measured using the IOPI, to better characterize the functional relationships between orofacial muscle weakness and jaw mobility in SMA patients.9,21
A reduction in strength was observed in our patients despite all are patients were on treatment with nusinersen but there are important considerations to make. Treatment was initiated late in this cohort (age at onset 3 months and age at treatment initiation 17 months) and especially there are no natural history data on the degree of muscle weakness in the tongue, lips and jaw muscles at baseline and over time. There is general consensus that in a progressive neurodegenerative disorder, a reduction in progression or a stability over time, is to be considered a positive effect and patients can be classified as “responders” in that specific domain. The lack of this information does not allow to interpret the effects of treatment, but our results provide additional data supporting the concept that feeding and swallowing difficulties remain major complications in infants with SMA type 1. 6 Despite a limited number of patients, the study by van der Heul et al. showed that SMA type 1 infants who were symptomatic at the time of nusinersen initiation still presented between 8 and 12 months of age symptoms of swallowing problems such as fatigue during feeding, silent aspiration at VFSS with the need for nasogastric tube placement for all. The study by Weststrate et al. on bulbar function using the p-FOIS questionnaire in a larger sample of symptomatic SMA type 1 patients treated with nusinersen (median age at treatment initiation: 11 months) clearly reported persistent impaired bulbar function as a significant complication in most treated patients. 3 In our study, lower p-FOIS values is associated with lower tongue pressures.
Labial and lingual pressures were positively correlated with age at symptom onset. This correlation was expected because bulbar symptoms are often reported to be more severe in patients with a severe generalized form of the disease, in whom symptoms are often observed earlier after birth, suggesting a relationship between bulbar function and disease severity.
Of interest, the results showed that labial pressure values were positively correlated with overall motor function as assessed by the CHOP INTEND (this scale does not include bulbar function assessment) and nutritional status (via BMI) in SMA type 1 patients, suggesting a correlation between facial motor strength, motor function, and weight gain evolution in these patients. However, these findings should be confirmed in longitudinal studies before being considered conclusive. The high CHOP INTEND scores observed most likely reflect the effect of medication on general motor function, and the observation of a positive correlation with labial muscle strength measurement suggests an effect of treatment on facial motor function. This is also supported by the observation of a negative correlation between labial pressure and delayed treatment initiation (first nusinersen injection). Indeed, the earlier the start of treatment, the better the patients’ labial pressure, with a minimum follow-up of 1 year and 5 months to assess treatment efficacy. These observations are in line with several studies that assessed global motor function as a function of time at treatment initiation,21,22 in which early treatment was beneficial for improving overall motor function. In terms of clinical management, this observation suggests that patients whose CHOP INTEND score on treatment remains low over time should receive increased swallowing vigilance.
Children with SMA type 1 and two SMN2 copy numbers frequently required gastrostomy. An Australian study showed that the rate of gastrostomy was significantly higher in children with two compared to three SMN2 copy numbers. 23 No statistically significant association was found however between pressures and the presence of a gastrostomy, which may be due to a lack of uniformity in the indications/criteria for gastrostomy placement or to the fact that gastrostomy may reflect difficulty in the pharyngeal phase, but this was not evaluated in this study.
Comparative data on the natural history of swallowing function in untreated SMA type 1 patients are not available. Such data are now difficult to obtain due to DMT availability, whereas in the past, swallowing assessments were not routinely performed since nearly all SMA type 1 patients required gastrostomy and invasive ventilation, rendering these evaluations of limited clinical relevance.
This study has several limitations. First, formal power calculations were not performed a priori. However, in the context of ultra-rare diseases like SMA type 1, traditional sample size calculations based on power analysis are often impracticable. The global population of SMA type 1 patients is extremely limited, and studies typically aim to recruit all available eligible patients rather than a statistically predetermined sample. This is a recognized characteristic of rare disease research, where the alternative to studying small cohorts is not conducting research at all. Despite this limitation, our findings provide valuable descriptive data and hypothesis-generating insights that would otherwise remain unexplored.
More importantly, feeding difficulties may result from dysfunction in one or more swallowing phases. With the IOPI measurement system, only the oral phase of swallowing can be studied. Oral muscle weakness affects the oral preparatory phase of swallowing and typically manifests as weakness of the sucking muscles associated with instability during sucking and chewing. In the context of SMA, especially SMA type 1, the oral phase is often complicated by structural deficits, malocclusion, or limited mouth opening. 24 This parameter was not measured in this study. Furthermore, the IOPI does not assess the pharyngeal phase of swallowing, which is also associated with significant difficulties in SMA patients.
IOPI assessment cannot be performed accurately before the age of 4–5 years, making its use difficult at earlier ages. In younger SMA type 1 patients, general clinical evaluation, weight gain evaluation, and swallowing questionnaires such as the OrSAT (under 24 months of age) and p-FOIS should be preferred. 8
Conclusions
This study confirms that objective measurement of lip and tongue strength is feasible and reliable in children with SMA type 1 from the age of 4–5 years. Compared with healthy controls, symptomatic SMA type 1 patients exhibit persistent weakness of muscles involved in the oral phase of swallowing, despite prolonged survival and marked overall functional improvement. Orofacial weakness was associated with poorer global motor function and earlier symptom onset, underscoring the importance of close monitoring of nutritional status in SMA type 1 children, particularly those treated later or presenting with severe generalized weakness. These findings further support the need for early initiation of SMN-modulating therapies.
The IOPI may represent a promising functional biomarker for assessing bulbar involvement in SMA type 1. Its use as a routine swallowing assessment tool could facilitate larger studies with repeated measurements over time, paving the way for multicenter longitudinal investigations combining objective strength assessment with qualitative swallowing evaluations. Such approaches should be complemented by validated questionnaires, scales (i.e., p-FOIS, OrSAT) and instrumental assessments such as FEES. Larger studies are needed to confirm the value of IOPI in the long-term follow-up of SMA type 1 patients. By providing an early and objective measure of orofacial weakness, the IOPI may help clinicians quantify deficits, tailor therapeutic interventions, and anticipate functional difficulties. However, the absence of validated threshold values for early risk detection currently limits its use as a standalone screening tool.
Footnotes
Abbreviations
Acknowledgments
We are grateful to the patients and parents for giving us permission to run this trial.
The authors of this article are members of the ERN EURO NMD. We thank the members of the ERN EURO NMD
Author contributions
Pr Nicolas Deconinck received consulting fees in the context of advisory Board of Biogen, Roche, and Novartis Gene Therapy.
Dr Federica Trucco reports participation in Scientific Advisory Boards for Roche UK and teaching initiatives for Biogen, Avexis, Roche, and BREAS.
Pr Giorgia Coratti received fees as consultant/advisory board member/steering committee member from Biogen, Roche, Novartis and Scholar Rock.
Pr Eugenio Mercuri received fees as consultant/advisory board member/steering committee member from Biogen, Roche, Novartis and Scholar Rock.
Pr Valeria Sansone provided scientific and educational activities for Roche, Biogen, Novartis, Dyne, Avidity, Pepgen, Arthex, Lupin.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nicolas Deconinck was supported by the FNRS (Belgium) in the context of a CDR grant (n°J.0047.20).
Fonds De La Recherche Scientifique - FNRS, (grant number J.0047.20).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data statement
Data available upon reasonable request to the authors.