
Abstract
Nerve ultrasound (n-US) supports the diagnosis of multifocal motor neuropathy (MMN), though most studies focus on nerve enlargement (NE) and its distribution. This study explored nerve echotexture using ultrahigh-frequency ultrasound (UH-FUS) in 13 MMN patients (mean age 61.9 years, disease duration 147 ± 105 months). NE was detected in 77%, preferentially involving median nerve, yet conduction blocks corresponded to NE in only 15%. Notably, 92% showed mixed/hyperechoic echotexture, including three patients with normal CSA, suggesting microstructural remodeling beyond swelling. No hypoechoic nerves were observed, consistent with limited acute inflammation. Combining echogenicity with NE assessment may improve n-US sensitivity, especially in atypical MMN.
Introduction
Multifocal motor neuropathy (MMN) is a rare, immune-mediated disorder characterized by a purely motor neuropathy without sensory loss. Its electrophysiological hallmark is the presence of conduction blocks (CB) on nerve conduction studies (NCS).1,2 Clinically, MMN typically begins with asymmetric distal weakness predominantly involving the upper limbs; as the disease progresses, the lower limbs or, more rarely, cranial nerves may also be affected.3,4 Diagnosis is based on the 2010 European Federation of Neurological Societies and Peripheral Nerve Society (EFNS/PNS) criteria and according to these criteria, CB is defined as a > 50% reduction in the negative compound muscle action potential (CMAP) area after proximal stimulation of a motor nerve. 5 However, whether CMAP amplitude 6 or area should be used to define CB remains debated.
Supportive diagnostic features include normal sensory NCS, normal or mildly elevated cerebrospinal fluid (CSF) protein, the presence of serum anti-GM1 IgM antibodies, and positive brachial plexus magnetic resonance imaging (MRI). 5 A favorable clinical response to intravenous immunoglobulin (IVIg) therapy also supports the diagnosis, with an overall sensitivity between 46% and 61%. 7 Nerve ultrasound (n-US), though not yet included among formal supportive criteria, has shown a diagnostic sensitivity up to 83%. 7 Nerve enlargement (NE), reflected by increased cross-sectional area (CSA) of peripheral nerves or brachial plexus roots, can be detected even in nerves with normal NCS.8,9 These ultrasound abnormalities do not directly correlate with CB and often persist or even progress despite clinical or electrophysiological improvement after treatment.9–12 Moreover, n-US can help distinguish autoimmune motor neuropathies from disorders characterized by axonal degeneration or lower motor neuron syndromes,13,14 though small or focal CSA increases alone are insufficient for diagnosis. 15 Combining MRI and n-US findings may improve diagnostic accuracy. 16
Only few studies have explored the underlying pathological changes in MMN, and their findings remain controversial. While some have described mild demyelination without inflammation,17,18 others, such as Taylor et al. reported mild inflammatory changes without clear demyelination at conduction block sites, 19 suggesting the coexistence of axonopathy at the site of the block with secondary distal demyelination. 2
High- and ultrahigh-frequency nerve ultrasound (UH-FUS) offer detailed, non-invasive visualization of peripheral nerve pathology. In chronic inflammatory demyelinating polyneuropathy (CIDP), hypoechoic NE reflects active demyelination, whereas hyperechoic fascicles indicate chronic inflammation with axonal loss; normal CSA with fascicular dedifferentiation suggests fibrotic or “burned-out” changes.20–22 Building on these findings, the present study aims to characterize UH-FUS (28–33 MHz) features in MMN, focusing specifically on echogenicity assessment.
Material and methods
This single-center retrospective study was conducted at the Neuromuscular Disease Center of Nice University Hospital, analyzing medical records of patients with MMN followed between 2020 and 2022. Diagnoses were established according to the 2010 EFNS/PNS criteria, 5 and the study was registered in the French clinical trials registry (NCT04978623). All participants underwent detailed neurological evaluation and UH-FUS, as part of routine care.
Demographic and clinical data included age, sex, disease duration, anti-GM1 IgM antibody status, CSF findings, and brachial plexus MRI results. Muscle strength was quantified using an adapted Medical Research Council (MRC) sum score assessing the following muscles: arm abductors, elbow flexors/extensors, wrist flexors/extensors, first dorsal interosseous, abductor pollicis brevis, abductor digiti minimi, hip flexors, knee extensors/flexors, foot dorsiflexors, extensor digiti minimi, and toe flexors. Examinations were performed by neuromuscular specialists.
All patients received maintenance IVIg infusions every 4–6 weeks and were considered clinically stable, defined as unchanged MRC scores for ≥4 months before evaluation. Electroneuromyography (ENMG; Keypoint, Medtronic) was performed within 1–3 months of ultrasound to document CB.
Ultrasound imaging was performed using two high-frequency probes (UHF33 and UHF28 MHz, Canon Aplio i800) by an experienced sonographer. The UHF33 probe (max depth 15 mm) operated in “General” mode, while the UHF28 probe (max depth 25 mm) was used for deeper structures. Bilateral median (MN) and ulnar (UN) nerves were examined from wrist to axilla. The probe was applied perpendicularly with minimal pressure, maintaining neutral limb positioning except during ulnar nerve evaluation at 90° elbow flexion. CSA was measured manually along the hyperechoic epineurial border at standardized levels: MN at wrist, 10 cm distal to wrist crease, antecubital fossa, mid-arm, and axilla; UN at wrist, 10 cm distal to pisiform, 5 cm above elbow, mid-arm, and axilla. Bilateral cervical roots C5–C7 were examined by ultrasound, measuring CSA at the level of the corresponding transverse processes, from origin to main trunk, with the patient supine and the neck slightly extended to optimize visualization.
NE was defined based on our reference thresholds (mean ± 2 SD) obtained from 20 healthy subjects aged over 18 years: MN ≥13 mm2 (wrist), ≥10 mm2 (forearm), ≥12 mm2 (antecubital fossa), ≥13 mm2 (mid-arm/axilla); UN ≥11 mm2 (wrist/forearm), ≥13 mm2 (above elbow), ≥12 mm2 (mid-arm/axilla); cervical roots C5 ≥ 11 mm2, C6 ≥ 12 mm2, and C7 ≥ 17 mm2. Correspondence between NE and CB sites was systematically recorded.
Intranerve variability (maximum/minimum CSA) was calculated for each MN and UN. Asymmetry was assessed using the side-to-side difference of intranerve variability (SSDIVA), defined as the ratio between the side with higher and lower intranerve CSA variability, according to published reference data.23,24 Asymmetry of C5–C7 nerve roots was calculated as the absolute side-to-side difference divided by the mean value and expressed as a percentage; values >20% were considered abnormal. Results are reported in Supplementary Table 1. Echotexture of MN and UN was classified as normal, hypoechoic, or mixed/hyperechoic based on revised criteria (Figure 1).20,21 The predominant pattern was defined when present in ≥10 of 20 examined sites.
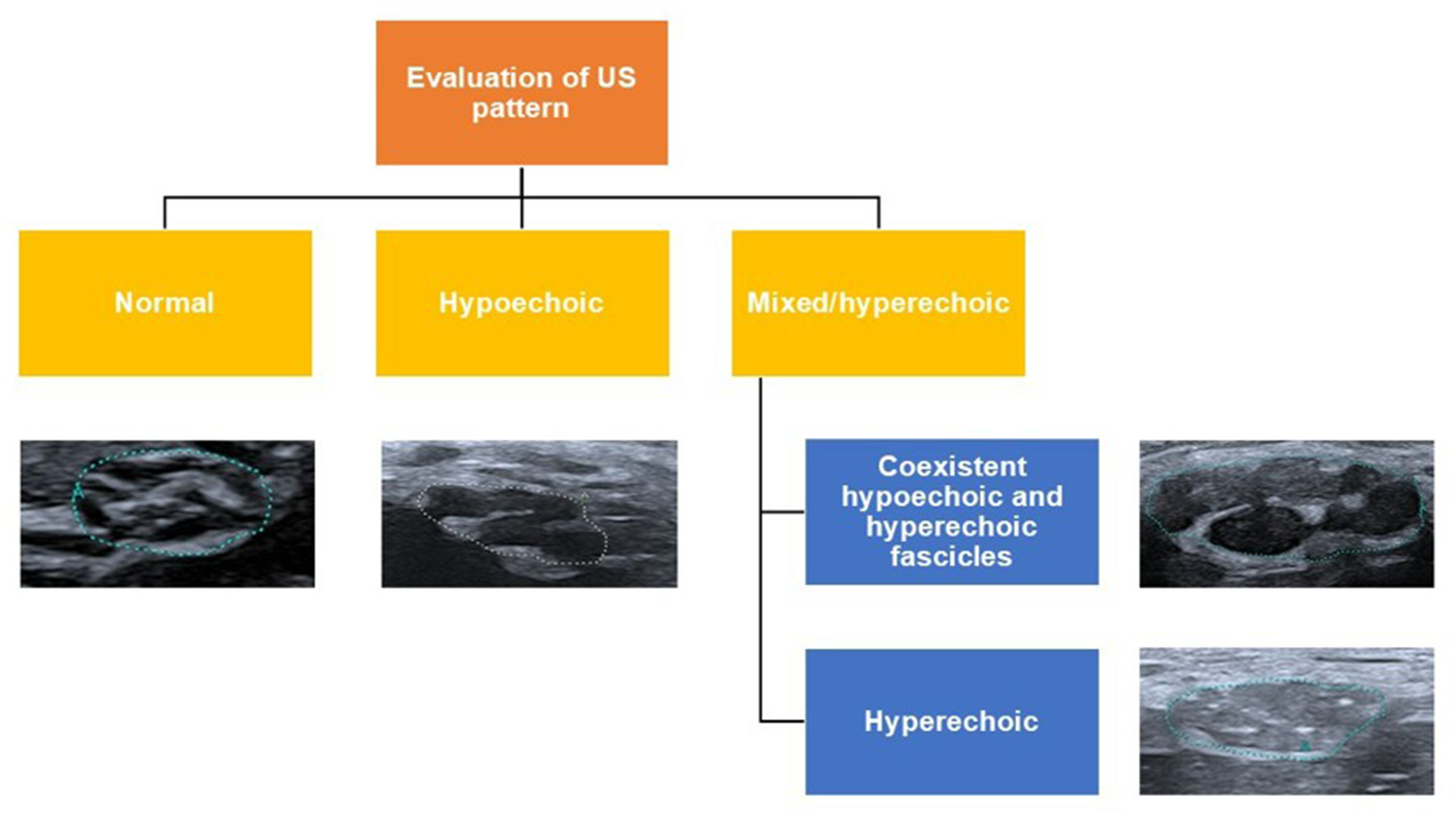
Visual assessment of ultrasound (US) echogenicity patterns and classification in normal, hypoechoic, and mixed/hyperechoic. Mixed/hyperechoic is defined by the coexistence of hypoechoic and hyperechoic fascicles or predominantly hyperechoic fascicles.
Results
Our cohort included 13 patients (nine men and four women) with a mean age of 61.9 years (range, 42–87). The mean disease duration was 147 ± 105 months (mean ± SD). According to the EFNS/PNS criteria, three patients were classified as having definite, four as probable, and six as possible MMN. IgM anti-GM1 antibodies were tested in all patients, with seven (54%) testing positive. CSF was performed in seven patients and revealed a mild protein elevation (0.55–1 g/L) in two cases (28%). Brachial plexus MRI was conducted in five patients and was normal in all instances. The main clinical and ultrasound findings are summarized in Table 1.
Demographic, clinical and ultrasound findings in our cohort (n = 13). Abbreviations: Anti-GM1 anti-ganglioside GM1; CB conduction block; CSA cross-sectional area; EFNS/PNS European Federation of Neurological Societies/Peripheral Nerve Society; F female; M male; MN median nerve; MRC Medical Research Council; NA not available; NE nerve enlargement; UN ulnar nerve; US ultrasound. Increase of CSA is highlighted in bold. For cervical roots enlargement, 0 means no enlargement, 1 means enlargement.
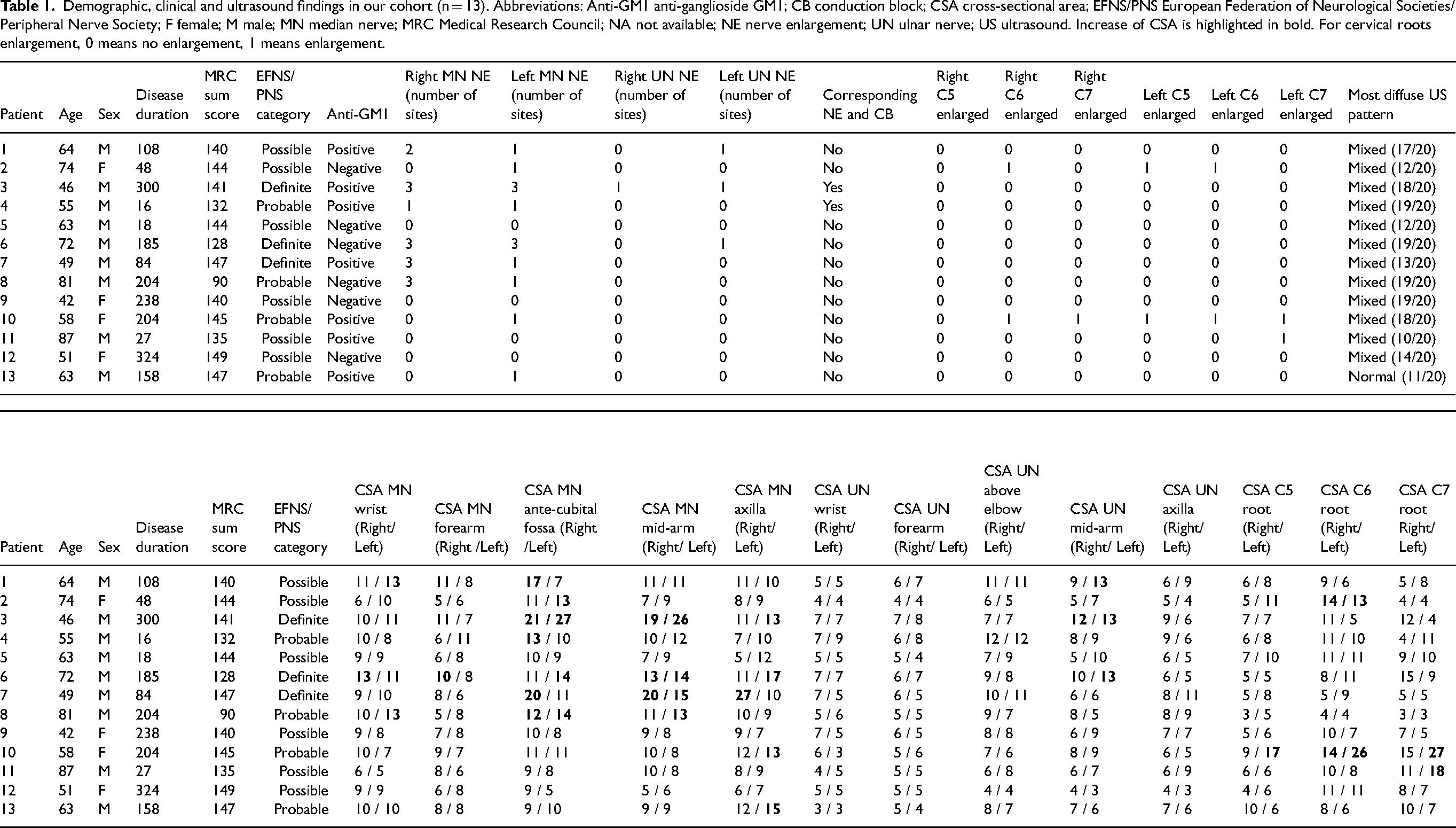
When considering CSA alone, 10 patients (77%) showed NE in at least one nerve and/or root, whereas 3 patients (23%) had normal CSA across all examined sites. The MN was the most frequently affected (n = 9, 69%), followed by cervical roots (n = 3, 23%) and the UN (n = 3, 23%). UN involvement was most often observed at the mid-arm, while MN abnormalities were detected, in decreasing order of frequency, at the antecubital fossa, axilla, mid-arm, forearm, and wrist. A definite CB corresponded to NE in only two patients (15%).
Regarding asymmetry, cervical nerve roots showed asymmetry in 92% of patients (n = 12), followed by the MN in 46% (n = 6). UN asymmetry was observed in only one patient.
Twelve of the 13 patients (92%) exhibited an altered echotexture, predominantly of a mixed/hyperechoic pattern; notably, three of these patients had normal CSA values at all examined sites and a possible MMN according to EFNS/PNS criteria. Moreover, neither the MN nor the UN showed hypoechoic echogenicity at any of the sites studied.
Discussion
This single-center study confirms the role of UH-FUS in the evaluation of patients with MMN while providing novel morphological insights through echogenicity assessment. When considering CSA, NE, although generally mild, localized, or multifocal, was observed in 77% of cases, consistent with a recent multicenter data. 7 In line with previous observations, 9 NE was more frequent in the median nerve and cervical roots and was not consistently associated with CB, with a definite correspondence observed in only a small proportion of patients. This dissociation suggests that morphological and electrophysiological abnormalities may reflect distinct disease mechanisms, 11 with ultrasound detecting structural changes that nerve conduction studies may miss.
This is the first study specifically examining the diagnostic relevance of echogenicity patterns in MMN. Loss of normal fascicular architecture and a mixed or inhomogeneous echotexture were observed in 92% of patients, consistent with diffuse nerve remodeling. These alterations were also detected in nerves with normal CSA, indicating that MMN is characterized not only by focal CSA increase but also by broader structural reorganization. This reorganization may reflect segmental demyelination, axonal loss, or intraneural fibrosis, as reported in histopathological studies.17–19 In this context, altered nerve echotexture, independently of CSA enlargement, may represent a structural marker of MMN and contribute to the identification of disease in the atypical presentations.
In contrast to CIDP, no hypoechoic nerves were detected, suggesting that edema and acute inflammation are not characteristic features of MMN. The mixed echotexture may partly reflect the long disease duration; however, it is present even in patients with a relatively shorter disease duration (approximately two years). This observation is consistent with histopathological evidence showing absent or minimal inflammatory infiltrates and supports the concept of MMN as a predominantly nodal or paranodal disorder rather than a disease characterized by diffuse demyelination or endoneurial inflammation.19,25–26
In summary, the distribution of ultrasound abnormalities shows a characteristic asymmetric pattern, with preferential involvement of proximal motor nerves and roots, which may be less accessible to routine electrophysiological assessment.8,22 Visual assessment of echogenicity, enabled using high-frequency probes (>28 MHz), combined with the evaluation of asymmetric CSA enlargement, may improve the diagnostic performance of nerve ultrasound in MMN. These features were observed across all EAN/PNS diagnostic categories (definite, probable, and possible MMN), supporting their potential relevance throughout the disease spectrum. Future studies should investigate whether UH-FUS can increase diagnostic confidence in patients classified as probable or possible MMN.
In our cohort, brachial plexus MRI was unremarkable, whereas nerve ultrasound revealed structural abnormalities in most patients, underscoring the complementary diagnostic value of UH-FUS and its high spatial resolution in detecting subtle changes in MMN. 16
Technological advances, including higher-frequency probes (>50 MHz), 24 semi-automated echogenicity analysis, and contrast-enhanced techniques, may further improve nerve microstructure characterization. 27 In CIDP, quantitative echogenicity measures have been associated with clinical progression,28,29 supporting the potential relevance of similar approaches in MMN. Longitudinal and early-stage studies are needed to determine whether echogenicity changes correlate with disease activity or treatment response.
The limitations of this study include the small sample size, the absence of interscalene trunk assessment data due to methodological constraints despite its recognized relevance in MMN,10,13,16 and the study's single-center retrospective design. Future prospective, multicenter studies integrating ultrasound, electrophysiological, standardized trunk evaluation and inclusion of a healthy control group, are needed to confirm and extend these findings.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261426071 - Supplemental material for Not only cross-sectional area: Echogenicity matters in nerve ultrasound studies of patients with motor multifocal neuropathy
Supplemental material, sj-docx-1-jnd-10.1177_22143602261426071 for Not only cross-sectional area: Echogenicity matters in nerve ultrasound studies of patients with motor multifocal neuropathy by Simona Maccora, Sabrina Sacconi, Nicolas Azulay, Mihai Bogdan Ioncea, Andra Ezaru, Michele Cavalli, Luisa Villa, Giulia Tammam, Charles Raffaelli and Angela Puma in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors have no acknowledgement to declare.
Ethical considerations
This study received approval from the relevant ethics committee and was registered in the French clinical trials registry under the identifier NCT04978623.
Authors’ contribution
SM contributed to data analysis and manuscript writing and revision. SS and CR conceptualized the study, wrote, and critically revised the manuscript. NA contributed to conceptualization, data collection and approved the final draft. MBI, AE, MC, LV, and GT collected the data and approved the final version of the manuscript. AP contributed to the study conception and data collection, participated in drafting and revising the first version of the manuscript, and approved the final version for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.