
Abstract
Background:
Prodromal symptoms of sporadic amyotrophic lateral sclerosis (SALS) including muscle cramps were reported; however, their detailed characteristics have not been sufficiently studied.
Objectives:
To clarify the detailed profiles of prodromal symptoms in SALS.
Methods:
Patients with SALS (n = 47) and healthy controls (n = 25) were enrolled. A questionnaire-based survey was conducted to investigate symptoms before and after disease onset, including sensory, autonomic, sleep, cognitive disturbances, and frequent muscle cramps. Frequent muscle cramps were defined as those occurring at least twice per month in the lower limbs, or at least once per month in the upper limbs or trunk. We evaluated the relationship between surveyed symptoms and clinical characteristics.
Results:
Prodromal frequent muscle cramps were observed in 29.8% of SALS patients, most frequently in the lower limbs. With disease progression, the sites with cramps increased, and the frequency of cramps during awakening also increased. The SALS patients with prodromal cramps had greater lean mass than those without (p = 0.023). Multivariate analysis showed that the presence of cramps after disease onset was associated with a slower longitudinal decline in the ALSFRS-R score (p = 0.048). Upper limb-onset SALS patients experienced cramps more frequently before onset than bulbar-onset patients did (p = 0.033).
Conclusions:
Frequent muscle cramps often precede muscle weakness during the prodromal phase of limb-onset SALS. The frequency of cramps increased with disease progression. Prodromal cramps were associated with lean mass, whereas cramps after disease onset were associated with a slower rate of disease progression.
Introduction
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease characterized by the rapid progression of upper and lower motor neuron loss. ALS causes muscle weakness and atrophy, leading to death in an average of 3–4 years after disease onset. 1 Many clinical trials have been conducted to find a cure for ALS, but unfortunately, no cure has been developed yet. This is partially because neurodegeneration has already advanced substantially by the time patients experience muscle weakness or atrophy. Therefore, initiating therapeutic interventions during the earlier or prodromal phases of ALS is important.
A recent study of carriers of familial ALS-causing gene mutation revealed that the prodromal phase could be recognized by symptoms such as muscle cramps, neurological examination signs, and electromyography (EMG) abnormalities that precede progressive muscle weakness and atrophy.2,3 Furthermore, the elevation of plasma neurofilament light chain (NfL) levels observed in some presymptomatic familial ALS patients 4 shows that neurodegeneration has already occurred during the prodromal phase. In addition, metabolic alterations may precede NfL changes in presymptomatic ALS gene mutation carriers. 5 Prodromal changes have also been reported in sporadic cases. For example, two studies reported that muscle cramps before disease onset are associated with rapid functional decline in sporadic ALS patients.6,7 Our recent study revealed that an increase in serum creatine kinase (CK) levels precedes the beginning of muscle atrophy. 8 A German ALS registry reported that physical activity in ALS patients starts to decrease several years before disease onset. 9 A Swedish longitudinal cohort study reported that alterations in carbohydrate, lipid, and apolipoprotein metabolism were observed 5–10 years before the disease onset of sporadic ALS, 10 indicating that the prodromal changes precede symptoms typically associated with motor neuron loss.
Therefore, it is important to comprehensively investigate prodromal symptoms of sporadic ALS beyond muscle-related symptoms, including sensory, autonomic, and cognitive symptoms. Here, we conducted a retrospective study to investigate the prodromal symptoms of sporadic ALS patients to reveal their characteristics and their relationships with clinical characteristics.
Methods
Participants
We studied consecutive patients clinically diagnosed with the revised El Escorial Criteria of definite, probable, probable laboratory-supported, or possible ALS. The principal inclusion criterion was a lack of family history. All patients with ALS were evaluated at Nagoya University Hospital. At registration, ALS patients were assessed during hospitalization at the initial evaluation and followed up every six months at the outpatient clinic of Nagoya University Hospital or by telephone. Volunteers without neurological disorders were recruited as age- and sex-matched healthy controls (HCs). HCs were assessed at the outpatient clinic of Nagoya University Hospital. All the ALS patients and HCs were Japanese and evaluated at Nagoya University Hospital between November 2015 and March 2023.
Definition of disease onset and onset site
Disease onset was defined as when the ALS patient initially recognized muscle weakness. The ALS patients were classified into three groups according to the site where they initially recognized the muscle weakness: upper limb-onset type, lower limb-onset type, and bulbar-onset type.
Questionnaire about prodromal symptoms
The questionnaire consisted of questions about the presence of sensory disturbances, autonomic disturbances, sleep disturbances, cognitive disturbances, and muscle cramp symptoms at two different time points: before disease onset and after disease onset. ‘After disease onset’ was defined as the time between the onset of weakness of any musculature and the baseline evaluation. ‘Before disease onset’ was defined as the period more than one month before disease onset. We first asked participants yes/no-questions regarding the presence of each symptom. If the response was “yes”, we further asked open-ended questions to obtain additional details, such as the timing of symptom onset, frequency, and severity.
Sensory disturbances included abnormal sensations, paresthesia, and pain. Autonomic disturbances included constipation, lower urinary tract symptoms such as frequent urination, urinary urgency, urinary incontinence, difficulty urinating, and symptoms related to orthostatic hypotension such as lightheadedness after standing up. Sleep disturbances included insomnia and symptoms related to rapid eye movement sleep behavior disorders such as dream enactment behaviors. Cognitive impairment included subjective memory impairment and symptoms related to executive function disorders.
Muscle cramps were defined as sudden, painful contractions of a muscle. The questions about the symptoms of muscle cramps were asked carefully to distinguish them from similar symptoms such as spasticity, clonus, myokymia, and fasciculation. Especially, frequent muscle cramps was defined with the following criteria: at least twice per month in the lower limbs, or at least once per month in the upper limbs or trunk.6,11 The characteristics of the muscle cramps, including the timing of the muscle cramps matching the criteria of frequent muscle cramps, the site of the muscle cramp, the severity assessed using the Columbia Muscle Cramp Scale,12,13 the situation when the muscle cramps occurred, and the medications used for the muscle cramps, were investigated. The sites of the muscle cramps were classified as the upper limb, lower limb, trunk, or neck. 12 Muscle cramps and subjective muscle weakness in each limb after the initial evaluation were also assessed regularly every 6 ± 3 months.
Blood and urine tests
Venous blood samples were collected in the supine position after more than 12 h of fasting and after waking up during hospitalization. Urine samples were also collected after more than 12 h of fasting. At the outpatient clinic, venous blood samples were collected while the patients were in the sitting or supine position after more than 12 h of fasting. Urine samples were collected and stored following the Urine & Kidney Proteome Project Standards and were coded to ensure anonymity. 14 We measured the blood serum levels of creatine kinase (CK), creatinine (Cr), cystatin C, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and neurofilament light chain (NfL). The serum levels of NfL were measured via the Simoa NF-Light Advantage Assay Kit v2 (104073) by Scrum Inc. (Tokyo, Japan). We measured the urine levels of the N-terminal titin fragment and Cr. The urine levels of the N-terminal titin fragment were measured with an ELISA system via the titin-N Fragment Assay Kit-IBL (Immuno-Biological Laboratories Co. Ltd, Gunma, Japan) according to the manufacturer's instructions.15,16 The urinary levels of the titin N-terminal fragment were standardized according to the urinary Cr level to adjust the urine concentration to pmol/mg/dL. 15
Clinical measurements
Disease severity was assessed via the Japanese version of the revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R).17,18 Pulmonary function tests, including forced vital capacity (FVC), were performed via a spirometer (FUDAC-77; FUKUDADENSHI, Tokyo, Japan). 19 Body composition was evaluated via dual-energy X-ray absorptiometry (DXA) via fan-beam technology (Discovery A; Hologic, Inc., Bedford, MA) and electromyography (EMG) using concentric needle electrodes. DXA is utilized to evaluate body composition, including lean body mass, fat mass, and bone mineral content. 20 Lean mass index (LMI) was calculated as lean mass divided by height squared (kg/m2). 21 EMG was performed by trained and experienced neurologists and assessed on muscles in four regions: the deltoid muscle, the biceps brachii muscle, and the first dorsal interosseous muscle in the cervical region; the quadriceps femoralis muscle and the tibialis anterior muscle in the lumbosacral region; the sternocleidomastoid or trapezius muscle and the tongue muscle in the brainstem region; and the thoracic paraspinal muscles in the thoracic region. The active denervation potential included fibrillation potentials and positive sharp waves. 22 The chronic denervation potential included motor unit potentials of increased duration, increased amplitude, and increased phases. 22 The DXA results, which was performed within one week after a radiological examination with contrast agents or radioisotopes, were excluded because they could influence the results. Fasciculations was defined as apparently random, spontaneous muscular twitches visible at the skin surface. 23
Statistical analysis
The chi-square test, unpaired t test, Mann‒Whitney U test, McNemar's test, Friedman test, and Wilcoxon signed-rank test were used to compare variables between the two groups. The Bonferroni correction was applied for multiple comparisons where appropriate, and the adjusted p-values are indicated in the table footnotes. In addition, logistic regression analysis was performed with the presence of muscle cramps before disease onset as the dependent variable and lean mass, age, and sex as independent variables. Data with missing values were analyzed using available cases only. With respect to missing DXA data, additional analyses were performed using multiple imputations by chained equations under the assumption of missing at random. The fully conditional specification (FCS) method with predictive mean matching (PMM) was applied as the imputation model. Multiple imputation was applied only to variables obtained from DXA, including lean mass, fat mass, and bone mineral content, which had partial missingness. A total of 100 imputed datasets were generated to ensure stable estimates. After imputation, the derived variable lean mass index (lean mass divided by height squared) was recalculated. The imputation model included the baseline clinical characteristics analyzed in this study, together with individual item scores of the ALSFRS-R and the presence or absence of muscle cramps. Variables with missing data that were not essential for the present analysis were excluded from the imputation model. Statistical analyses were performed on the pooled datasets according to Rubin's rules. For continuous variables, comparisons between patients with and without muscle cramps were conducted using independent-samples t-tests. The time from disease onset to the beginning of muscle cramps for each onset type was compared via Kaplan‒Meier estimates. The log-rank test was used to compare the Kaplan‒Meier plots among the groups, and the Bonferroni method was used as a post hoc test for each pair of groups. To perform the regression analyses, ALS patients were divided into two groups according to their age at onset, sex, site of onset, disease duration, total ALSFRS-R score, frequent muscle cramps at baseline and frequent muscle cramps before disease onset. The cutoff values for age at onset, disease duration, and the total ALSFRS-R score were set as the medians for this ALS cohort. Standardized regression coefficients were used to express β. p < 0.05 was considered to indicate statistical significance. All the data are presented as the means ± standard deviations unless stated otherwise. Statistical Package for the Social Sciences 29.0.1.0 software (IBM Japan, Tokyo, Japan) and Graph Pad Prism version 9.2.0.322 (GraphPad Software, Boston, Massachusetts, USA) were used to perform all the statistical analyses.
Results
Participant characteristics
Fifty-two patients with sporadic ALS and 25 age- and sex-matched HCs were enrolled. Five patients with ALS were excluded: one of five for severe dementia and the other four for loss of spirometry data. Finally, 47 patients with ALS and 25 HCs were analyzed.
The mean disease duration of the patients with ALS was 23.2 ± 23.1 months. The disease onset site of the patients with ALS was the upper limb for 36.2% of patients, the lower limb for 46.8% of patients, and the bulbar for 17.0% of patients. There were no patients with respiratory-onset ALS (Table 1, Supplemental Table 1 and 2).
Baseline characteristics of the patients with ALS.
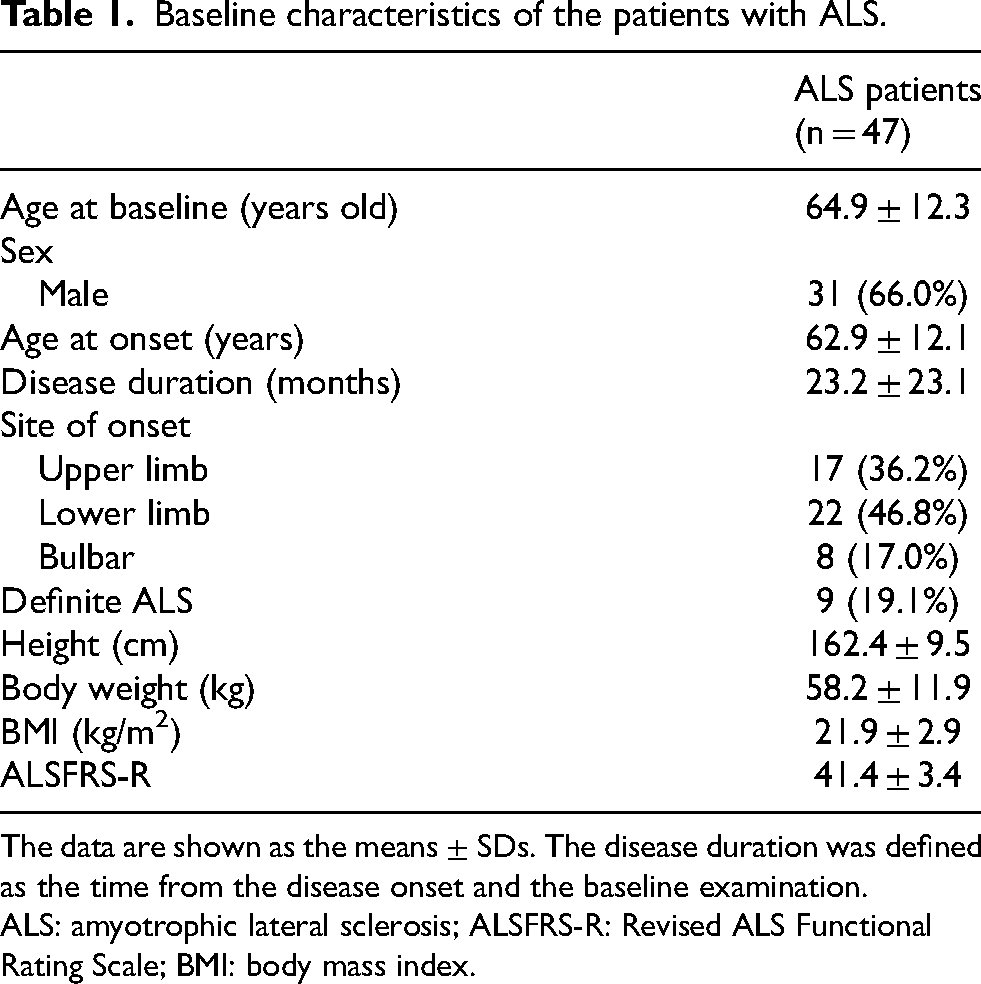
The data are shown as the means ± SDs. The disease duration was defined as the time from the disease onset and the baseline examination.
ALS: amyotrophic lateral sclerosis; ALSFRS-R: Revised ALS Functional Rating Scale; BMI: body mass index.
Comparison of symptoms between ALS patients and HCs and their longitudinal changes in ALS patients
At the baseline evaluation, there were no significant differences in the frequency of sensory disturbances, lower urinary tract symptoms, orthostatic hypotension, sleep disturbances, or cognitive impairment between the ALS patients and HCs (Table 2). Patients with ALS experienced constipation and frequent muscle cramps more frequently than HCs did. Symptoms related to sensory disturbances and cognitive impairment were unchanged in frequency from pre- to post-onset. Although constipation and sleep disturbances were observed in patients with ALS after disease onset, those frequencies before disease onset were relatively small. Frequent muscle cramps were commonly observed both before and after disease onset. Fourteen out of 47 (29.8%) ALS patients experienced frequent muscle cramps before disease onset, which began, on average, 36.2 months before the onset of muscle weakness (median: 28 months; range: 1–118 months). The occurrence of frequent muscle cramps rose to 42.6% in the post-onset phase. Overlap between frequent muscle cramps and sensory disturbances before disease onset was observed in 3 patients, however, no significant association was found (the chi-square test, p = 0.410).
Comparison of symptoms between patients with ALS and HCs.
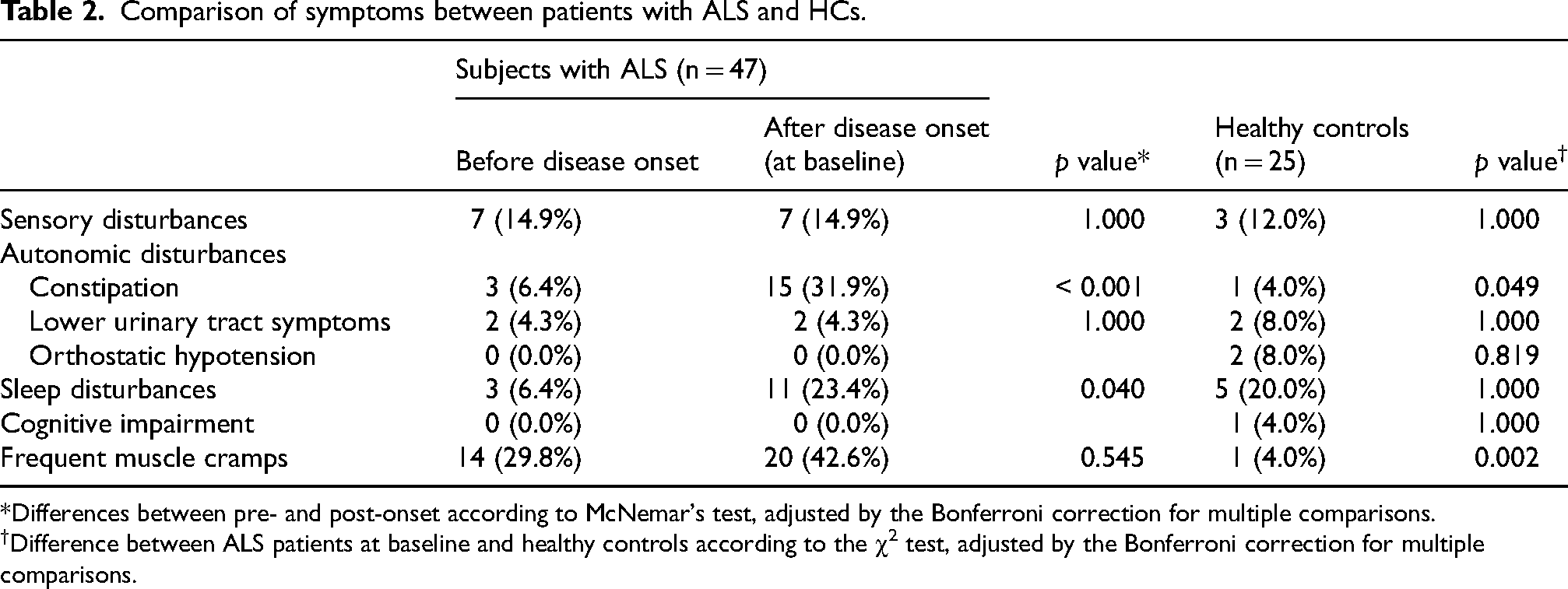
*Differences between pre- and post-onset according to McNemar's test, adjusted by the Bonferroni correction for multiple comparisons.
Difference between ALS patients at baseline and healthy controls according to the χ2 test, adjusted by the Bonferroni correction for multiple comparisons.
The most common site of the frequent muscle cramps was the lower limbs, the frequency of which increased with disease progression (Table 3). Frequent muscle cramps in other regions also increased with disease progression. The number of sites with muscle cramps significantly increased as the disease progressed. The severity of muscle cramps was mostly mild to moderate and did not differ between before and after disease onset. Frequent muscle cramps occurred more often during sleep than while awake before disease onset, whereas they occurred more often while the patients were awake after disease onset. The frequency of cramps while awake increased with disease progression. A few patients with ALS used medication for muscle cramps at any disease stage.
Longitudinal changes in frequent muscle cramps in patients with ALS.
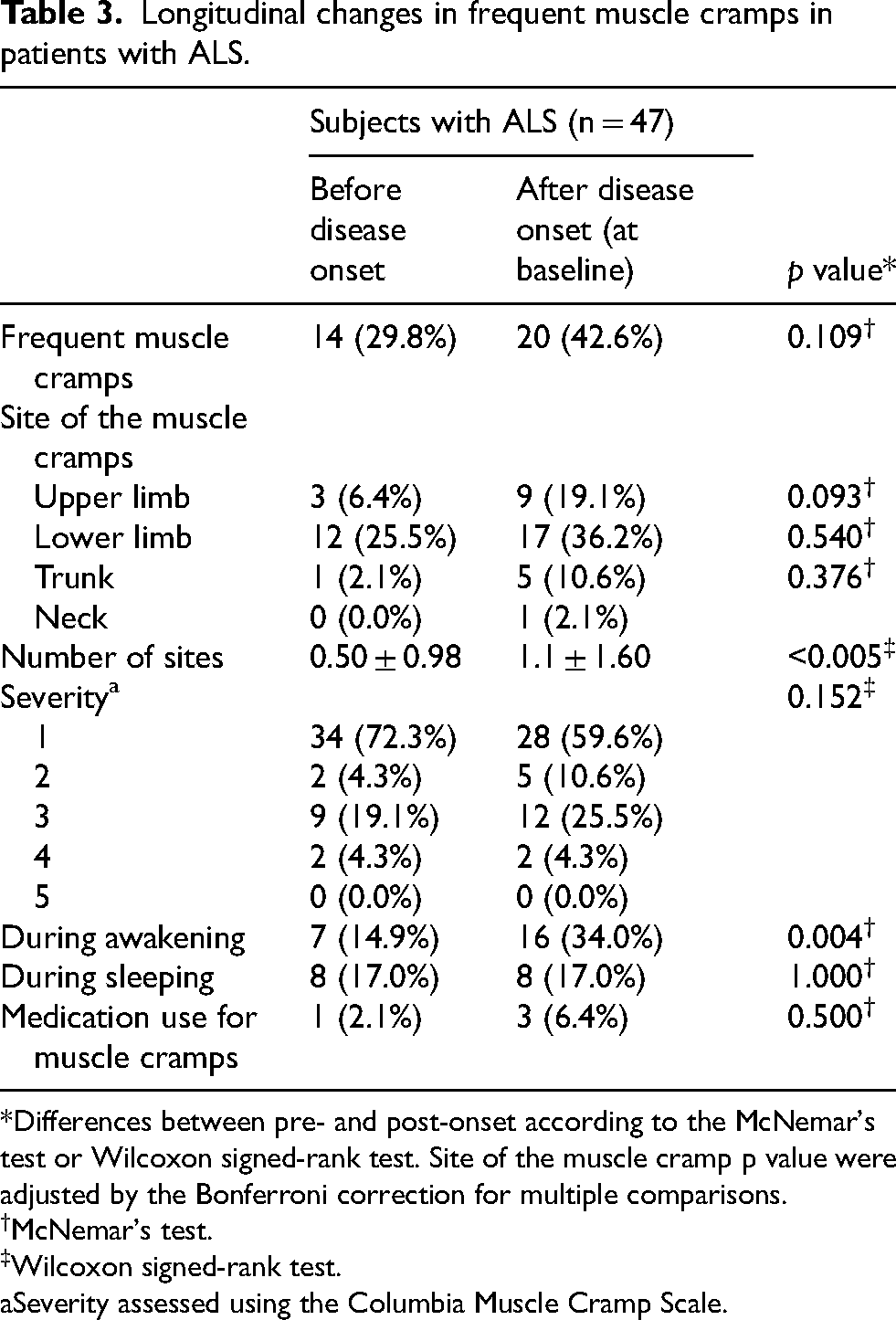
*Differences between pre- and post-onset according to the McNemar's test or Wilcoxon signed-rank test. Site of the muscle cramp p value were adjusted by the Bonferroni correction for multiple comparisons.
†McNemar's test.
‡Wilcoxon signed-rank test.
Severity assessed using the Columbia Muscle Cramp Scale.
Comparison between ALS patients with and without prodromal muscle cramps
The baseline clinical characteristics of the patients with ALS with or without frequent muscle cramps before and after disease onset are shown in Table 4 and Supplemental Table 3. ALS patients with prodromal muscle cramps had a significantly greater lean mass and Lean mass index (LMI) measured with DXA than did those without prodromal muscle cramps. After adjusting for age and sex using logistic regression analysis, greater lean mass remained significantly associated with the presence of muscle cramps before disease onset (OR = 1.240, 95% CI: 1.019–1.510, p = 0.032). This result was also confirmed in the analysis using multiple imputation for missing data (Supplemental Table 4). There was no significant difference in the spirometry, laboratory, or electromyography indices between the groups. Moreover, we did not detect differences in the ALSFRS-R scores at baseline or its progression rate between the groups. On the other hand, ALS patients with muscle cramps at baseline were significantly younger, showed a slower progression rate of the ALSFRS-R score in a prospective observation, and had lower serum NfL levels than those without muscle cramps. Multiple regression analysis revealed that frequent muscle cramps at baseline, but not during the pre-onset phase, were associated with slow progression rates in a prospective observation (Table 5). There were no significant differences in any of the characteristics between ALS patients with and without constipation and between those with and without sleep disturbances before disease onset. As for sensory disturbances, ALS patients with the symptom before disease onset had larger BMI and smaller rate of weight loss, however there was no difference in other indices. (Supplemental Tables 5–10).
Comparison of the baseline clinical characteristics between ALS patients with and without frequent muscle cramps.
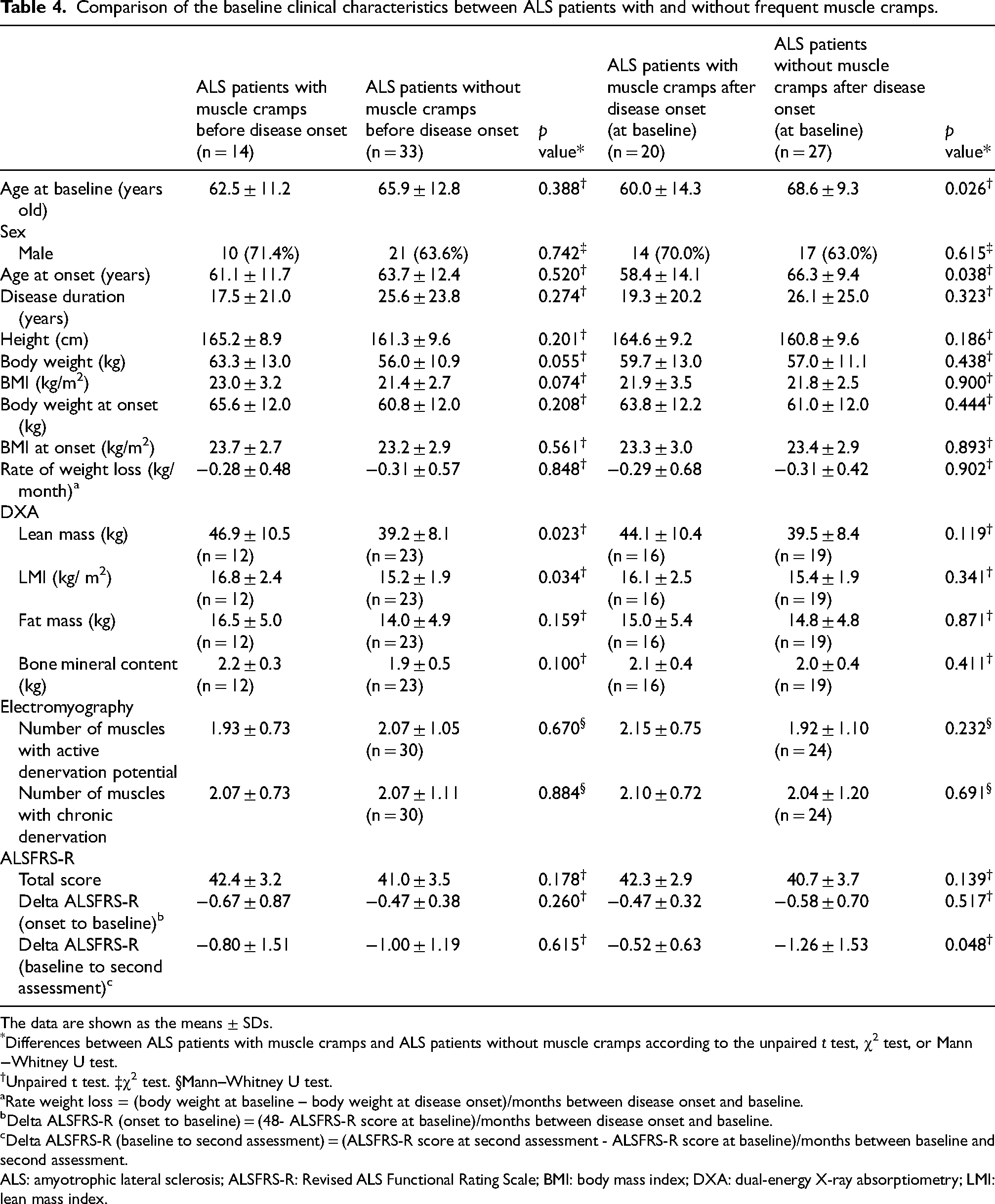
The data are shown as the means ± SDs.
*Differences between ALS patients with muscle cramps and ALS patients without muscle cramps according to the unpaired t test, χ2 test, or Mann−Whitney U test.
†Unpaired t test. ‡χ2 test. §Mann–Whitney U test.
Rate weight loss = (body weight at baseline – body weight at disease onset)/months between disease onset and baseline.
Delta ALSFRS-R (onset to baseline) = (48- ALSFRS-R score at baseline)/months between disease onset and baseline.
Delta ALSFRS-R (baseline to second assessment) = (ALSFRS-R score at second assessment - ALSFRS-R score at baseline)/months between baseline and second assessment.
ALS: amyotrophic lateral sclerosis; ALSFRS-R: Revised ALS Functional Rating Scale; BMI: body mass index; DXA: dual-energy X-ray absorptiometry; LMI: lean mass index.
Factors associated with the longitudinal decline in the ALSFRS-R score.
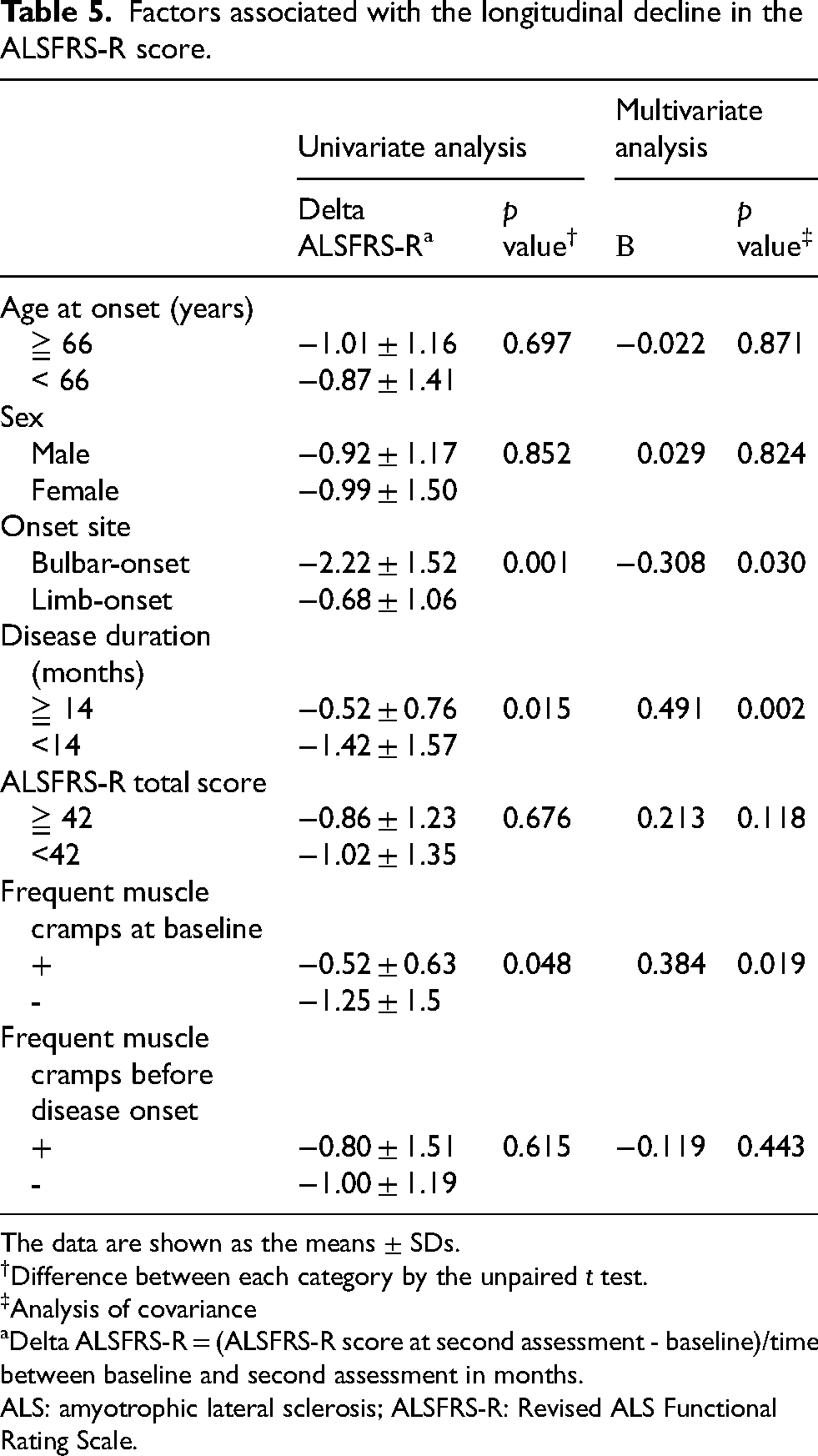
The data are shown as the means ± SDs.
Difference between each category by the unpaired t test.
Analysis of covariance
Delta ALSFRS-R = (ALSFRS-R score at second assessment - baseline)/time between baseline and second assessment in months.
ALS: amyotrophic lateral sclerosis; ALSFRS-R: Revised ALS Functional Rating Scale.
We then investigated the differences in longitudinal changes in muscle cramps between ALS patients with and without prodromal frequent muscle cramps. In patients with prodromal frequent muscle cramps, the proportion of patients with muscle cramps tended to decrease slightly with disease progression. In contrast, the proportion of patients with frequent muscle cramps increased slightly in the group without prodromal frequent muscle cramps (Supplemental Figure 1A). The frequency of muscle cramps increased in both groups as the disease progressed (Supplemental Figure 1B).
Associations between prodromal muscle cramps and the site of onset
We next analyzed the longitudinal profiles of prodromal cramps with respect to the site of onset in ALS patients. Before the onset of muscle weakness, approximately half of the limb-onset ALS patients experienced frequent cramps, but none of the bulbar-onset patients developed prodromal cramps (Supplemental Table 11). Kaplan‒Meier curves were used to visualize the relationship between the emergence of frequent muscle cramps and disease onset in patients with ALS with respect to the site of onset (Figure 1). Compared with patients with bulbar-onset ALS, those with upper limb-onset ALS experienced frequent muscle cramps more often. Although not statistically significant, a similar trend was found between the lower limb-onset and bulbar-onset patients. No significant differences were observed in the prevalence of other prodromal symptoms according to the sites of onset (Supplemental Figure 2).
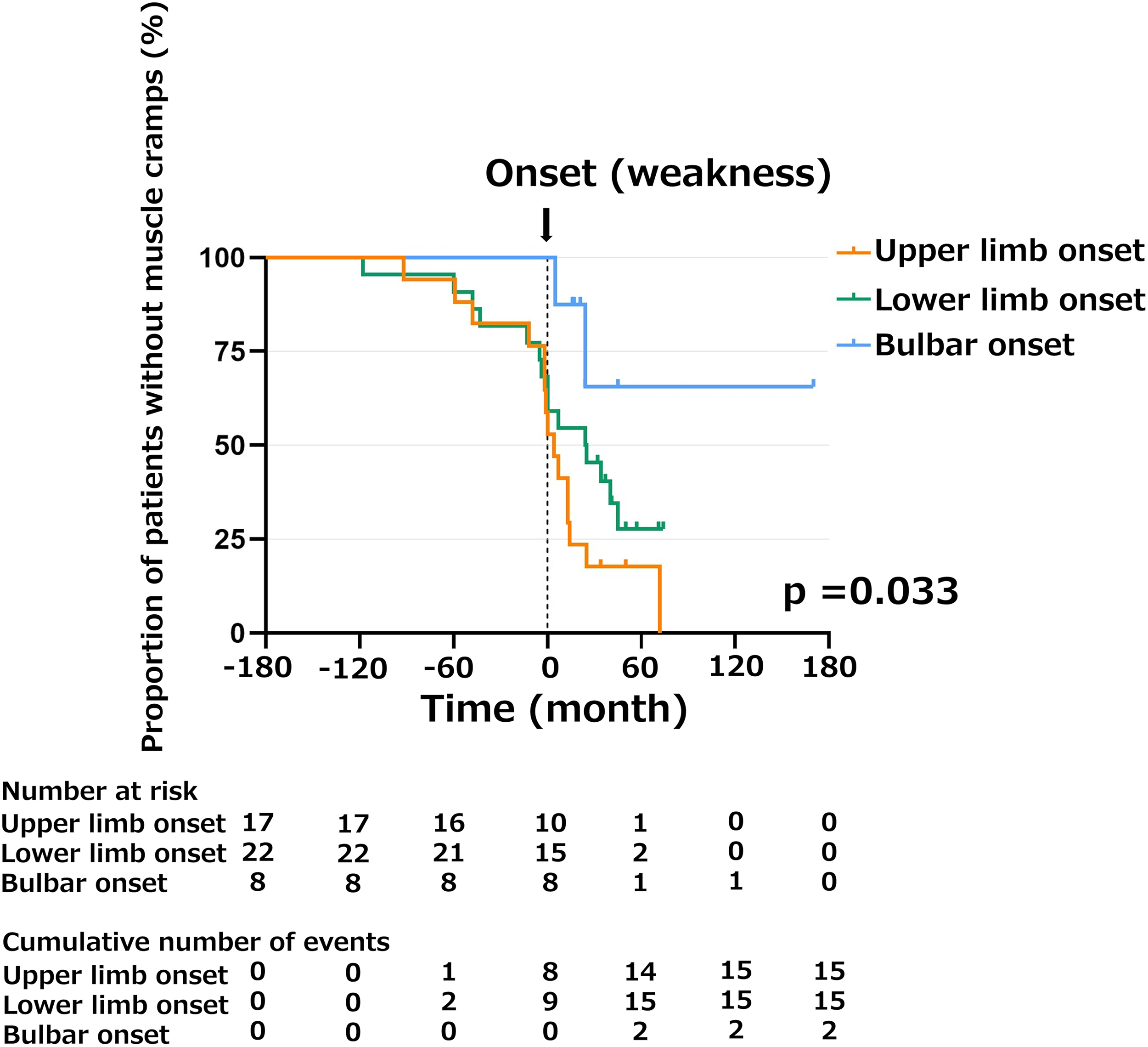
Kaplan–Meier curves of the beginning of frequent muscle cramps in patients with ALS. The Kaplan−Meier curve estimates for muscle cramps in ALS patients with upper limb onset (yellow line), lower limb onset (green line), and bulbar onset (blue line). Frequent muscle cramps were significantly different among the three groups (p = 0.033). Post hoc analyses via Bonferroni correction revealed a significant difference between the upper limb onset and bulbar onset groups (p = 0.023) but no significant difference between the other groups. The crosses indicate censored data points.
Comparison of the clinical characteristics between limbs with muscle cramps before and after weakness onset
To investigate the relationship between the initiation of frequent muscle cramps and muscle weakness within each individual limb, we selected limbs that had both frequent muscle cramps and muscle weakness at baseline. Those limbs were analyzed separately on the basis of whether the frequent muscle cramps occurred before or after the onset of muscle weakness (Table 6). Thirteen (13.8%) upper limbs and 21 (22.3%) lower limbs in 47 subjects with ALS had both frequent muscle cramps and muscle weakness. While indices of DXA, EMG, and fasciculations were equivalent between the muscles with prodromal cramps and those with post-onset cramps, upper motor neuron signs were more common in the upper limbs that presented frequent muscle cramps before muscle weakness onset than in those that presented frequent muscle cramps after muscle weakness onset.
Comparison of the clinical characteristics between limbs with frequent muscle cramps and those with weakness before baseline.
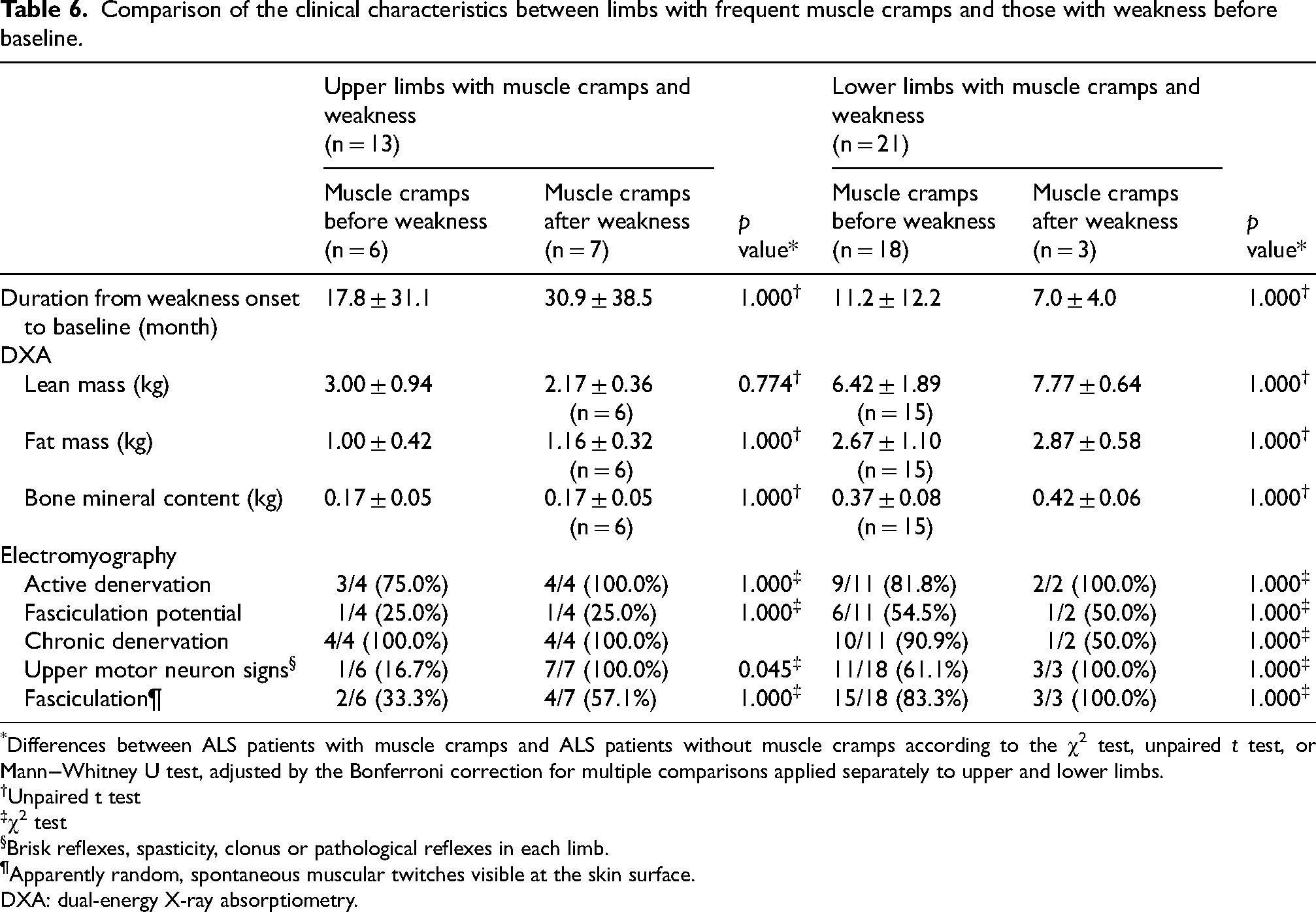
*Differences between ALS patients with muscle cramps and ALS patients without muscle cramps according to the χ2 test, unpaired t test, or Mann−Whitney U test, adjusted by the Bonferroni correction for multiple comparisons applied separately to upper and lower limbs.
†Unpaired t test
‡χ2 test
Brisk reflexes, spasticity, clonus or pathological reflexes in each limb.
Apparently random, spontaneous muscular twitches visible at the skin surface.
DXA: dual-energy X-ray absorptiometry.
Discussion
In this study, we attempted to reveal the characteristics of prodromal symptoms in ALS patients via a questionnaire-based investigation of symptoms before disease onset. Among the investigated symptoms, frequent muscle cramps were prominent at the prodromal stage of ALS, which is consistent with a previous report. 6 The present study demonstrated that 29.8% of ALS patients had frequent muscle cramps before disease onset, and the initiation of those cramps preceded the initial onset of muscle weakness by approximately three years, which is similar to the findings of previous studies reporting that muscle cramps occurred in 20–30% of ALS patients before disease onset and preceded disease onset by 15.1 ± 12.0 months.6,7 With disease progression, the number of sites with muscle cramps significantly increased, and the frequency of muscle cramps during awakening also increased. At the symptomatic stage, 42.6% of ALS patients had frequent muscle cramps, which is consistent with previous studies showing that muscle cramps occurred in 60–95% of ALS patients after disease onset, especially in those with limb-onset ALS.6,7,24 Frequent cramps were more common in patients with limb-onset ALS than in those with bulbar-onset ALS throughout the disease course.
Regarding the mechanism of muscle cramps in ALS, it is hypothesized that the lower motor neurons in ALS patients have abnormalities in Na+ and K+ conductance and that the axonal hyperexcitability of the lower motor neurons causes muscle cramps and fasciculations. 25 In a study using induced pluripotent stem cells (iPSCs) from patients with familial ALS, iPSC-derived motor neurons initially displayed hyperexcitability followed by a progressive loss of action potential output and synaptic activity. 26 Our study revealed that upper limbs with muscle cramps before muscle weakness have fewer upper neuron signs, possibly because of predominant lower motor neuron degeneration. These findings suggest that frequent muscle cramps are a prodromal symptom of muscle weakness or atrophy, reflecting early lower motor neuronal hyperexcitability.
Prodromal biomarkers have been well investigated in familial ALS. In some prodromal familial ALS patients, mild motor impairment, including abnormalities on neurological examinations and EMG, precedes subjective muscle weakness, 4 and the loss of motor units may begin as much as 16 months before disease onset. 27 Moreover, plasma NfL levels are elevated as much as 12 months before the emergence of the initial clinical symptoms or signs of ALS,4,28 indicating that motor neuron degeneration begins before the symptomatic onset of familial ALS. Although the timing of muscle cramps beginning in sporadic ALS patients in our study varied, it was similar to the timing of plasma NfL elevation in familial ALS patients, suggesting that prodromal muscle cramps reflect the beginning of motor neuron degeneration.
With respect to the relationship between clinical characteristics and muscle cramps, our study demonstrated that ALS patients with prodromal muscle cramps had greater lean body mass on DXA at the baseline evaluation. Considering that there was no significant difference in the amount of weight loss from disease onset to baseline between the ALS patients with and without muscle cramps, the lean body mass or skeletal muscle mass before disease onset would have been greater in the patients with prodromal muscle cramps than in those without prodromal muscle cramps. Frequent muscle cramps were observed more frequently in the lower limbs than in the upper limbs from the prodromal to the progressed phases. These findings indicate that frequent muscle cramps, a sign of prodromal motor neuron degeneration, are likely to occur at sites associated with high lean body mass in ALS patients. A previous study revealed that prodromal muscle cramps are related to rapid functional decline in the ALSFRS-R score. 6 In contrast, in the present study, multivariate analysis revealed that muscle cramps at baseline were associated with a prospective slower functional decline in the ALSFRS-R score, independent of known prospective factors, such as the site of disease onset. A previous study has also reported that reinnervation is associated with the preservation of muscle strength in ALS patients. 29 Therefore, in the present study, the slower disease progression observed in those with muscle cramps at baseline may indicate that the cramps resulted from hyperexcitability induced by collateral reinnervation. However, there was no significant difference in retrospective and prospective functional declines in the ALSFRS-R score between the ALS patients with and without prodromal muscle cramps. This may be due to differences in patients’ background features: the duration from disease onset to baseline was longer, and the decline in the ALSFRS-R score was smaller in the present study than in the existing literature. Further studies with larger populations are needed to clarify the relationship between the presence of prodromal muscle cramps and disease progression in sporadic ALS patients.
Our study clarified the detailed characteristics of muscle cramps in the prodromal phase in sporadic ALS patients. However, this study has several limitations. First, as this study was a single-center study and the number of patients was relatively small, selection bias could not be excluded. Particularly, the relatively small number of bulbar-onset cases in our cohort warrants cautious interpretation. Second, although the proportion of prodromal muscle cramps was similar to that reported in previous studies, recall bias may have affected the results because the investigation of prodromal symptoms was retrospective. Third, as we defined disease onset as when subjective symptoms of muscle weakness or atrophy appeared in ALS patients, there may be a discrepancy between the reported disease onset and the accurate timing of weakness initiation. Fourth, information regarding patients’ physical activity levels before and during the disease course was not collected, although they may have influenced the occurrence or perception of symptoms such as muscle cramps. Finally, upper limb cramps were relatively rare, resulting in a limited number of limbs assessed. Furthermore, the number of limbs assessed by EMG was even smaller, as EMG was sometimes performed unilaterally.
Conclusion
Frequent muscle cramps emerge as a prodromal symptom in sporadic ALS patients. In sporadic ALS patients with limb onset disease, frequent muscle cramps occur, particularly in the lower limbs, and increase with disease progression. The initiation of frequent muscle cramps may reflect hyperexcitability and subclinical degeneration of lower motor neurons before disease onset in sporadic ALS patients. Furthermore, the presence of frequent muscle cramps at baseline was associated with a prospective slower functional decline in the ALSFRS-R score.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602261422971 - Supplemental material for Characteristics of muscle cramps as a prodromal symptom of sporadic amyotrophic lateral sclerosis
Supplemental material, sj-docx-1-jnd-10.1177_22143602261422971 for Characteristics of muscle cramps as a prodromal symptom of sporadic amyotrophic lateral sclerosis by Shota Komori, Daisuke Ito, Atsushi Hashizume, Shinichiro Yamada, Yoshiyuki Kishimoto, Takahiro Kawase, Ayano Kondo, Masashi Suzuki, Mai Hatanaka, Chisato Oba and Masahisa Katsuno in Journal of Neuromuscular Diseases
Footnotes
Acknowledgment
This study was partly presented at the 64th annual meeting of the Japanese Society of Neurology.
ORCID iDs
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects endorsed by the Japanese government. This study was approved by the Ethics Review Committee of Nagoya University Graduate School of Medicine (No. 2015-0041), and all participants provided written informed consent before participation.
Contributors
SK and MK designed the study. SK, DI, AH, SY, YK, TK, AK, MS, MH and CO acquired the data. SK analyzed the data. SK, DI, AH, SY, YK, TK, AK, MS, MH, CO and MK interpreted the data. SK, DI, and MK drafted a significant portion of the manuscript and its figures. All the authors critically reviewed and approved the final version of the manuscript. No medical writer or editor was involved in the creation of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Japan Society for the Promotion of Science (JSPS KAKENHI) (Grant Numbers 23K14773 and 23H00420) and AMED (Grant Numbers JP24wm0425013 and JP24wm0625301).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.