
Abstract
In the era of disease-modifying therapy (DMT), almost all patients with spinal muscular atrophy (SMA) type I treated after onset, but before 6 months of age, develop early-onset, rapidly progressive scoliosis by 2 years of age, despite improvements in their motor function. Seven symptomatic patients with SMA type I who were treated before the age of 6 months were included in this retrospective observational study. Scoliosis had developed in all patients by 27 months of age. Among them, the patients who could stand with support or independently (standing patients; n = 3) tended to present with more progressive scoliosis than the sitters (n = 4). All standing patients demonstrated thoracic hyperkyphosis before or at the time of their scoliosis diagnosis. Despite receiving DMT, these patients continued to show residual key manifestations of SMA type I. Chronic difficulty maintaining posture due to trunk muscle weakness in the lying, sitting, or standing position was considered to be the main contributor to the development and progression of the scoliosis. The development and progression of such scoliosis, which begins in infancy, may be related to inappropriate postural management, which is not currently recognized as such by clinicians, caregivers, or guardians. In this population, it is important to closely monitor patients for such scoliosis from soon after the diagnosis of SMA. As this type of scoliosis progresses rapidly during the early developmental stage, when surgery is not possible, it is necessary to establish a proactive non-surgical management strategy for it.
Introduction
Spinal muscular atrophy (SMA) is a progressive neuromuscular disease, which is mainly caused by biallelic pathogenic variants of the survival motor neuron 1 (SMN1) gene, and its severity is indirectly correlated with the SMN2 copy number, which is a major disease modifier. 1 It is an autosomal recessive genetic disorder, with an incidence rate of approximately 1 in 10,000 live births worldwide, but its incidence is lower in Japan (approximately 1 in 20,000 live births).2,3 SMA is clinically classified into five subtypes, from type 0 (fetal onset) to type 4 (adult onset). SMA type I (in which most patients possess 2 copies of the SMN2 gene), which accounts for approximately 60% of all SMA cases, develops in early infancy, and patients with the condition are unable to sit independently in their natural courses. In the absence of disease-modifying therapy (DMT), the life expectancy of patients with SMA type I is less than 2 years. SMA type II (in which the predominant copy number of the SMN2 gene is three) is another severe phenotype of SMA, in which patients temporarily achieve independent sitting, but eventually lose the ability to sit due to disease progression. SMA types I and II together account for approximately 80% of SMA cases. 4
Currently, three innovative DMTs, nusinersen (N; an antisense oligonucleotide), onasemnogene abeparvovec (OA; a gene therapy drug delivered using a viral vector), and risdiplam (a small molecule drug), have been approved as treatments for SMA. These DMTs exhibit significant effectiveness when used for early treatment, including presymptomatic treatment.5–9 In patients with SMA type I, irreversible neurodegeneration is considered to progress rapidly from birth, with 95% of the anterior horn cells of the spinal cord being lost by 6 months of age.10,11 Therefore, early diagnosis (via newborn screening [NBS]) is essential for initiating treatment early and minimizing neuronal loss. 12 However, currently, although the implementation of NBS for SMA (SMA-NBS) is expanding globally, it remains limited to several developed countries. 13 Consequently, many patients with SMA type I still receive their initial treatment after disease onset.
Scoliosis is one of the major orthopedic complications seen in patients with SMA. Eighty percent of SMA patients present with progressive scoliosis during the natural course of their disease.14,15 It is considered to be caused by progressive axial muscle weakness and insufficient support for the growing spine. 16 In a previous study, most patients with SMA type II and patients with type III who lost the ability to walk before age 10 developed scoliosis as their disease progressed, and 80% and 71% required surgical interventions for their scoliosis, respectively, with the median age at scoliosis surgery reported to be 9.9 years of age. 17 Although there have been several studies of the natural history of patients with SMA type I,18–20 no data are available on scoliosis in these patients. This is because many children with the condition die early, and scoliosis in SMA type I patients was not a focus of research prior to the availability of DMTs.
In the DMT era, early onset and rapidly progressive scoliosis develops by 24 months of age in almost all SMA type I patients treated with DMT after disease onset, but before 6 months of age.21,22 Most early-onset scoliosis develops and progresses from around 5 months of age and is characterized by rapid progression, with the Cobb angle increasing at a mean rate of 2.3 degrees per month. In SMA type I patients with scoliosis who exhibited a Cobb angle of 40 degrees or more, a decline in motor function was observed despite treatment with DMT. 21 Moreover, while the scoliosis progression rate was reduced in patients with milder types of SMA whose motor function was improved by DMT, it increased in patients with SMA type I, even though their motor function was also improved by DMT. 23 Therefore, we consider that there are specific pathological conditions that underlie the early onset and rapid progression of the scoliosis seen in SMA type I. However, there is limited data about this early-onset scoliosis. In this multicenter retrospective study conducted across 12 Japanese SMA centers, we characterized the onset, progression, and contributors to early-onset scoliosis in SMA type I patients in whom DMT was initiated within 6 months of birth.
Study design and participants
This study was approved by the ethics committee of Osaka Women's and Children's Hospital (protocol code: 1701, 11 March 2023). A waiver of the need to obtain informed consent was also approved due to the retrospective nature of the study, in which existing data that did not include any identifiable private information were analyzed, and we displayed an opt-out notification in the participating hospitals. The inclusion criteria were (i) patients with genetically confirmed SMA (either homozygous deletion of, or a compound heterozygous mutation in, SMN1) born between April 2017 and March 2023, and (ii) symptomatic SMA patients in whom DMT was initiated within 6 months of birth, as such patients almost inevitably develop early-onset scoliosis by 24 months of age.21,22
The clinical data of each patient were gathered from study groups, including information regarding age, SMN2 copy number, age at symptom onset, age at diagnosis, the selected therapeutic agent, age at the start of treatment, age at the start of rehabilitation, the frequency of rehabilitation, tracheostomy status, and tube feeding status. The motor function of each patient was evaluated by reviewing The Children's Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP-INTEND) score, Hammersmith Infant Neurological Examination Section 2 (HINE-2) score, and Hammersmith Functional Motor Scale-Expanded (HFMSE) score, which are commonly used to evaluate the motor function of patients with SMA. 24 These scores were determined every 3 to 6 months.
The degrees of scoliosis, lumbar lordosis, and thoracic kyphosis in each patient were evaluated every 3 to 12 months by obtaining spinal X-rays in both the frontal and sagittal planes and measuring the Cobb angle, which is the angle formed by the extension of the most inclined terminal vertebral endplate, every 3 to 6 months. Scoliosis, lumbar hyperlordosis (LHL), and thoracic hyperkyphosis (THK) were defined as Cobb angles exceeding 10, 60, and 50 degrees, respectively.25,26 Basically, spinal X-rays were taken in the supine position and also in the sitting position when possible. Trends in Cobb angle progression were determined by assessing the changes in the angle between each timepoint.
Statistical analysis
Continuous variables are reported as medians and ranges. Given the limited sample size, formal statistical comparisons were not performed. Data management and descriptive analyses were conducted using GraphPad Prism (GraphPad Software, San Diego, CA, USA).
Results
Included patients and the regions of Japan covered by this study
Between April 2017, when DMT drugs for SMA were approved for use in our country, and March 2023, there were forty patients with newly diagnosed SMA at our 12 study institutions, which cover approximately 20% of the regions of Japan. Twenty-one patients had SMA type I, and seven of them met all of the inclusion criteria for this study (Table 1). One of these seven patients (case 3) was diagnosed through NBS and treated with DMT after symptom onset at 25 days of age. SMA-NBS was initiated in some areas of Japan in 2019 and has gradually expanded to other parts of the country. As of 2023, SMA-NBS only covered approximately 50% of Japan, and this study included a mixture of one case that was diagnosed through SMA-NBS and other cases that were diagnosed in general medical practice after the onset of symptoms.
Characteristics of each included case.
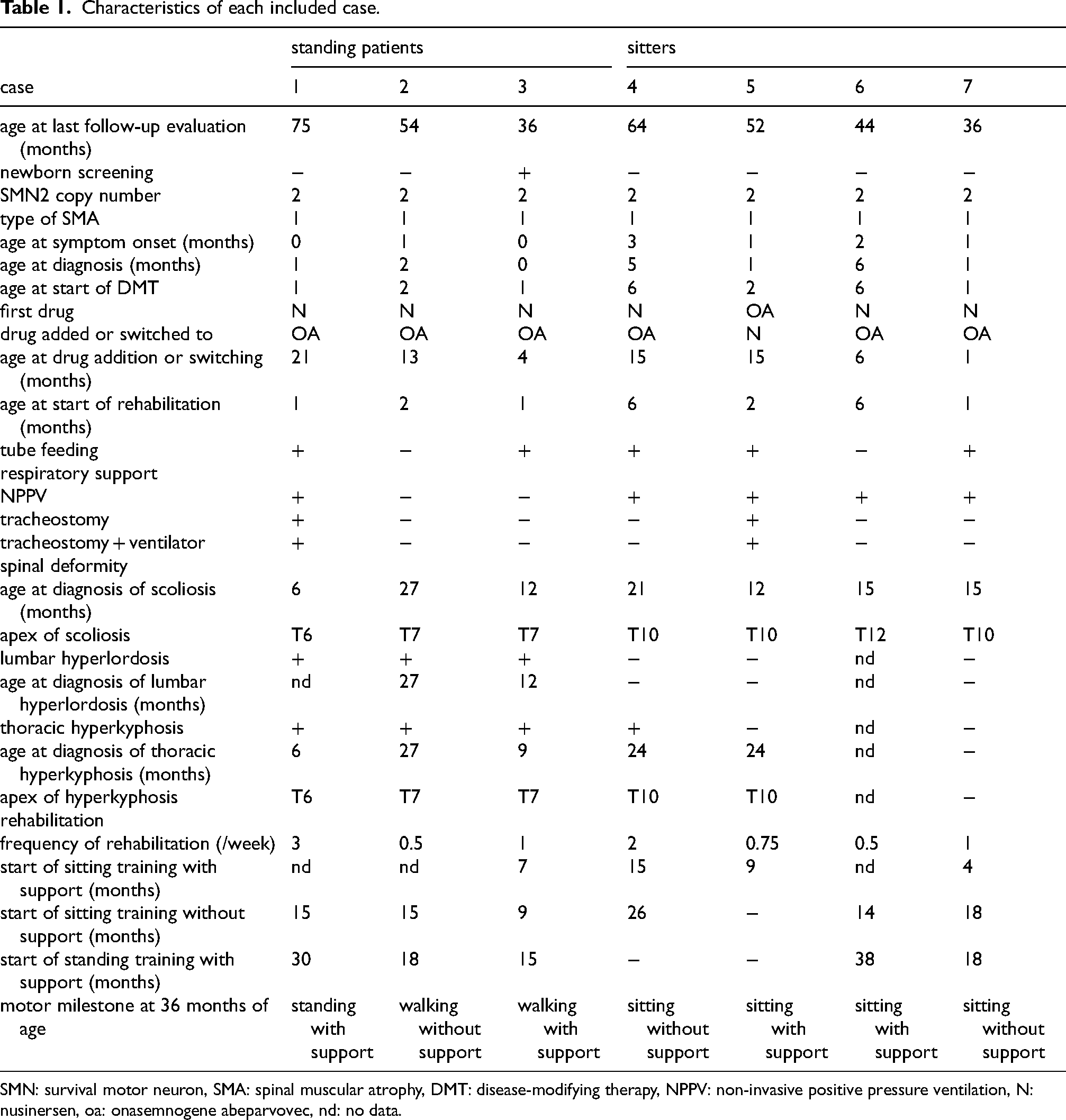
SMN: survival motor neuron, SMA: spinal muscular atrophy, DMT: disease-modifying therapy, NPPV: non-invasive positive pressure ventilation, N: nusinersen, oa: onasemnogene abeparvovec, nd: no data.
Clinical features of all patients
All of the subjects had two copies of the SMN2 gene. The median age at the onset of SMA symptoms was 1 month (range: 0–3 months), the median age at the diagnosis of SMA was 1 month (0–6 months), and the median age at the initiation of treatment with DMT was 2 months (0–6 months). Bridge therapy with N followed by OA was initiated in 6 patients. One patient was initially treated with OA before receiving add-on therapy with N. Five patients required tube feeding. Five patients required respiratory support with non-invasive positive pressure ventilation, and two of them subsequently required tracheostomy and mechanical ventilator support. Tracheostomy was performed in case 1 at 9 months of age due to recurrent aspiration pneumonia and in case 5 at 24 months of age due to recurrent respiratory infections. The median CHOP-INTEND scores for the patients at 3 and 6 months of age were 26 (11–42) and 34 (15–44), respectively (Figure 1, Supplementary material). Three patients were able to stand with support or independently at 36 months of age (standing patients), and the other patients were classified as sitters.
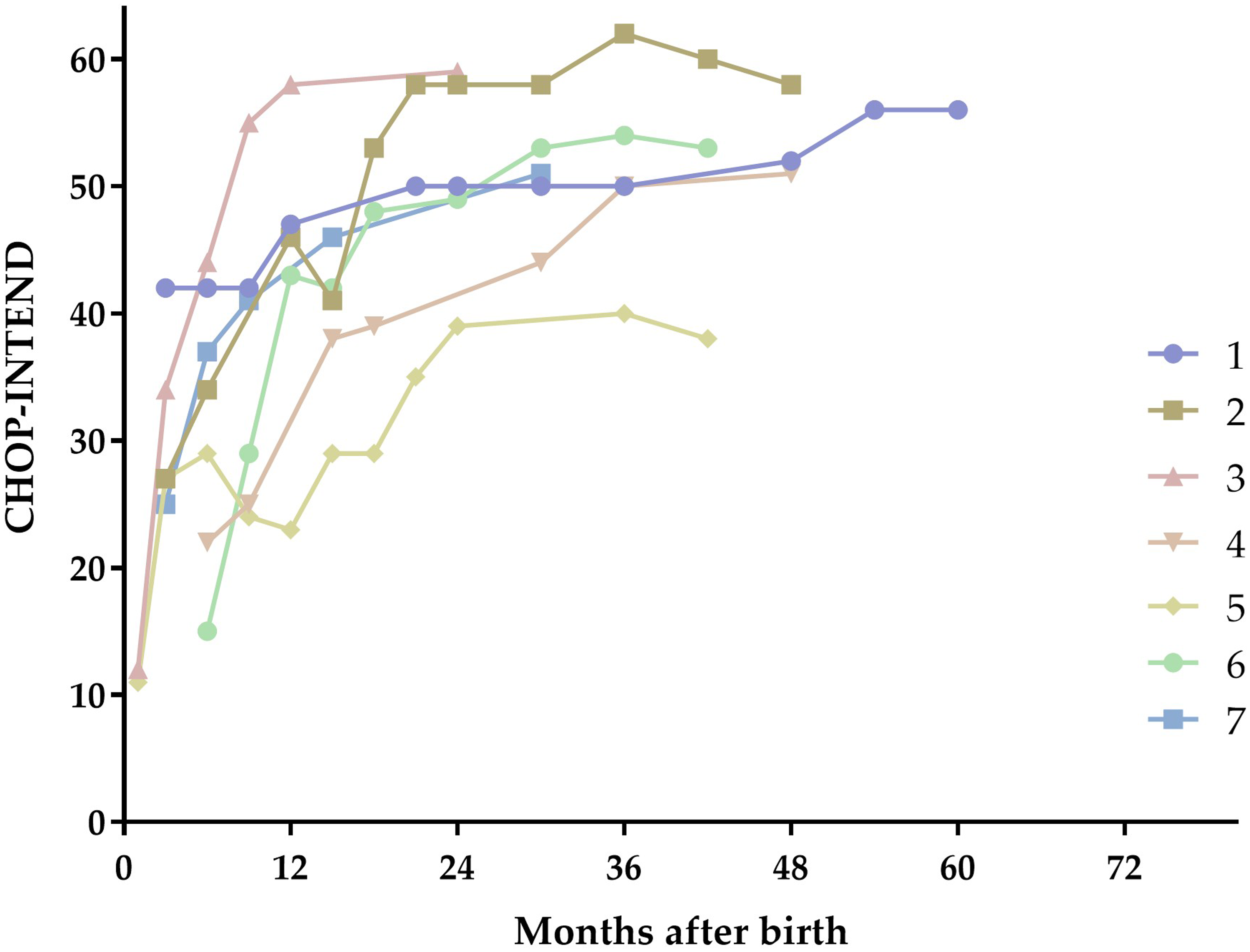
The course of the motor function improvements in each case
Scoliosis was identified in 15 of 21 patients (71%) with SMA type I at our study institutions, and in all 7 patients included in this study. Of these, scoliosis was diagnosed in 5 patients by 18 months of age, in 6 patients by 24 months of age, and in all patients by 27 months of age (Figure 2, Supplementary material). The median age to the diagnosis of scoliosis was 15 months (6–36 months). The median Cobb angle at the diagnosis of scoliosis was 23 degrees (14–37 degrees). The mean Cobb angle progression rate (MPR-C) was 0.98 degrees/month from birth to the last evaluation in all patients. In the 5 patients that developed scoliosis by 18 months of age, the MPR-C was 1.63 degrees/month. At the final follow up, the Cobb angle exceeded 40 degrees in 3 of 7 patients. None of the patients exhibited declining motor function during their clinical courses (Figure 1). LHL and THK were observed in 3 and 4 of 6 patients, respectively (there were no data for one patient). The apex of the kyphosis and the apex of the scoliosis in each case were located at the same vertebral level (Figure 3). Six patients were diagnosed with scoliosis after the start of sitting training. The median age at the start of sitting training was 9 months (4–15 months) (Table 1).
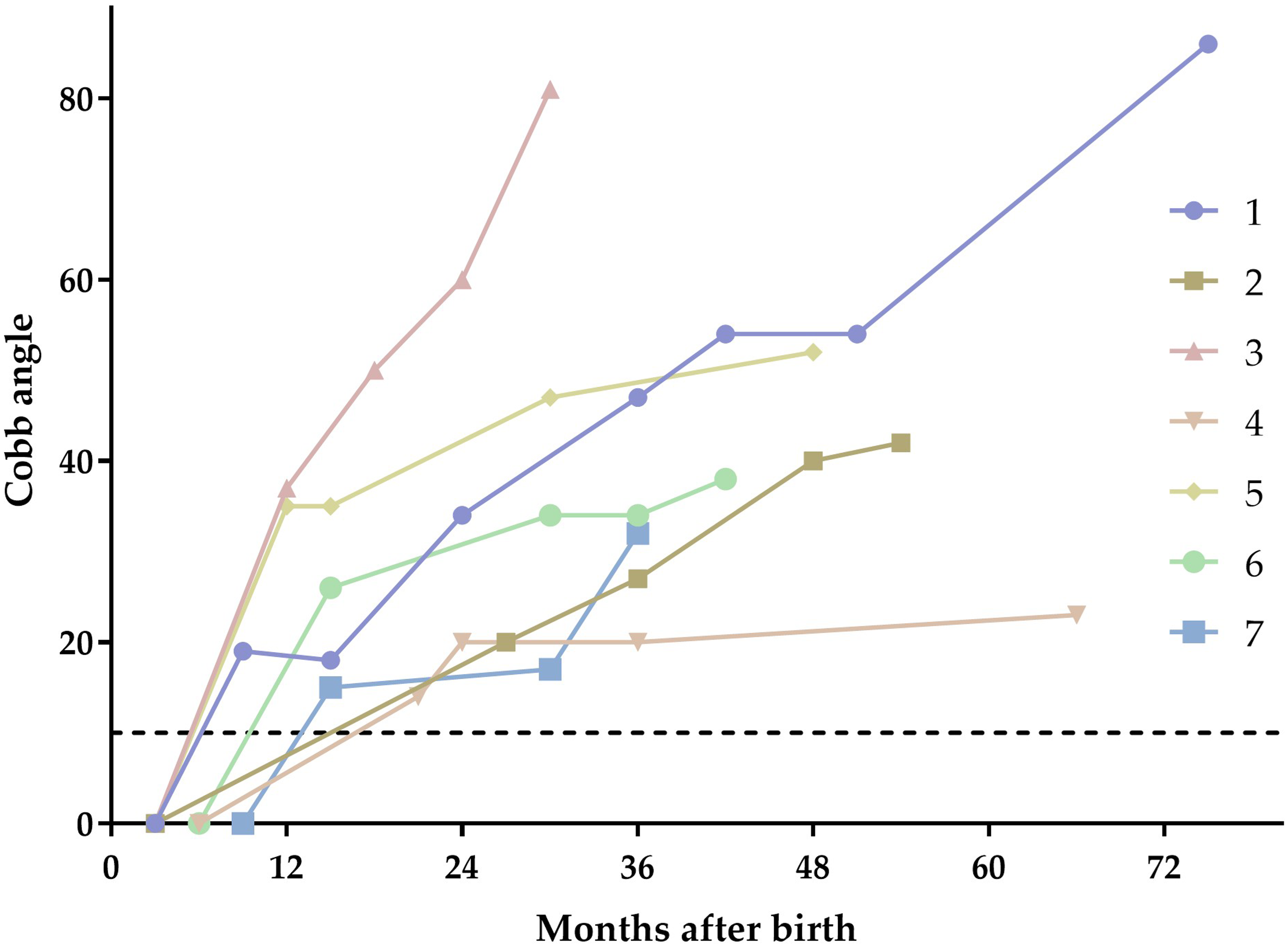
The progression of scoliosis in each case
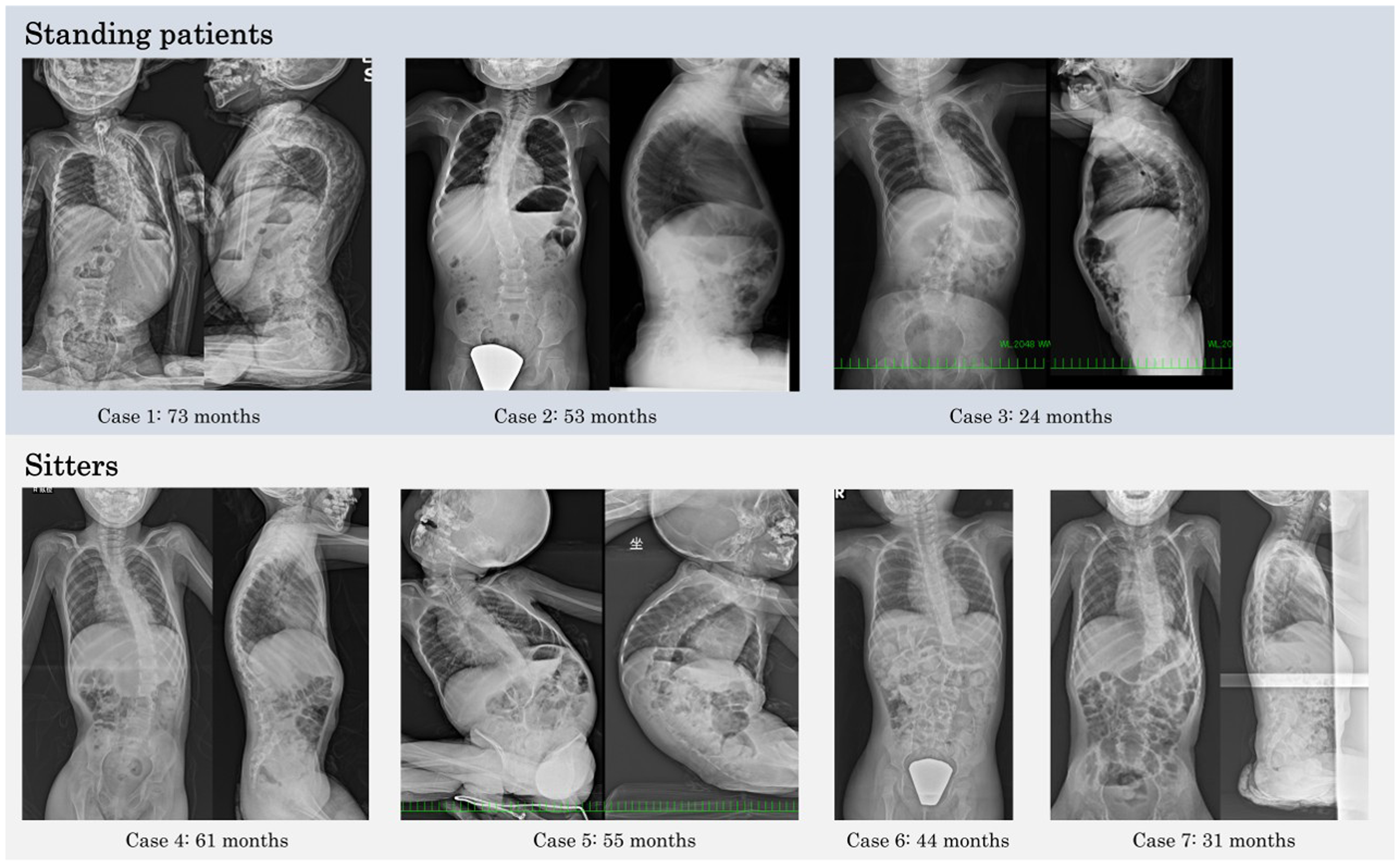
Spinal X-rays in each patient with progressive scoliosis
Comparison of the standing patients and sitters
The median age at the onset of SMA symptoms was 0 months (range: 0–1 months) for the standing patients and 1.5 months (range: 1–3 months) for the sitters (Table 1). In these groups, the median age at diagnosis was 1 month (range: 0–2 months) and 3 months (range: 1–6 months), respectively; the median age at the initiation of treatment with DMT was 1 month (range: 0–2 months) and 4 months (range: 1–6 months), respectively; the median age at the diagnosis of scoliosis was 12 months (6–12 months) and 15 months (12–21 months), respectively; and the median Cobb angle at the diagnosis of scoliosis was 23 degrees (20–37 degrees) and 20.5 degrees (14–35 degrees), respectively. The MPR-C from birth to 36 months of age was 1.43 degrees/month and 0.92 degrees/month in the standing patients and sitters, respectively (Figure 4). In the standing patients, the MPR-C was greater after the start of standing training (median: 1.00 degrees/month, range: 0.81–3.50 degrees/month) than from birth to the last evaluation before standing training (0.50 degrees/month, 0.28–2.92 degrees/month). Thoracic scoliosis was noted in all patients, but the scoliosis apices were located at T6–7 and T10–12 in the standing patients and sitters, respectively. All 3 standing patients had THK before or at the diagnosis of scoliosis. The median age at the diagnosis of THK was 9 months (6–27 months).
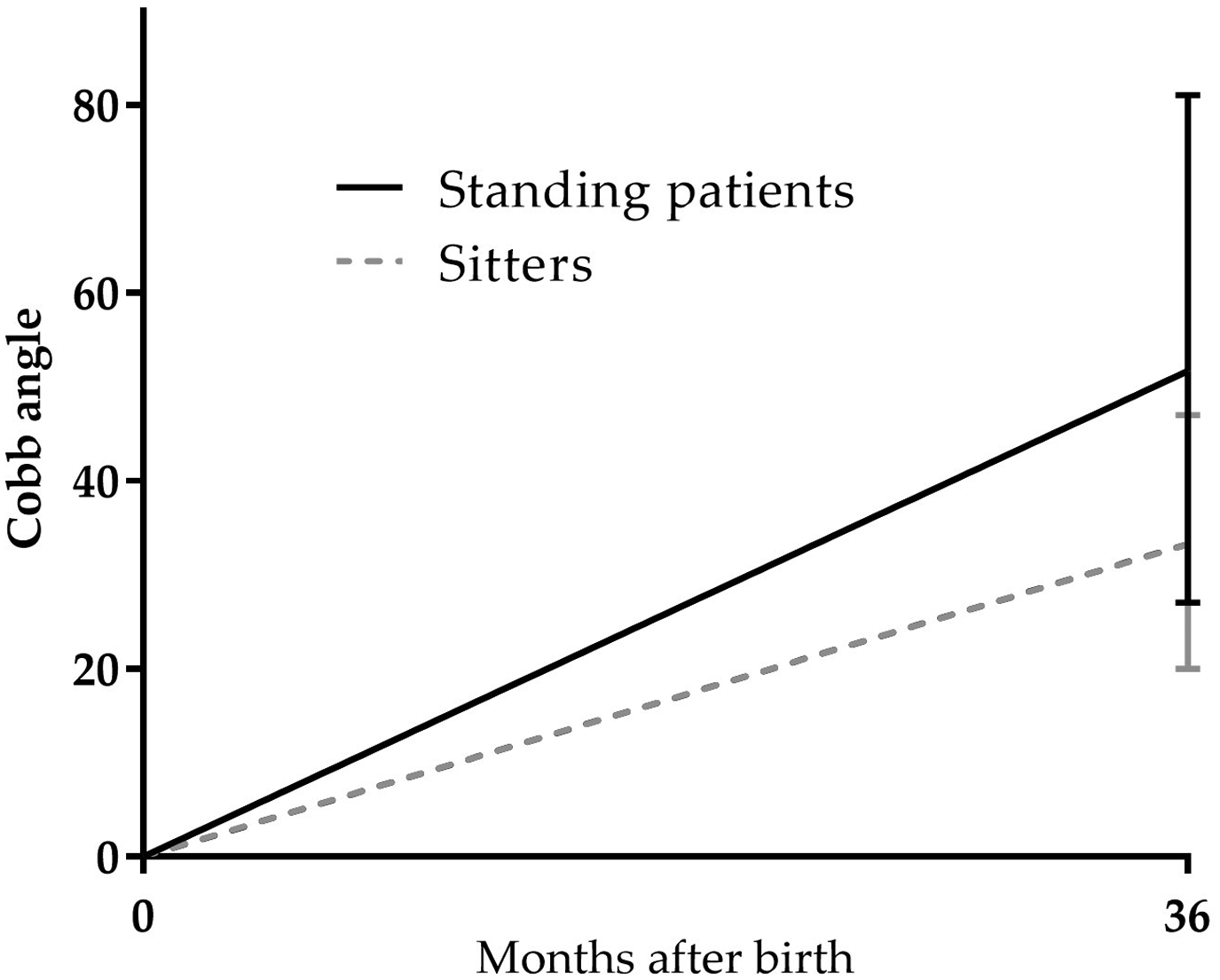
The difference in the scoliosis progression rate from birth to 36 months of age between the standing patients and sitters
The especially impressive clinical course of case 3
The patient in case 3 was diagnosed through NBS, but was already symptomatic before they were treated with DMT, and had no congenital spinal deformities. The patient's CHOP-INTEND score increased from 34 at 3 months of age to 59 at 2 years of age. Sitting training was started from 7 months of age. The patient was able to sit independently at 1 year of age and was able to walk with support at 2 years of age. While the patient's motor function improved greatly, THK was first identified at 9 months of age, and scoliosis and LHL were also identified at 12 months of age. The scoliosis progressed rapidly thereafter. The Cobb angle increased from 37 degrees at 12 months of age to 81 degrees at 30 months of age. The apex of the scoliosis was located at T7. Rehabilitation in this case began at two months of age. However, due to limited clinical awareness of such early-onset scoliosis, adequate postural management was not implemented. Consequently, the patient was often held upright in a kyphotic posture during infancy, and by 2 years of age, when they exhibited scoliosis, they often sat with insufficient postural support at home.
Discussion
The early-onset scoliosis described in previous studies as inevitably developing in 93–100% of patients with SMA type I that are treated with DMT after symptom onset, but within 6 months of birth, was also seen in our study.21,22 In larger case series, the incidence of spinal deformity in SMA type I treated with DMT was approximately 80%, 27 whereas in this case series the median treatment initiation age was 12 months, suggesting the inclusion of milder cases. Our included seven patients comprised relatively more severe patients with a correspondingly higher risk of scoliosis. Thus, this early-onset scoliosis can be considered to be a problem that is only seen in a very specific subgroup of patients with SMA type I who are diagnosed symptomatically and treated early with a DMT. However, even if SMA-NBS is widely implemented, approximately 20% of patients detected by NBS are already symptomatic at the time of diagnosis,28,29 and hence, such early-onset scoliosis is likely to persist in this population. Although the motor function of such patients can be improved with DMT, they still exhibit significant manifestations of SMA type I, such as generalized muscle hypotonia, respiratory problems, and dysphagia, during their developmental courses. In our study, the patients in cases 1 and 3, for whom clinical data from infancy were largely available, already had scoliosis in infancy, when they still exhibited neck instability and could only roll over in bed. Therefore, the infantile-onset spinal deformities seen in these cases suggest that, as well as a chronic poor posture driven by generalized hypotonia and inappropriate postural management (for example, excessive upright holding or premature sitting practice with insufficient postural support) contributed to this early-onset scoliosis. After they were able to sit unsupported, ongoing inadequate head control and trunk muscle weakness, especially the inability to support their own head weight, likely promoted both the development and progression of scoliosis and may have affected where on the spine the scoliosis occurred. Although the factors that affect where on the spine the apex of scoliosis is located are unclear, the higher apex and faster Cobb-angle progression seen in the standing patients may imply that head-support demands concentrate stress on the cervical-thoracic spine more than on the lower thoracic region.
In our study, the standing patients showed more rapid scoliosis progression than the sitters. Similarly, a previous study showed that treated SMA type I patients with better motor function had more progressive scoliosis, although the number of reported cases was limited. 23 These results suggest that the rapid progression of early-onset scoliosis should be monitored closely in symptomatic patients with two copies of SMN2, especially patients with greater potential for DMT-induced motor function improvements, such as post-onset patients diagnosed through NBS and those that are treated earlier. We hypothesize that the greater progression of scoliosis seen in the standing patients was because of the imbalance caused by the fact that their motor milestones improved relatively quickly, but their muscle strength and endurance remained immature. As a result, they exhibited poor postures when seated or standing more frequently and for longer periods than the weaker sitting patients. As THK in such cases is considered to present in infancy before the onset of early-onset scoliosis, repeated careful evaluation for spinal deformity, including the identification of risk factors associated with inappropriate postural management, is considered to be required from immediately after the diagnosis of SMA.
Our study had several limitations. First, it was a retrospective study with a small sample size. In addition, the data obtained from the patients were heterogeneous, and some were lacking. Unfortunately, routine spinal X-rays were only taken after the onset of scoliosis in most cases. In case 2, scoliosis was first evaluated at 27 months of age, but was suspected to have actually developed before 24 months of age. As sagittal X-rays were rarely taken, the evaluation of sagittal spinal deformity before the onset of scoliosis was insufficient. Given the small number of cases, the finding that the scoliosis of the standing patients progressed more rapidly than that of the sitters may have been influenced by significant selection bias. Further accumulation of cases is needed to clarify this issue. Furthermore, little data were available on aggravating factors related to the onset of this early-onset scoliosis, such as how long the patients with trunk weakness spent sitting without support in their daily lives, due to a lack of awareness of this early-onset scoliosis among healthcare providers. In addition, no association between scoliosis and rehabilitation was identified due to the small number of cases and insufficient data. Therefore, prospective studies involving standardized imaging protocols and detailed posture monitoring are required. As this early-onset scoliosis progresses rapidly, we recommend combining frontal and sagittal spinal X-ray evaluations conducted in the supine position every 6 months with inspection and palpation for spinal deformities at each visit from the time of SMA diagnosis until 24 months of age. If spinal deformity is detected, shortening the imaging interval to every 3 to 4 months should be considered, with careful attention paid to minimizing cumulative radiation exposure.
Regarding treatment for scoliosis in patients with SMA, non-surgical treatments, such as a spinal brace, are usually recommended for pediatric patients. However, there is no evidence that bracing is effective at preventing the progression of such scoliosis, and surgical treatment is required if the scoliosis progresses.24,30,31 Growth-friendly surgery, including instrumentation with magnetic growing rods, is recommended for cases of early-onset scoliosis in pediatric patients under 8 years of age.30,32 However, such surgery is highly invasive and carries a high risk of postoperative complications. In addition, upper thoracic scoliosis and thoracic kyphosis are additional risk factors for complications. 33 It is generally desirable to perform these surgeries after school age. 34 The progression of this early-onset scoliosis starts in infancy, usually without physicians, caregivers, or guardians being aware of it. As it progresses rapidly during an early developmental stage when surgical management is impossible and may impair motor function improvements in SMA patients treated with DMT, a proactive non-surgical management strategy for this scoliosis that can be initiated soon after the diagnosis of SMA should be established to prevent scoliosis or delay surgical intervention as long as possible.
Although all of our patients underwent routine rehabilitation after the initiation of DMT, our results suggested that rehabilitation based on standard policies was insufficiently effective at preventing the progression of this early-onset scoliosis. On the other hand, we recently reported the case of a 6-year-old SMA type I patient, who was treated with DMT after onset and exhibited slight early-onset scoliosis at 15 months of age, but his scoliosis was prevented from progressing with an aggressive rehabilitation program focusing on postural management, while his motor development continued to progress. 35 Our experience suggests that proactive physical therapy that is started immediately after the diagnosis of SMA type I and focuses on continuous, careful postural management, including support for the head's weight, the avoidance of poor habitual postures, and antigravity positional training, under close postural supervision may be effective at preventing the progression of this early-onset scoliosis and at promoting appropriate motor improvements following DMT. We are currently conducting a prospective study to evaluate the efficacy of close monitoring and proactive rehabilitation interventions focusing on postural management for preventing such early-onset scoliosis in SMA type I patients treated after onset, with the hope of establishing a specific rehabilitation strategy for SMA type I patients in the DMT era (registration number: UMIN000053208).
Conclusions
Although our data are insufficient for drawing definitive conclusions about the clinical features of this early-onset scoliosis, its clinical course in some cases suggests that it develops and worsens during infancy due to the residual key manifestations of SMA type I and inappropriate postural management (that is not currently recognized as such by clinicians, caregivers, and guardians). Notably, the condition may worsen more rapidly in patients who demonstrate greater DMT-induced improvements in motor function. In this population, including patients diagnosed through NBS, it is important to be aware of the possibility of such scoliosis developing soon after diagnosis, to monitor its progression closely, and to document in detail all potential risk factors that could lead to inappropriate postural management. Further studies involving larger numbers of cases and closer early follow-up are needed to clarify the clinical prognosis of this early-onset scoliosis. Interventions aimed at mitigating any identified risk factors for this early-onset scoliosis may suppress its progression. We hope that, through such continuous efforts, a practical management strategy for such early-onset scoliosis will be established.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251414327 - Supplemental material for Characteristics of early-onset, rapidly progressive scoliosis in spinal muscular atrophy type I treated with disease-modifying therapy -a multicenter retrospective study conducted in Japan-
Supplemental material, sj-docx-1-jnd-10.1177_22143602251414327 for Characteristics of early-onset, rapidly progressive scoliosis in spinal muscular atrophy type I treated with disease-modifying therapy -a multicenter retrospective study conducted in Japan- by Tomokazu Kimizu, Reiko Arakawa, Mikiko Hasegawa, Tomoko Mizuno, Ryosuke Bou, Emiko Kobayashi, Toshio Saito, Kazuhiro Muramatsu, Yoshi-Ichiro Kamijo, Tamaki Kato, Kenji Inoue, Mitsuo Motobayashi, Yuichi Abe, Keisuke Oki, Saki Yokawa, Daisuke Tamura and Keiko Yanagihara in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgements
We would like to thank Prof Kayoko Saito, MD, PhD, for her expert advice on SMA for this article. We are grateful to all study participants for contributing their data.
Author contributions statement
Tomokazu Kimizu: Writing - original draft, Visualization, Project administration, Methodology, Investigation, Formal analysis, Conceptualization, Funding acquisition; Reiko Arakawa: Writing - review & editing, Visualization, Resources, Methodology, Investigation; Mikiko Hasegawa: Writing - review & editing, Visualization, Resources, Methodology, Investigation; Tomoko Mizuno: Writing - review & editing, Resources; Ryosuke Bou: Writing - review & editing, Resources; Emiko Kobayashi: Writing - review & editing, Resources; Toshio Saito: Writing - review & editing, Supervision; Kazuhiro Muramatsu: Writing - review & editing, Supervision; Yoshi-Ichiro Kamijo: Writing - review & editing, Supervision; Tamaki Kato: Writing - review & editing; Kenji Inoue: Writing - review & editing; Mitsuo Motobayashi: Writing - review & editing; Yuichi Abe: Writing - review & editing; Keisuke Oki: Writing - review & editing; Saki Yokawa: Writing - review & editing, Methodology; Daisuke Tamura: Writing - review & editing, Methodology, Supervision; Keiko Yanagihara: Writing - review & editing, Methodology, Supervision
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Japan Agency for Medical Research and Development (AMED) under Grant Number JP25dk0310127.
Declaration of generative AI and AI-assisted technologies in the writing process.
During the preparation of this work, the authors used Microsoft Copilot in order to improve the manuscript's readability and language. After using this tool, the authors have reviewed and edited the content as needed and take full responsibility for the content of the publication.
Declaration of competing interests
The authors declare the following financial interests/personal relationships, which may be considered as potential competing interests: Tomokazu Kimizu reports consulting fees from Chugai Pharmaceutical Co., Ltd, and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan; Chugai Pharmaceutical Co., Ltd; and Novartis Pharmaceutical Co., Ltd Reiko Arakawa reports consulting fees from Chugai Pharmaceutical Co., Ltd; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan, Chugai Pharmaceutical Co., Ltd, Novartis Pharmaceutical Co., Ltd, and Roche Korea Co., Ltd; and participation on Data Safety Monitoring Boards and Advisory Boards for Biogen Japan, Chugai Pharmaceutical Co., Ltd, and Novartis Pharmaceutical Co., Ltd Mikiko Hasegawa reports consulting fees from Chugai Pharmaceutical Co., Ltd, and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan; Chugai Pharmaceutical Co., Ltd; and Novartis Pharmaceutical Co., Ltd Ryosuke Bou reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan; Chugai Pharmaceutical Co., Ltd; and Novartis Pharmaceutical Co., Ltd Emiko Kobayashi reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Chugai Pharmaceutical Co., Ltd, and Novartis Pharmaceutical Co., Ltd Toshio Saito reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan and Chugai Pharmaceutical Co., Ltd, and payment for expert testimony from Biogen Japan and Chugai Pharmaceutical Co., Ltd Kazuhiro Muramatsu reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan and Novartis Pharmaceutical Co., Ltd Tamaki Kato reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan; Chugai Pharmaceutical Co., Ltd; and Novartis Pharmaceutical Co., Ltd, and is a site principal investigator for clinical trials conducted by Biogen or Novartis Pharmaceutical Co., Ltd Kenji Inoue reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Biogen Japan; Chugai Pharmaceutical Co., Ltd; and Novartis Pharmaceutical Co., Ltd
The remaining authors do not have any conflicts of interests related to this article to declare.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.