
Abstract
Background:
Despite advancements in spinal muscular atrophy (SMA) management, evaluating outcomes in adults remains difficult. Standard motor scales often show floor/ceiling effects and fail to capture patient-relevant constructs. This creates a disconnect between clinical measurements and the lived experience of adults with SMA, particularly in regulatory contexts requiring demonstrable benefit. This qualitative study explored the evaluation priorities, expectations, and preferences of adults with SMA and the corresponding assessment challenges faced by healthcare practitioners (HCPs).
Methods:
Semi-structured interviews with 18 adults with SMA (types 1b-3) and 31 multidisciplinary HCPs from 14 specialized French centers were conducted. Data were analyzed using reflexive thematic analysis and triangulation.
Results:
Adults with SMA found standard assessments burdensome, fatiguing, and lack relevance. Their primary goal was maintaining an acceptable life balance, a dynamic equilibrium between their disease state and an adapted environment. This balance hinged on preserving specific keystone abilities (e.g., joystick control, independent transfers), which are highly individualized and critical for social participation. Patients prioritized the assessment of these specific abilities. HCPs corroborated the limitations of standard tools (insensitivity, confounding factors) and logistical constraints. In response, HCPs have developed numerous “home-made,” non-validated assessments and used personalized tools to capture meaningful changes, especially in severely affected patients.
Discussion:
A discrepancy exists between current standardized SMA assessments and patients priorities. It highlights a need for outcome measures that align with patients’ priorities, particularly “keystone abilities.” HCPs’ innovative approaches offer a promising direction for future assessment development, advocating for a shift towards individualized, holistic evaluation in SMA care.
Keywords
Introduction
Spinal muscular atrophy (SMA) is a progressive neuromuscular disease characterized by the degeneration of spinal cord motor neurons and caused by a mutation or deletion of the SMN1 gene. 1 SMA presents with various phenotypes, depending on the age of onset and the severity of muscle weakness and atrophy. In the past decade, the advances of supportive care and the introduction of disease-modifying therapies, such as nusinersen, onasemnogene abeparvovec, and risdiplam, have significantly improved motor function and survival, especially in patients with infantile-onset SMA.2–4
However, these therapeutic gains also expose gaps in outcome measurement approaches for adolescents and adults. 5 Traditional functional motor scales, such as the Hammersmith Functional Motor Scale Expanded (HFMSE), Revised Upper Limb Module (RULM), and Motor Function Measure-32 (MFM-32 or MFM), though commonly used, demonstrate ceiling and floor effects that limit their sensitivity across the full spectrum of disease severity.6,7 In particular, their ability to detect meaningful clinical changes in adults with advanced disease is limited. Furthermore, constructs such as participation and role functioning are poorly assessed in these motor-centric tools.
Efforts to address these limitations have led to increased interest in patient-reported outcome measures (PROMs), including instruments like the Spinal Muscular Atrophy Independence Scale (SMAIS), the SMA Health Index (SMA-HI), Quality of Life for genetic Neuromuscular disorders (QoL-gNMD), or the Patient Reported Outcomes Measurement Information System (PROMIS).8–11 These tools seek to capture more holistic dimensions of health such as fatigue, respiratory capacity, swallowing, and autonomy, which are critical to patients but underrepresented in standard clinical assessments. 11 However, challenges remain around responsiveness, interpretability, real-world applicability, and alignment with patient-defined goals. 11
The International Classification of Functioning, Disability and Health (ICF) framework provides a conceptual structure for understanding these discrepancies between physiological performance and lived experience. It distinguishes between impairments, activity limitations, and participation restrictions, and allows a structured analysis of inconsistencies between motor-function assessments and more participatory evaluations. Functioning is influenced not only by body structure and function but also by activities, participation, personal and environmental factors. 12 Instruments such as the Goal Attainment Scale (GAS) 13 and Canadian Occupational Performance Measure (COPM) 14 build on this framework by identifying and tracking progress in domains personally meaningful to the patient, often revealing benefits overlooked by quantitative motor tests. Studies have shown, for example, improvements in COPM scores despite no changes in MFM-32 scores, 15 suggesting that standard outcome measures may fail to detect clinically important benefits.
The ICF framework also reveals some limitations. While it conceptually separates the ideas of ‘activity’ and ‘participation’, the classification system itself does not. The ICF qualifiers for participation are essentially measures of competence, or the ability to execute a task. It also lacks specificity to describe the relationships between its different domains. 16 The Family of Participation-Related Constructs (fPRC) framework, refines and expands the concept of participation in two essential and distinct components: attendance (simply the act of “being there”) and involvement (the experience of participation while attending that may include elements of engagement, motivation, persistence, social connection, and affect). 16 The ICF also inadequately addresses the varied lived experiences highlighted by Social Role Theory (SRT). Each role is a set of rights, duties, expectations, norms, and behaviors that a person has to face and fulfill 17 and has been shown to contribute to functioning and health. 18 To our knowledge no research has studied these aspects of participation for adults with SMA.
In France, following regulatory approval of therapies for adults with SMA in 2018, assessment protocols and reimbursement eligibility have increasingly depended on measurable clinical benefit.19,20 This has amplified the demand for robust, individualized evaluation tools. Given the scarcity of data concerning adults with SMA, numerous questions have emerged regarding the appropriate indications for treatment and subsequent follow-up within this demographic. The resulting strain on expert centers and the complexity of therapy-related planning has led to the implementation of multidisciplinary team meetings 21 aimed at harmonizing practices and supporting equitable decision-making.
However, significant gaps remain regarding how adolescents and adults with SMA perceive treatment evaluation, their health priorities, and how well current clinical tools align with these expectations. This is particularly the case for SMA adults with the most severe forms of the disease for whom no outcome measures are able to capture changes. 5 It raises crucial questions about meaningful aspects of health and the ecological validity of outcome assessments. The International Society for Pharmacoeconomics and Outcomes Research (ISPOR) have developed a set of core principles for selecting and developing measurements in research and clinical care that are meaningful for patients, starting with defining meaningful aspects of health – defined as aspects of functioning that a patient: a) does not want to become worse, b) want to improve, or c) wants to prevent. 22
In order to identify measurements that reflect more accurately the lived experience of SMA adults, the aim of this study is to explore:
The expectations, priorities, and preferences of adults with SMA in relation to their experience of existing treatment evaluation (including aspects of content – what are the meaningful aspects of health to assess? – and logistical considerations – what could be an acceptable effort from their perspective?). The challenges faced by Healthcare practitioners (HCPs) in their attempt to tailor assessments to individual patient goals within variable resource conditions.
Given the limited prior research and the need to contextualize clinical practices in real-world settings, a qualitative methodological approach was chosen as most suitable to explore these under-investigated dimensions from both adults with SMA and provider's perspectives. 23
Methods
We employed a triangulation approach, utilizing qualitative data obtained from semi-structured interviews with both adults with SMA and HCPs, to develop a model of SMA adults’ priorities, expectations and preferences toward treatment evaluation.
Study design
A multidisciplinary scientific committee of SMA specialists and a sociologist designed a two-part qualitative study (Figure 1).

Study design process. Legend: The 8 HCPs participating in developing the parameters of the qualitative study were all used to caring for SMA adults. They comprised two neurologists, a pulmonologist, a physiotherapist, an occupational therapist and a nurse, members of the scientific committee and a Physical and Rehabilitation Medicine (PRM) specialist and a psychologist from a reference center for rare neuromuscular diseases.
The study design was a collaborative and iterative process led by the principal sociologist in partnership with a multidisciplinary scientific committee. This committee comprised eighteen HCPs with deep expertise in SMA from eight different specialized centers.
After a definition of the research objectives, the process continued with a series of foundational workshops with a smaller group of eight HCPs including two neurologists, a pulmonologist, a physiotherapist, an occupational therapist, a nurse, a Physical and Rehabilitation Medicine (PRM) specialist, and a psychologist. These serve to ground the sociological inquiry in the clinical and social realities of adults living with SMA. The HCPs drew upon their extensive clinical practice and direct patient interactions to serve as the primary determinants for identifying key research domains and relevant inclusion criteria. These workshops functioned (1) on the one hand to educate the sociologist on the nuances of SMA, its care pathways, and the organization of specialized centers and (2) on the other hand to identify critical gaps in knowledge from both patient and HCPs perspectives.
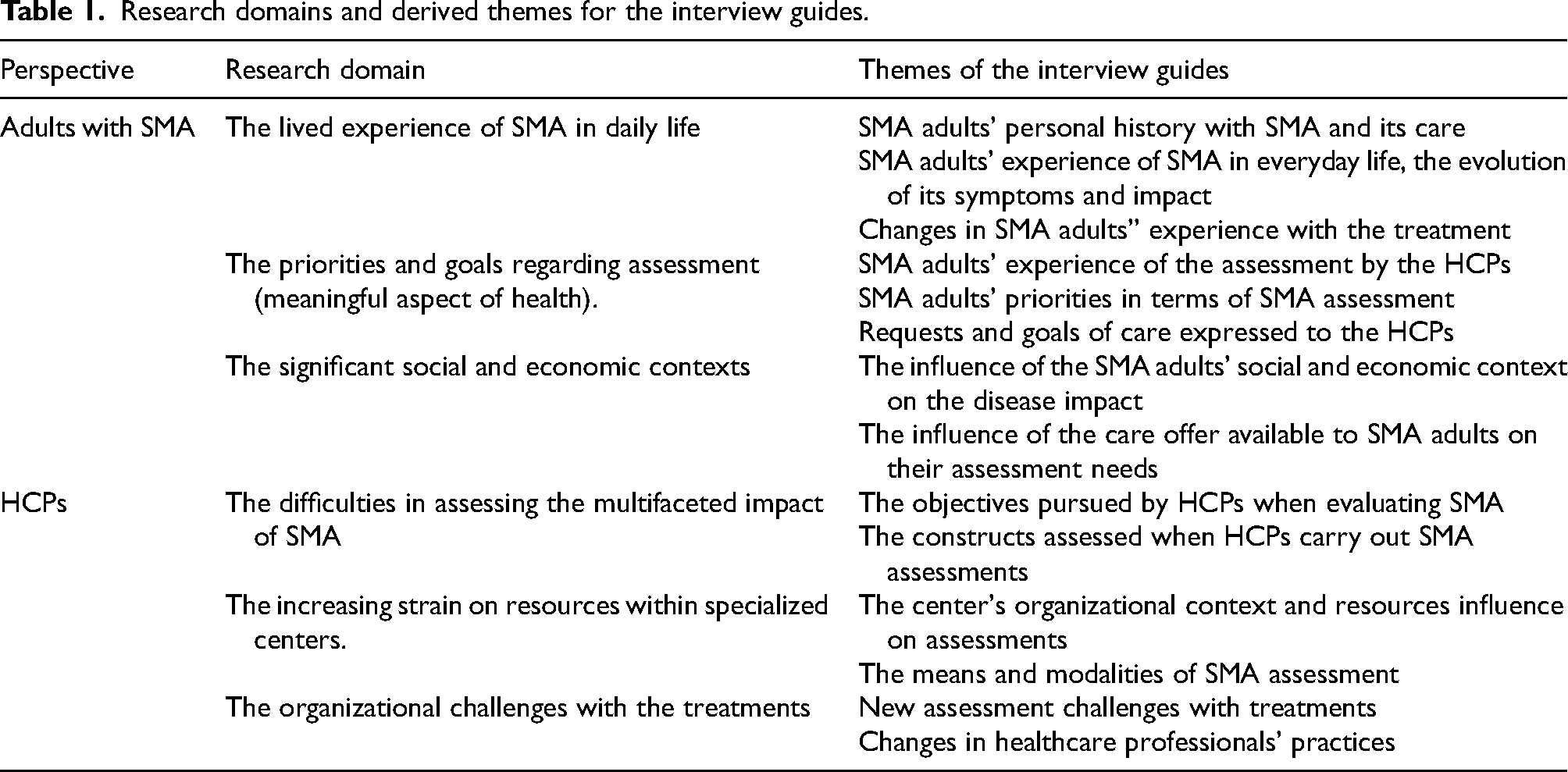
Several research domains emerged and directly informed the development of thematic interview guides for both SMA adults and HCPs (Table 1).
Research domains and derived themes for the interview guides.
The scientific committee ultimately reviewed the research domains and inclusion criteria before defining the inclusion process.
Sampling
To represent the diversity of adults with SMA and types of care, a purposive sampling was directed towards achieving maximum variation in both patients and HCPs characteristics. 24 Twenty-one criteria were identified to describe the diversity of adults with SMA and five were selected as main inclusion criteria. For HCPs, eight inclusion criteria were identified (supplementary material table 5).
Data saturation was determined by the sociologist (GM) when no additional themes emerged during data analysis. It was discussed with the scientific committee during the research as recruitment, data collection and data analysis were performed simultaneously and iteratively.
Recruitment
Adults with SMA were recruited through a call for participation disseminated in specialized centers, specifically targeting those who met the study's inclusion criteria. Volunteers then contacted the sociologist responsible for the interviews directly. In addition, some of the persons with SMA encountered offered to relay this call to other SMA adults in their network.
During an initial qualification interview conducted by telephone, the sociologist collected the person with SMA characteristics required for inclusion in the study. If the person met the defined criteria, they were invited to take part in an in-depth interview.
HCPs were recruited by being formally invited to participate in the study by the scientific committee. The initial plan was to recruit HCPs from eight centers. Due to difficulties in recruiting certain profiles, recruitment was extended to fourteen centers during the study.
No prior connection existed between the interviewer and the participants whether they were persons with SMA or HCPs.
Data collection and processing
The interview guides for both adults with SMA and HCPs were derived from the above domains and themes (appendix 2).
Interviews followed a semi-structured format, allowing the emergence of new themes and conducted by an experienced sociologist (GM). Patients’ interviews took place at their home and lasted between 90 and 150 min. The interviews with HCPs were conducted during their work time using secured videoconference. They lasted between 45 and 100 min. All the interviews were conducted between 2022.07.28 and 2023.02.20, audio-recorded and transcribed.
After the interview, only transcripts were kept, anonymized, and stored on a server certified for health data storage. They were imported into the qualitative software analysis Nvivo (version 14.23) for data analysis.
Data analysis
We employed reflexive thematic analysis, 25 supplemented by inductive coding of emergent themes. The process followed six iterative stages.
After a phase of familiarization with a corpus of the first fourteen SMA adults interviews and eighteen HCPs interviews (stage 1), the sociologist analyzed the transcriptions to identify the emerging themes, develop a coding list and identify connections between codes to organize the data hierarchically into concepts and categories using Nvivo (stage 2). This coding map was reviewed and updated by the scientific committee (stage 3). Then, the sociologist (MG) coded the other four patient interviews and thirteen HCPs interviews from the updated coding map, which was gradually deepened and improved (stage 4). A re-reading of the entire corpus of interviews was performed to verify and specify the coding map (stage 5) before a second review by the scientific committee (stage 6). The final coding map is detailed in appendix 6.
Triangulation was achieved through analysis of both patient and HCP datasets. Analytical memos and audit trails were maintained for transparency. Results and interpretation were progressively and iteratively reviewed by the scientific committee.
Finally, the results and their interpretation were shared and validated by the participants of the study during two online presentations. At the end of these online presentations, SMA adults and HCPs indicated that they recognize themselves in the results.
Researcher reflexivity statement
The research team critically examined their positionality throughout the study, adhering to best practices in qualitative research and the SRQR checklist. The lead qualitative analyst, a sociologist with expertise in narrative methods and clinical research, was responsible for data collection and initial analysis. His independent role, separate from adults with SMA and HCPs environments, enhanced interpretive neutrality. The scientific committee, comprising clinicians from multiple disciplines with practical SMA care insights, provided domain-specific knowledge, influencing the design and thematic interpretation. This collaborative approach ensured a balance between in-depth understanding and analytical rigor. The team regularly discussed their diverse epistemological orientations and potential biases, applying reflexive thematic analysis principles.
Results
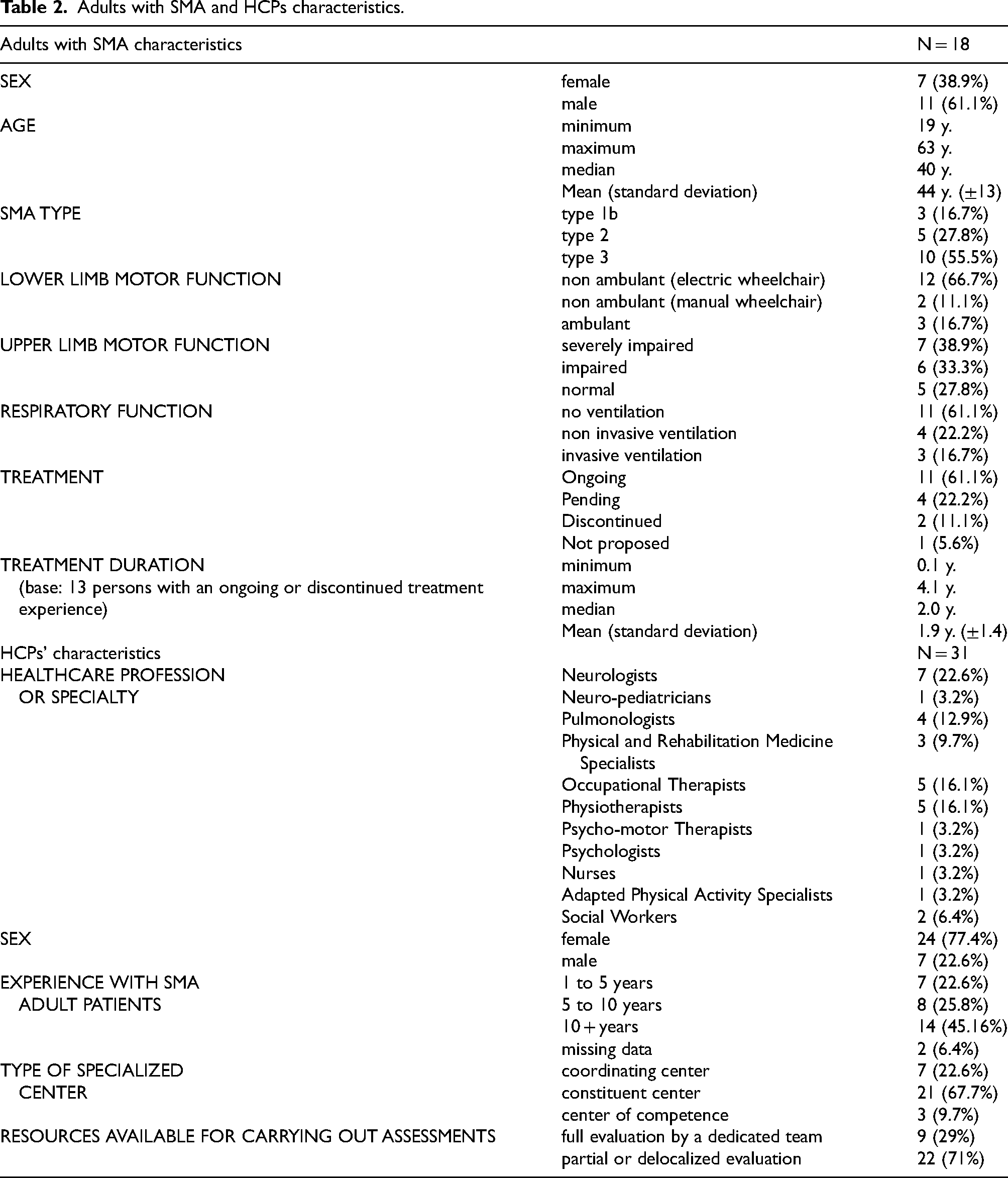
Saturation was reached after interviewing 18 adults with SMA and 31 HCPs recruited from 14 specialized centers. The complete sample is described on Table 2.
Adults with SMA and HCPs characteristics.
Adults with SMA expect evaluations that accurately reflect their situation
See Figure 2

Model of adults with SMA expectations, priorities, and preferences in relation to treatment evaluation.
Adults with SMA find that existing assessments lack relevance
Adults with SMA consistently reported concerns regarding the relevance and precision of current functional motor scales and timed tests. A notable discrepancy was noted between the standardized assessments performed in clinical settings and their real-world functional performance. This issue was particularly pronounced in individuals with type 1b and type 2 SMA, who frequently exhibited floor effects with standardized measures. [This person has severe disabilities resulting from his disease, he is confined to an electric chair and is only able to move one finger] “Look, these evaluations are… how can I put it? They're impossible for me to pass, even at the most basic level.
“He [his physician, a SMA specialist] had told me that “And in fact I find that the assessments are not necessarily always adapted because there are things that I'll be able to do with my right arm since I'm right-handed, but that I won't be able to do with my left arm, and vice versa. There are other things I can do more easily with my left arm, which has more amplitude today, even if I have better dexterity on the right. I have more amplitude in my left arm, so all that isn't taken into account in the system”. (Patient 7, type 2, ongoing treatment) “For instance, I just lost the ability to lift my mug right when it started getting a bit colder… “The problem is, we had our last appointment in early September, and the weather was still warm. The next one is scheduled for, I think, March. If it's ten degrees colder then, my scores will undoubtedly be much worse. Will I be positioned in the exact same way for the test? I don't know. I tried to memorize the table they had me at and all that, but… you see the issue. I told him, ‘This is a bit absurd.’ If you really want a reliable test, you should do it every month. Doing it every six months is pointless.” (Patient 8, type 2, pending treatment) “For me, the interpretation of the results makes me wonder. I mean, it's not done every time under the same conditions. Apart from my state of shape, where there's nothing we can do about it, “For type 2, they [assessments] don't work because there is a floor or ceiling effect. Well, above all, the floor effect. So you have to find other, more sensitive evaluations. Because when you've only got fingers and hands that move, it's hard to find a measure” (PRM specialist 3). “– So, I have this type 3 patient. He was walking, then he lost some weight, did his physical therapy, and [his assessments] got better. – What's the reason for that? – Well, the weight loss, for one.
Adults with SMA experience a burden of assessment
Adults with Spinal Muscular Atrophy reported that assessments are demanding, particularly for individuals with severe forms of the disease. A single assessment could consume an entire day, leading to significant fatigue. Prolonged transportation to specialized centers via ambulance, the lack of resting opportunities throughout the day, and the physical exertion required for functional motor, strength, and timed tests contribute to this fatigue. The burden is exacerbated in centers where multidisciplinary consultations are not organized, often necessitating patients to visit multiple locations for different specialists (e.g., motor function and pulmonary assessment). “It takes me a minimum of two-and-a-half hours to get there [to the hospital] […] So I do the MFM after two-and-a-half hours of road on the first day when I arrive at the hospital. […] “So, you see, this Monday, I'm at the hospital for an all-day evaluation. They'll do a blood test, an ECG, and then I have three hours with a physical therapist who's going to put me through a whole bunch of tests.” (Patient 14, type 3, ongoing treatment)
HCPs involved in assessments acknowledged this burden and adapted their practices accordingly (e.g., maintaining a consistent assessment order, accounting for patient fatigue). “
Adults with SMA priority: maintaining an acceptable life balance
Patients frequently identified the stabilization of their condition as a desirable outcome, which they aimed to achieve through treatment. When their current condition allows for satisfactory social participation, the objective becomes its maintenance. “I know this might be hard to believe, but “What's gone is gone. I don't have any hope for a major recovery. That's just how it is.
“I'm not saying that the treatment is a miracle, “The expectations of adults are not the same [as those of children],
This equilibrium contributes to what can be termed an acceptable life balance, representing the acceptable effort and cost required to attain satisfactory social participation.
First, adults with SMA generally perceived the attainment of a stable disease as largely beyond their control. Treatment is seen as an additional avenue to achieve this objective. Most endeavored to maintain or preserve their motor skills for as long as possible through training, physiotherapy and fatigue management strategies. This resulted in an important logistic and mental load. However, this is also contingent upon the availability of care services in their residential area. “I'm used to living with it. It's a matter of daily management if you want to have a ‘successful’ personal and professional life. It's about organizing around the challenges of the physical disability, but if you adapt, you can manage the situation effectively. “To speak the language of the bureaucracy means communicating our precise needs, especially regarding hours, in accounting terms… Because that's all they understand anyway… “ “– So, is it complicated to get funding for that kind of equipment? –
Adults with SMA expect assessment of their “keystone abilities”
Given that environmental modifications cannot be implemented at the same pace as the disease progresses, maintaining an acceptable life balance hinged on a select set of capabilities, hereinafter termed keystone abilities. These keystone abilities are essential for maintaining function. Much like the keystone in architecture, their loss would lead to the collapse of an acceptable life balance.
Therefore, adults with SMA often identified certain abilities as crucial for maintaining an acceptable life balance especially when they anticipated the consequences of losing them. This is the case of a man who felt more and more difficulty raising his hands, affecting his ability to eat and to reach objects around him. He anticipated that losing this ability would necessitate increased human assistance for his daily tasks and a complete overhaul of his daily organization. “Afterward, when it comes to eating… well, if you like, I put my head down instead of raising my hand, and I eat more and more messily, dirty, meaning I eat with my fingers. […]
HCPs corroborated that not all patients’ abilities are equal, that some are more critical than others and therefore more worthy to be evaluated. “So, this is a very dynamic 27-year-old woman. She works, she goes out at night with her friends, and so on. She drives her car, but then she needs two crutches to walk into her house. She uses a manual wheelchair to get around at work.
Table 3 provides examples of keystone abilities, identified through interviews and categorized by SMA type.
Examples of keystone abilities according to the SMA type.
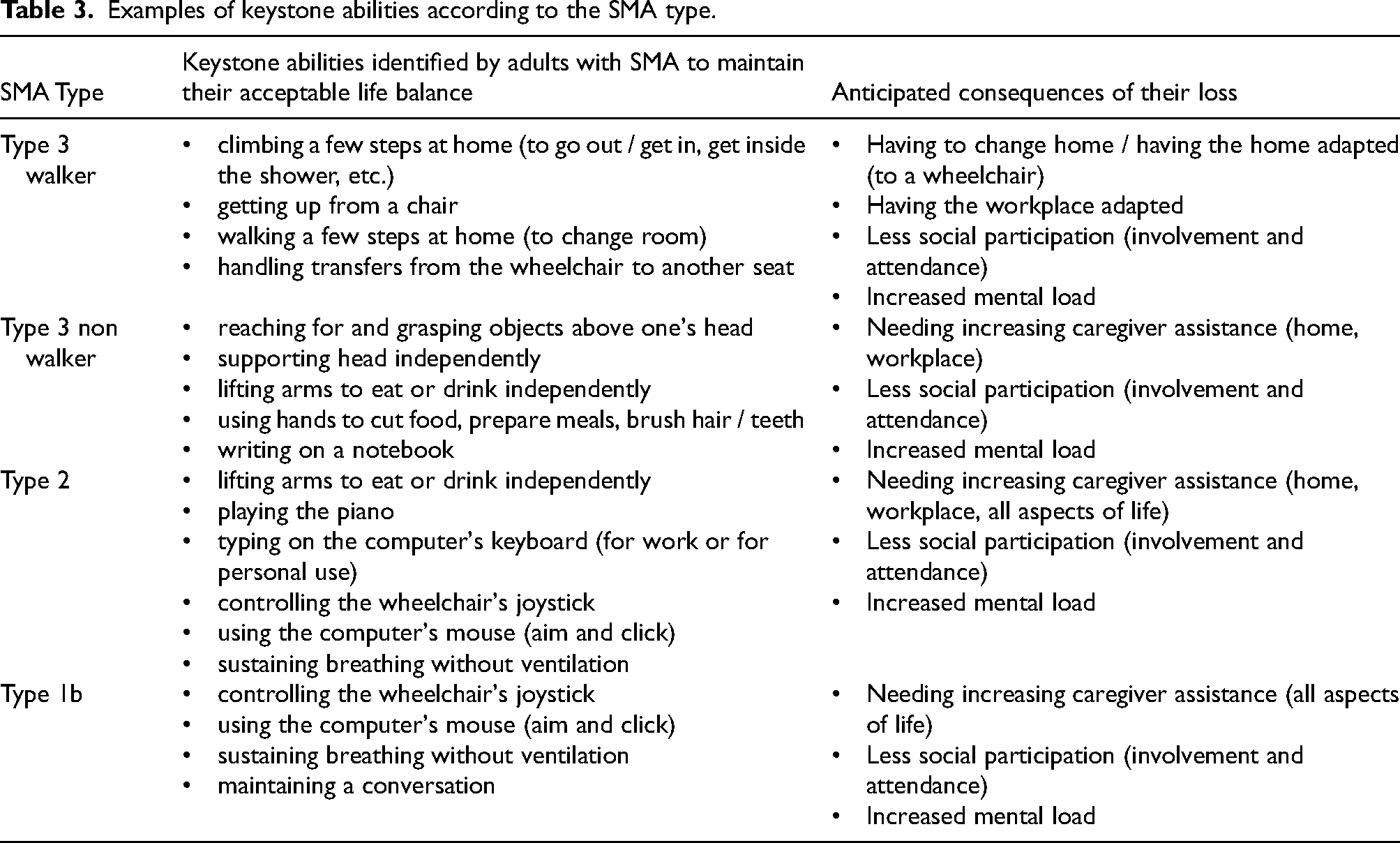
Persons with this severe condition reported expecting these keystone abilities to be assessed accurately. Some persons with SMA emphasized the importance of evaluating the abilities they are losing rather than focusing on measurable outcomes. “I think you should concentrate on the gestures you're losing. If the aim is to evaluate over a year or two and not ten years, but gestures that we're losing, that we're struggling with […] to brush my teeth for instance, that's something that has changed. I need someone to hold my arm now” (Patient 8, type 2, pending treatment)
Thus, the loss of these keystone abilities has severe consequences, compelling patients to implement significant changes to their environment and daily organization. This often entails an increased reliance on human assistance, the adoption of new technical aids, a re-evaluation of home adaptations, and a heavier organizational burden in everyday life. Consequently, a loss of spontaneity in daily activities and social participation is observed. “– So if you were to lose the use of your left arm, what would that mean? – Oh, “You see […] an idea that frightens me: the day I started using home help, I was told: ‘To be quick, there are two ways: either you use an agency, which you pay, and it takes care of payslips, replacing absentees, etc., or you can be a direct employer.’ […]
HCPs are reinventing their evaluation practices of adults with SMA
See Figure 3

Model of HCPs’ practices in evaluating adults with SMA.
HCPs are pressured to provide quantified evaluations of adults with SMA
The advent of innovative therapies and their subsequent reimbursement have introduced new objectives and constraints in the management of adults with SMA. Due to the French Transparency Commission's requirement for treatment decisions to be made in multidisciplinary team meetings, healthcare professionals needed systematic assessments to harmonize the treatment decision-making process. “– Why is it so important to have that data? – – But how can you tell if a patient is deteriorating or just stable?
– That's exactly the point. “
Due to the scarcity of clinical trial data in adult populations, HCPs have noted a deficit of information to guide medical decision-making. They reported that existing data do not adequately differentiate the drug's effect from routine management, inform appropriate assessment strategies, or enable stratification of expected outcomes and assessments based on disability level. “There have been some studies on risdiplam that included patients up to age 22 or 23, but they involved very few patients. As for nusinersen, the studies were conducted in children, not in adults with disabilities. They've relied on a lot of natural history data and open-label, treated-cohort follow-up studies to suggest it's quite effective.
HCPs face several challenges in the assessment of adults with SMA
a) Logistical constraints guide the selection of evaluation methods.
The requirement to assess patients has led to an increased workload for specialized centers where systematic assessments were not previously a routine component of adult SMA care. As this new obligation was not matched with a corresponding increase in resources, centers were constrained to utilize existing staff within the existing hospital framework, where each interaction with a healthcare professional occurs within a consultation setting.
While some centers have successfully established multidisciplinary consultations, others are required to conduct evaluations using available personnel and resources. Consequently, approaches to these challenges vary, depending on the specific center and its available resources, leading to discrepancies in assessment practices across institutions. “ the specific center, characterized by heterogeneous resources allocated to assessments, leading to the selection of indicators and evaluations based on the center's practical capabilities; “… the individual patient, whose objectives and expressed needs differ, necessitating the discussion and selection of indicators with the patient that are predicated on meaningful activities of daily living; “This is a perfect example. “We need to be able to offer things that are truly tailored to the patient and their specific life. the severity of the disability, which presents challenges in assessment due to the limited availability of tailored instruments and may necessitate the development of ad hoc indicators; “The fact is, when a patient is very severely affected… basically, their entire functional life consists of being in an electric wheelchair and moving their hand on a joystick to go forward, back, and turn. “And then,
and (iv) participation in research projects, which mandates the utilization of standardized indicators.
b) HCPs strive to overcome standardized assessment limitations
HCPs expressed concerns regarding the absence of sufficiently sensitive and precise assessment tools to guide treatment decisions. The challenge of selecting appropriate assessments for each adult with SMA arose at every stage of treatment: initiation, maintenance, and discontinuation. Currently, HCPs reported relying solely on standardized assessments, including motor function scales (e.g., MFM, HFMSE, or RULM), strength measurements, and endurance or timed tests (e.g., 6MWT, 10MWT). Several limitations of standardized assessments were identified.
Firstly, these assessments often lack sensitivity and precision, necessitating multiple measurements over several months to reach definitive conclusions. This can result in delayed treatment initiation, potentially leading to missed opportunities for patients. Consequently, HCPs reported frustration regarding the inadequacy of current instruments and a pressing need for sensitive evaluations to identify treatment windows and monitor treatment response. “– If I need three or four data points just to confirm that my condition is declining, that means I could have potentially changed the treatment back here [at an earlier point]. Am I really forced to wait until I've declined this far? I keep telling myself, ‘Maybe it will bounce back at the next point,’
– So it puts you in a position of having to wait and see the outcome of the battle before you can act.
–
Furthermore, HCPs reported difficulty in isolating specific treatment effects, as standardized motor function scales are susceptible to various confounding factors, including patient weight, level of training and physical activity, pain (from immobilization), and weather conditions (temperature). Controlling these factors is challenging, particularly when assessments are conducted only every 4 to 6 months. This necessitates the collection of additional ecological information regarding context, such as weight, training level, patient fatigue, and test-taking conditions, all of which must be documented by clinical evaluators. “Yes,
“
HCPs have developed home-made assessment to tackle the challenge of assessing adults with the most severe forms of SMA
Given the scarcity of validated assessment tools for patients with severe disabilities, HCPs were frequently required to devise novel evaluations.
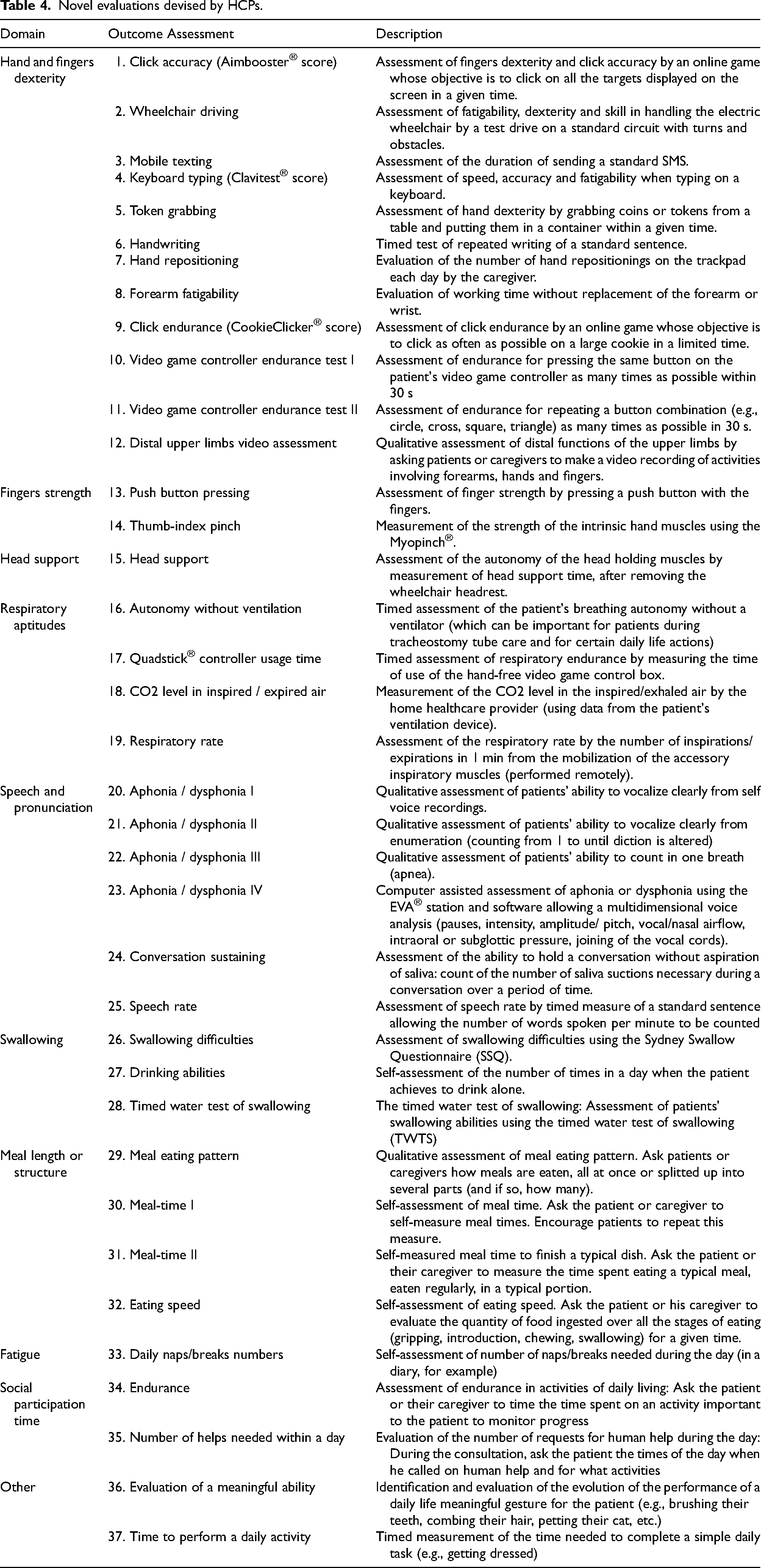
The development of specific indicators for these patients often involved adapting existing neuromuscular scale items (e.g., by modifying starting positions or altering exercises) or creating novel timed tests to measure endurance or fatigability in simple tasks. “To ensure reproducibility, I used materials from the MFM like the CD and the small grid. “But in this case,
Novel evaluations devised by HCPs.
Discussion
Our study identifies the treatment evaluation preferences and priorities of adults with SMA. Standardized 6-month assessments conducted in specialized centers are perceived as burdensome and largely irrelevant by this population. Instead, they expressed a desire to achieve or maintain an acceptable life balance at a specific time and within a particular environment, which hinges on a few keystone abilities essential for social participation and quality of life. Adults with SMA emphasized that these keystone abilities are meaningful to assess and crucial for preservation or improvement.
Conversely, our study reveals that HCPs encounter challenges in providing quantified assessments for adults with SMA for treatment decision-making. These challenges stemmed from limited workforce and a lack of relevant instruments, particularly for patients with the most severe forms of the disease. Due to issues such as lack of sensitivity and prevision, ceiling and floor effects, and confounding factors that interfere with standardized measurements, HCPs could only observe disease progression, stabilization, or functional improvement over extended periods. This highlights a clear discrepancy between the expectations of adults with SMA and current assessment practices.
Our findings substantiate and expand on known limitations of standard motor function assessments6,7,26,27 (such as the HFMSE, RULM, and MFM) by demonstrating that current tools insufficiently capture patient functioning in its entirety, particularly from the patient perspective.
Drawing on the ICF framework and its critics, our results indicate a gap between biological function-based measurements and broader, context-dependent experiences of daily functioning and quality of life. Specifically, contextual factors, both environmental and personal, emerged as crucial moderators of patients’ capacity to perform daily activities, aligning with the ICF's core domains of Activity and Participation. This builds on and complements prior qualitative research on adults with SMA,28,29 reinforcing that activity and participation are inseparable from contextual influence.
Previous literature has attempted to better integrate subjective experience into a more detailed explanatory model of how contextual, environmental, personal, and social factors influence individuals’ performance. The concept of capabilities, defined as possible functioning within the lived environment, bridges the gap between capacities in a standardized environment (such as those used for neuromuscular assessment in clinical centers) and performance as the achieved functioning in the lived environment (encompassing its physical, institutional, technological, social, and symbolic aspects). 30 In line with this, our interviews underscore how environmental changes (e.g., caregiver departure, alterations in social networks) can disproportionately modify patients’ capabilities and performance, even at a constant level of physiological impairment.
Within a fixed setting of environmental factors, personal factors, and social influences, these keystone abilities facilitate social participation, encompassing both attendance and involvement, thus functioning. Therefore, not all capacities or capabilities are equal and some are identified as more strategic for adults with SMA and then, more worthy to be precisely assessed and monitored to appraise the treatment effect.
Also, the concept of acceptable life balance indicates that achieving satisfactory participation incurs a cost for adults with SMA. The worsening of SMA or living in a less and less adapted environment increases this cost. Maintaining acceptable social participation necessitates effort to ensure environmental adaptation and preserve physical abilities, consuming time, financial resources, and energy, ultimately leading to increased mental load and fatigue. However, this cost is not described in the main models of functioning such as ICF or fPRC. Our study underlies that acceptable life balance is in fact a dynamic equilibrium among physical ability, and environmental fit at an acceptable cost and emerges as a new axis for meaningful functioning.
Also, the concepts of acceptable life balance and keystone abilities possess practical implications and could emerge as novel outcome measures.
Although keystone abilities are rarely measured in practice, HCPs frequently resort to supplementing standardized assessments with ad hoc and personalized indicators, which are often developed in collaboration with patients. This trend may elucidate the growing interest in personalized outcome measures using GAS or COPM.31,32 This may also explain the development of novel indicators based on repeated measures in the home environment, leveraging technologies like ActiMyo33,34 to monitor changes in patients’ performance within their everyday settings.
Therefore, evaluating keystone abilities can be envisioned in two avenues of exploration:
Maintain flexibility in assessment tools: GAS offers a promising framework, contingent upon active patient collaboration in identifying specific functional objectives and especially keystone abilities. HCPs should specifically inquire about these during discussions with adults with SMA. Furthermore, existing validated assessments could be adapted to identify items most closely related to keystone abilities. Develop standardized tools for underserved areas: The creation of new standardized instruments seems imperative for domains currently inadequately evaluated by existing tools (e.g., fine motor skills of the hands, speech). These novel instruments must balance individualized assessment with generalizability. Consequently, the development of quantifiable measurement tools in these areas is a critical ongoing initiative. The set of assessments devised by HCPs to evaluate individuals with severe forms of the disease appears to be a fruitful starting point for the development of these instruments.
The concept of acceptable life balance emphasizes the importance of the environment. However, recent research highlights the frequent omission of the physical environment in participation measures, 35 despite its widely acknowledged importance. Assessing acceptable life balance would provide a means to approximate an individual's level of adaptation to their environment. It would also shed light on the response shift observed in quality of life evaluations.36,37
Thus, an acceptable life balance could be considered a survival endpoint. It could be defined prospectively and integrated into research to determine when adults with SMA lose it and the treatment contribution to its maintenance.
This study is subject to several limitations. Firstly, while the sample size was sufficient according to SRQR and thematic analysis guidelines, it was restricted to French adults receiving care within a specific healthcare system. Although data saturation was achieved, future studies should investigate potential selection bias, particularly regarding non-participation and its reasons. A more socioculturally diverse or international sample could offer nuanced insights into expectations or assessment priorities as well as on evaluation practices by HCPs. Secondly, although perspectives from both patients and healthcare professionals were solicited, incorporating additional stakeholder voices such as caregivers, policymakers, and payers may further contextualize the implications of the identified disconnects in assessment paradigms. Thirdly, the cross-sectional nature of this study precludes the capture of how patient expectations may evolve over time or with disease progression. This is a critical yet often overlooked aspect, given the progressive and unpredictable nature of SMA.
In conclusion, this study provides valuable insights that can inform the future development of care practices for adults with SMA. Significant emphasis should be placed on incorporating the patient's living environment into the assessment process to obtain a more holistic understanding of their functional status. Finally, it is essential to develop robust and reliable methodologies for identifying and monitoring the critical keystone abilities described by patients, as these measures would complement standardized assessments and provide a more patient-centered approach to evaluation and care planning.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251413326 - Supplemental material for A qualitative study of the discrepancy between patient expectations and assessment practices in 5q-adult spinal muscular atrophy in France
Supplemental material, sj-docx-1-jnd-10.1177_22143602251413326 for A qualitative study of the discrepancy between patient expectations and assessment practices in 5q-adult spinal muscular atrophy in France by Guillaume Montagu, François-Constant Boyer, Marcela Gargiulo, Samuel Pouplin, Aurélie Barrière, Edouard Berling, Céline Bonnyaud, Pascal Cintas, Jean-Yves Hogrel, Lucie Le Goff, Brice Marchadier, Ghislain N’Dah Sekou, David Orlikowski, Hélène Prigent, Alexandra Pruvot, Juliette Ropars, Emmanuelle Salort-Campana, Tanya Stojkovic, Guillaume Nicolas, Sharam Attarian and Pascal Laforêt in Journal of Neuromuscular Diseases
Supplemental Material
sj-docx-2-jnd-10.1177_22143602251413326 - Supplemental material for A qualitative study of the discrepancy between patient expectations and assessment practices in 5q-adult spinal muscular atrophy in France
Supplemental material, sj-docx-2-jnd-10.1177_22143602251413326 for A qualitative study of the discrepancy between patient expectations and assessment practices in 5q-adult spinal muscular atrophy in France by Guillaume Montagu, François-Constant Boyer, Marcela Gargiulo, Samuel Pouplin, Aurélie Barrière, Edouard Berling, Céline Bonnyaud, Pascal Cintas, Jean-Yves Hogrel, Lucie Le Goff, Brice Marchadier, Ghislain N’Dah Sekou, David Orlikowski, Hélène Prigent, Alexandra Pruvot, Juliette Ropars, Emmanuelle Salort-Campana, Tanya Stojkovic, Guillaume Nicolas, Sharam Attarian and Pascal Laforêt in Journal of Neuromuscular Diseases
Footnotes
Acknowledgment
We thank all patients, caregivers and healthcare professionals who participate in this study. We especially thank the specialized centers who participated to the interviews and recruitment: Garches, Institut de Myologie/Paris, Reims, Nancy, Grenoble, Lille, Lyon, Marseille, Créteil, Nantes, Angers, La Réunion, Clermont-Ferrand and Dijon.
We also would like to thank Thomas Lansaman, MD and Nayla Debs for their contribution to the study design.
Authors contributions
|
Design or conceptualization of the study Major role in the acquisition of data Analysis or interpretation of the data Drafting or revising the manuscript for intellectual content |
GM |
|
Design or conceptualization of the study Analysis or interpretation of the data Drafting or revising the manuscript for intellectual content |
F-CB, MG, SP |
|
Design or conceptualization of the study Drafting or revising the manuscript for intellectual content |
AB, EB, CB, PC, J-YH, LL, BM, GNS, DO, HP, AP, JR, ES, TS |
|
Drafting or revising the manuscript for intellectual content |
GN |
|
Design or conceptualization of the study Drafting or revising the manuscript for intellectual content Supervision of the work |
SA |
|
Design or conceptualization of the study Analysis or interpretation of the data Drafting or revising the manuscript for intellectual content Supervision of the work Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved |
PL |
All authors read and approved the final manuscript
Consent for publication
We obtained from all participants the consent for publication of their anonymized data.
Ethics approval and consent to participate
This study complies with the French MR-004 reference methodology 38 that provides a framework for the processing of personal data for the purpose of studies, evaluations or research not involving the human person as studies that do not meet the definition of research involving the human person. 39 Indeed, in France, studies in the field of social sciences in healthcare are not considered medical research involving the human person. 40 All participants signed a consent form before the interviews. (appendix 3).
Funding
This study was financed by the French affiliate of Roche Pharmaceutical Company. The funder did not participate in the data collection, data analysis or data interpretation.
Roche France SAS,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
In compliance with the General Data Protection Regulation and to preserve the confidentiality of study participants, the raw qualitative data can't be shared.
Competing interests
EB, F-CB, J-YH, CB, SP, TS, AB, PC, MG, LL, GN, DO, HP, JR, ES, SA, PL received fees (advisory boards, presentations) from Roche.
BM and AP are employees of Roche France SAS, which supported this study.
GM is an employee of unknowns SAS, who received grants from Roche France SAS to conduct this analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.