
Abstract
Background:
There is a considerable challenge in managing non-dystrophic myotonias (NDM), due to the lack of gold-standard outcome measures to assess NDM burden on activities of daily living and quality of life from the patient's perspective.
Objective:
In this study, we aim to develop and validate a specific NDM patient-reported outcome (PRO) questionnaire.
Methods:
The Active-NDM questionnaire was developed through a modified 2-round Delphi procedure integrating feedback from stakeholders and a systematic literature review, with input from 11 national clinical experts. The questionnaire was validated in a pilot study of 10 patients with NDM. Both clinical experts and patients assessed questions for pertinence/relevance and clarity. We excluded questions that were not considered pertinent/relevant, and reformulated any judged to be poorly formulated, by >80% of the experts/patients. We also excluded questions with <80% reproducibility during the pilot study.
Results:
Based on feedback from experts and findings of the systematic literature review, we identified 130 questions, of which 100 were unduplicated. During the Delphi process, we removed 66 questions due to lack of pertinence and/or relevance. In the pilot study, patients with NDM evaluated the resulting 34-questions for pertinence, clarity, and reproducibility. Subsequently we removed 9 questions that did not achieve the required level of reproducibility.
Conclusion:
We developed the Active-NDM questionnaire, composed by 25 questions, figuring as a new NDM-specific measure to determine the impact of the disease on patients’ activities of daily living and quality of life. Active-NDM could be a valuable tool in the management of patients with NDM. These findings should be interpreted as preliminary. Larger-scale validation studies are warranted to confirm the tool's psychometric properties and generalizability.
ClinicalTrials.gov identifier: NCT06136416
Keywords
Introduction
Non-dystrophic myotonias (NDM) are a rare group of neuromuscular disorders, with a worldwide prevalence of approximately 1 in 100,000 individuals.1–4 Myotonia, delayed relaxation of muscles following voluntary contraction, is the primary symptom of NDM.1,5,6 Patients complain of muscle stiffness, pain, weakness, and it often has an adverse impact on daily life activities.1,5,6 Patients with NDM often struggle with tasks such as releasing a firm grip, walking, climbing stairs or even standing, and have an increased risk of falls. In some patients, myotonia can affect facial muscles, tongue, and other bulbar muscles, resulting in difficulties with speaking, chewing, and swallowing.1,5,6 Due to the continuous contraction of the muscles, patients frequently display muscle hypertrophy,2,7 which can have a negative impact on body image.
The severity of NDM symptoms can vary widely among individuals. Some patients may experience mild discomfort, whereas others face severe muscle stiffness or even periodic paralysis in certain cases, depending on muscle activity or external temperature. 1 Despite the absence of progressive muscle wasting or reduced life expectancy, as seen in myotonic dystrophies, the symptoms of NDM can lead to substantial functional impairment and a decreased quality of life.1,8
The management of NDM remains predominantly symptomatic, focusing on alleviating the primary symptom of myotonia. Currently, mexiletine – a class 1b anti-arrhythmic – is the only medication officially approved by regulatory agencies in Europe and the UK for treating myotonia in adults with NDM.9,10 Mexiletine is a non-selective voltage-gated sodium channel blocker that reduces the abnormal excitability of muscle fibers, thereby improving muscle relaxation and reducing myotonia.9,11,12 Other treatments such as lamotrigine and acetazolamide are also increasingly used in clinical practice. Notably, lamotrigine has shown comparable efficacy to mexiletine in reducing myotonia severity in randomized controlled trials, offering an alternative for patients who do not tolerate mexiletine or for whom it is contraindicated. 13
One widely used patient-reported outcomes (PRO) instrument in neuromuscular disorders is the Individualized Neuromuscular Quality of Life questionnaire (INQoL), which has also been applied in NDM studies. However, although it covers several relevant domains, INQoL was not specifically developed for NDM and does not fully capture the condition's hallmark features, such as the episodic and situational nature of myotonia. This limitation highlights the need for a more tailored tool focused on NDM-specific symptoms and their daily impact, which led us to develop the Active-NDM questionnaire. In addition, the absence of a gold-standard outcome measure for assessing the impact of myotonia on activities of daily living and quality of life of NMD patients is a major challenge in NDM management. Although in the last years several tools and PRO have been developed, there is no consensus on the best approach to measure treatment impact and disease progression in NDM. Additionally, only a limited number of longitudinal studies have examined the natural history of NDM, 14 which hinders the development of clear clinical endpoints and standardized management protocols. Therefore, there is a need for ongoing research to better define PRO measures and to improve treatment strategies for NDM.9,14,15 This study describes the development and validation of a PRO questionnaire (Active-NDM), tailored to assess the impact of NDM on patients’ daily lives. This tool aims to enhance clinical assessments, inform treatment strategies, and provide consistent measurement of patient-reported data for evaluating disease progression and therapeutic efficacy in NDM.
Materials and methods
To develop and validate a PRO questionnaire assessing the impact of NDM on patients’ daily lives, we used a combined approach. We first conducted a modified Delphi process (supervised by SS and AA), an iterative, multistage method that gathers experts’ consensus on a specific topic16,17 and serves as an effective tool for solving complex healthcare problems. Traditionally, the Delphi procedure includes multiple questionnaire rounds to achieve consensus on selected topics. We introduced as a first step an extensive literature and database search to identify the domains and the questions of interest. Expert group discussions then helped refining key topics and relevant questions for the Delphi procedure. After completing this process, we conducted a pilot study to validate the questionnaire with patients.
The whole approach is summarized in Figure 1.
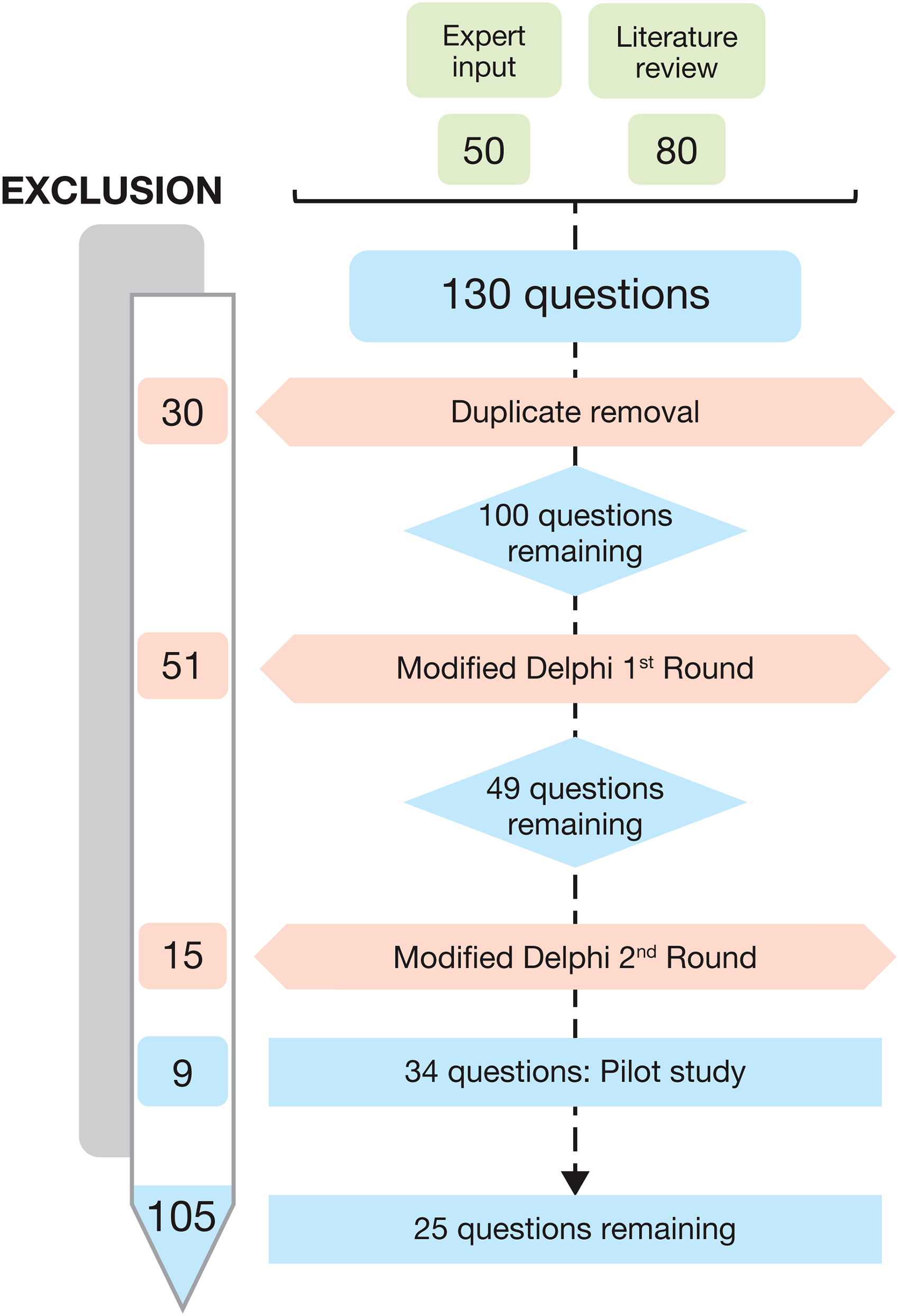
Flow chart of the study data elements. The numbers correspond to the number of questions.
Expert panel selection
The expert panel comprised national leading specialists in NDM, ensuring broad representation across France. We selected as a core team of five experts from the Neuromuscular Disease Reference Center in Nice, including one physiotherapist, one psychologist and three physicians. Additionally, we included six national experts, all neurologists from different Neuromuscular Disease Reference Centers across France. The leading neurologist (SS) and a project manager (AA) served as facilitators for the panel.
Literature and database review
Before starting the Delphi process, we conducted a systematic literature search of studies published between January 2000 and May 2024 in the PubMed, Cochrane Library, and Embase databases to identify relevant publications on NDM or closely related neuromuscular channelopathies. Our research focused on symptoms and functional impairments reported by patients, outcome measures, perception of quality of life, disease burden, and response to therapy. Existing patient-reported outcome measures used in neuromuscular disorders were also taken into consideration for identifying useful items for the questionnaire. The MeSH search terms included 'Non Dystrophic Myotonia', 'Non Dystrophic Myotonia quality of life', 'Non Dystrophic Myotonia activity', 'Non Dystrophic Myotonia therapeutics’, and 'outcome measures’. We screened English-language articles for eligibility based on their title, abstract, and full-text availability. Two authors (AA, SS) evaluated the publications and identified the questions to be included in the questionnaire.
Conceptual framework development
Based on the findings of the literature and database review, we established a preliminary conceptual framework to guide item generation and ensure balanced domain coverage. The framework was structured around two major dimensions reflecting the multidimensional impact of NDM: (1) symptom burden, including myotonia, pain, fatigue, weakness, and muscle hypertrophy or atrophy; and (2) functional and psychosocial impact, covering daily activities, emotional wellbeing, social relationships, independence, and body image.
The initial pool of items identified from the literature was categorized within these predefined domains. This organization was used to structure the Delphi evaluation, during which NDM experts assessed the relevance and clarity of each item within its domain. The framework was subsequently reviewed during patient interviews, where participants confirmed that these domains adequately captured the main aspects of their experience with NDM.
Delphi process rounds
A first draft of the questionnaire was created based on experts’ opinion and literature review. A discussion with the experts was also made regarding the period of time for reporting symptoms. Duplicate questions were removed (SS, AA), and the refined questionnaire was subjected to a Delphi process using a digital evaluation grid (Figure 1). Each item in the initial pool was evaluated by the expert panel based on two criteria: (1) clinical and patient-reported relevance and (2) clarity of wording. To achieve this goal, Expert panelists evaluated each question using two separate 5-point Likert scales were employed: one assessed the clarity of the formulation of the question (ranging from 1: poorly formulated to 5: very well formulated) and the other assessed its pertinence (ranging from 1: not pertinent to 5: very pertinent). Items deemed unclear were reformulated and reassessed. Redundant items, those capturing the same concept as another, were also identified and removed to ensure the uniqueness of each question. This iterative evaluation process led to a reduction in the total number of items. Responses were anonymized for each round.
We selected an 80% agreement threshold to define consensus, in line with established Delphi methodology literature, which commonly considers consensus achieved when ≥75–80% of panelists agree.18,19
Delphi panelists were encouraged to discuss all the questions that did not meet these criteria to find an agreement and provide the rationale for their decisions during each round.
Responses were analyzed to determine consensus by the panel facilitators (SS, AA). A question was retained if >80% of panelists agreed on the clarity of its formulation and/or its pertinence (score ≥4–5 on the clarity Likert scale); otherwise, it was revised and re-evaluated. If the pertinence was problematic for >80% of panelists (score 1–2 on the pertinence Likert scale) the question was removed. Questions that did not achieve consensus were revisited in the second round of the Delphi process, which included anonymized scores and comments from the first round. Remaining contentious questions were discussed in plenary sessions using video conferencing tools.
The Active-NDM questionnaire was refined through this iterative process, to ensure it accurately reflected issues that impact the activity and quality of daily life of patients with NDM from the point of view of a multidisciplinary panel of experts.
Pilot study – patients’ perspectives
Although patients were not involved in the initial Delphi process, a qualitative component was included during the initial phase of pilot study.
The initial item pool was intentionally developed using literature and clinician expertise to ensure comprehensive coverage of clinically recognized NDM manifestations. During the content validation phase, patients were explicitly encouraged to comment on relevance, clarity, and completeness, and to suggest additional items if they felt certain aspects were missing.
Furthermore, patients participated in a subsequent refinement phase through semi-structured interviews, during which they were invited to provide feedback on item clarity, relevance, and completeness, and to suggest modifications or additional items. Based on their feedback, linguistic and structural adjustments were made to improve item clarity and alignment with patients’ lived experience.
Questions that failed to meet on the >80% pertinence/clarity threshold in the pilot study were flagged for review, with the goal of ensuring that the formulation of the final questionnaire would be clear for the patients and would effectively capture NDM patients’ experiences on the impact of the disease on the activity of daily living and on quality of life. Secondary analyses focused on the revised Questions that were poorly rated for clarity by >80% of respondents but deemed pertinent by >80% of respondents were also revised.
Pilot study
Following the Delphi process, and patients’ feedback, the Active NDM questionnaire was tested by NMD patients in a pilot study at Nice University Hospital (CHU Nice). This study was designed as an observational (Recherches Impliquant la Personne Humaine [Research Involving Humans] Type 3 [RIPH3]), single-center investigation. It included male or female patients over 18 years of age with a defined genetic diagnosis of NDM (Figures 1–2). The main exclusion criteria included participation in an interventional study with an investigational drug, pregnancy, or active breast-feeding. Patients were included regardless of treatment status, but all were symptomatic at recruitment. Diagnosis of NDM was confirmed by genetic testing. Treatment status and symptom presence were systematically recorded during patient screening.
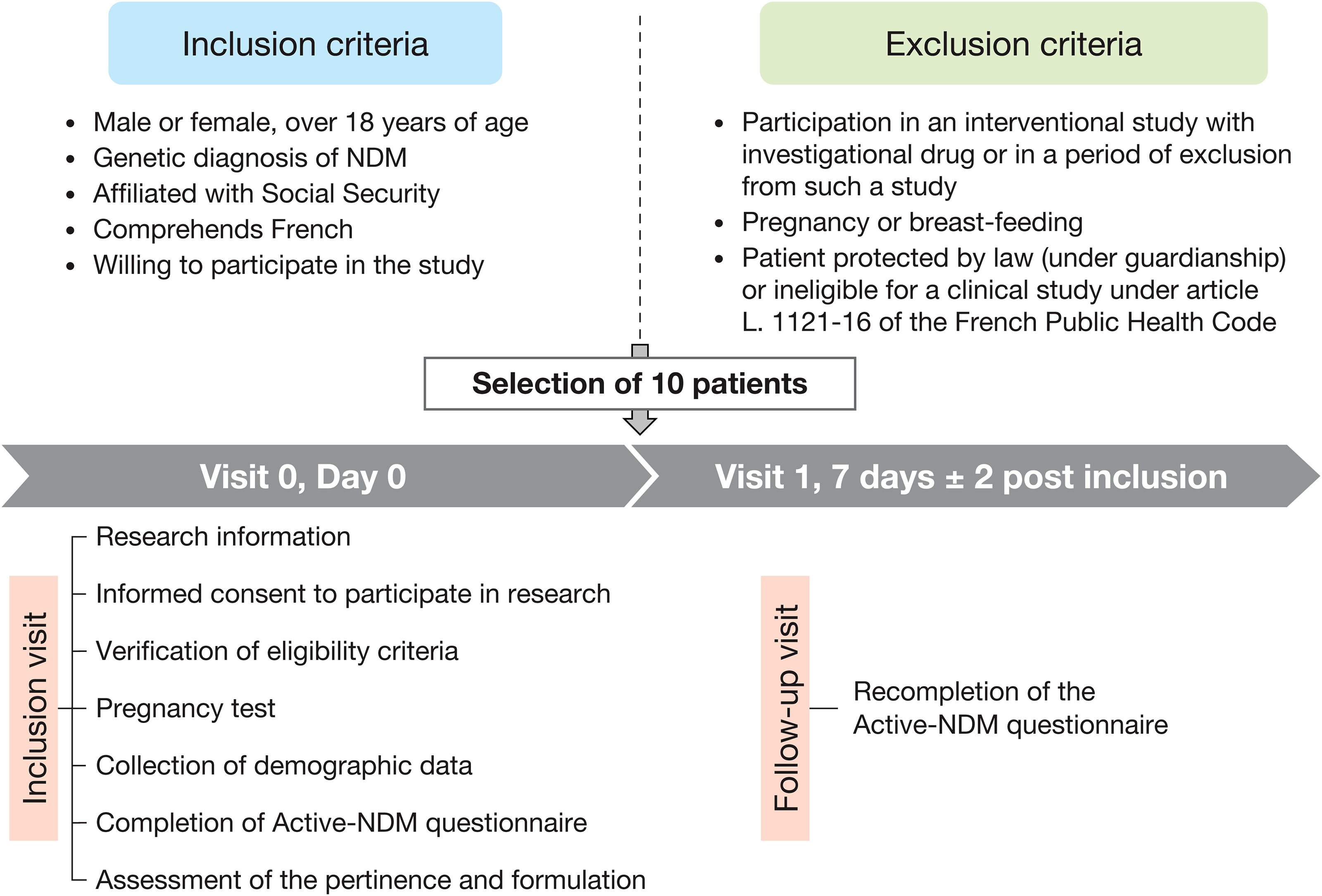
Pilot study methodology, including inclusion and exclusion criteria and timeline.
The main aims of the study were to assess the Active-NDM questionnaire's pertinence, and clarity of formulation from patient perspective, and in addition, to test reliability. Accordingly, the study was conducted over two timepoints: baseline (Day 0) and Day 7. Participants were instructed to report symptoms experienced during the previous 7 days to minimize recall bias and facilitate longitudinal assessment. On Day 0, patients completed both the Active-NDM questionnaire and an evaluation grid to assess the pertinence and clarity of the questions. Additionally, patients provided feedback on the questionnaire during a semi-structured interview. On Day 7, patients completed the questionnaire again to assess its reproducibility over time (Figure 2).
A semi-structured interview was conducted following completion of the questionnaire. The interview guide explored participants’ comprehension of the instructions and items, clarity of the wording, perceived relevance of each item to their lived experience, and any suggestions for improvement. This process aimed to assess the content validity and ensure the tool's accessibility and relevance to individuals with NDM.
The Commission Nationale de l’Informatique et des Libertés (French National Commission for Information Technology and Liberties) approved the processing of personal data for use in the Active-NDM study (approval number 2003095 v 0). The Pilot Study was approved by the Comité de protection des personnes Ile de France VI (Committee for the Protection of Persons, Ile de France VI, approval number 2023-A02257-38). All patients provided written informed consent prior to their participation.
Questions that failed to meet on the >80% pertinence/clarity threshold in the pilot study were flagged for review, with the goal of ensuring that the formulation of the final questionnaire would be clear for the patients and would effectively capture NDM patients’ experiences on the impact of the disease on the activity of daily living and on quality of life.
Secondary analyses focused on the revised questions that were poorly rated for clarity but deemed pertinent by >80% of respondents. Additionally, we analyzed the overall distribution of responses to ensure that the questionnaire comprehensively covered the intended domains.
Data collection and entry
A standardized Case Report Form (CRF) was used to collect baseline characteristics including demographics, treatment status, genetic subtype, symptom profile, and disease duration. Data were collected on paper and then entered into an encrypted Microsoft Excel file. Double data-entry checks were performed to ensure accuracy. The dataset was subsequently imported into R for statistical analysis (v4.4.2; R Core Team 2021, https://www.r-project.org/).
Statistical analysis
Descriptive statistics were generated using R for each question in the Active-NDM questionnaire. Frequencies and percentages were calculated for categorical variables; means and standard deviations were computed for continuous variables. These statistics helped to summarize the distribution of responses and provided insights into central tendencies and variability.
Results
Questions selected after literature review
After removing meta-analyses and reviewing titles and abstracts, 89 studies were selected for further evaluation. These included 1 Delphi study or panel-based analysis, 1 book chapter, 4 commentaries or letters, 10 reviews, 19 case reports, and 54 original research articles. Twenty-seven studies were included in the systematic literature review following screening and full-text reviews. We also explored the literature focusing on NDM symptomatology and its impact on activities of daily living and quality of life.1,8,12,15 We identified 10 recurrent words that appear to be relevant and important for people with NDM: 5 were signs or symptoms of the disease (myotonia, pain, muscle weakness, fatigue, and muscle atrophy/hypertrophy); while 6 were related to areas of daily life that can be impacted by these signs and symptoms and included physical activity, emotional wellbeing, independence, relationships, and body image. These inputs formed the foundation of the Active-NDM questionnaire and helped to support its evaluation.
Based on existing reported outcome measures used in neuromuscular disorders (such as INQoL, SF-36, and the Myotonia Behavior Scale), literature review, and input from the expert panel, we identified 130 questions that were pertinent to the impact of NDM on daily living and quality of life. In particular, 50 questions were based on input from stakeholders at the study center and 80 based on the systematic literature review. Several items were adapted or reworded from existing validated tools, while others were newly formulated to reflect symptoms and impacts that are particularly salient in NDM. After removal of duplicates, 100 questions were retained and entered the first round of the Delphi process.
Delphi process
In the first round of the Delphi process, consensus was reached for reformulation of 33 questions. After reformulation, 51 questions were removed because they were not considered pertinent by the >80% of experts. In total, 49 questions entered the second Delphi round for reaching consensus. During the second round, although no questions required reformulation, 15 questions were removed as they were not considered relevant in the evaluation of NDM by the expert panel. Each question was discussed before final elimination. At the end of the Delphi process, the Active-NDM questionnaire was composed of 34 of the original 100 questions. After the Delphi rounds, a plenary discussion with the experts panel was realized regarding how to categorize, in terms of time, the frequency of the reported symptoms. We decided to report the frequency of the signs and/or symptoms of the patients in “never”, “sometimes”, “regularly”, “often” and “very often”, referred to the last month/lasts weeks. This version of the questionnaire was tested in the pilot study.
Pilot study - patient demographics and clinical characteristics
Ten patients were enrolled between March and May 2024. Patients had a mean age of 43 ± 20 years and they were split evenly between males and females (Supplementary Table 1). Seventy percent (70%) had myotonia congenita (MC) associated with mutations in the CLCN1 gene encoding the muscle chloride channel, of which 71% were autosomal recessive Becker MC and 29% were autosomal dominant Thomsen MC. The remaining 30% had autosomal dominant paramyotonia congenita (PMC) associated with mutations in the SCN4A gene encoding the Nav1.4 voltage-gated sodium channel. Although the mean age of myotonia onset was 12 ± 10 years, the mean age of NDM diagnosis was 33 ± 21 years reflecting a mean diagnostic delay of 21 ± 17 years (range 5–52 years). Seven of the 10 patients were receiving antimyotonic treatment with mexiletine at a dose of either 333 mg/day (n=5) or 167 mg/day (n=2), while the remaining 3 patients were not receiving antimyotonic treatment. Based on the recorded treatment-start dates (2004–2023), the mean duration of mexiletine therapy at baseline was 7.9 ± 6.3 years. All three untreated patients had clinically and genetically confirmed non-dystrophic myotonia.
Patient feedback on question relevance/pertinence and clarity
All the 34 Active-NDM questions were judged as pertinent by 90% of the patients (9/10). Four questions were poorly rated for clarity by >80% of patients and reformulated. After reformulation, all questions were submitted again to the patients, and a consensus regarding pertinence and clarity was reached. Based on this feedback, no questions were removed from the questionnaire. After reaching consensus, semi-structured interviews were also conducted for discussing and evaluating, in a more extensive, open-ended way, patients’ opinions and suggestions regarding the items of the questionnaire. Their feedback provided insights into the everyday impact of NDM symptoms and contributed to modify and refine the questionnaire format.
Reproducibility of the questionnaire questions
The full 34 Active-NDM questionnaire was tested for reproducibility. Nine questions had a reproducibility of <80% (i.e., <8/10 patients responded in the same way at baseline and when the questionnaire was repeated at Week 1). The pilot testing phase involved 10 NDM patients and was not designed for psychometric validation. Rather, it aimed to assess the clarity, acceptability, and relevance of items through qualitative feedback. No formal reliability testing was performed at this stage due to the limited sample size.
A semi-structured interview was conducted with each of the patients to ensure that we were not removing crucial questions. These interviews highlighted patients’ preference for shorter PRO measures that limit the time and effort required to complete the questionnaire during real-life use and the redundancy. This step led to the reduction of the initial 34-item draft to 25 items by removing one irrelevant item (body image), merging redundant items, and simplifying unclear or overly long activity descriptions. This ensured better clarity and reduced respondent burden while maintaining comprehensive coverage of key NDM symptoms and functional limitations.
Final active-NDM questionnaire
Following the pilot study, 25 questions were included in the final Active-NDM questionnaire (Supplementary Table 2). To ensure that the Active-NDM questionnaire provided comprehensive coverage of symptoms and their impact on patient's daily life, we then mapped the data in each of the 25 questions to the 10 fields identified with literature review and experts’ opinions and we obtained a good distribution of the questions among the different fields.
Discussion
NDM can have a severe impact on daily life activities and quality of life. A standardized tool to evaluate this burden could have a major impact on disease management, allowing clinicians to modulate pharmacological and non-pharmacological treatment and would be beneficial to evaluate candidate treatments in clinical trials. Indeed, sponsors, regulators, and patient advocacy groups require direct input from patients about the impact of treatment on symptoms, daily life activities, and quality of life. PROs are critical tools to achieve that because they measure how a patient feels and functions without being influenced by clinician perceptions.
A key issue for NDM clinical trials and longitudinal follow-up in real life is the lack of standardized measures to determine the severity and frequency of myotonia and, in particular, how it impacts patients’ daily lives. The IMPACT study identified that patients with NDM experienced a range of burdens including muscle stiffness, mobility issues, fatigue, muscle pain, anxiety, falls, difficulties with speech, relationship problems, and issues with independent living. 10 Antimyotonic treatment was associated with improvements over a wide range of these NDM associated burdens, with 80–100% of patients reporting improvements in muscle stiffness, mobility, falls, muscle pain, daily activities, and anxiety. 10
The findings from studies such as IMPACT, and the results from our systematic literature review, indicate that measuring the burden of myotonia in people with NDM encompasses a wide range of factors. Hence, the burden of NDM is inadequately captured by measures routinely used in clinical trials such as patient reported stiffness, dynamometry, the timed up and go (TUG) test, the sit-to-stand test, or the 10-meter walk test.9,20
The Individualized Neuromuscular Quality of Life (INQoL) questionnaire is a valuable and widely used patient-reported outcome measure in neuromuscular diseases, including among individuals with non-dystrophic myotonia (NDM). It covers several important domains such as myotonia, daily living, social relationships, emotional wellbeing, and body image. However, despite including relevant items, INQoL was not specifically developed for NDM and remains a general tool for neuromuscular conditions. As such, it may not fully capture the episodic nature, variability, and functional impact of NDM symptoms in daily life. In future validation phases, the Active-NDM questionnaire will be systematically compared with the INQoL to benchmark its psychometric performance. This comparison will determine whether Active-NDM provides complementary and more NDM-specific information regarding the daily functional impact of myotonia, thereby addressing some of the limitations of INQoL in this population.
Other tools more specifically developed for NDM have also been used in clinical settings and trials, including an Interactive Voice Response (IVR) diary for patients with NDM and the Myotonia Behavior Scale (MBS). Both instruments have demonstrated longitudinal validity and have been employed in therapeutic studies.1,21 The IVR diary, for instance, allows patients to record symptom fluctuations (including stiffness, weakness, pain, and fatigue) in real time, thereby minimizing recall bias. 21 Similarly, the MBS was developed to quantify myotonia-related behaviors and symptom severity based on daily functioning. 21 While both tools have strengths—particularly their specificity to NDM—they also have limitations. The IVR requires regular patient input via phone-based or digital entries, which may limit feasibility in long-term monitoring. Moreover, like most patient-reported outcome (PRO) tools, they may not fully capture the broader functional and psychosocial consequences of myotonia in daily life.2,22 In the present pilot study, no additional standardized outcome measures such as MBS, specific IVR tool, or SF-36 were included for comparison. This limitation will be addressed in future validation steps by incorporating these established tools to better assess the questionnaire's validity and performance.
In this context, the Active-NDM questionnaire was developed to complement existing tools by providing a more targeted and disease-specific assessment of symptom burden and its day-to-day consequences in patients with NDM. 23
Since NDM is associated with precise symptoms, we developed the Active-NDM questionnaire as a specific tool able to examine the impact of myotonia, pain, muscle weakness, fatigue, and muscle atrophy/hypertrophy; as well as the influence of NDM on daily activities and quality of life including domains such as relationships, emotional wellbeing, independence, and body image perception. The Active-NDM questionnaire, with 25 questions, was developed using a modified Delphi process and was further refined in a pilot study involving 10 patients with NDM based on this process, the Active-NDM questionnaire included questions that were considered pertinent and well formulated by >80% of experts and patients with NDM, and that elicited reproducible responses in >80% of patients with NDM. As with previous studies, 23 question reproducibility was tested over a 1-week period to limit the potential impact of actual changes in NDM disease severity and to reduce the likelihood of patients recalling and copying their original answers. This modus operandi was used to allow the convergence of several inputs in order to create a PRO with “content validity”, meaning that it was relevant and specific for the group of diseases being studied. To achieve this goal, we conducted an extensive literature review in order to better understand the natural history of NDM, the key symptoms/signs that may improve with treatment, and the impact of clinical benefit in real life. This initial process helped us in selecting the questions of interest that then underwent the Delphi process.
The Delphi process involved a multidisciplinary panel of experts whose main aim was to provide meaningful insight to simplify the questionnaire and refine its formulation. Indeed, completing sometimes lengthy PRO questionnaires can be burdensome for patients, causing fatigue or their attention span to decrease towards the end. As a result, data accuracy and reproducibility may be adversely affected, which represents an unethical use of a patient's time and effort. To avoid this issue, we sought input on the pertinence, formulation, and reproducibility of the questions from 10 NMD patients who were directly involved in the ACTIVE-NDM questionnaire development through the pilot study. Semi-structured interviews were also performed to refine the questionnaire and achieve a final version that reflected both experts’ and patients’ insights. The pilot study was monocentric and conducted in a relatively small population of NDM patients, nevertheless, we ensured that the included patients were representative of the general adult NDM population in term of age and distribution of genetic diagnosis. Most of the patients carried CLCN1 gene mutations associated with MC and patients with SCN4A mutations associated with PMC were also represented. Moreover, as with previous studies, 10 the patients experienced delays in receiving an NDM diagnosis following the onset of myotonia symptoms of on average 21 ± 17 years. In our cohort, 80% of the patients were treated with mexiletine, while 20% were not receiving treatment. The results of this pilot study confirmed the pertinence and formulation of the questions selected by the expert panel but challenged the reproducibility of some of the questions in real-life. For this reason, after a semi-structured interview with each of the patients, we decided to remove these questions from the final version of the Active-NDM questionnaire. This removal also reflected patients’ preference for a shorter questionnaire, to make it easier to complete.
This study presents many limitations. Due to feasibility constraints and the rarity of NDM, patient input was integrated at a later stage through semi-structured interviews during the pilot study, allowing final modifications and better definition of the items thanks to the patients’ perspectives. We are aware that an earlier involvement of patients during the initial phase of generation of items, which is usually recommended in the development of patient-reported outcome measures, might have provided a better insight of the disease and highlighted the need for other additional items, or different shades of signs and symptoms. However, our approach allowed us to assess item interpretation, relevance, and at the final phase the questionnaire was integrated with patients’ suggestions.
Moreover, we acknowledge that environmental and behavioral modifiers known to influence NDM symptoms, particularly ambient temperature and physical activity levels were not systematically recorded in this pilot phase. Patients completed the questionnaire under usual daily conditions, without specific control of these factors. In the upcoming multicenter validation study, we will include dedicated items assessing temperature exposure and physical activity levels and evaluate their impact on symptom reporting. This will help distinguish true changes in symptom burden from fluctuations driven by external variables, thereby improving the precision and interpretability of the Active-NDM scores.
In addition, the pilot version used frequency-based response options without a defined recall period. Patients completed the questionnaire twice one week apart, and no change in symptom severity was reported, supporting preliminary reproducibility. However, future validation phases will implement a specific recall period and assess whether adding severity ratings and contextual factors enhances the instrument's responsiveness.
We acknowledge that a formal evaluation of reliability and other psychometric properties was not feasible within the pilot sample. Although reproducibility was assessed in only ten patients, this step served as an initial screening to identify unstable or ambiguous items. The small sample reflects the pilot nature of the study and the rarity of NDM. A comprehensive validation phase is planned, including larger multicenter cohorts and advanced psychometric analyses such as factor analysis and test-retest reliability to assess the measurement properties of Active-NDM. In future validation work, responsiveness and the minimal clinically important difference (MCID) of the ACTIVE-NDM will be assessed. Determining the MCID will rely on both anchor-based and distribution-based methods, including patient-reported global impression of change, in order to identify what constitutes a meaningful change from the patient's perspective.
Another limitation of this study is the imbalance in treatment status among participants, with seven patients receiving antimyotonic therapy and only three not undergoing any treatment. While this reflects the real-world clinical context and recruitment constraints inherent to rare diseases like NDM, such an imbalance may influence patients’ symptom reporting and perceived impact. As a result, generalizability may be affected. Future validation phases will aim to recruit a more balanced sample with regard to treatment exposure to better capture the diversity of patient experiences.
Another key limitation is the monocentric design of the pilot study and the relatively small number of participants. Although efforts were made to ensure representativeness in terms of age and genetic subtypes, the limited sample size reduces the generalizability of the findings. Future multicenter studies involving larger and more diverse cohorts are planned to address this issue.
In conclusion, Active-NDM is a new NDM-specific measure to determine the impact of NDM on patients’ daily living. Although it requires further development and validation, Active-NDM would provide a useful measure for the longitudinal mapping of the burden NDM as well as evaluating the positive impacts of current antimyotonic treatments and potential future candidate drugs. The next steps in developing this tool will include validation by an international group of NDM experts, analysis of the psychometric properties of the questionnaire using factor analysis, and further testing of the Active-NDM questionnaire in multicenter studies.
Supplemental Material
sj-pdf-1-jnd-10.1177_22143602251412470 - Supplemental material for Active-NDM: Development of a patient-reported outcome questionnaire to measure the impact of non-dystrophic myotonia on activity of daily living
Supplemental material, sj-pdf-1-jnd-10.1177_22143602251412470 for Active-NDM: Development of a patient-reported outcome questionnaire to measure the impact of non-dystrophic myotonia on activity of daily living by Ahmed Amara, Michele Cavalli, Andra Ezaru, Angela Puma, Jérémy Garcia, Sophie Meiran, Aurora Parrotta, Savine Vicart, Yann Péréon, Emmanuelle Salort-Campana, Martin Moussy, Aleksandra Nadaj-Pakleza, Rocio Nur Villar-Quiles and Sabrina Sacconi in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors would like to thank the participants in the pilot study for their valuable feedback on the Active-NDM questionnaire. Medical writing assistance, supported by Lupin Neurosciences, was provided by Dr Mike Lappin.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Lupin Neurosciences.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ahmed Amara (AA): No conflict of interest
Michele Cavalli (MC): No conflict of interest
Andra Ezaru (AE): No conflict of interest
Angela Rita Puma (ARP): No conflict of interest
Jérémy Garcia (JC): No conflict of interest
Sophie Meiran (SM): No conflict of interest
Aurora Parrotta (AP): No conflict of interest
Savine Vicart (SV): Received a consulting fee from Lupin
Yann Peréon (YP): Received a consulting fee from Lupin
Emmanuelle Salort-Campana (ESC): Received a consulting fee from Lupin
Martin Moussy (MM): Received a consultant fee from Lupin
Aleksandra Nadaj-Pakleza (ANP): Received a consulting fee from Lupin
Rocio Nur Villar-Quiles (RNVQ): Received a consulting fee from Lupin for the present study
Sabrina Sacconi (SS): SS received a consulting fee and a grant from Lupin for the present study
Data availability
Data is available upon reasonable request
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.