
Abstract
Background:
Neuromuscular diseases (NMD) cause progressive muscle weakness, significantly impairing functional abilities. Light powered assistive devices hold strong promises for improving mobility and independence in NMD. The current work investigated the efficacy and biomechanical effects of the MyoSuit that provides assistance during functional tasks, by supporting hips and knees.
Methods:
Seventeen adults with NMD studied during a 2-min walk test, a 10-meter walk test, and a 30-s sit-to-stand test with and without using the MyoSuit. Muscle activation, joint kinematics, and spatio-temporal gait parameters were recorded.
Results:
Knee extensor and hip extensor strength were 22.8 ± 42.9% and 71.2 ± 58.2% of predicted force, respectively. 2MWT was 76.3 ± 25.1% of predicted distance. Walking and sit-to-stand performances were reduced. Significantly, cadence, and stride length decreased, while step duration increased. Muscle activation showed decreased rectus femoris and altered timing in gluteus maximus and gastrocnemius medialis. The range of motion of hip abduction-adduction increased, and hip flexion-extension decreased during gait. Major contributors to reduced gait performance as identified using a LASSO were longer double support and step duration, and lower stride length, foot strike angle and variability in lateral step and hip adduction.
Conclusion:
The MyoSuit was not associated with improvements in functional performance in NMD. The use of the device was associated with kinematic alterations and the assistance provided alleviated recruitment of the rectus femoris. The proposed approach is promising but further tailoring of the device is required to address specific needs of individuals with severe muscle weakness.
Keywords
Introduction
Neuromuscular diseases (NMD) are characterized by a progressive decline in muscle strength, with the severity and distribution of this weakness greatly impacting the extent of functional impairments. Muscle weakness leads to significant reductions in functional abilities 1 and negatively affects quality of life by diminishing autonomy, limiting social participation, and contributing to depression. Additionally, physical inactivity leads to higher risk of falls, chronic pain, decreased bone mass, weight gain, and cardiovascular and pulmonary events. Nevertheless, a residual level of muscle strength can often be retained over time, allowing for ambulation and primary transfers even in the later stages. 2 These activities require considerable compensatory strategies, imposing high loads on joints and muscles, which increase the risk of falls and fatigability. 3 Currently, there is no cure for most NMD. Rehabilitation efforts can mitigate some symptoms, but most patients continue to experience functional impairments. 4 Assistive devices, such as traditional aids like crutches and knee orthoses, have been used to facilitate functional movements including walking, sit-to-stand transitions, and stair climbing. However, these devices have limitations as they are essentially passive. Recent advancements in exoskeleton technology offer enhanced compensatory support for daily activities, potentially extending ambulation and improving quality of life despite disease progression. 5 The MyoSuit (Myoswiss AR, Zurich, Switzerland) provides assistance during gait and transfer movements and is a part of a class of lightweight, powered and wearable exoskeleton simultaneously assisting knees and hips. 6 Given its non-self-supported design, the weight of the device is supported by the patient. A research group investigated its potential for people with various gait disorders 7 , its effect during stair ascent in healthy participants 8 , and its feasibility in patients with heart failure, lung transplantation, spinal cord injuries, or stroke during gait.7,9,10 Haufe et al. (2020) showed that the MyoSuit was safe in patients with gait impairments and may improve gait speed after four sessions of training in some participants 7 . Importantly, the added weight of exoskeletons in patients with severe muscle weakness poses a paradox, potentially compromising their efficacy. Additionally, patients’ compensatory mechanisms create uncertainties about the devices’ effectiveness. To the best of our knowledge, no study has explored the use of MyoSuit in patients with primary NMD. Therefore, this study aimed to assess the effects of MyoSuit on performance, perceptions, and underlying mechanisms related to alterations in spatio-temporal gait parameters, joint kinematics, and muscle activation during gait and functional transfer tasks in adults with NMD. Specifically, we seek to determine whether this assistive device significantly impacts performance during a 2-min walk test (2MWT), 10-meter walk test (10mWT), 30-s sit-to-stand test (STS30), and static postural stability (SWAY). We hypothesize that active assistance on hips and knees joints would benefit static and dynamic stability during functional tasks. We hypothesized that the use of the device will not necessarily be associated with improved performance while participant's perception, kinematics, and muscle activation will be positively affected. We also hypothesized that participants with less severe impairments will experience greater beneficial effects.
Materiels and methods
Participants
Individuals aged between 18 and 70 years diagnosed with muscular dystrophies, inflammatory myopathies, or congenital myopathies were included. Participants were required to be able to walk independently for two minutes in a corridor and perform at least three sit-to-stand transitions in thirty seconds. Technical aids such as canes, crutches, light knee and ankle orthoses were permitted. Exclusion criteria comprised individuals using rigid knee braces, those with unstable cardiomyopathy, orthostatic hypotension, balance disorders with non-neuromuscular causes, or recent trauma (within the last six months), severe osteoporosis, severe vascular disorders of the lower limbs. All participants provided informed written consent. The study conformed to the Declaration of the Helsinki and was approved by the ethics committee (ID RCB: 2019-A00155-52; NCT05199246).
Experimental protocol
Patients attended three sessions: each spaced 2 days to 2 weeks apart. The first visit, lasting 90 min, was dedicated to familiarization with the MyoSuit, including device setup, adjustment of settings, and user training. During installation, padding was fitted to the patients. Setting and familiarization involved adjusting the level assistive torque from the lowest 1 to the largest 5 and cable range of motion to best suit the patients’ needs during walking and transfers functional tasks according to manufacturer's guidelines. The second and third visits started with strength assessment performed using a Biodex System 4-Pro dynamometer (Biodex, Inc., Shirley, New York) as previously described. 11 Participants performed three repetitions of isometric maximum voluntary contractions (MVC) for hip, knee, and ankle flexion and extension. Maximal EMG during MVCs was used for EMG normalization during functional tasks (see below). Participants then underwent the following tests: 30-s sit-to-stand test (STS30), three repetitions of a static postural stability test (SWAY), two trials of a 10-meter walk test (10mWT), and a 2-min walk test (2MWT). These tests were conducted without the device during the second visit and with the device during the third visit. Recorded variables included the number of repetitions (STS30), time duration (10mWT), distance covered (2MWT), perceptions, and spatiotemporal outcomes using inertial measurement units (IMUs, see below). Additionally, muscle activation (measured with surface EMG) and kinematics measured with IMUs and were recorded during the STS30 and 2MWT. At the end of the second visit, patients underwent a second familiarization session with the device lasting at least 45 min, adjusted according to their exertion levels.
Exoskeleton device
The MyoSuit exoskeleton is a powered lightweight bi-articular lower limb and non-self-supported exoskeleton assisting the knees and hips. It is a textile based user-initiated robotic device designed to assist mobility impairments in daily life. 6 The MyoSuit comprises a backpack with the motor unit, bilateral knee orthoses and three bilateral layers. The garment layer serves as the interface between the user and the device. The ligament layer passively assists in hip flexion. The active layer, functioning as an actuator routed along the limb, actively assists the movement of the hip and knee joints. The actuator detects an increase in cable length during the active phase and responds by retracting it, thereby providing the necessary active assistance. Two different modes were used during visits. The anti-gravity mode which assists participants in “concentric” contraction mode adapting the assistance while the user is moving. The isometric mode that provides continuous assistance was used during SWAY. With the battery pack worn on the back, the MyoSuit total weight was 5.5 kg. During the familiarization sessions of the first two visits, the device's assistance was adjusted progressively to deliver the maximum level of assistance (from 0 to 5), ensuring the settings remained acceptable for the participant. Constant feedback on the perceived assistance in knee and hip extension range of motion cable assistance was used to individually optimize the settings aiming to deliver the maximal acceptable assistance level, following manufacturer guidelines for proper setup.
Recordings during walking and sitting transfer tests
The STS30 was performed on a chair with armrests, that participants were allowed to use. They were instructed to repeat sit-to-stand and stand-to-sit transitions as many times as possible in 30 s. 12 The postural SWAY test was performed for 30 s on a firm surface with eyes open and fixing a mark on the wall. Participants were asked to remain as still as possible during the trial. 13 Participants started the 10mWT standing with feet parallel behind the starting line and were instructed to walk as fast as possible, decelerating after the finish line. The 2MWT took place on a twenty-five-meter corridor, where participants were asked to cover the longest distance possible, self-managing their effort. 14 Patients had at least three minutes resting periods between each test and trial. Verbal analog scale (VAS) was used to measure participants’ perceptions of stability, exertion, dyspnea and pain. 15 Participants provided a whole number between 0 and 10, where “0” represented the minimum conceivable and “10” represented the maximum conceivable. Perceptions using VAS were collected after each trial. At the end of the third visit, participants answered two validated questionnaires: the modified Nordic Musculoskeletal Questionnaire (NMQ) and the System Usability Scale (SUS;.16,17 The NMQ was then reported on a scale from 0 as “no discomfort” to 10 as “extreme discomfort”. The SUS is divided in 5 categories from 0 as “worst usability” to 10 as “best imaginable usability”. Surface EMG activity was collected bilaterally with wireless electrodes (Trigno quattro-sensor or Trigno mini-sensor, Delsys Inc., Boston, USA) over gluteus maximus (Gmax), biceps femoris (BF), vastus lateralis (VL), rectus femoris (RF) and gastrocnemius medialis (GM), placed and aligned according to SENIAM recommendations. 18 Electrodes were secured with tapes to limit movement artefacts and prevent detachment. The EMG signals were amplified, digitized at 2000 Hz, and recorded in LabChart PRO V8.1.25 software (AD Instruments, Bella Vista, Australia) and band-pass filtered (20 to 500 Hz). Kinematic was collected using eleven IMUs Opal V2C® System placed over sternum, lumbar, thighs, calves, and feet according to manufacturer's instruction (APDM, Portland, USA). IMUs signals were recorded in Moveo Explorer software (APDM, Portland, USA), amplified, and digitized at 128 Hz. The software computed spatio-temporal gait parameters and joint angles of hips, knees, and ankles (in all degrees of freedom). Each test and trial were pre-programmed and included a three second still period before the start of the test for calibration IMUs.
Data analysis
Data analysis was performed using the R environment. Largest MVC for each joint movement and side were used for analysis. The percentage of predicted muscle strength (MVCpred) was computed using previously published equations.11,19 Kinematic and muscle activation patterns characteristics data were processed for the 2MWT and STS30. Percentage of predicted distance for the 2MWT (2MWTpred) was computed using previously published equations. 14 Maximal EMG values (EMGmax) during MVC trials were retrieved. The rectified and filtered EMG envelopes during walking and sit-to-stand tests were normalized to EMGmax. The following features were computed from the normalized EMG signal during phases of each gait cycle (i.e., stance and swing) and during each repetition of STS30 (i.e., sit-to-stand and stand-to-sit) in each recorded muscle: average peak value (EMGpeak), average area under the curve as an index of muscle work (EMGAUC). Average and standard deviation of gait cycle percentage of EMGpeak occurrence (EMGavg and EMGSD, respectively) were processed for 2MWT. The shift in the mean and median power frequency between the last tenth and the first tenth cycles of 2MWT, were derived from the band-passed EMG signal to estimate induced muscle fatigue (EMGMPF and EMGMDF, respectively). Regarding kinematic and kinetic, joints’ range of motion and spatio-temporal gait parameters were recorded and processed in the Moveo Explorer software. Joint angle values during 2MWT and STS30 were low-pass filtered using a second-order butter-worth filter (3.5 Hz). 20 To detect cycles and phases during STS30 based on hip flexion signals, extreme negative values were adjusted. The derivative was smoothed to identify critical points, thresholds based on signal quantiles distinguished significant peaks, and cycles were identified by locating local minima and maxima, defining sit-to-stand and stand-to-sit transitions. Joint angles for each joint during each gait cycle, comprising both stance and swing phases for the 2MWT and sit-to-stand and stand-to-sit phases for the STS30, were averaged. The following features were computed: average joint range of motion (JARoM), average time corresponding to the peak joint angle, and the standard deviation of this time (JAavg and JASD, respectively).
Statistics
Statistical analyses were performed in the R environment. Normality of the data was tested using the Shapiro-Wilk test and visual inspection. Non-parametric tests were used for non-normally distributed variables. Effect sizes were computed using Cohen's d. The Wilcoxon rank-sum test was specifically used to compare the condition without and with the use of the MyoSuit, VAS, spatio-temporal parameters corresponding to each test, and for STS30 and 2MWT, EMG outcomes, as it is suitable for non-parametric comparisons between two dependent groups. Due to significant compensation during STS30, JA and EMG statistics were analyzed separately for the right and left sides. For 2MWT, statistics on both sides were average. Signals shapes of EMG and JA across time were tested between conditions using a statistical parametric mapping method with a two-way repeated-measures analysis of variance (ANOVA). 21 To address the issue of multiple comparisons, a Bonferroni correction was applied. Statistical parametric mapping analysis compared signal values (EMG or JA) using post-Hoc calculation at each percentage of the gait cycle or STS30 cycles without versus with the use of the MyoSuit. Potential relationships between variables were assessed using Pearson's correlation coefficients. Potential relationships between the predicted 2MWT distance and other variables were assessed using Pearson's correlation coefficients. This analysis was intended to identify potential determinants of performance changes, in order to better understand why some participants may benefit from the MyoSuit while others would not. A penalized Least Absolute Shrinkage and Selection Operator (LASSO) regression model was employed to identify the determinants of the 2MWTpred in both conditions altogether and delta STS30rep based on unassisted features. Specifically, for each test, dataset corresponding respectively to 2MWT or STS30 were divided into two subsets: 80% for model training and 20% for validation. Both the training and test datasets included participants from both assisted and unassisted conditions in 2MWT model and only unassisted conditions in STS30 model. This split was performed randomly at each iteration, ensuring that data from each participant was used only in one of the subsets at a time. The process was repeated 1000 times to ensure robustness. During each iteration, the variables selected in the predictive equation were recorded, and the model's performance was evaluated using root mean squared error (RMSE), mean squared error (MSE), mean absolute error (MAE), and the coefficient of determination (R²) calculated on prediction errors on test dataset. The LASSO model was chosen specifically because it penalizes coefficients, effectively reducing the impact of correlated variables by shrinking some of them to zero, even if they may be good candidates. This regularization approach allows the model to select the most relevant predictors while mitigating the risk of overfitting caused by multicollinearity. This iterative process allowed for the identification of contributing variables, even in the presence of potential collinearity, providing a partially explanatory model. We opted for 1000 iterations instead of evaluating all possible combinations to balance computational efficiency with robust variable selection, as exploring every combination would have been computationally prohibitive. To identify the top 500 models, we used the following criterion: models with the lowest prediction errors, based on the MSE calculated at each iteration on the test data, were selected. Specifically, models whose MSE ranked within the lowest 50% were retained for further analysis. This 50% threshold was determined after visual inspection of the distribution of prediction errors, which revealed a significant performance drop beyond this point. The variables selected in more than 50% for 2MWT and 70% for STS30 (for robustness) of these top 500 models were retained for a second modeling cycle. Both thresholds for variable selection were determined empirically, as the distribution of selection frequencies showed a marked decline around this value in the most performant models. Once the variables were identified, we assessed overfitting and estimated the variance in performance metrics by repeating this process with the selected variables. In each iteration, the prediction errors (RMSE, MSE, MAE, and R²) were calculated on the test dataset in order to quantify performance variance and evaluate the robustness of the predictions. The means and standard deviations of the performance indicators were computed based on the distributions of the recorded metrics from each iteration. The estimation of the regularization parameter λ was performed only once at the beginning of each of the two 1000-iteration cycles, using the entire dataset and a 10-fold cross-validation process. This optimal λ was then applied in each iteration of the LASSO model. At the end of all iterations, a final model was estimated using the entire dataset, with λ re-estimated similarly, but limited to the selected variables, to obtain the final coefficients and assess the overall performance of the model.
Results
Population
A total of 17 patients with NMD were included: 3 women, 14 men, age: 59.0 ± 12.0 years, body mass: 77.4 ± 25.0 kg, height: 1.8 ± 0.1 cm, BMI: 25.2 ± 7.3; 10 with muscular dystrophies (facio scapulo humeral dystrophy, Becker muscular dystrophy, myotonic dystrophy, myofibrillar myopathy, limb girdle muscular dystrophy), 5 with inflammatory idiopathic myopathies (idiopathic body myositis), and 2 with congenital myopathies (central core disease). Six participants used technical aid during walking (crutches, canes or ankle-foot orthosis). One fall occurred in one patient while wearing the device during the third visit, without injury. One participant did not perform the third visit (sickness unrelated to the experiment). Predicted muscle strength values for the lower limbs are displayed in Figure 1. MVCpred was 22.8 ± 42.9% for knee extension strength, 33.2 ± 47.0% for knee flexion strength, 71.2 ± 58.3% for hip extension strength and 38.9 ± 53.1% for hip flexion strength.
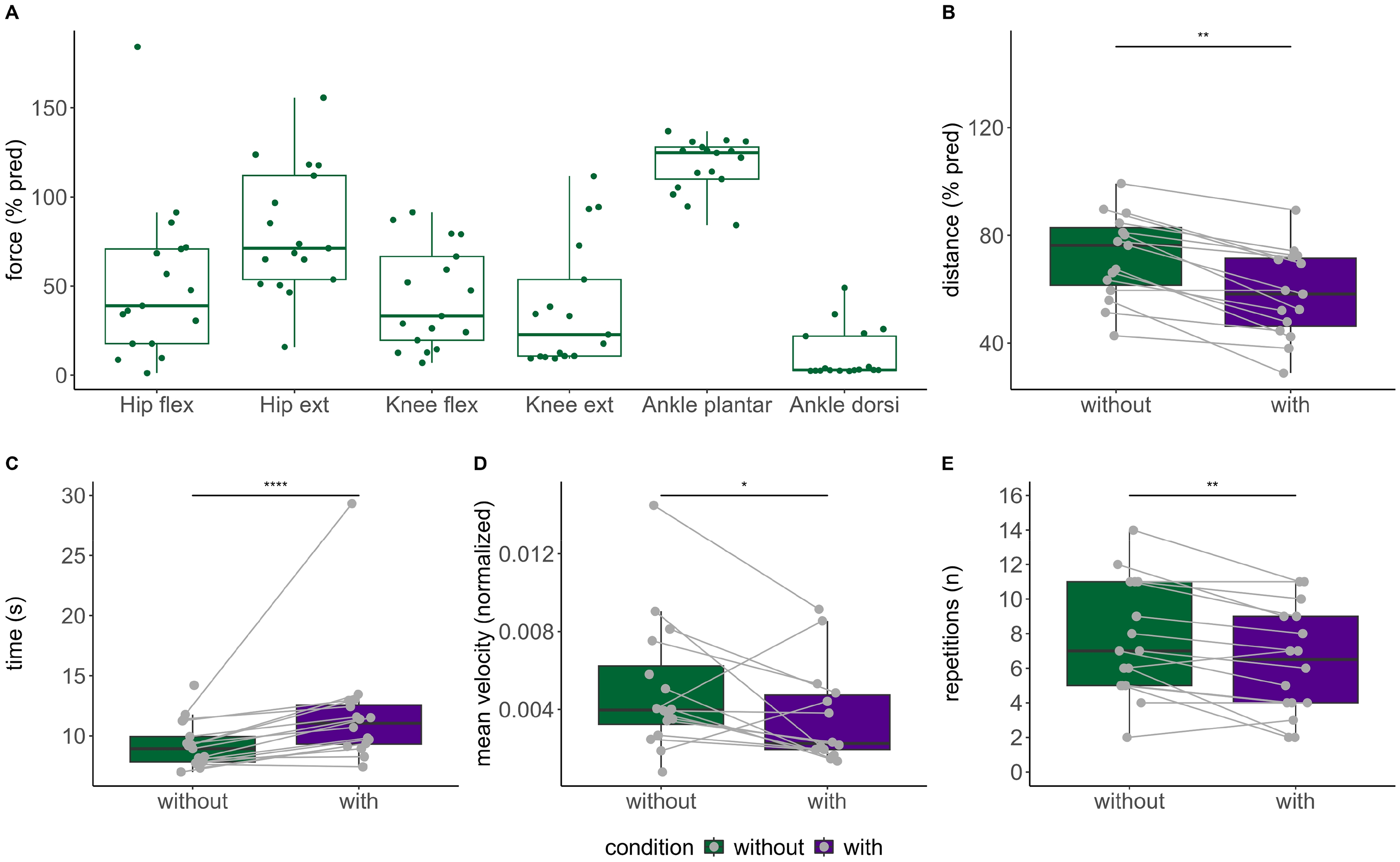
Maximal predicted muscle strength (A). Comparisons of 2-min walk test predicted distance (B), 10-meter walk test time duration (C), postural sway mean velocity (D) and 30-s sit-to-stand number of repetitions (E) without and with the use of the MyoSuit. All variables are displayed as boxes and whiskers plots, median (thick middle line), interquartile range (end of box), and range between maximal and minimal value (vertical lines) are presented. Each participant is represented by a point in both the with and without exoskeleton conditions, connected by a line. ****, p < 0.0001. Hip flex, hip flexion; Hip ext, hip extension; Knee flex, knee flexion; Knee ext, knee extension; Plantar flex, plantar flexion; Dorsi flex, dorsi-flexion; %pred, predicted value in percent.
Comparisons of performance without and with wearing the MyoSuit
2MWT distance was significantly lowered with large effect when using the MyoSuit (105.2 ± 42.3 m vs. 135.0 ± 46.0 m; 58.2 ± 25.3% vs. 76.3 ± 25.1, both p < 0.01 with large effect). The time duration during 10mWT when using the MyoSuit was significantly longer with large effect (11.1 ± 3.3 vs. 8.9 ± 2.1 s, p < 0.0001). Performances and performance changes (with vs. without) in 2MWT, STS30, 10mWT are displayed in Figure 1 and Table 1, and postural SWAY in Table 2 and Figure 2.
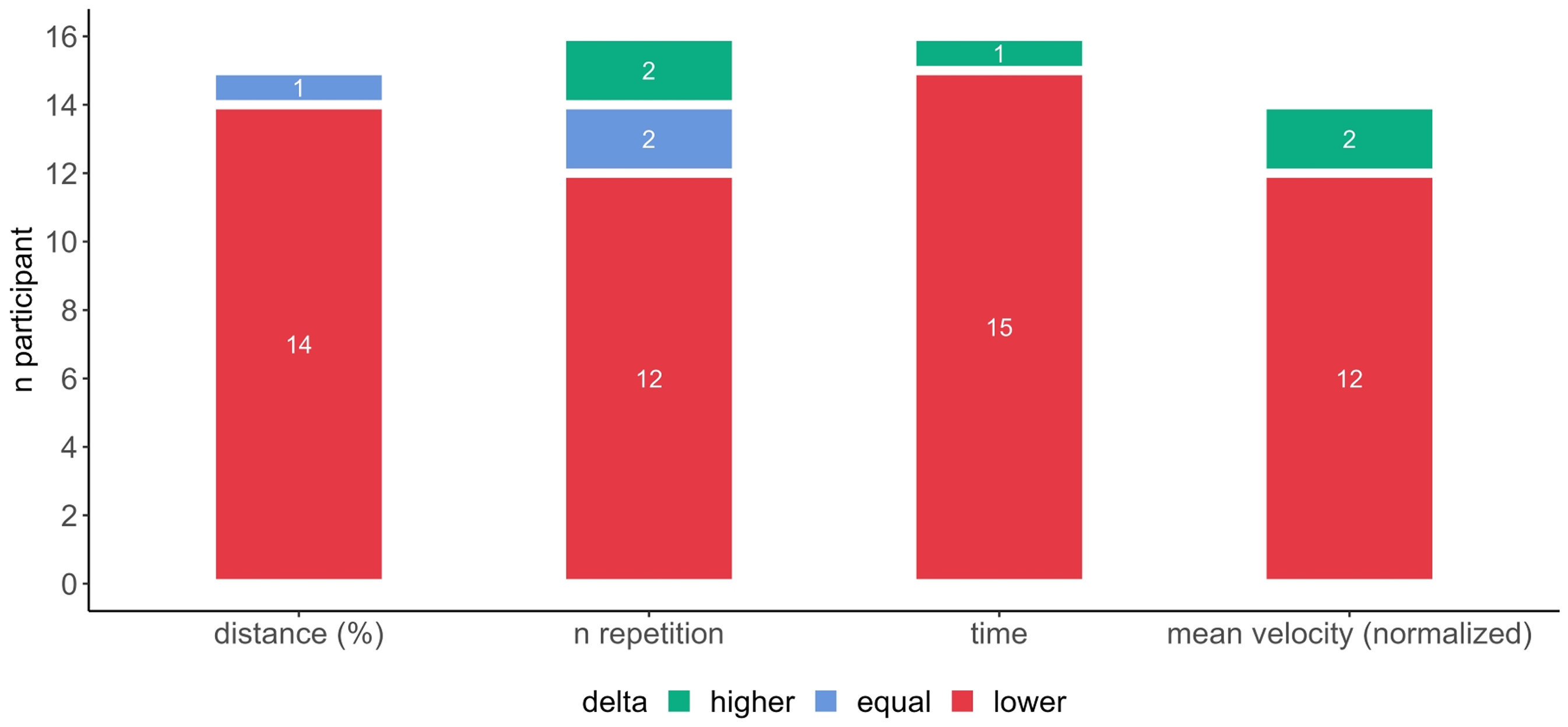
Difference in performance between assisted and non-assisted during 2-min walk test, 30-s sit-to-stand, 10-meter walk test, and static postural stability test when using the MyoSuit in patients with neuromuscular diseases.
Spatio-temporal parameters during the 2-min walk test and the 10-meters walk test in both conditions without and with the use of the MyoSuit.
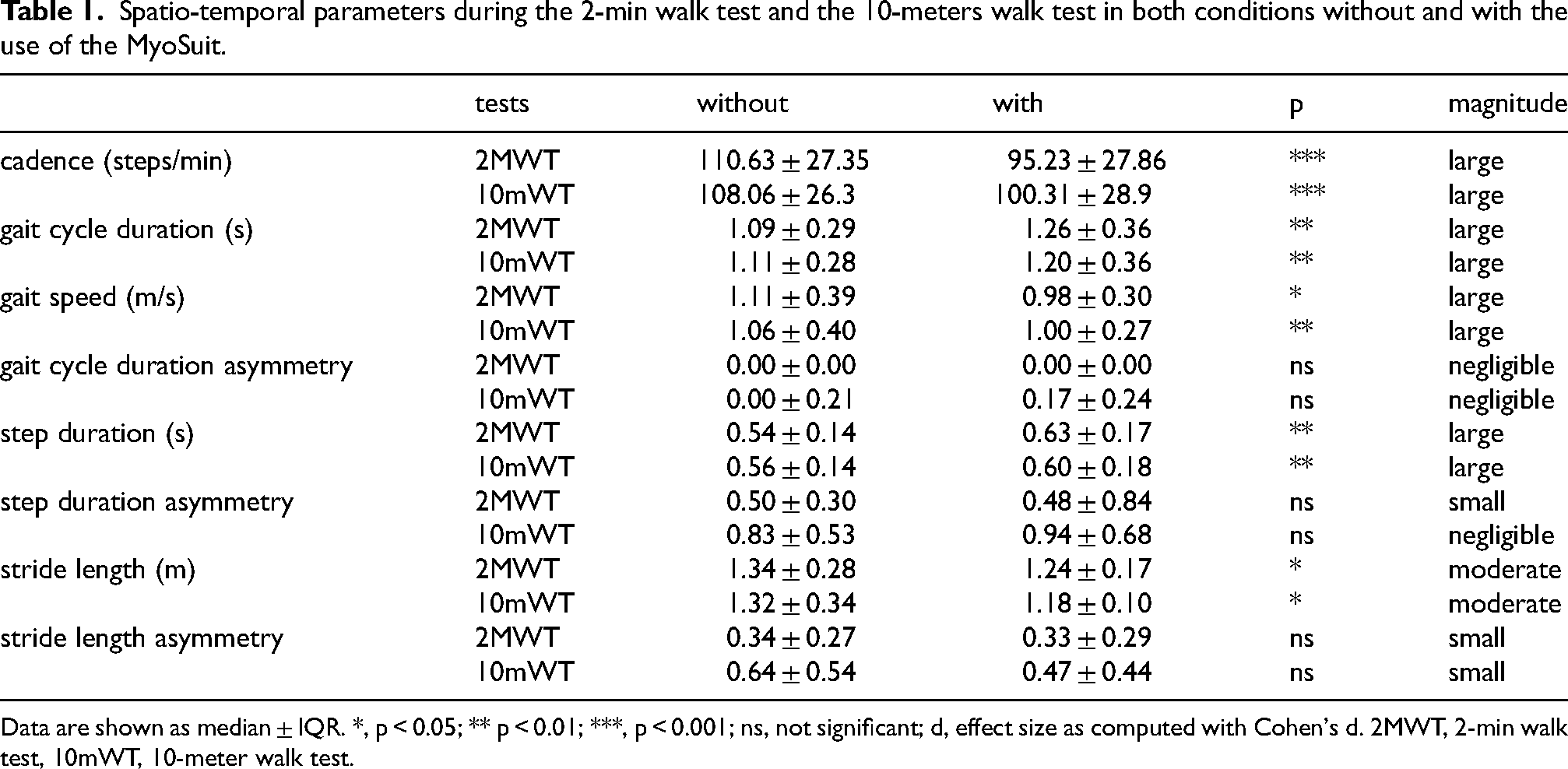
Data are shown as median ± IQR. *, p < 0.05; ** p < 0.01; ***, p < 0.001; ns, not significant; d, effect size as computed with Cohen's d. 2MWT, 2-min walk test, 10mWT, 10-meter walk test.
Normalized spatio-temporal static postural parameters in both conditions without and with the use of the MyoSuit.
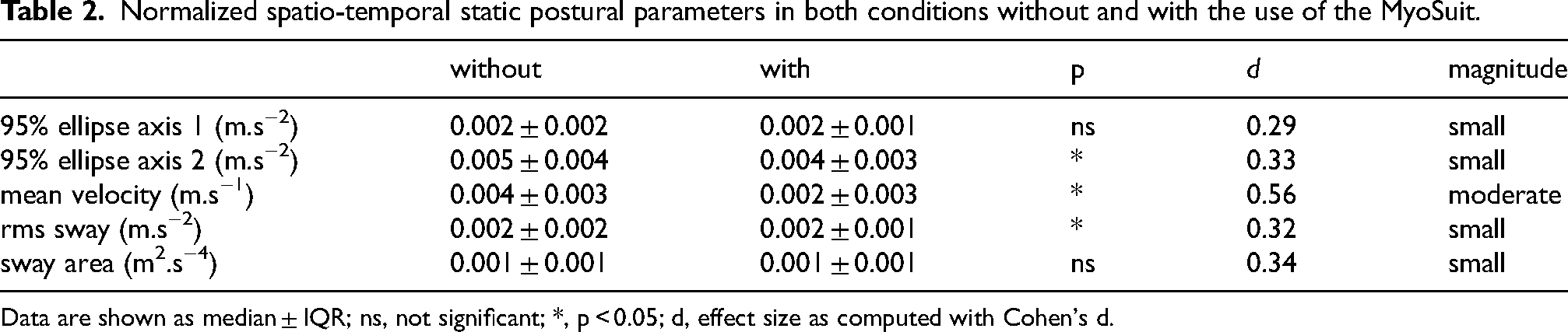
Data are shown as median ± IQR; ns, not significant; *, p < 0.05; d, effect size as computed with Cohen's d.
Regarding other tests, there was a significant performance decrease when using the device during STS30 (6.5 ± 5.0 vs. 7.0 ± 6.0 repetitions, p < 0.01). Postural SWAY variables are displayed in Table 2. Normalized mean velocity SWAY, RMS SWAY and normalized 95% ellipse were significantly lower when using the MyoSuit. During the 2MWT and 10mWT, gait speed, stride length and cadence were significantly decreased when using the MyoSuit with large effect sizes (all p < 0.05). Step duration was significantly increased with large effect size (p < 0.01). No statistical difference was found regarding asymmetries of gait cycle duration, step duration, and stride length (all p > 0.19).
Changes in perceived stability, exertion, dyspnea, and pain
Perceptions with and without the MyoSuit at the end of the STS30 and 2MWT are shown in Figure 3. Perceived dyspnea with use of the MyoSuit during STS30 was significantly lower with moderate effect size (2.5 ± 1.5 vs. 3.0 ± 3.0, p < 0.05). No statistical difference between conditions in perceived stability, exertion, and pain was found for other tests (all p > 0.05). Results regarding the usability (SUS) and the comfort (NMQ) while wearing the Myosuit are displayed in Figure 4.
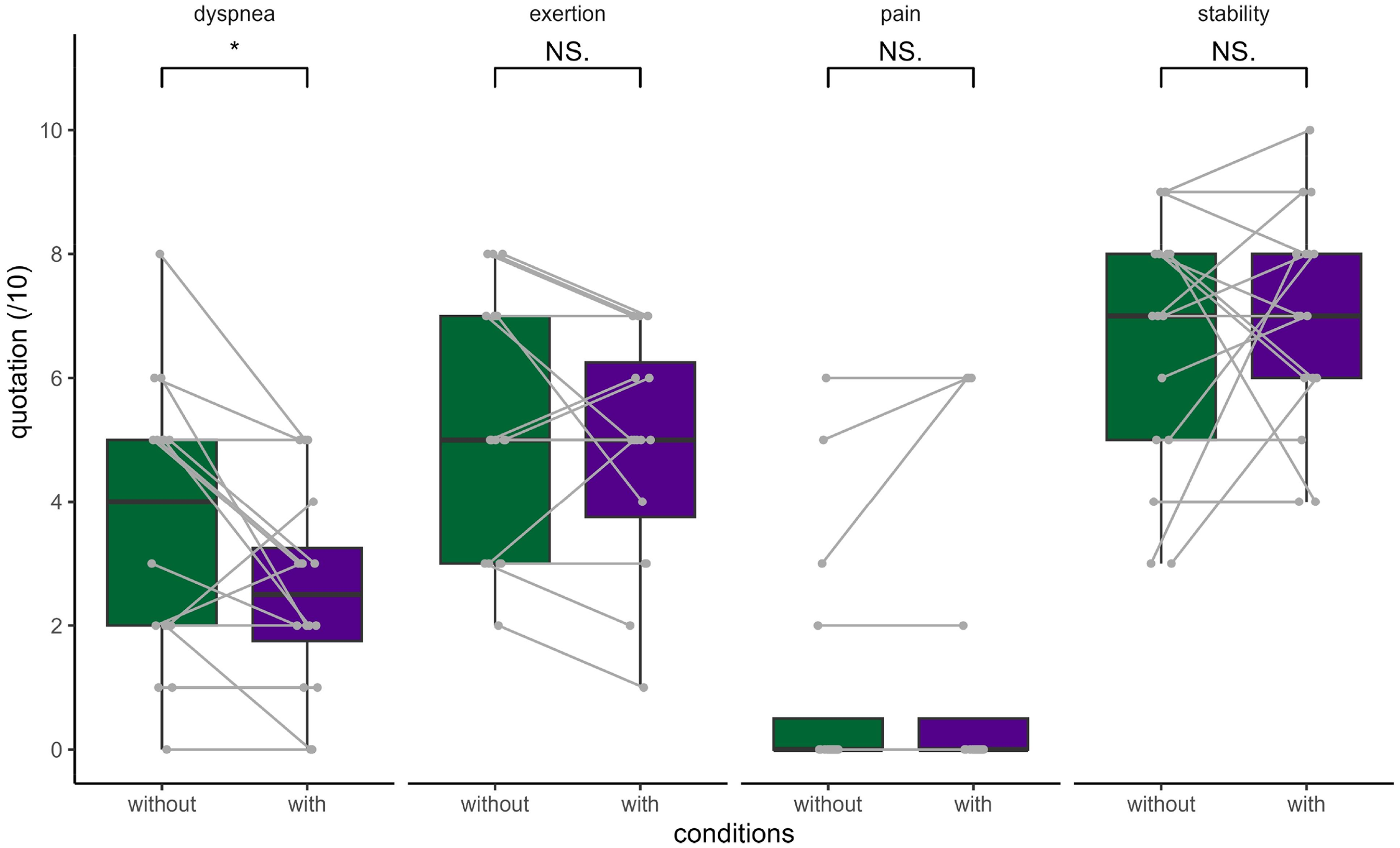
Comparison of verbal analog scale quotes of stability, exertion, pain, and dyspnea in condition without and with the assistance of the MyoSuit during 30-s sit-to-stand test. Quotes are displayed as boxes and whiskers plots, with the median (thick middle line), interquartile range (end of boxes) and vertical as range between maximal and minimal value Each participant is represented by a point in both the with and without exoskeleton conditions, connected by a line. *, p < 0.05.
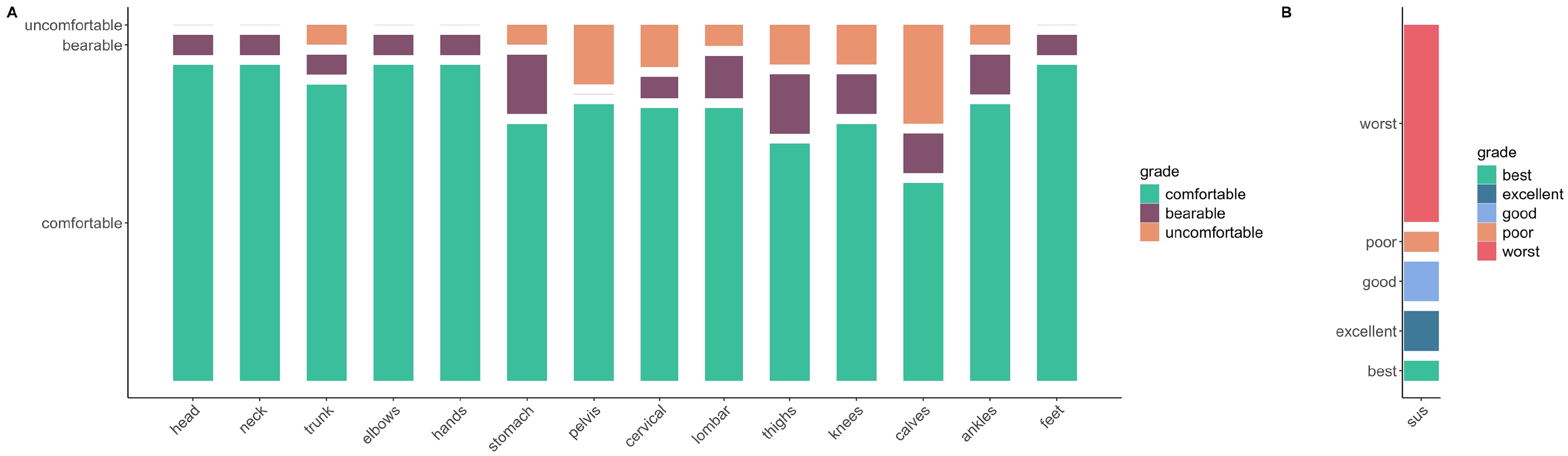
Distribution of the perceived comfort when using the MyoSuit assessed with the modified nordic questionnaire (A) and the usability of the device assessed with the system usability scale (B). In A, the scale is divided into 3 categories for each body part: comfortable (green), bearable (purple) and uncomfortable (orange). In B, the system usability scale (SUS) is divided into 6 categories of usability: best (green), excellent (dark blue), fair (pink), good (light blue), poor (orange) and worst imaginable (red). In both parts of the figure, the amplitude of each subcategory reflects the number of participants whose responses corresponded to it. Thus, the larger the amplitude, the greater the number of participants whose level of comfort or usability (A and B, respectively) matched that subcategory.
Joint kinematics
We were not able to record JA during 2MWT in four participants and in five participants during STS30 due to technical issues. Hip abduction-adduction, hip and knee flexion-extension and ankle dorsiflexion-plantarflexion angles during gait cycle during the 2MWT without and with the use of the exoskeleton are displayed in Figure 5. The range of motion for each measured joint and movement during both 2MWT and STS30 tests are displayed in Table 3. During 2MWT, hip flexion-extensionRoM was significantly lowered with moderate effect when using the MyoSuit during the stance phase (p < 0.01). Hip abduction-adductionRoM was significantly increased with the MyoSuit over both stance and swing phase in 2MWT with moderate effect (both p < 0.01) and decreased during STS30 test with large effect (p < 0.05). No other statistical difference in range of motion was found in any of the joints measured, either during STS30 or 2MWT. Results of statistical parametric mapping for joint angles are presented in Figure 5. A significant condition × time (percentage of the gait cycle) interaction was found for hip flexion-extension (all p < 0.05) with three blocks where there was a lower hip angle with the use of the MyoSuit during STS30.
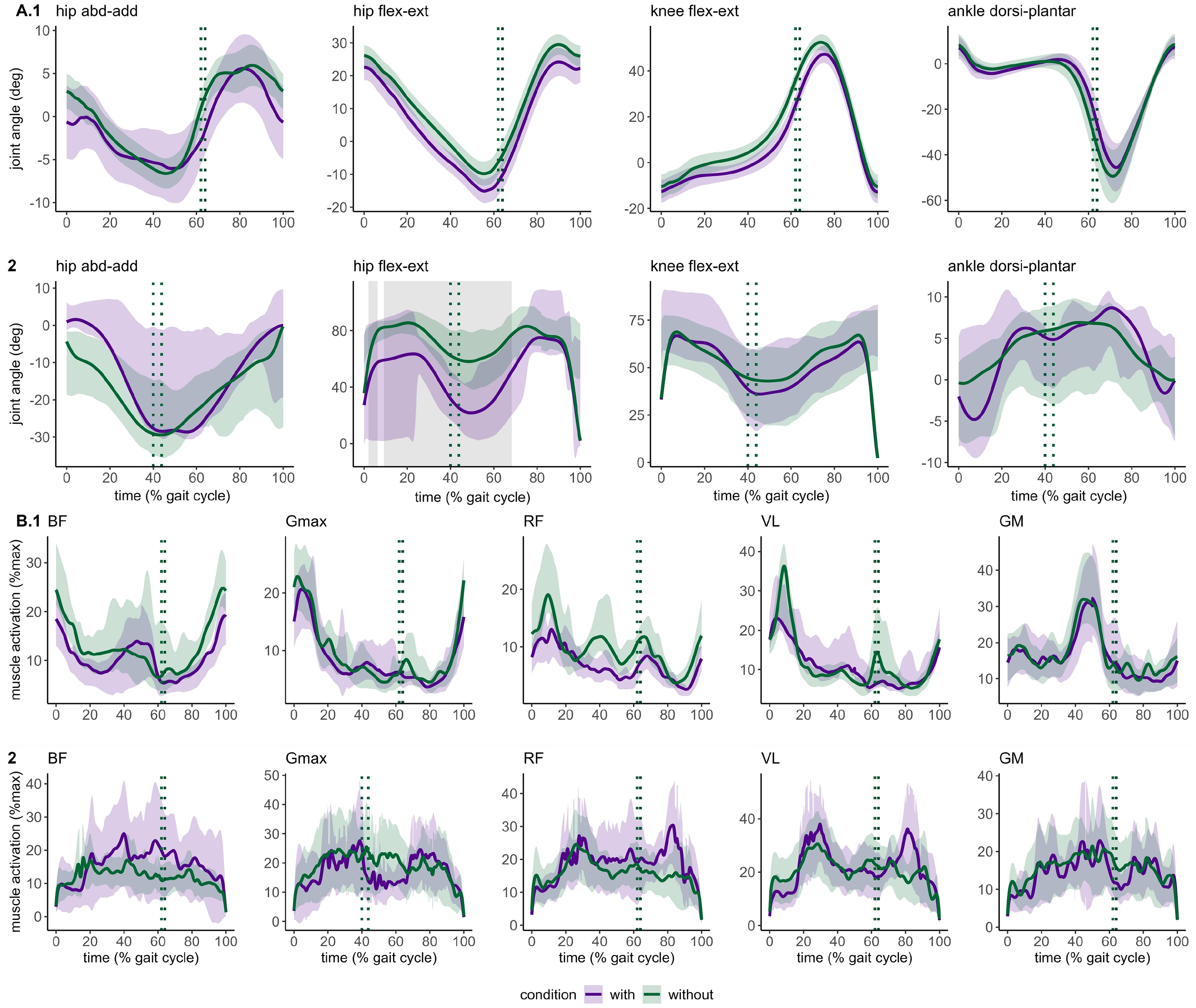
Average time-varying joint angle and electromyography (EMG) patterns measured during gait cycles (A and B, respectively) during the 2-min walk test (2MWT, A.1, B.1) and 30-s sit-to-stand (STS30, A.2, B.2). A represents joint angle amplitude data for hip adduction-abduction, hip and knee flexion-extension and ankle dorsi- and plantar-flexion. B displays EMG amplitude for biceps femoris (BF), gluteus maximus (Gmax), rectus femoris (RF), vastus lateralis (VL) and gastrocnemius medialis (GM). Thick lines are average joint angle and average normalized EMG (A and B, respectively) and shaded areas are the corresponding confidence intervals (95%). At 0% on the x-axis corresponded to heel strike in 2MWT (A.1 and B.2) and start of sit-to-stand in STS30 (B.1 and B.2). Vertical dashed lines show the average time of toe-off during the gait cycle and the sit-to-stand and stand-to-sit transition in STS30. Grey areas show the periods when a significant difference was observed without and with the MyoSuit in joint range of motion and EMG amplitude. All p < 0.05. abd, abduction; add, adduction; flex, flexion; ext, extension; dorsi, dorsiflexion; plant, plantarflexion; deg, degree.
Range of motion for hip, knee, and ankle without and with the use of MyoSuit in stance and swing phases during the gait cycles of the 2-min walk test and in sit-to-stand and stand-to-sit phases during the 30-s sit-to-stand test.
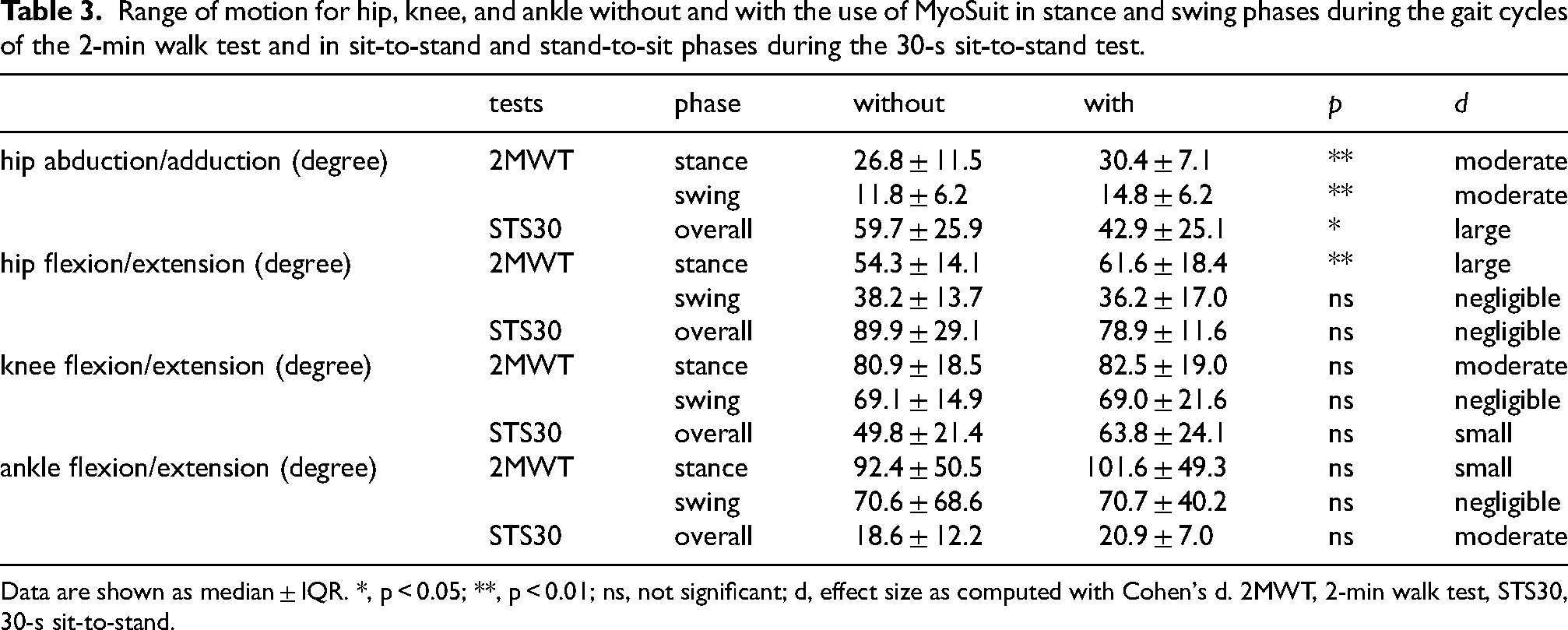
Data are shown as median ± IQR. *, p < 0.05; **, p < 0.01; ns, not significant; d, effect size as computed with Cohen's d. 2MWT, 2-min walk test, STS30, 30-s sit-to-stand.
Joints angle peak time variability during gait cycle are presented in Figure 6. A significantly larger hip flexionSD was found when using the MyoSuit (3.80 ± 2.73 vs 2.16 ± 0.93% of gait cycle, p < 0.01). Knee flexionSD and knee extensionSD occurred significantly sooner when using the MyoSuit with moderate effect (25.44 ± 17.03 vs. 35.74 ± 13.41%, and 1.78 ± 1.19 vs. 2.26 ± 1.72% of gait cycle, respectively, both p < 0.05). No statistical differences were found for any of the JAavg time occurrence.
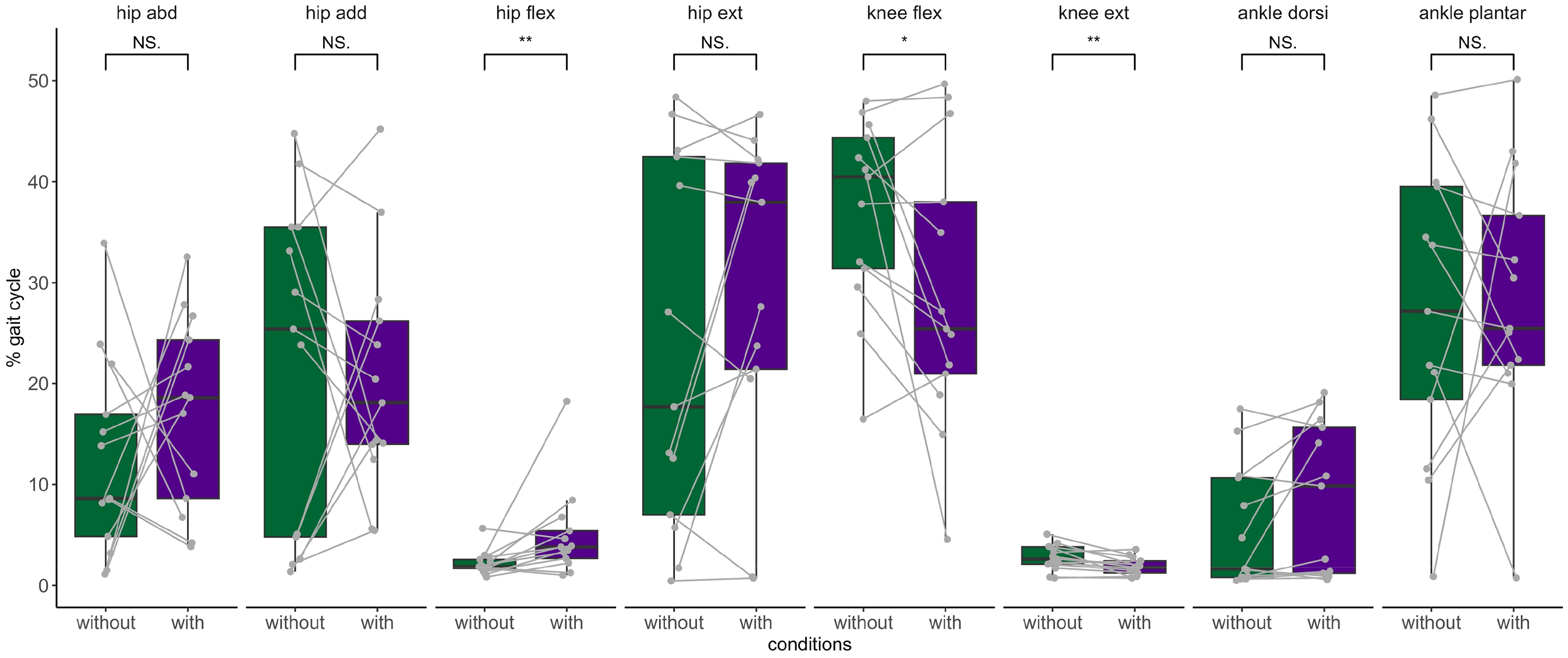
Comparison of standard deviations’ peak occurrence (in percentage of gait cycle) of the hip abduction, hip adduction, hip flexion, hip extension, knee flexion, knee extension, ankle dorsiflexion and plantarflexion. The standard deviation time peak occurrence is the time variability when the joint motion is at its peak angle. Box and whisker plots represent the distribution of the values, thick line is the median, thin lines of the box are interquartile, and vertical line is the range between maximal and minimal value Each participant is represented by a point in both the with and without exoskeleton, connected by a line. flex, flexion; plantar, plantarflexion; abd, abduction; ext, extension; dorsi, dorsiflexion *, p < 0.05; **, p < 0.01 and ***, p < 0.001; NS, not significant.
Results for kinematics parameters during 2MWT and 10mWT gait tests are presented in Table 4. Time spent in stance was significantly increased during both 2MWT and 10mWT when using the device (time duration in percentage of the gait cycle for double support, single limb support, swing and stance, all p < 0.001). Double support time spent during stance phase was significantly longer (p < 0.001) and time spent with a single limb support was reduced when using the device (p < 0.001). During the 2MWT, the circumduction was significantly greater with moderate effect (p < 0.05). No statistical differences were observed regarding asymmetry.
Comparison of spatio-temporal gait parameters of locomotion without and with the use of MyoSuit during 2-min walk test and 10-meter walk test.
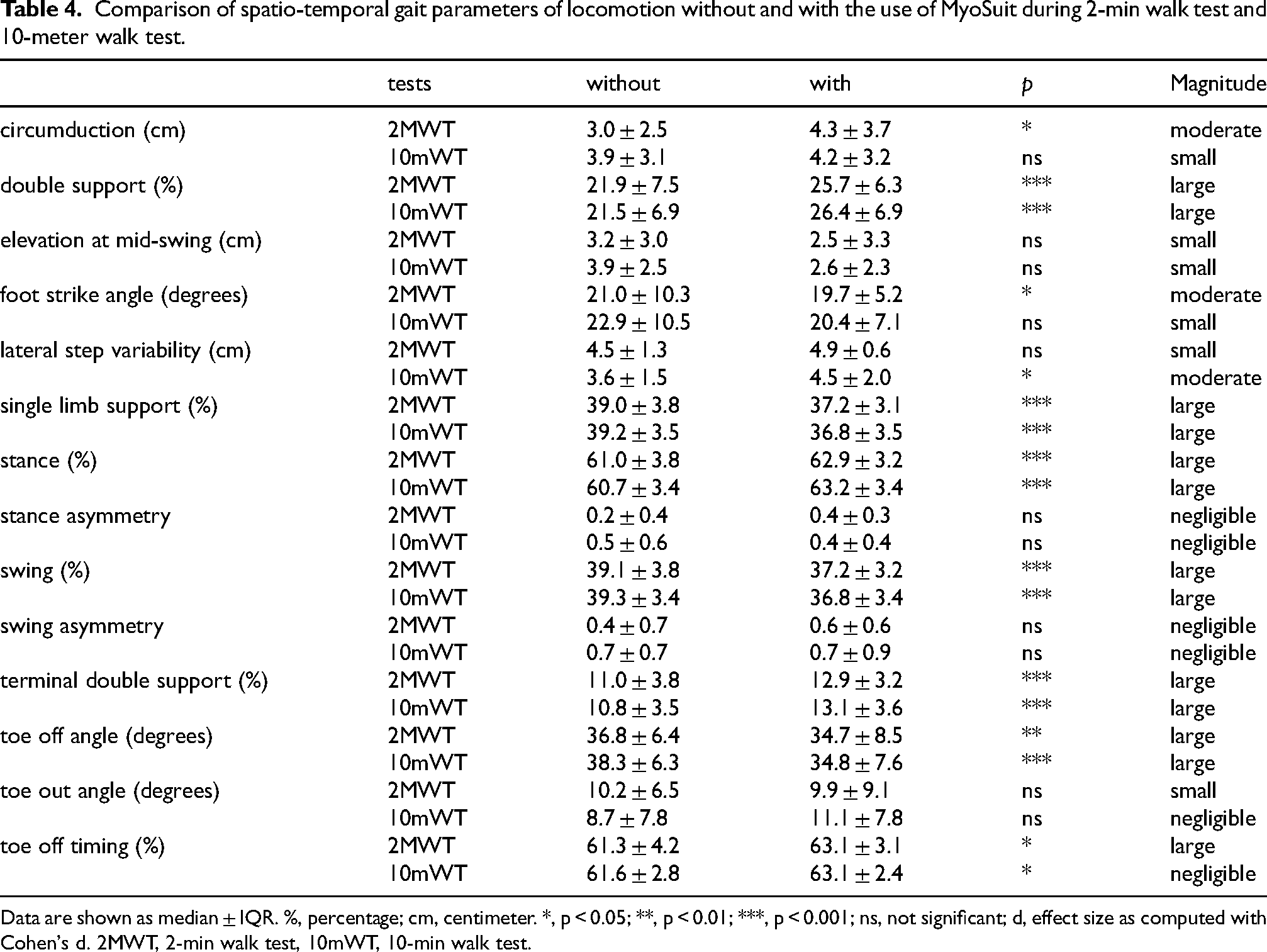
Data are shown as median ± IQR. %, percentage; cm, centimeter. *, p < 0.05; **, p < 0.01; ***, p < 0.001; ns, not significant; d, effect size as computed with Cohen's d. 2MWT, 2-min walk test, 10mWT, 10-min walk test.
Muscle activation patterns
Muscle activation and workload as assessed with EMG during 2MWT and STS30 are presented in Figure 7. During 2MWT, no statistical differences were observed in any muscle regarding peak activation. RFAUC was significantly reduced while wearing the exoskeleton over the whole gait cycle with moderate effect (57.6 ± 40.1 vs. 93.95 ± 84.35, p < 0.05). During the 2MWT, GMavg occurred significantly sooner (35.6 ± 19.1% gait cycle vs. 45.4 ± 12.8% gait cycle, p < 0.001) and GmaxSD was significantly lower with the device (32.0 ± 26.1% gait cycle vs. 33.0 ± 18. % gait cycle, p < 0.05). No statistical difference in median power frequency was observed in any studied muscle (all p > 0.2). During STS30, RFpeak and RFAUC in stand-to-sit phase were significantly higher when using the MyoSuit (35.03 ± 31.60 vs. 25.73 ± 22.77% and 92.8 ± 60.7 vs. 72.8 ± 61.4, respectively, both p < 0.05). BFAUC during STS30 was significantly reduced with the device (66.3 ± 154.7 vs. 121.2 ± 103.1%, p < 0.05). No other statistical difference was found in other muscles (all p > 0.08). Results of statistical parametric mapping are displayed in Figure 5. A significant condition x time (percentage of the gait cycle) interaction in VL muscle was found in 2MWT.
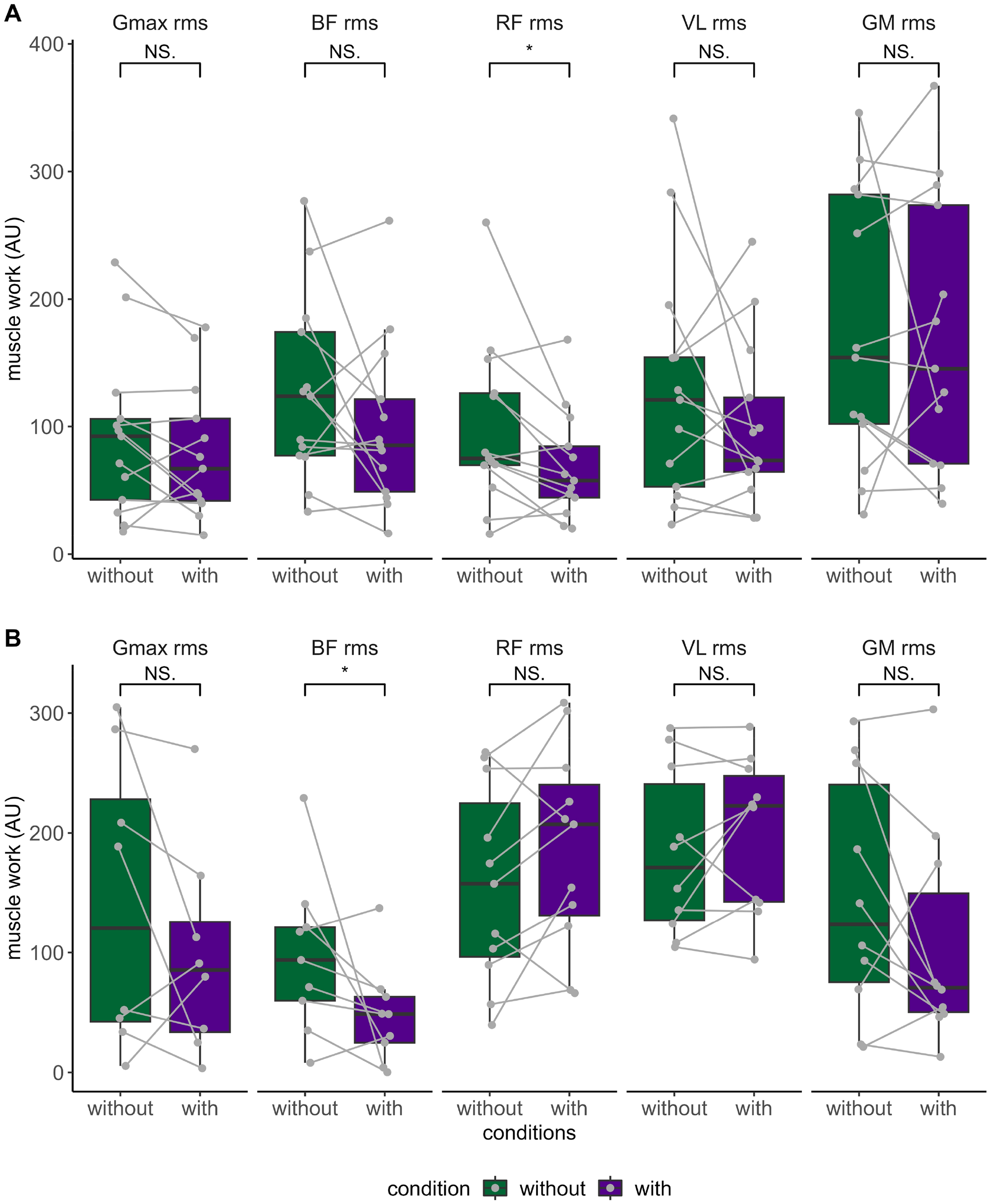
Comparison of muscle work overall gait cycle (A) and muscle work overall sit-to-stand and stand-to-sit cycle (B) of the gluteus Maximus (gmax), Biceps femoris (bf), Rectus femoris (rf), Vastus Lateralis (vl) and gastrocnemius Medialis (gm). Box and whisker plots represent the distribution of the peak normalized muscle activation, thick line is the median, thin lines of the box are interquartile, and vertical line is the range between maximal and minimal value. Each participant is represented by a point and a line linked condition without and with the use of the MyoSuit. *, p < 0.05; **, p < 0.01; NS., not significant; AU, arbitrary unit.
Determinants of changes in performance when using the MyoSuit during the 2MWT and STS30
The predicted 2MWT distance results were processed by incorporating data collected both with and without the device into the model. Significant positive relationships were found between 2MWTpred and predicted muscle strength in flexion and extension for both hip and knee flexors/extensors (all r > 0.25 and p < 0.05). Toe off time was negatively associated to 2MWTpred (r = –0.61, p < 0.0001). Pain was negatively associated with 2MWTpred (r = –0.50, p < 0.0001). Spatio-temporal parameters were associated with the magnitude of decreased in gait performance when using the device (Figure 8.A). We observed longer time spent in double support (r = -0.56, p < 0.001), higher lateral step variability (r = -0.39, p < 0.001), shorter stride length (r = 0.73, p < 0.001), and longer step duration (r = –0.79, p < 0.001) were related to smaller 2MWTpred. Hip abductionSD and ankle dorsiflexionSD were negatively correlated with 2MWTpred (r = –0.47 and −0.46, respectively, both p < 0.0001). Lower foot strike angle was associated with lower 2MWTpred (r = 0.36, p < 0.05).
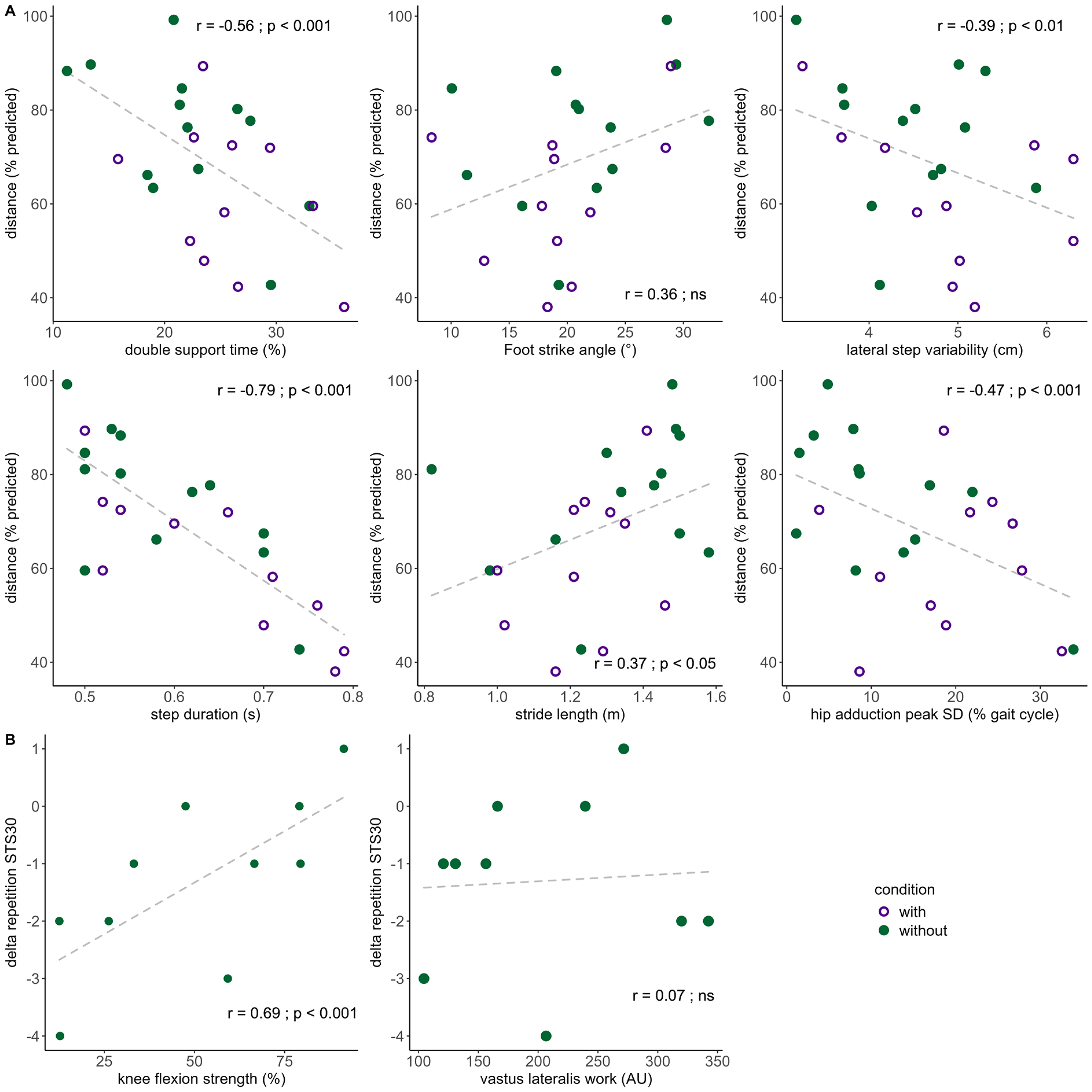
Relationship between (A) 2-min walking distance (2MWT) and most selected features in penalized least absolute shrinkage and selection operator (LASSO) regression model and (B) in 30-s sit-to-stand (STS30) repetitions and selected features in penalized LASSO regression model in patients with neuromuscular diseases when using or not the MyoSuit. The 2MWT distance in relationship with double support time duration, ankle angle at foot strike, lateral step variability, step duration, stride length, and the standard deviation of hip adduction occurrence. The difference in assisted and unassited STS30 performance in relationship knee flexion strength and vastus lateralis muscle activation workload. Each participant is represented by a unique colored point (without MyoSuit), and a diamond (with MyoSuit) during 2MWT and each participant is represented by a point (delta performance) in STS30. Correlation coefficient (r) and p values are shown.
Penalized LASSO regression model results are displayed in Figure 9 and Table 5 for both 2MWT and changes in STS30. In the first 1000 LASSO models, double support time duration, ankle angle at foot strike, lateral step variability, step duration, stride length and hip abductionSD were selected over fifty percent of the time within the best half LASSO models for 2MWT. The performances of the models with all features versus 6 features were compared using R2 and reduced overfitting was observed (R2 = 0.65 with all features and R2 = 0.85 with 6). The performance of the 500 best models using six variables were as follows: MSE was 29.0 ± 19.3, R2 was 0.85 ± 0.15 and RMSE 5.1 ± 1.7% 2MWTpred and MAE was 4.2 ± 1.5% 2MWTpred. Variances for each participant between actual and predicted 2MWTpred and actual versus predicted delta performance STS30pred using both models are displayed in Figure 9. The performance of the final LASSO model with the whole dataset was as follows: MSE = 12.0, R2 = 0.96, and MAE = 2.6% 2MWTpred. Regarding changes in STS30 performance, the first 1000 LASSO models selected predicted knee flexion strength, and VLAUC as predicting variables. The performance between the model using two features versus the model using all features of the 500 best models was as follows: R2 was 0.71 ± 0.19 vs. 0.45 ± 0.21, MSE was 1.4 ± 1.0 vs. 4.3 ± 2.0, RMSE was 1.1 ± 0.5 vs 1.9 ± 0.8 delta STS30pred, and MAE was 1.0 ± 0.4 vs. 1.7 ± 0.8% delta STS30pred. The performance of the final LASSO model using the entire dataset was as follows: MSE = 0.72, R2 = 0.68, and MAE was 0.69 STS30pred.
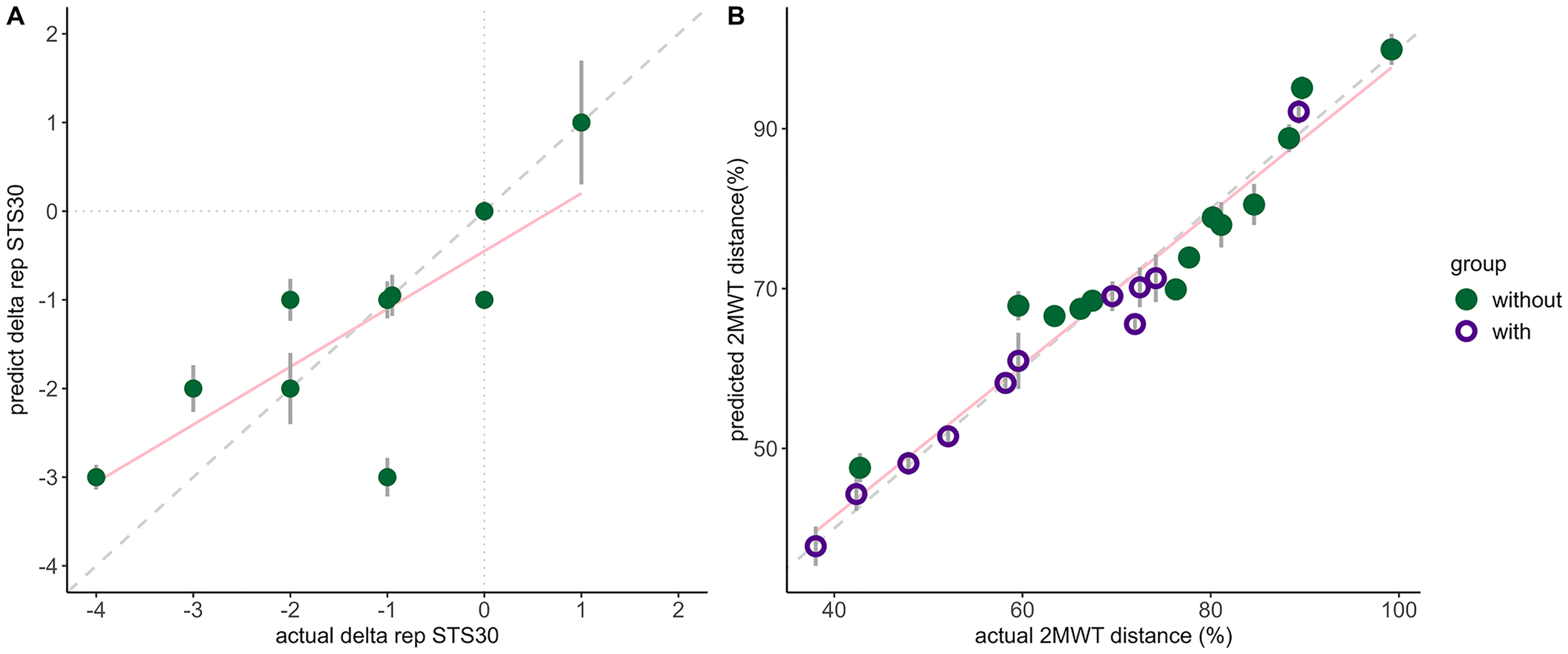
Penalized least absolute shrinkage and selection operator (LASSO) regression prediction to predict 2-min walk test distance (B) and during 30-s sit-to-stand (A). A represents the comparison between actual and predicted percentage of 2MWT predicted distance. Circle (without) and diamond (with) represented participants, and a unique color is attributed to each participant (n = 24). B represents the comparison between actual and predicted delta repetitions with versus without the MyoSuit during STS30. Circle represented participants (n = 10). Vertical grey associated is the variance of their own prediction, dashed grey line corresponds to the identity line, and pink line is line of the penalized LASSO regression. Model predicting 2MWT distance used the step duration, toe-off angle, perceived stability, ankle dorsiflexion and knee extension strength and average in ankle dorsiflexion, plantarflexion, and hip flexion peak occurrence and model predicting delta STS30 used hip and knee flexion strength and Rectus Femoris and Vastus Lateralis activation work. Id, participants.
Penalized least absolute shrinkage and selection operator (LASSO) regression equation parameters predicting 2-min walk test performance using the seven most selected features and predicting 30-s sit-to-stand assisted performance based on the three features measured in unassisted condition.
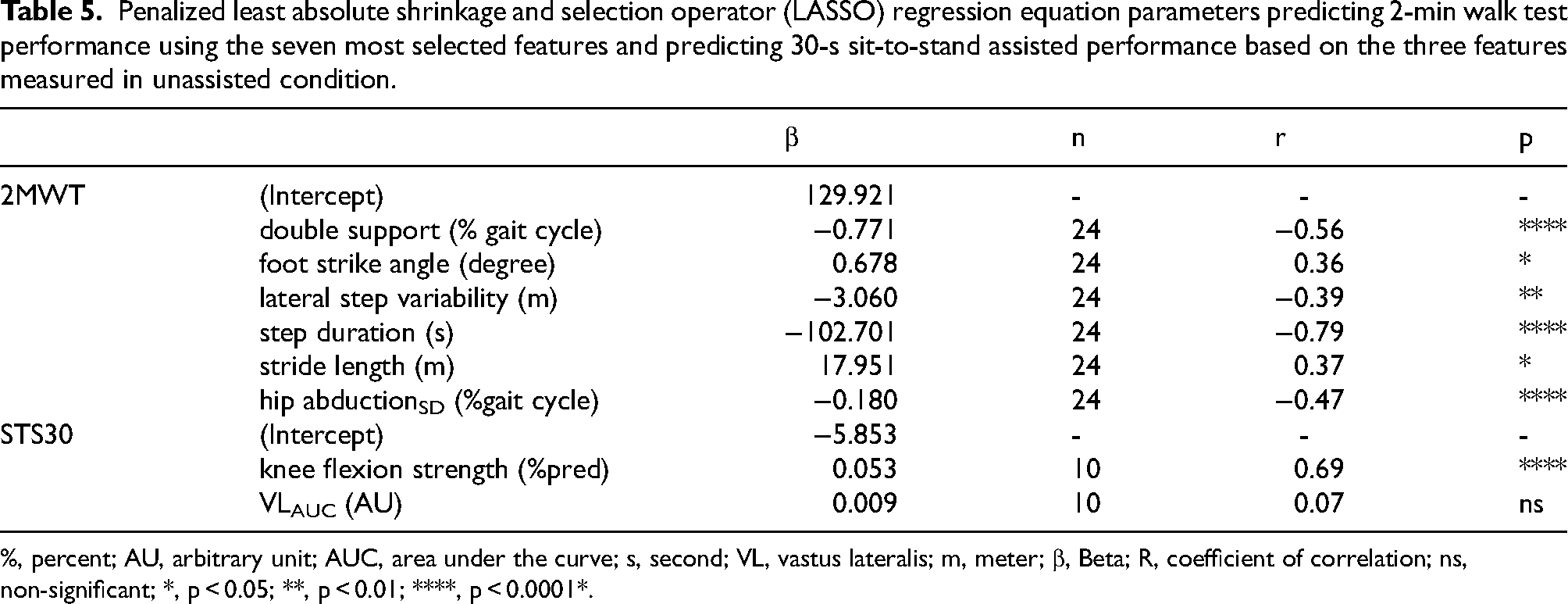
%, percent; AU, arbitrary unit; AUC, area under the curve; s, second; VL, vastus lateralis; m, meter; β, Beta; R, coefficient of correlation; ns, non-significant; *, p < 0.05; **, p < 0.01; ****, p < 0.0001*.
Discussion
This study aimed to investigate the effects of the bi-articular assistive exoskeleton MyoSuit in adults with NMD on gait, sit-to-stand/stand-to-sit transitions, and static postural stability. To the best of our knowledge, this is the first study to assess the effects of the MyoSuit on muscle activation, perceptions, movement kinematic and spatio-temporal parameters, during standardized functional tasks in individuals with NMD. The use of the MyoSuit was safe with no adverse events. At the group level, performances during the 10mWT, STS30, and 2MWT were reduced with the device while static postural stability improved. Few participants equaled or improved performance in each assessed functional task with the use of the MyoSuit. The device also induced greater hip abduction during gait highlighting an increase in circumduction of the lower limbs. We also found reduced activation in hip flexors during the gait cycle. During sitting transfers, hip abduction activation was reduced resulting in standing up kinematic pattern change. Models were built to predict performance in the 2MWT and STS30 when using the device. Key determinants of 2MWT distance identified with a LASSO regression were time spent in double support, lateral step variability, step duration, stride length, and the kinematic variability in hip abduction-adduction. The model predicting changes in STS30perf highlighted knee flexion strength capacity and VL muscle activation workload without the device as predictors.
Effects of the MyoSuit on static postural stability
Postural stability was impaired as previously observed in patients. 22 Sway and velocity of the center of mass with the MyoSuit was reduced, suggesting a positive effect on static postural stability. 22 One key question was the balance between negative effect of added mass and the benefits of the assistance. In contrast with previous work assessing the effects of backpack loading, 23 we did not observed increased GM muscle activation suggesting that the repartition of weight and/or the benefits of constant assistance during standing favored a more stable posture. 24 One must note that muscle activation was low during this test (below 8%), which might have limited the detection of potential changes. Static stability was assessed with eyes open that might have hindered the detection of changes. 25 Finally, potential changes in perceptions using the VAS scale might not have been detected, particularly in stability and exertion, due to the ceiling and floor effect of this type of scale.
Effects of MyoSuit on stand-to-sit, sit-to-stand transitions and gait patterns
As hypothesized, the number of repeated sit-to-stand/stand-to-sit transition was significantly reduced at the group level when using the MyoSuit. Interestingly, three of four patients who improved or maintained their STS30 performance received the lowest assistance levels and did not have the highest or lowest lower limb strength. In contrast with previous research, 7 the combined assessment of kinematic and muscle activation during sitting transfer provided detailed insights regarding the effect the MyoSuit on STS30 biomechanical patterns. The muscle activation patterns in the VL and Gmax muscles were similar to those previously observed using the MyoSuit during sitting transfers (Figure 5). 7 The distribution of muscle activation between antagonists only regarded bi-articular muscles, with an increase in RF activation (hip flexor and knee extensor), and a decrease in BF activation (hip extensor and knee flexor) with the MyoSuit. During the stand-to-sit phase, the RF muscle was engaged in an eccentric contraction to slow down the descent onto the chair. The additional weight of the MyoSuit, combined with minimal assistance during the sitting phase, likely resulted in elevated RF muscle activation. In contrast, BF muscle activation decreased over time in both phases of sitting transfers (Figure 5). The initiation of the chair rise extension phase is associated with hip extension, 26 which also triggers the assistance, thereby reducing BF activation. During the seating transition, BF activation was minimal (< 10%), likely due to the timing of tendon release by the MyoSuit. This release limited BF activation, as the eccentric hip extension was already being supported by the device. The only kinematic pattern that was altered when using the device was hip abduction-adduction, which showed a reduced range of motion. Weaknesses in hip flexors and extensors are known to induce important compensations. One common strategy is to increase circumduction by producing higher hip abduction to produce strength to stand up and maintain stability. Hip abduction-adduction may be reduced by the MyoSuit's assistance in hip extension, compensating for impaired strength and enabling participants to position their feet more easily when standing.
As anticipated, gait performance during the 2MWT was also reduced at the group level when using the MyoSuit. These findings differed from previous results from studying adults with lower-limb weaknesses or teenager with cerebral palsy, both reported increased in gait performance while wearing the device.7,27 Effects of training should be considered as motor adaptations to MyoSuit assistance may be longer due to movement compensations in individuals with NMD. 7 As other research noted, progression during assisted and unassisted functional task may be attributed to both learning and rehabilitation effects, thus one cannot rule out that some participants might have improved their performance after more training sessions. 28 Changes in spatio-temporal gait parameters uncovered with the MyoSuit suggest a notable shift towards a more stability-oriented gait pattern, rather than performance. However, participants did not report any improvements in perceived stability during the 2MWT with the device. The MyoSuit induced a slower walking pace in participants, as evidenced by a decrease in gait speed and stride length coupled with an increase in step duration. Interestingly, despite differences in age, pathology, and small sample sizes across studies, similar patterns of slower walking speed and reduced stride length have been observed, suggesting consistent spatiotemporal effects of the device.27,29 Although participants showed comparable functional capacity at baseline, their underlying etiologies differed, and congenital forms are likely associated with longer-standing adaptations. This limits the extent to which the present findings can be generalized across all NMDs. This is further supported by increased double support time, reduced single-limb support time, and prolonged stance phase duration. Prolonged double support, a critical phase for balance due to the wider support polygon, may be partly attributed to the added mass, layer stiffness, and inertia of the device. 7 The decrease in gait speed during the 2MWT was likely due to significant reductions in cadence and stride length, with the latter potentially resulting from the powered assistance limiting leg extension and propulsive function at the end of the stand phase. Moreover, the altered biomechanical pattern caused by the tendon shortening and release timing may have contributed to the reduced cadence and thus, gait speed. This aligns with previous findings that increased stance phase duration is associated with lower gait speed in patients with NMD. 30 These differences in biomechanical gait patterns with and without the MyoSuit highlight several critical changes in kinematic and muscle activation. Increased hip abduction-adductionRoM during the stance phase suggests that strength impairment forced participants to compensate with higher hip mobility in the frontal plan. In patients with NMD, impaired gait is often associated with hip flexor weakness, inducing compensations such as circumduction to keep moving the leg forward, which increases hip abduction. 31 The hip joint exhibited greater movement amplitude and increased variability in extension, which could enhance stride length but is hindered by the temporal variability caused by the termination of the assistance at toe-off. The peak of hip extension and tendon release occurring together at the end of the stance phase causes random tendon release, leading to significant risk of imbalance, especially in patients with NMD. Interpretation of hip pattern changes is hindered by the lack of information regarding gluteus medius and minimus muscle as hip abductors. Knee extension assistance at the start of the stance phase supplemented the eccentric contraction of the quadriceps muscles to counteract gravity, resulting in reduced activation of the RF. The knee extension and flexion time variability decreased at their highest joint angle and might resulted in increasing knee stability, reducing the risk for knee buckling. An earlier GM activation may enhance push-off power during the late stance phase of gait, contributing to reduce the ankle plantarflexion propulsive effect while maintaining stability. 32 Of note, changes in kinematic and muscle activation during gait cycles may also be explained, at least in part, by the reduced gait speed. One major limitation of our work is the use of IMUs for kinematic assessment, which has demonstrated limitations in populations with gait impairments. The device's initialization period may introduce inaccuracies in joint angle measurements at the start of the gait cycle. Therefore, we opted to report only joint range of motion values.
Determinants of reduced gait performance when using the MyoSuit
The present study identified six key determinants predicting 2MWT performance, providing comprehensive insights on the effects of the MyoSuit on gait performance. Spatio-temporal gait parameters, which decreased significantly with the MyoSuit, were crucial for explaining the reduced 2MWT distance. Among them, the time spent in double support phase emerged as a key determinant. Longer double support time duration indicated a compensatory mechanism in patients with NMD attempting to enhance balance. In addition, step duration was longer when using the device and largely influenced by longer double support duration. The MyoSuit appears to focus on increasing leg support through tendon shortening, enhancing static and dynamic stability rather than improving gait performance, which leads to an extended stance phase. The added weight and movement compensation altered the feedback to the assistance algorithm, which may have prioritized gait stabilization. This resulted in increased double support time and step duration, reflecting lower gait performance with the assistance. Stride length is a direct indicator of gait speed and was found to be a key determinant of the reduced 2MWT distance. Shorter stride lengths are typically associated with reduced lower limb strength and joint range of motion. 33 The assistance in hip and knee extension stabilized the leg on the ground, but the assistance did not allow participants to increase the patient's ability to do longer stride length in comparison with unassisted gait pattern. Lateral step variability, which reflects inconsistencies in step width, suggests that patients with lower 2MWT performance, especially when using assistance, were searching for balance. Kinematic variability of the hip adduction was also identified as determinant in reduced 2MWT distance. Variability in hip adduction timing indicated that the use of the MyoSuit may be responsible for increased CoP variability in dynamic condition. The pelvic instability induced by impaired muscle strength suggested its crucial role in gait impairments. 31 Additionally, impaired hip muscle strength could diminish the positive effects of the assistance, which primarily focuses on enhancing antero-posterior stability during walking. Finally, a lower ankle angle at foot strike was characteristic of reduced 2MWT performance, aligning with previous studies on the effects of lower gait speed. 33 Although the ankle joint was not directly assisted, the MyoSuit affected it by reducing its range of motion at heel strike. This reduction predicted lower 2MWT performance due to an impaired push-off phase, leading to less effective propulsion. 34 A flatter foot strike, often seen in individuals with NMD, was caused by impaired dorsiflexors that was likely exacerbated by the added weight during the swing phase. Consequently, a flatter foot strike may lead to increased energy expenditure and decreased walking speed and distance.
Determinants of performance changes in STS30 when using the MyoSuit
The model predicted changes in STS30 performance with assistance from the MyoSuit based on unassisted kinematic, muscle activation, VAS, and strength capacity measurement. As one participant improved performance and two others maintained it, we sought to identify the reasons only a few patients with NMD benefited from the MyoSuit while the majority of them did not. Our findings highlighted unassisted knee flexion strength, and VL muscle workload outcomes were predictors for improvement in STS30perf with assistance. Enhanced knee flexion strength improved control, predicting more repetitions within the assisted STS30 test. Since the MyoSuit does not assist in knee flexion, this strength likely plays a key role in maintaining balance during the movement, significantly increasing STS30's performance in assisted condition. Knee flexor muscles play a key role at the end of the sit-to-stand phase, acting as antagonists by co-contracting eccentrically to balance the hip and knee extensors. 26 The positive relationship between knee flexion strength and improved STS30 performance suggests that patients with higher knee flexion strength would better perform with the use of the MyoSuit. In addition, maintaining stability from unassisted joint movement, in combination with powered assistance, is crucial for improving performance in individuals with NMD. The VL muscle workload was the second predictor in the model. The VL muscle, as a knee extensor, is essential for both standing up from a seated position and controlling the stand-to-sit transition through eccentric contraction. The MyoSuit assists knee extensor muscles when standing up. 6 However, no relationship was found between unassisted VL muscle workload and the ability to benefit from MyoSuit assistance in STS30. The results suggest a non-linear relationship between VL activation and assisted sit-to-stand improvements, as one of the four knee extensors, does not consistently compensate and its contribution varies relative to the other. Participants who benefited from the MyoSuit had moderate VL muscle workload, while those who experienced decreased performance had either higher or lower workload without assistance. This may indicate that optimal knee extensor strength is crucial for effectively benefiting from MyoSuit assistance. However, further investigation should be done with a larger sample size to better understand the relationship between knee extensors muscle strength and changes in STS30perf. Altogether, both force production capacities appear to be crucial in gaining performance with assistance, as they play a key role in triggering the assistance and following the inertia of the movement to maintain stability until the trunk is fully upright in a standing position. Impaired strength capacity and muscle activation of knee joint during STS30 without assistance were key predictors supporting our hypothesis that the device would benefit participants with lower weakness.
Although the models for both sit-to-stand transition and walking tests showed good predictive performance, further investigations with larger sample sizes are necessary to validate these findings and ensure their generalizability. Another limitation is that participants performed the functional tasks, using their usual technical aids, if needed. While this approach ensured ecological validity and each participant were considered as their own control, the potential impact of technical aids on outcomes remains. Future studies could test the “technical aid” effect on predictive models. This approach provides a nuanced understanding of the complex interplay between muscle strength, activation patterns, and functional outcomes, offering a robust framework for designing effective assistive devices in individuals with severe muscle weakness.
This study evaluated the MyoSuit exoskeleton's effects on gait, sit-to-stand transitions, and static postural stability in patients with NMD. While the results showed that participants experienced some level of assistance, there remains potential for further optimization. However, usability scores and discomfort reports indicated that the current version of the device is perceived as poorly usable and uncomfortable by many participants, which may limit its acceptability. Assessing the impact of such devices in individuals with NMD is inherently complex due to the wide variability in terms of usability, comfort, muscle weakness and compensatory mechanisms within this population. As a result, generalizing outcomes can be challenging. Since assessments were performed after only a brief familiarization period, the findings primarily reflect short-term effects and may not capture potential gains that could emerge with repeated use or progressive training. Future designs should focus on tailoring the exoskeleton to better address these diverse biomechanical needs, suggesting promising avenues for enhancing its effectiveness and overall support for functional improvement in this population.
Footnotes
Acknowledgments
We gratefully acknowledge MyoSwiss AG (Zurich, Switzerland) for providing access to the MyoSuit device, which made this work possible. We extend our sincere gratitude to the participants in this study.
Ethical considerations
The study conformed to the Declaration of the Helsinki and was approved by the ethics committee (ID RCB: 2019-A00155-52; NCT05199246).
Consent to participate
All participants provided informed written consent
Author contributions statement
RF and DB conceived and designed research, performed experiments, analyzed data, interpreted results of experiments, prepared figures, drafted manuscript, edited and revised manuscript, approved final version of manuscript. CA, CG and JS performed experiments, analyzed data, and approved final version of manuscript. FF analyzed data, edited, and revised manuscript, approved final version of manuscript. GB and OB conceived and designed research, edited and revised manuscript, approved final version of manuscript. JYH conceived and designed research, edited and revised manuscript, approved final version of manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
King Baudouin Foundation United States, French Muscular Dystrophy Association (AFM-Téléthon).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.