
Abstract
Objective:
This scoping review aims to explore and map the most frequently reported limitations in activities of daily living (ADLs) among individuals with spinal muscular atrophy (SMA), with the goal of informing clinical assessment and multidisciplinary care strategies.
Methods:
The review followed the Joanna Briggs Institute (JBI) methodology for scoping reviews and adhered to the PRISMA-ScR reporting guidelines. A comprehensive search was conducted across PubMed, Scopus, Web of Science, and Embase up to December 2024. Eligible studies included qualitative, quantitative, and mixed-methods designs that reported ADL limitations in individuals with any SMA subtype. Data were extracted and descriptively synthesized, with additional input from a multidisciplinary rehabilitation team to provide practical clinical recommendations.
Results:
Sixteen studies were included, encompassing a wide range of methodologies and SMA types. The most frequently reported ADL limitations included mobility (e.g., walking, transferring, climbing stairs) and self-care tasks (e.g., dressing, toileting, feeding). Upper limb function and instrumental ADLs, such as cooking, writing, and technology use, were less frequently assessed but emerged as important in maintaining autonomy, particularly in adults. Recent studies post-gene therapy demonstrates a broader focus on daily functioning and patient-reported outcomes. A multidisciplinary framework outlining domain-specific interventions and professional roles was developed based on the extracted data.
Conclusions:
While mobility remains central to SMA-related disability, this review highlights the substantial burden of self-care and upper limb limitations. Findings support a shift toward more comprehensive, patient-centered assessment and rehabilitation approaches in SMA care.
Introduction
Spinal muscular atrophy (SMA) is a rare neurodegenerative disorder caused by a deficiency of the survival motor neuron (SMN) protein, most commonly due to homozygous deletions or mutations in the SMN1 gene with an estimated prevalence of 2.12/100,000.1–3 The condition leads to progressive degeneration of lower motor neurons in the spinal cord, resulting in symmetrical muscle weakness, hypotonia, and atrophy. Clinically, SMA manifests across a spectrum of severity, from the most severe congenital form type 0 or early-onset type I to the more slowly progressive type IV, with classification determined by age of onset and the maximum motor milestone achieved. 4 Advancements in care standards and the emergence of gene-based therapies (GBTs) have significantly improved survival rates and functional outcomes for these patients, fundamentally changing the disease trajectory. 5 Today, the SMA phenotype is understood as a continuum, with greater emphasis placed on current functional status and treatment response. 6
Across all types, however, SMA remains a profoundly life-altering condition, with long-term implications for autonomy, participation, and quality of life. 7
While motor function has traditionally served as the principal outcome in SMA research and clinical care, this focus does not fully reflect the wideness of difficulties encountered in daily life. 8
Activities of daily living (ADLs) are classically conceptualized along a continuum that spans from basic ADLs (BADLs), fundamental self-care actions such as toileting, feeding, and dressing, to instrumental ADLs (IADLs), the more cognitively and socially complex activities that sustain independent living and participation in education, work, and community life.9–12 In many cases, ADLs offer a more meaningful reflection of functional independence than traditional clinical measures. 10 These activities are not only critical for maintaining autonomy but also for supporting psychosocial well-being and caregiver relationships.13–15 As SMA care evolves, there is increasing recognition that capturing limitations in ADLs is essential to understanding patients’ real-world functioning and informing truly patient-centered care.16,17
Despite the relevance of ADLs, the existing literature remains fragmented in its approach to their assessment. Studies vary widely in terms of which ADLs are evaluated, how they are defined, and the tools used to capture them. 15 In many cases, outcome measures have focused heavily on mobility-related milestones, with less consistent attention paid to upper limb function, self-care, or tasks requiring fine motor coordination.8,18 Yet, qualitative reports consistently highlight that individuals with SMA, particularly those with types II and III, often struggle with seemingly simple actions like preparing food or independently using the bathroom, which have profound implications for daily autonomy.19,20
This inconsistency in how ADLs are conceptualized and measured has become even more relevant in light of recent therapeutic advances. 4 The advent of disease-modifying treatments such as nusinersen, risdiplam, and gene transfer therapy has significantly altered the clinical trajectory of SMA, allowing many individuals, particularly those diagnosed with type I, to attain functional milestones that were previously considered unattainable.5,21,22
As patients live longer and with improved motor capacity, their functional needs and priorities have evolved.16,17 Although this transformation is not the primary object of the present study, it provides a critical backdrop: any attempt to understand ADL limitations in SMA must now consider the shifting clinical profile of this population and the new challenges posed by an extended functional lifespan.
To date, no structured synthesis has systematically examined which ADLs are most frequently reported across the SMA literature. Understanding these patterns is essential for improving assessment practices, guiding therapeutic focus, and ensuring that rehabilitation efforts align with what truly matters in patients’ lives. 7 The aim of this scoping review is therefore to explore and map the existing evidence on ADLs in SMA, with an emphasis on the most commonly reported activity limitations. In doing so, this work seeks to clarify which domains have received attention, where gaps remain, and how future research can better support individuals with SMA in their pursuit of meaningful independence. Moreover, based on the findings, the review aims to offer preliminary clinical suggestions and examples of good practice to help healthcare professionals address the most frequently encountered ADL challenges in this population.
Methods
Study design
Given the breadth and exploratory nature of the objective of this study, a scoping review methodology was deemed appropriate. This approach is consistent with the Joanna Briggs Institute (JBI) methodology for scoping reviews, as outlined in their official reviewer's manual. 23 The review process adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist 24 to ensure transparency and methodological rigor. A pre-registered protocol was not developed for this review, as it is not mandatory for scoping reviews. Further methodological details are available upon request from the corresponding author.
Inclusion and exclusion criteria
Eligible studies for this review were those involving participants diagnosed with SMA of any type (I, II, III, or IV) and reporting functional impairments in at least one ADL domain. Included studies adopted qualitative, quantitative, or mixed-methods designs that directly assessed ADL limitations. Studies were excluded if they focused solely on biomechanical, genetic, or neurophysiological outcomes without linking them to functional performance in ADLs. Articles were also excluded if they reported on interventions without evaluating their impact on ADL function, or if they were review articles, conference abstracts, or editorials. Only peer-reviewed articles published in English were considered for inclusion.
Search strategy
A comprehensive literature search was conducted across four major databases: PubMed, Scopus, Web of Science, and Embase. The search string combined keywords and MeSH terms related to spinal muscular atrophy and functional outcomes, including “Spinal Muscular Atrophy,” “Activities of Daily Living,” “Self-care,” “Mobility,” and “Functional Independence.” No restrictions were applied regarding SMA type or patient age group. Additional studies were identified by manually screening the reference lists of included articles and relevant systematic reviews. The search included all studies published up to December 2024.
Study screening and selection
The article selection process was managed using Rayyan, a web-based tool designed to support systematic and scoping reviews. Rayyan automatically removed duplicate records and enabled blinded, independent screening of titles and abstracts by multiple reviewers. 25
Following the initial database search, titles and abstracts were screened independently by two reviewers to assess potential eligibility. Studies deemed relevant underwent full-text review to determine whether they met all predefined inclusion criteria. Discrepancies were resolved through discussion, with Rayyan's blind review feature facilitating independent evaluation prior to consensus. When necessary, a third reviewer was consulted to adjudicate disagreements. Only studies meeting all inclusion criteria were retained for final analysis.
Data extraction and synthesis
A structured data extraction form was developed to systematically chart relevant information from each included study. Extracted variables included author and year, country of origin, study type, SMA subtype(s), sample size, participant age range, assessment tools used, method of ADL evaluation, and the specific ADL domains reported. Descriptive analysis was performed to identify and quantify the most frequently reported ADL sub-domains across studies. Because fewer than half of the included studies explicitly labelled tasks as basic or instrumental, and several outcome measures intermingle items from both categories, we analysed each ADL task exactly as reported rather than re-classifying them into BADL/IADL groups. This task-level approach minimised subjective misclassification and preserved clinical granularity across the life-span. For studies with qualitative designs, illustrative participant quotes related to activities of daily living were also extracted. These quotes were reviewed only after the descriptive synthesis of ADL domains was completed and were not used to derive or influence the main findings. Instead, selected quotes were included in the Discussion to contextualize and exemplify the synthesized results.
Development of the multidisciplinary management framework
Following the synthesis of extracted data, the identified ADL limitations were reviewed and discussed by a multidisciplinary rehabilitation team from Pediatric Neurorehabilitation Hospital in Brindisi (Italy). All reported limitations and their corresponding domains from the 16 included studies were independently collated by two authors (M.R., G.G.); any discrepancies were adjudicated by a third author (A.T.). The frequency with which each limitation occurred across the evidence base was also documented. A multidisciplinary panel, comprising a child-neuropsychiatrist, physiatrist, physiotherapist, occupational therapist, speech-language pathologist, and psychologist, subsequently examined the consolidated list. Each clinician proposed practical, evidence-informed strategies for intervention and implementation within his or her scope of practice. Through iterative discussion, overlapping proposals were harmonised, producing a final set of interventions that were linked to the professional disciplines primarily responsible for their application in routine rehabilitation settings.
Results
Study selection and flow
A total of 16 studies were included in this scoping review.13,14,19,20,26–37 Table 1 provides a comprehensive overview of the included studies.
Scoping review data extraction table: ADL in SMA patients.
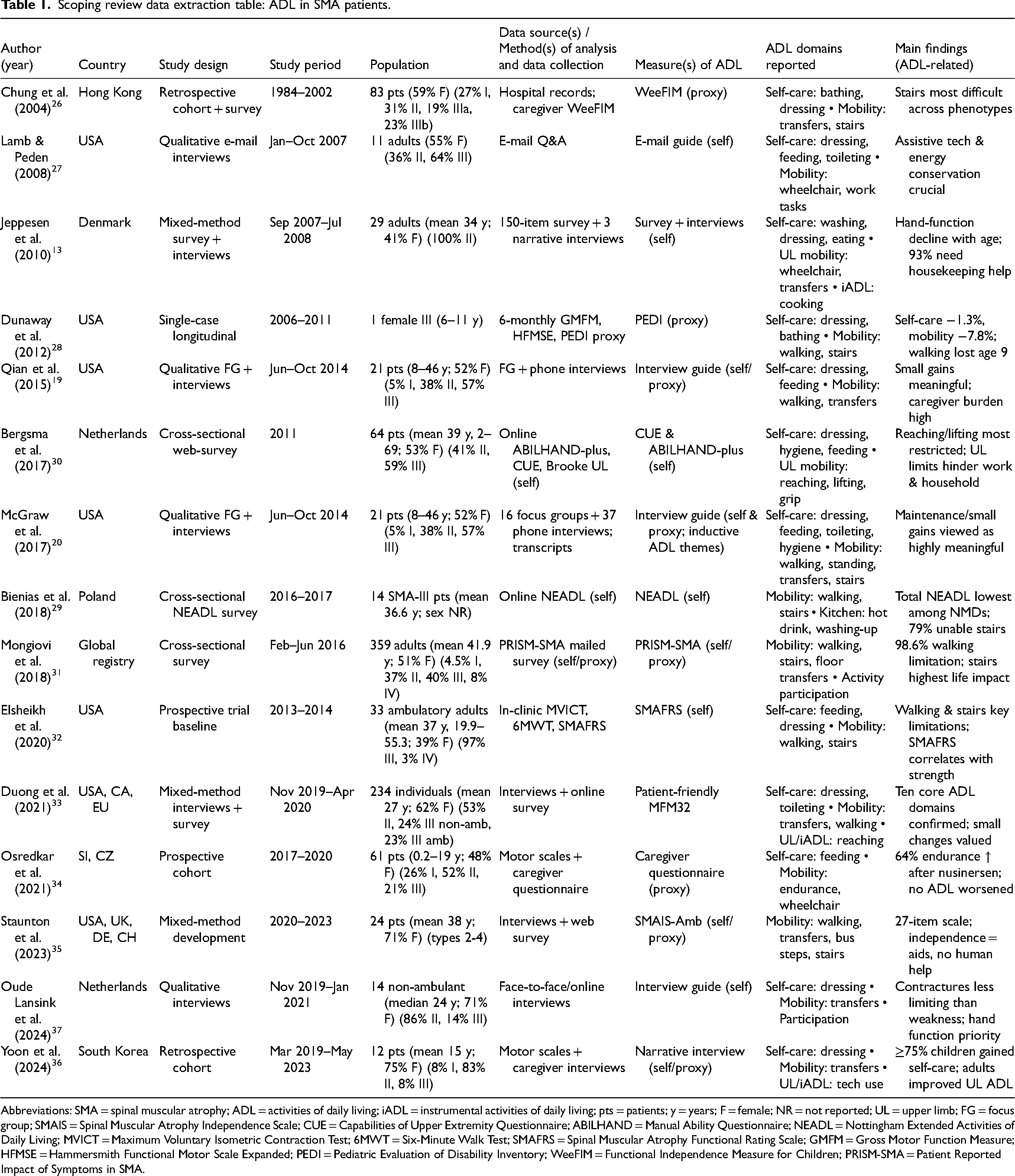
Abbreviations: SMA = spinal muscular atrophy; ADL = activities of daily living; iADL = instrumental activities of daily living; pts = patients; y = years; F = female; NR = not reported; UL = upper limb; FG = focus group; SMAIS = Spinal Muscular Atrophy Independence Scale; CUE = Capabilities of Upper Extremity Questionnaire; ABILHAND = Manual Ability Questionnaire; NEADL = Nottingham Extended Activities of Daily Living; MVICT = Maximum Voluntary Isometric Contraction Test; 6MWT = Six-Minute Walk Test; SMAFRS = Spinal Muscular Atrophy Functional Rating Scale; GMFM = Gross Motor Function Measure; HFMSE = Hammersmith Functional Motor Scale Expanded; PEDI = Pediatric Evaluation of Disability Inventory; WeeFIM = Functional Independence Measure for Children; PRISM-SMA = Patient Reported Impact of Symptoms in SMA.
Characteristics of included studies
The included publication comprised cross-sectional surveys, qualitative interviews, mixed-method approaches, observational studies, and longitudinal case series. Populations ranged across all major SMA types (I–IV), with participants including infants, children, adolescents, and adults. The total sample represented a broad spectrum of disease severity and functional status.
Most of the studies focused on individuals with SMA types II and III, although several also included patients with type I and, to a lesser extent, types IIIb and IV. Sample sizes ranged from single-case longitudinal reports to large-scale surveys involving over 300 participants. Both ambulant and non-ambulant individuals were represented. A range of assessment tools was employed, including patient-reported outcome measures (e.g., PRISM-SMA), clinician-rated scales (e.g., WeeFIM, SMAFRS, MFM32), and thematic analyses derived from interviews or focus groups.
The most frequently reported self-care ADLs included dressing, toileting, bathing, eating, and personal hygiene (e.g., brushing teeth, washing face). Mobility-related challenges were commonly reported in walking, transferring, climbing stairs, and wheelchair use. Several studies also identified limitations in upper limb function, impacting tasks such as writing, reaching, feeding, and using technology. Instrumental ADLs, including kitchen-related activities, work or school participation, and communication, were less frequently reported but emerged in selected studies, particularly among adolescents and adults.
Reported ADL limitations
Figure 1 illustrates the frequency with which each ADL sub-domain was reported across the included studies. Across the 16 included studies, the most frequently cited limitations were general mobility (13 studies), dressing (10), toileting (6), and walking (5). Less commonly reported were other self-care tasks (e.g., eating, personal-hygiene items such as brushing teeth or washing face) and upper-limb or instrumental activities (e.g., writing, technology use, kitchen tasks), each appearing in ≤ 2 studies.
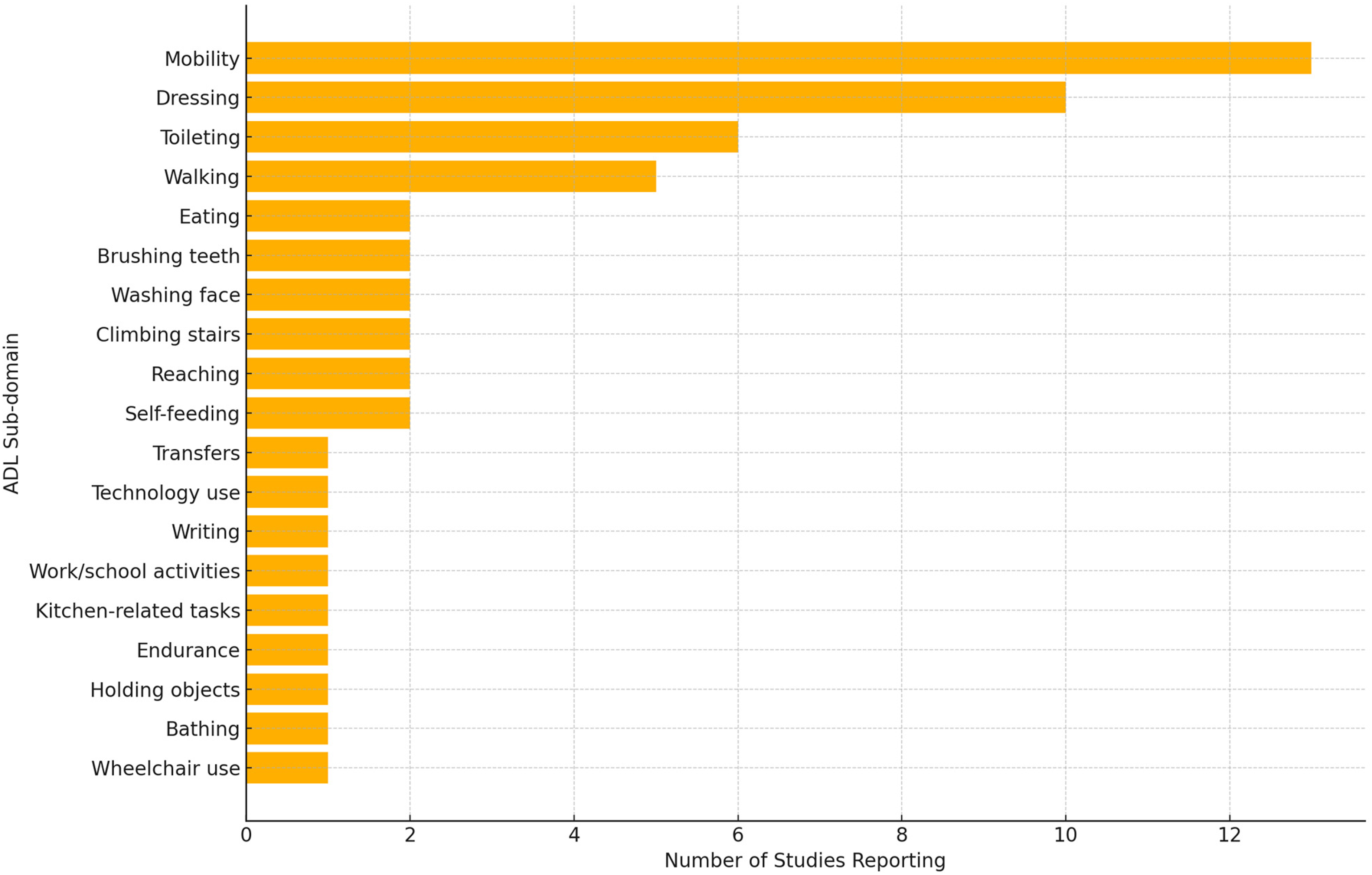
Frequency of specific ADL sub-domains reported in the included studies.
Multidisciplinary management framework
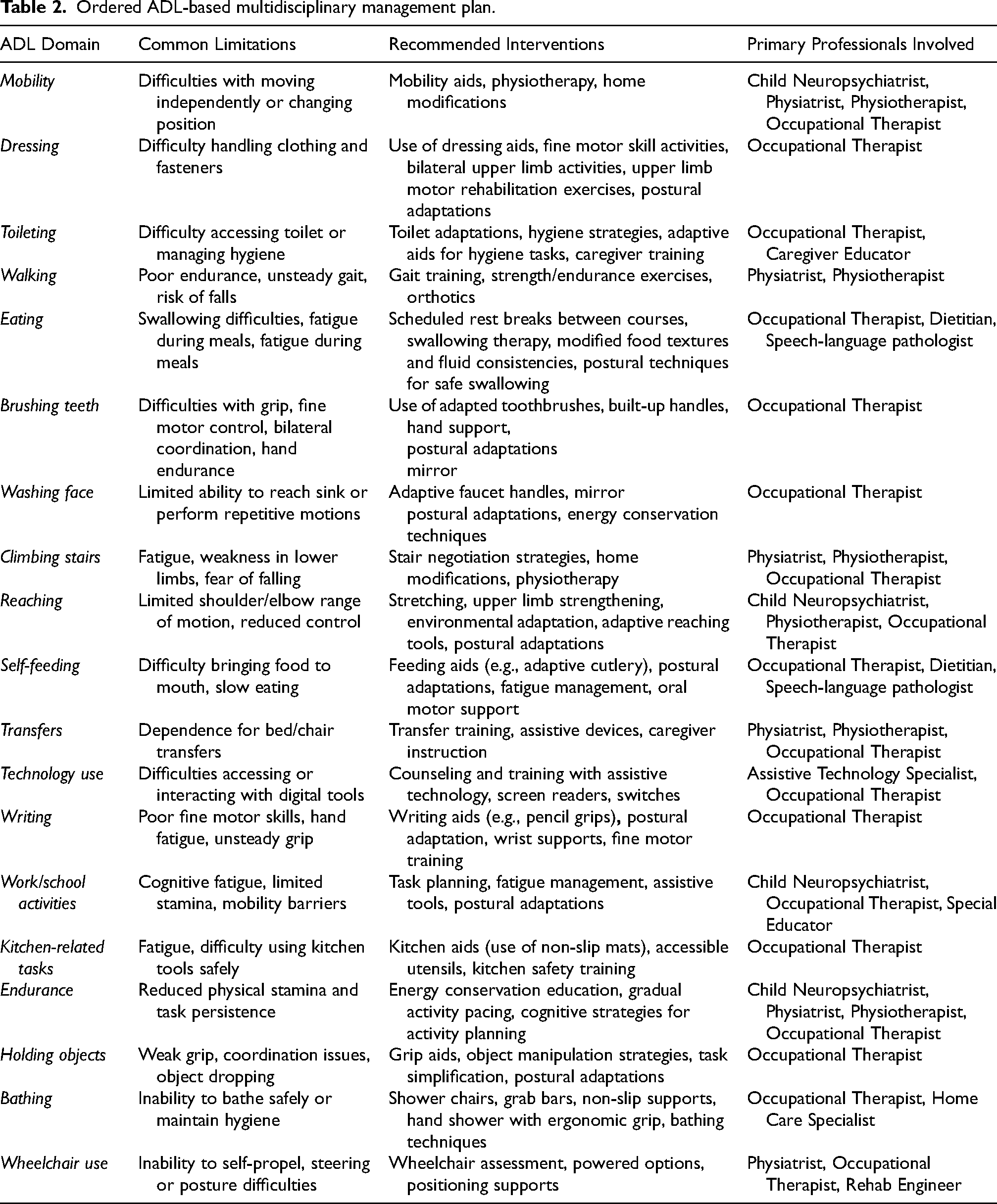
In addition to the extraction of reported ADL limitations, a structured synthesis of corresponding clinical management strategies was developed and is presented in Table 2. This table outlines a multidisciplinary management framework organized by ADL domain, identifying common functional limitations, recommended interventions, and the primary professionals involved in addressing each domain.
Ordered ADL-based multidisciplinary management plan.
Discussion
This scoping review provides a comprehensive synthesis of the impact of SMA on ADLs, revealing both expected and underappreciated functional limitations. Mobility impairments emerged as the most commonly reported ADL limitation, aligning with the well-documented progressive motor decline in SMA. However, our findings also emphasized that self-care tasks, particularly dressing and toileting, were significantly affected, yet they receive scant attention in the most recent international care standards.2,5 This highlights the need for a broader, more patient-centered approach to ADL assessment and intervention.
Reflecting the natural course of SMA, mobility-related limitations such as walking, climbing stairs, transferring, and wheelchair use were among the most frequently cited ADL impairments. Cross-sectional analyses demonstrated that nearly all individuals with SMA reported mobility restrictions, with 98.6% of respondents in the PRISM-SMA study 31 indicating mobility impairments as a major barrier to independence.
However, beyond mobility, self-care tasks, particularly dressing and toileting,13,14,19,20,26,27,30,33,34,36,37 also emerged as highly burdensome ADLs, yet they appeared less studied and underrepresented in current SMA rehabilitation guidelines and multidisciplinary care pathways.
Several qualitative studies highlighted that dressing difficulties were among the most commonly reported ADL limitations,13,19,20 often requiring full assistance in severe cases. Dressing challenges stem from upper limb weakness, muscular contractures, postural instability, and fatigue, further exacerbating daily dependence on caregivers. 37
Similarly, toileting difficulties have been widely noted,14,28,33 yet few studies systematically evaluated adaptive strategies or functional outcomes related to toileting independence.
The broader psychosocial impact of this dependence was reflected in a caregiver's account from the study by Qian et al. (2015), 19 where a patient's mother stated, “He's very dependent on me, and it's driving me crazy… He won’t let his father or anybody else take him to the bathroom or change him or feed him or anything. That drives me crazy personally because I never get a break.” The lack of autonomy in toileting and dressing could deeply affect not only the individual's quality of life but also the caregiver's emotional well-being and overall family dynamics.
Consistently incorporating self-care tasks into standardized assessments may offer clinicians deeper insight into the everyday challenges faced by patients and caregivers, helping to uncover needs that are often overlooked in mobility-focused evaluations. 38
The extent of ADL limitations varied by SMA phenotype.
In SMA type I, where profound motor impairment was present from infancy, mobility and self-care functions were almost entirely dependent on caregiver assistance. 34 In contrast, individuals with SMA type II and III experienced a more gradual decline in function, with self-care ADLs progressively deteriorating due to the natural course of motor neuron degeneration and muscle atrophy. 39 As muscle weakness advances, even tasks requiring minimal strength, such as dressing and toileting, could become increasingly challenging. 27 Notably, one of the included studies 28 documented a case of complete mobility loss, illustrating the predictable trajectory of neuromuscular decline in the pre-gene therapy era. Over a 54-month follow-up, the patient with SMA type III exhibited a 7.8% decline in mobility, accompanied by a more substantial 12.2% increase in caregiver assistance for self-care tasks, particularly dressing and toileting. 28 This progression underscored the typical pattern of functional deterioration in individuals with SMA, particularly among those who were untreated. 8 Proactively addressing self-care needs earlier in the disease course may offer greater benefit than waiting until substantial functional decline has occurred. 16
While much of the SMA literature focused on mobility impairments, upper limb function was comparatively underrepresented, despite its essential role in maintaining independence in daily activities. 18 This gap was echoed in the study by McGraw et al. (2017), 20 where a participant with SMA type II reflected, “Even if it doesn't do anything with my legs, even just my arms, because I can't really open doors or reach very far across the table, or lift normal things. My arms get tired easily, so if it could improve my arm strength that would be good… Like if I'm writing or typing or even just holding something,” underscoring the profound role that upper limb strength plays in maintaining autonomy in daily tasks.
Several studies30,33 indicated that tasks requiring fine motor control, such as writing, using technology, and grasping objects, presented significant challenges, yet they were rarely the primary focus of intervention studies. Notably, individuals with SMA type II and III who retained some ambulatory function relied heavily on upper limb function for independence, making these findings particularly relevant.20,30,37 Likewise, household-related ADLs, such as cooking and cleaning, have been scarcely reported in adults with SMA. 30 Historically, this could be partially attributed to the fact that a proportion of individuals with SMA types I, II, and III did not survive into adulthood due to disease-related complications. 4 Even among those who reached adulthood, many had severe functional limitations that precluded engagement in more complex ADLs, such as household tasks, which require a greater degree of motor independence. As a result, these activities have been underrepresented in both clinical research and functional assessments, with greater emphasis placed on more fundamental self-care and mobility tasks.
Studies using validated outcome measures such as the WeeFIM 26 and SMA Functional Rating Scale (SMAFRS) 32 confirmed that these limitations were widespread across all SMA subtypes, reinforcing the impact of functional impairments beyond mobility alone. 40 These assessment tools provided valuable clinical insights into how SMA affected daily functioning, yet they were historically applied with a greater focus on gross motor function rather than a comprehensive evaluation of broader ADLs. 33
Reflecting recent advancements in SMA care, the findings of our scoping review suggested a shift in research focus, with more recent studies placing greater emphasis on an expanded range of ADLs. While earlier studies predominantly emphasized mobility and basic self-care,29,31,32 post-gene therapy research expanded its scope to include upper limb function, household tasks, and social participation, reflecting the evolving needs and abilities of SMA patients.35–37 This highlighted the importance of continuously updating functional assessments and rehabilitation strategies to ensure they remained aligned with the evolving clinical presentation of SMA in the era of advanced treatments. 16
However, despite this expansion in research focus, the methodological heterogeneity of the included studies presented a challenge in synthesizing ADL findings. Several studies relied on patient-reported outcomes,31,33 whereas others employed clinician-administered functional scales.32,33 While these tools provided valuable insights, their differences in scope and structure complicated direct comparisons across studies. Furthermore, longitudinal data on ADL progression remained scarce, with the majority of studies adopted cross-sectional designs that offered only static snapshots of functional impairments13,29–32. Only a few studies, such as Osredkar et al. (2021) 34 and Yoon et al. (2024), 36 included multi-year follow-up assessments that tracked ADL changes over time, which limited the ability to understand how functional abilities evolved with disease progression and how emerging therapeutic interventions impacted real-world ADL performance.
Additionally, existing assessments did not fully capture the patient's lived experience. Several qualitative studies19,20 indicated that patients prioritized different ADLs compared to those typically measured in clinical trials. For instance, caregivers of predominantly non-ambulant children and adolescents with SMA types II and III in Pera et al. (2017), 14 small functional improvements in daily tasks (e.g., independently dressing or using utensils) were considered more meaningful than broader motor-function gains. This discrepancy underscored the need for more comprehensive, patient-centered ADL assessments.
Despite growing evidence of social participation limitations in SMA, few studies have investigated structured interventions aimed at improving accessibility in work, education, and psychosocial well-being.13,31 .These limitations were vividly illustrated in the words of a young adult with SMA, who shared, “I actually went to a festival over the weekend and I needed to use a handicapped bathroom, and the only handicapped accessible bathrooms in the whole entire place were for VIP… They couldn’t get it through their heads that they need a handicap accessible bathroom for everyone,” further adding, “Even my friends will be like do you want to come to this party… and I’m like, I already went out today, I’m too tired.”. 19
The findings of this review suggest that rehabilitation efforts in SMA should extend beyond mobility interventions to include targeted support for self-care and fine motor ADLs. Although mobility aids such as wheelchairs and orthoses are routinely prescribed, interventions targeting self-care tasks, particularly dressing, toileting, and household activities, remain limited. Given the central role of upper limb function in maintaining independence, especially in individuals with SMA types II and III, rehabilitation programs should prioritize strategies that support autonomy in daily life, including adaptive dressing techniques, assistive feeding tools, and toileting supports. 37
There is growing recognition of the need for a broader, multidisciplinary approach to address the complex challenges faced by individuals with SMA. 41 A coordinated model involving physiotherapy, occupational therapy, speech therapy, and psychological support can help improve functional independence, emotional well-being, social participation, and overall quality of life. 17
Multidisciplinary care plays a central role in supporting patients across education, employment, and daily living. 7 Occupational therapy can improve accessibility in school and work environments through tailored interventions. 5 Speech therapy may assist individuals with bulbar involvement in maintaining effective communication. 6 Psychological support, including psychotherapy and counselling, is essential for managing the emotional burden of chronic disability and promoting social integration. 42 Assistive technologies such as communication devices, ergonomic workspaces, and upper limb supports can further facilitate participation in professional and community life. 33
Study limitation
This scoping review should be interpreted with caution. Consistent with JBI and PRISMA-ScR guidance, we did not undertake a formal risk-of-bias appraisal; therefore, the certainty of individual findings cannot be judged. The evidence base was heterogeneous (spanning qualitative, quantitative, and mixed-methods designs, different SMA phenotypes and age groups, and diverse outcome instruments) which precluded meaningful quantitative synthesis or direct effect-size comparisons. Because fewer than half of the primary studies explicitly distinguished basic from instrumental ADLs and many measurement tools conflated the two, we analysed each task exactly as reported, thus preserving detailed, practice-relevant information while forgoing the conventional BADL/IADL classification. Most data were cross-sectional and derived from small samples, limiting insights into functional trajectories, especially in the post-gene-therapy era. Finally, restricting the search to peer-reviewed English-language articles may have excluded relevant grey or non-English literature, and the participant quotes included in the Discussion were used solely for illustration after the descriptive synthesis rather than as thematic data.
Clinical and research implications
As SMA phenotypes evolve due to therapeutic advancements, clinical strategies must extend beyond mobility-focused interventions to include targeted self-care adaptations, upper limb rehabilitation, and assistive technologies.
Clinically, early intervention for self-care ADLs should be prioritized, as functional decline affects dressing, toileting, and household tasks well before complete mobility loss. Occupational therapy can support work and school accessibility, while speech therapy may aid communication and swallowing difficulties. Psychological support remains essential in addressing the emotional burden of chronic disability, promoting self-efficacy and social integration.
From a research perspective, standardizing ADL assessment tools is critical to ensure meaningful comparisons and longitudinal tracking of functional progression. Current measures often prioritize mobility-related outcomes, neglecting fine motor function and self-care. The integration of patient-reported outcomes and real-world data collection, including wearable sensors and video-based monitoring, could provide more accurate functional assessments. 43
As SMA care continues to evolve, ongoing research must reassess how ADL improvements are measured and how rehabilitation strategies are adapted to the shifting phenotype. A multidisciplinary and technology-driven approach will be essential in ensuring effective, patient-centered interventions that enhance autonomy and quality of life.
Conclusion
This scoping review highlights that while mobility impairments remain the most reported ADL limitation in SMA, self-care tasks such as dressing and toileting are equally significant but often under-recognised. Across the 16 studies, heterogeneous taxonomies and mixed self- versus proxy-reporting made category-level synthesis impractical, so a task-by-task analysis proved more informative. These gaps call for harmonised, longitudinal, task-specific ADL measures that can capture small yet meaningful functional changes in the post-gene-therapy era. Clinically, a multidisciplinary strategy that gives the same systematic attention to self-care and fine-motor ADLs as to gross-motor mobility will be essential for translating therapeutic advances into real-world independence.
Footnotes
Authors contributions
Conceptualization, A.T., G.G. and M.R; Methodology, M.R., G.M., C.F.; Software, M.R.; Validation, G.G., M.R. and A.T.; Formal Analysis, G.G. C.F., M.C.O.; Investigation, G.G., C.F., M.C.O.; Resources, M.R.; Data Curation, M.R.; Writing – Original Draft Preparation, G.G. and M.R.; Writing – Review & Editing, G.G., G.M. and M.R.; Visualization, A.T.; Supervision, A.T.; Project Administration, A.T.; Funding Acquisition, A.T.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by fund from European Union–Next Generation EU– NRRP M6C2 - Investment 2.1 Enhancement and strengthening of biomedical research within the National Health Service (NHS) - PNRR-MR1–2022–12376937 (to GG, MR, and AT).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be available on request to the corresponding author.
Human and animal rights
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.