
Abstract
We described ambulatory Duchenne muscular dystrophy (DMD) progression, across multiple functional measures, via previously established prognostic groups for loss of ambulation (LoA) and health states. Patients closer to vs. farther from LoA had greater declines in some measures (e.g., 6-min walk distance) and less change in others (e.g., timed rise from floor velocity) due to floor effects. Patients in the late vs. early ambulatory health state were concordantly shifted towards higher LoA risk. Findings further characterize health states and prognostic factors in ambulatory DMD and highlight the importance of multiple measures of function to fully characterize disease progression.
Background
Approximately one in 3600–6000 live male births is affected by Duchenne muscular dystrophy (DMD), an X-linked, degenerative neuromuscular disease. 1 As DMD progresses, patients experience motor function declines that eventually result in loss of ambulation (LoA). 2 Rates of DMD progression vary across individuals, 3 with LoA typically occurring at ages 10–16.4–6 While variable across patients, times to LoA can be well-predicted based on a patient's current functional profile. In particular, based on a patient's performance on the timed rise from floor (RFF) and timed 10-meter walk/run (10MWR), they can be placed in one of five prognostic groups with subsequent times to LoA ranging from a median of 1 year to > 5 years. 7
To better characterize DMD progression, Project HERCULES (Health Research Collaboration United in Leading Evidence Synthesis) has developed a model of DMD disease progression across eight health states (two ambulatory, one transfer, and five non-ambulatory states) based on input from clinicians, patients, and caregivers. 8 DMD patient ages, steroid treatment use, and functional profiles were characterized by health states in the Project HERCULES model by Muntoni and colleagues, 9 who concluded that the health states provide a detailed characterization of disease progression in DMD, with functional performance worsening with each successive health state.
The present study further characterizes ambulatory health states in DMD, considering the five validated prognostic groups described by McDonald et al. 7 and two ambulatory health states in the adapted Project HERCULES model of Muntoni et al. 9 Patients are characterized by motor function trajectories, cross-classification of the LoA prognostic groups and the HERCULES health states, and by time to an important pre-cursor milestone to LoA.
Methods
Data sources
Patient data were drawn from nine sources: placebo arms of drisapersen phase 3 trial DEMAND III (NCT01254019) and phase 2 trials (NCT01153932, NCT01462292), ataluren phase 3 trial PTC020 (NCT01826487), and tadalafil DMD phase 3 trial (NCT01865084) (provided by CureDuchenne, PTC Therapeutics, and Lilly, respectively); real-world data from Universitaire Ziekenhuizen Leuven (provided by the Leuven Neuromuscular Reference Center in Leuven, Belgium); and natural history data (ImagingDMD [NCT01484678], iMDEX [NCT02780492], and PRO-DMD-01 [NCT01753804]; the latter also provided by CureDuchenne).
Data sources were approved by the respective ethics committees of the original studies. This study analyzed previously collected, de-identified data.
Patient prognostic categories for LoA and ambulatory health states
Patients were categorized into the following five prognostic groups using a previously validated prognostic model for LoA based on timed RFF and 10MWR, from the furthest to the closest to losing ambulation: group 1 (RFF < 4 s, any 10MWR), group 2 (RFF = 4–7 s, any 10MWR), group 3 (RFF = 7–20 s, 10MWR < 10 s), group 4 (RFF = 7–20 s, 10MWR ≥ 10 s; or RFF ≥ 20 s, 10MWR < 10 s), and group 5 (RFF ≥ 20 s, 10MWR ≥ 10 s). 7
Patients were required to have non-missing RFF and 10MWR at baseline. Additionally, patients must have an early ambulatory or late ambulatory health state, as defined by the adapted Project HERCULES model based on ability to RFF and walk 10 m described in Muntoni et al., (i.e., early ambulatory: North Star Ambulatory Assessment [NSAA] RFF item [item #11] > 0 and walk item [item #2] > 0; late ambulatory: NSAA item #11 = 0 and item #2 > 0). 9 The NSAA includes 17 items important in the lives of patients with DMD, each scored as 0 (cannot do), 1 (can do with modification), or 2 (can do independently), with the total score ranging 0–34. 10 As reported by Muntoni et al., for the early and late ambulatory states from which our sample was drawn, steroid use (deflazacort or prednisone) was documented at over 90% of patient visits, suggesting relatively uniform adherence to current standards of care.9,11
A patient's first visit with non-missing information for RFF, 10MWR, and NSAA item performance was used as the index date (baseline). Follow-up was censored at the last assessment.
Outcomes and analyses
The main objective of this descriptive study is to characterize the motor function trajectories observed within the early and late ambulatory health states in the adapted Project HERCULES model of Muntoni et al. 9 To that end, patient characteristics were summarized at baseline overall, by prognostic group for LoA risk, and by ambulatory health state. Motor function trajectories (i.e., median changes from baseline during follow-up) for the total NSAA score, 6-min walking distance (6MWD; meter), RFF velocity (rises/second, multiplied by 10 for readability), and 4-stair climb (4SC) velocity (stairs/second) were characterized by prognostic group and visualized using spaghetti plots and plotted median trajectories at the patient level. The use of medians offers more meaningful insights than means, which can be disproportionately influenced by outliers, common in DMD due to variability in disease progression. Proportions of patients unable to RFF based on the NSAA item were calculated at baseline and two years post-baseline by prognostic group. Last observation carried forward was implemented for a maximum lookback period of 6 months to handle irregular visit schedules in the real-world data sources; as this study spanned several years, a 6-month lookback period is expected to have minimal impact on the study conclusion. The distribution of LoA prognostic categories was described by health state. Finally, time to approaching LoA (aLoA), defined as the first assessment with 10MWR > 10 s, which has been associated with LoA within the next 2 years (median time from aLoA to LoA ∼1 year),12–16 was evaluated using Kaplan–Meier analyses stratified by health state.
Results
Motor function trajectories of ambulatory patients by prognostic group for LoA
Of 1031 ambulatory patients with DMD, mean ± standard deviation (SD) age at baseline was 7.9 ± 2.5 years. All patients were male and 83.6% were white. Mean baseline NSAA total score was 23.0 ± 6.6. Patients were distributed across prognostic groups, with 31%, 38%, 22%, 6%, and 3% in groups ordered from the longest (group 1) to the shortest (group 5) predicted time to LoA. Patients in prognostic groups with longer predicted times to LoA were on average younger with better NSAA total scores and longer 6MWD at baseline (Supplementary Table S1).
Figure 1 illustrates the diverse disease trajectories of the five prognostic groups. During follow-up, median NSAA total score in group 1 remained constant for the first two years post-baseline and then dropped by approximately 2 points/year, while the score for other groups tended to drop from the first year. 6MWD dropped by less than 100 m from baseline over 6 years for groups 1 and 2, whereas in groups 3–5, 6MWD dropped over 100 m in the first 3 years. Over time, RFF velocities decreased substantially from baseline in group 1 and to lesser degrees in groups 2 and 3, whereas 4SC velocity decreased for most groups with the greatest decrease observed in group 1. For RFF and 4SC velocities, groups 3–5 showed limited movement shortly after the baseline due to a floor effect.
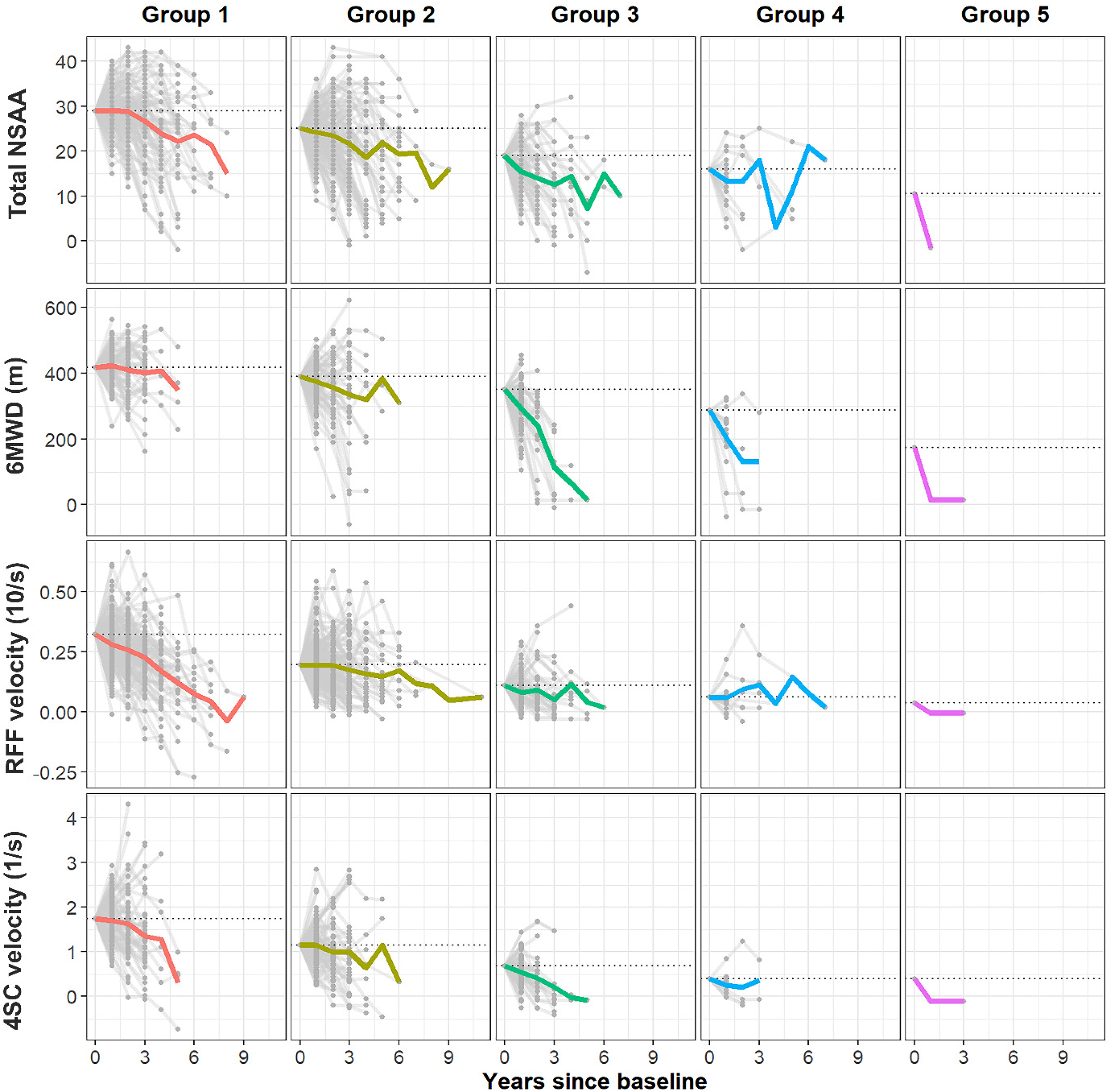
Patient-specific trajectories of change from baseline, anchored to start at the median value at baseline per group, across prognostic groups for ambulatory patientsa
The proportions of patients unable to RFF across prognostic groups from the longest (group 1) to shortest (group 5) predicted time to LoA increased from baseline levels of 0.6% (2/320), 1.5% (6/389), 14.5% (33/228), 55.4% (36/65), and 82.8% (24/29), respectively, to 5.6% (8/143), 18.3% (28/153), 61.3% (38/62), 63.6% (7/11), and 100.0% (1/1), respectively, at two years post-baseline.
LoA characteristics of early vs. late ambulatory patients
Among the 930 early ambulatory and 101 late ambulatory patients, mean ± SD age was 7.7 ± 2.4 and 10.2 ± 2.5 years, respectively, and 85.8% and 71.6% were white. Mean total NSAA score at baseline was 24.0 ± 6.0 and 14.1 ± 5.0, respectively (Supplementary Table S1).
In the early ambulatory health state, most patients (> 70%) were in prognostic groups with longer predicted times to LoA (34.2% in group 1, 41.2% in group 2). In contrast, in the late ambulatory health state, most patients (60%) were in groups with shorter predicted times to LoA (35.6% in group 4, 23.8% in group 5) (Figure 2(a)). Among patients with 10MWR ≤ 10 s at baseline (event-free patients at baseline), those in the early ambulatory health state had a median of 5.8 years to aLoA, whereas those in the late ambulatory health state had a median of 1.5 years to aLoA (Figure 2(b)).
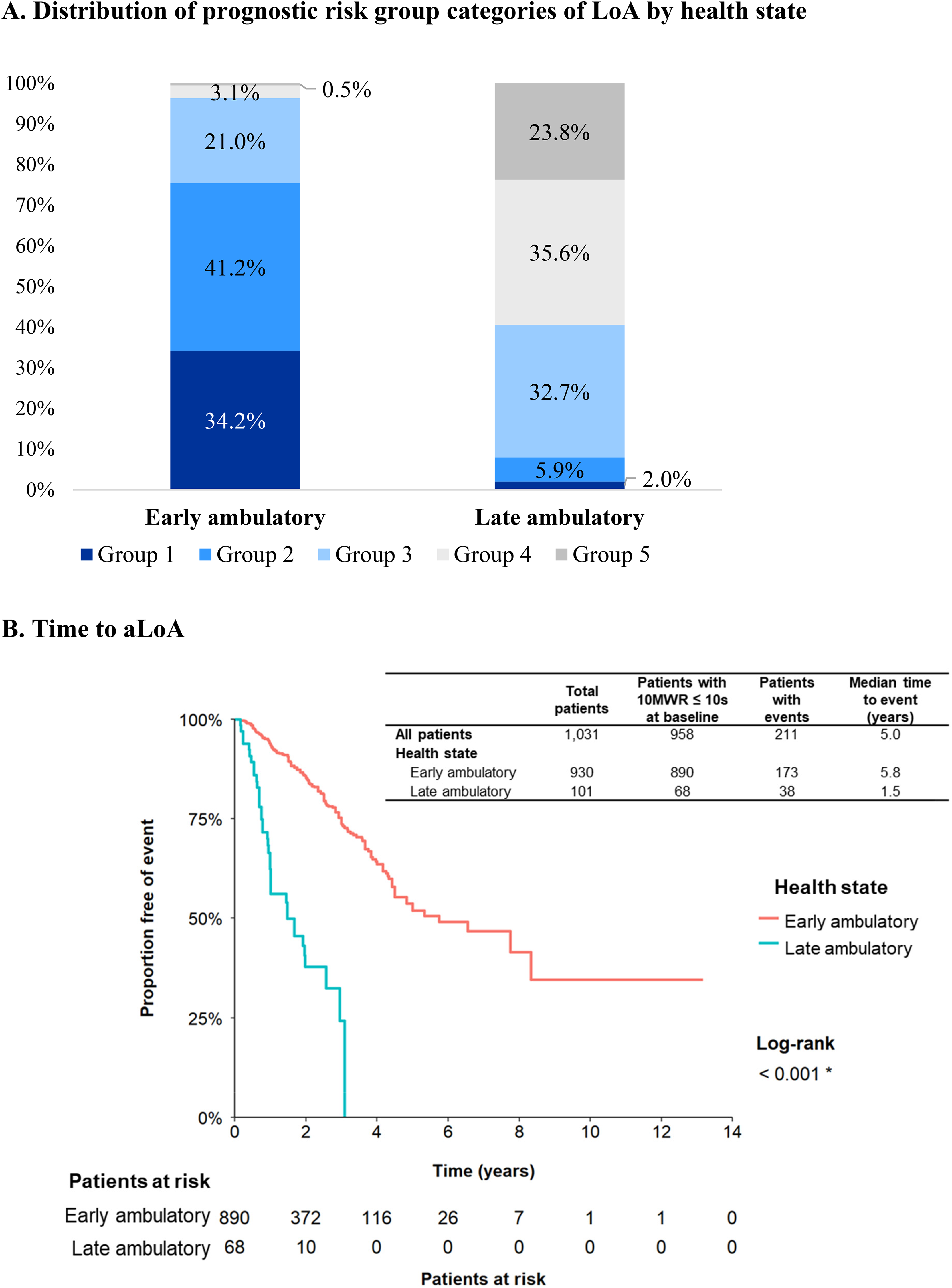
Prognostic categories for risk of LoA and time to aLoA by early vs. late ambulatory health statea,b. (a) Distribution of prognostic risk group categories of LoA by health state. (b) Time to aLoA.
Discussion
Ambulatory patients with DMD experience heterogeneous trajectories of motor function. However, these trajectories were predictable with categorization of patients into prognostic groups and health states. Across prognostic groups, different measures of motor function showed different patterns of change over time. Some measures declined faster for patients closer to LoA (e.g., 6MWD) whereas others hit a floor and were less sensitive to change approaching LoA (e.g., for many patients RFF velocity = 0 soon after baseline). This study estimated a 4-year longer median time to aLoA among early vs. late ambulatory patients.
Study limitations include the tendency of missing data for motor function assessments as patients approach poor function and LoA, which may lead to over-estimates of average function among recorded assessments. In addition, this study was exploratory in nature and was limited to the characterization of ambulatory health states in DMD, gross motor function trajectories, and times to aLoA. The relationship between other non-ambulatory health states and trajectories of upper limb motor function/pulmonary function was beyond the scope of these analyses. The relatively low number of patients in groups 4 and 5 may have impacted the findings. Lastly, the findings may not be generalizable to all races/ethnicities.
This study shows that previously validated prognostic groups and health states in ambulatory DMD can identify meaningful and concordant differences in motor function trajectories, helping to characterize the clinical meaning of these groupings. The need for multiple measures of motor function to fully characterize patient experiences of progression throughout the ambulatory phase is also highlighted.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251364694 - Supplemental material for Descriptive characterization of ambulatory health states in Duchenne muscular dystrophy: Motor function trajectories and times to loss of ambulation
Supplemental material, sj-docx-1-jnd-10.1177_22143602251364694 for Descriptive characterization of ambulatory health states in Duchenne muscular dystrophy: Motor function trajectories and times to loss of ambulation by Francesco Muntoni, James Signorovitch, Michaela Johnson, Andres Gomez-Lievano, Nate Posner, Patricia Dorling, Katherine Beaverson, Jose Alvir, Matthias Mahn, Susan J Ward, Nathalie Goemans, Krista Vandenborne, Eugenio Mercuri and Craig M McDonald in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
The authors are grateful to the patients for participating in the clinical assessments and for agreeing to make their data available for research. The authors would like to thank investigators and research staff from all the data sources used in this study. Finally, the authors thank Catherine Fernan, Adina Zhang, Chujun He, Eden Ma, and Flora Chik, who provided medical writing assistance and figure/table preparation as employees of Analysis Group, Inc., and was funded by Pfizer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Pfizer as part of the Collaborative Trajectory Analysis Project (cTAP) collaboration. The cTAP is a precompetitive coalition of academic clinicians, drug developers, and patient foundations formed in 2015 to overcome the challenges of high variation in clinical trials in DMD. cTAP has received sponsorship from Astellas (Mitobridge), Avidity Biosciences, BioMarin Pharmaceutical, Bristol Meyers Squibb, Catabasis, Daiichi Sankyo, Edgewise Therapeutics, Entrada Therapeutics, FibroGen, Italfarmaco SpA, Marathon Pharmaceuticals, NS Pharma, Pfizer, PTC Therapeutics, Roche, Sarepta Therapeutics, Shire, Solid Biosciences, Summit Therapeutics, Ultragenyx, Vertex Pharmaceuticals, Parent Project Muscular Dystrophy, Charley's Fund, and CureDuchenne, a founding patient advocacy partner and provider of initial seed funding to cTAP.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Francesco Muntoni was a member of the Rare Disease Scientific Advisory Group for Pfizer and of Dyne Therapeutics SAB and has participated in SAB meetings for PTC, Sarepta, Pfizer, Roche, Santhera, and Wave Therapeutics. UCL and Great Ormond Street Hospital have received funding from Pfizer, Italfarmaco, Wave, Santhera, Roche, NF Pharma, ReveraGen, Genethon, and Sarepta regarding clinical trials.
James Signorovitch cofounded the cTAP and is an employee of Analysis Group, Inc., which was a paid consultant to Pfizer in connection with the development of this manuscript.
Michaela Johnson and Andres Gomez-Lievano are employees of Analysis Group, Inc., which was a paid consultant to Pfizer in connection with the development of this manuscript.
Nate Posner is an employee of Pfizer Inc and owns stock/stock options.
Patricia Dorling, Katherine Beaverson, Jose Alvir, and Matthias Mahn were employees of Pfizer Inc. at the time the study was conducted.
Susan J. Ward cofounded and manages cTAP and has received funding from the membership of cTAP to facilitate this study.
Nathalie Goemans is an Editorial Board Member of this journal, but was not involved in the peer-review process nor had access to any information regarding its peer-review. In addition, Nathalie Goemans has received compensation for consultancy services from Eli Lilly, Italfarmaco, PTC Therapeutics, BioMarin Pharmaceutical, Pfizer, Avidity, Daiichi Sankyo, Wave, and Santhera and has served as site investigator for GlaxoSmithKline, Prosensa, BioMarin Pharmaceutical, Italfarmaco, Eli Lilly, Wave, and Sarepta.
Krista Vandenborne has received grants from NIH National Institute of Arthritis and Musculoskeletal and Skin Diseases/National Institute of Neurologic Disorders and Stroke, Parent Project Muscular Dystrophy, and the Muscular Dystrophy Association. She has also received funding from ltalfarmaco SpA, Sarepta Therapeutics, Summit Therapeutics plc, Catabasis Pharmaceuticals, Pfizer Inc, ldera Pharmaceuticals, Bristol-Myers Squibb, and Eli Lilly through grant awards to the University of Florida.
Eugenio Mercuri has served on clinical steering committees and/or as a consultant for Eli Lilly, Italfarmaco, PTC Therapeutics, Sarepta, Santhera, and Pfizer; has served as PI for GlaxoSmithKline, Prosensa, BioMarin Pharmaceutical, Italfarmaco, Roche, PTC, Pfizer, Sarepta, Santhera, Wave, NS Pharma, and Eli Lilly.
Craig M. McDonald has served as a consultant for DMD clinical trials for Astellas, Capricor Therapeutics, Catabasis Pharmaceuticals, Catalyst Pharmacuticals, Edgewise Therapeutics, Epirium Bio (formerly Cardero Therapeutics), FibroGen, Italfarmaco, Pfizer, PTC Therapeutics, Santhera Pharmaceuticals, Sarepta Therapeutics, and Solid Biosciences; and has received research support for clinical trials from Capricor Therapeutics, Catabasis, Catalyst Pharmaceuticals, Edgewise Therapeutics, Italfarmaco, Pfizer, PTC Therapeutics, Santhera Pharmaceuticals, Sarepta Therapeutics, and Solid Biosciences; he reports grants from the US Department of Education/National Institute on Disability and Rehabilitation Research, National Institute on Disability, Independent Living, and Rehabilitation Research, US NIH/National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH/National Institute of Neurologic Disorders and Stroke, US Department of Defense, and Parent Project Muscular Dystrophy US.
Data availability statement
All relevant aggregate data supporting the findings of this study are reported within the article and its supplementary materials. Restrictions apply to the availability of the underlying de-identified patient-level data. Data are available through requests made directly to individual institutions, subject to their requirements for data access.
Previous presentations
Part of the material in this manuscript was presented as poster presentation at the 7th Treat-NMD International Conference in Vancouver, Canada, in December 2022.
Supplemental material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.