
Abstract
Background:
Hypokalemic Periodic Paralysis (HypoPP) is a rare genetic neuromuscular disorder characterized by attacks of skeletal muscle weakness or paralysis with spontaneous recovery. The attacks are frequently triggered by specific factors, and previous studies have identified certain associated lifestyle factors, such as dietary intake and physical activity. However, there is currently no in-dept knowledge on how patients experience and self-manage triggering factors in their everyday life.
Objective:
In this study, we aimed to explore patients’ experiences with dietary intake and physical activity through semi-structured interviews. The research question was: Which strategies do individuals with HypoPP utilize in relation to dietary intake and physical activity to prevent or self-manage attacks of muscle weakness and paralysis?
Methods:
The study included 14 participants aged 21–58 years with HypoPP due to abnormalities in calcium channel function caused by pathogenic variants in the CACNA1S gene. The interviews were transcribed and analysed using Malterud's systematic text condensation.
Results:
The participants experienced that regular meals with controlled portions of complex carbohydrates, limited intake of simple carbohydrates, engaging in regular mild to moderate exercise combined with warm-up and cool-down, and avoiding physical inactivity made them less vulnerable to attacks of muscle weakness and paralysis. Furthermore, participants highlighted the cumulative effect of triggers, by consistently reporting feeling more susceptible to attacks when exposed to multiple triggers simultaneously.
Conclusions:
The participants experienced self-management through dietary modifications and adjustments in physical activity to reduce symptoms in CACNA1S-related HypoPP. A novel finding was the experienced cumulative effect of lifestyle-related triggering factors.
Keywords
Introduction
Primary hypokalemic periodic paralysis (HypoPP) is a rare genetic neuromuscular disorder with an estimated prevalence of 1:100.000. 1 Most individuals with HypoPP inherit the disorder in an autosomal dominant manner, although sporadic cases do occur. 1 The disorder is caused by pathogenic variants in the CACNA1S gene, which leads to abnormalities in calcium channel function, or by pathogenic variants in the SCN4A gene, affecting sodium channel function.2,3 These ion channels are expressed in skeletal muscles. 4 The phenotypes are heterogenous, including periodic paralysis without permanent muscle weakness, periodic paralysis with permanent muscle weakness, and permanent muscle weakness without a history of periodic paralysis. 5
In affected individuals, symptom onset typically occurs during the first or second decade of life, with patients experiencing periodic episodes of localized or widespread muscle weakness, lasting from minutes to hours, accompanied by hypokalemia and with spontaneous recovery. 1 The neuromuscular involvement is furthermore described to be progressive with development of permanent weaknesses, 6 with muscles along the spine, muscles in the hip and thigh, and calf muscles, being the most severely affected. 5 A recent study suggests that HypoPP significantly impairs quality of life, with progressive permanent muscle weakness and fatigue, especially with age, being more burdensome than attacks of muscle weakness and paralysis. 7
The attacks of muscle weakness and paralysis are frequently triggered by specific factors, and previous studies have identified lifestyle behaviors, as dietary intake and exercise, to be associated with the periodic muscle weaknesses in HypoPP.3,8 Carbohydrate-rich meals, hard physical activity, and rest following exercise are the most commonly reported lifestyle-related trigger factors.9,10 Other factors include cold environment and stress, 8 high intake of sodium, 11 dehydration and alcohol consumption, 10 and overeating 12 or eating irregular meals. 13 However, these factors have only been studied to a limited extent, and no previous studies have assessed and described the dietary factors or level of intensity and duration of physical activity in any detail. 9 Thus, evidence-based lifestyle recommendations for people with HypoPP are currently lacking.
To gain a deeper understanding of how lifestyle factors influence periodic muscle weakness and paralysis in HypoPP, we aimed to explore patients’ experience with dietary intake and physical activity. The research question was: Which strategies do individuals with HypoPP utilize in relation to their dietary intake and physical activity to prevent or manage attacks of muscle weakness and paralysis?
Methods
Recruitment
This study was approved by the Norwegian Regional Ethics Committee for Medical Research Ethics South-East reference number 222511, and the Data Protection Officer at Frambu Resource Centre for Rare Disorders. Information about the study was disseminated through the website and social media channels of Frambu Resource Centre for Rare Disorders. In addition, a personal invitation was sent to all individuals registered with HypoPP in the Norwegian Registry for Hereditary and Congenital Neuromuscular Diseases who were not already recruited in the study (n = 12). Inclusion criteria were 16–70 years of age and genetically verified HypoPP. A patient representative, recruited in collaboration with the Neuromuscular Disorders Association of Norway, participated in the conception and design of the qualitative study.
Collection of data
To explore the participants’ experiences, a semi-structured interview guide was developed. The interviews were performed digitally using Norsk Helsenett, a national provider of secure e-health solutions, and recorded with an Olympus Digital Voice recorder (VN-541PC). Each interview lasted between 45 to 90 min and was conducted from November 2022 to April 2023. The first author performed all the interviews. Before the interview, the participants were asked questions by the interviewer about their current use of medication, history of attacks, and if they had permanent muscle weakness. In addition, they were reminded about the main theme of the interview and their legal rights.
Initially, the participants were asked open questions about their experience with dietary factors and physical activity as triggers of attacks of muscle weakness or paralysis. To explore this in more detail, participants were asked specifically about their experience with all factors previously described in the literature as trigger factors. 9 The same approach, using open questions followed by more specific inquiries, was employed to explore the participants’ experience with factors that contribute to aborting or ameliorating an emerging attack, as well as strategies applied in their everyday lives to prevent attacks of muscle weakness and paralysis.
Data analysis
Audio recordings of the interviews were transcribed using f4transcript software. 14 Analysis was performed using systematic text condensation (STC). 15 This qualitative descriptive method involves four analytical steps: 1) Reading all transcribed interviews to gain a total impression, 2) Identifying and extracting meaning units, 3) Abstracting the contents of these units, and 4) Synthesizing descriptions and concepts into a cohesive whole. 15 First, the transcribed interviews were read in full to get an overall perspective of the material, noting preliminary themes relevant to the research questions, consciously setting aside preconceptions. In the second step, the interviews were read more in-depth, with meaning units being coded and transferred into a matrix in Microsoft Word with their respective quotations. The third step involved condensing and abstracting the most relevant meaning units and their sub-groups of quotes in relation to the research questions. In the final step, an analytical text was created by synthesizing the selected meaning units and quotations, supporting, and exemplifying the identified themes. The original transcripts were revisited to ensure the quotes remained true to their original context or meaning.
Results
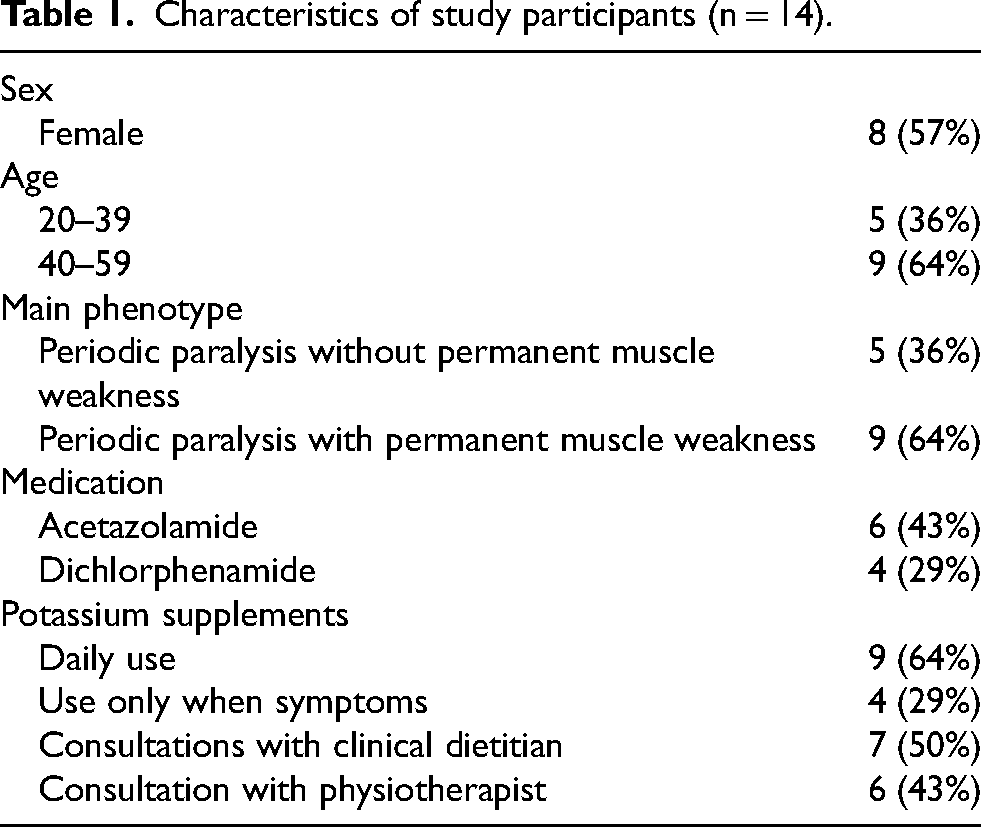
In total 14 people signed the informed consent form and participated in the study. All the participants were of Norwegian ethnicity and had pathogenic variants in the calcium channel gene: NM_000069.3 (CACNA1S) c.1583G > A (p.Arg528His) (n = 6), and NM_000069.3 (CACNA1S) c.3716G > A (p.Arg1239His) (n = 8). Further information on characteristics of study participants is listed in Table 1.
Characteristics of study participants (n = 14).
Maintaining a regular meal pattern with controlled portions of complex carbohydrates while limiting the intake of simple carbohydrates
All participants described that self-management through dietary modifications was an integral approach to prevent attacks of muscle weakness or paralysis, and some participants also described managing acute attacks through dietary modifications. A significant intake of foods rich in simple and refined carbohydrates, along with salt and irregular meal patterns, were described as dietary-related triggers. The likelihood of these dietary factors triggering an attack of muscle weakness or paralysis depended on several factors. In addition, variability was described in how strict the participants adhered to these dietary modifications in their everyday lives. Some also emphasized the difficulty of staying motivated and adhering to dietary restrictions, especially when there is no evidence regarding the long-term outcomes of the disorder, such as on the development of permanent muscle weakness.
Proportional link between simple carbohydrates and attacks
Foods rich in sugars and simple carbohydrates such as pastries, cakes, candy, chocolate, potato crisps, pommes frites, pizza, sweet and sour sauce, sugary drinks (juice, soda, lemonade and sweet alcoholic drinks), white bread, pasta, and rice were all described as potential triggers of attacks. The overall tolerability of simple carbohydrates varied among the participants. Nevertheless, all described a proportional correlation, and most participants made efforts to moderate their intake. Carbohydrates are a trigger, simple carbohydrates. The worst are pastries, sweet pastries are the worst. (…) I have always tolerated potatoes, but pasta, before there were whole grain variants of pasta, it was a super trigger. Not to mention pizza! (…) Candy for example, I cannot eat candy. Well, I can eat candy, but then I will pay for it. Participant no. 6 My triggers are pizza, pasta, white flour, and pastries, typical foods that contain simple carbohydrates with white flour. (…) I eat pasta once or twice a week, and I have rice to most of my meals, so I am not categorically dismissive against foods with simple carbohydrates, but I try to moderate my intake of it, I do. Participant no. 8
In addition to the food source, the total amount of simple carbohydrates consumed and the order in which foods were consumed within a meal were also perceived as determining factors. If simple carbohydrates were consumed first in a meal, overall tolerability decreased compared to when they were consumed towards the end of the meal. It absolutely depends on the amount, so if I binge on pizza and eat a whole pizza, things end badly. Participant no. 5 After work, I went to the store, was starving to death, so I bought candy. While I was making dinner, I ate the candy, and I became weak during dinner because things were done in the wrong order. I ate a lot of sugar before I ate food. Participant no. 4
Benefits of regular meals with unprocessed foods and complex carbohydrates
Many participants incorporated complex carbohydrates, such as potatoes and wholegrain varieties of bread, pasta, and rice, into their regular diet. Eating wholegrains, as opposed to refined grains, and choosing sugar-free or sugar-reduced alternatives over sugary drinks were perceived as key habits that were less likely to induce attacks of weakness and paralysis. Several participants also noted that a diet rich in wholegrains, vegetables, and legumes not only provided essential nutrients but also contributed to overall well-being, increased resilience to triggers, and prevented attacks. Likewise, meals that included a wide variety of nutritious and minimally processed foods, cooked from scratch, were experienced to mitigate the impact of dietary triggers. Yes, it is foremost food that I don’t tolerate, the food that contains simple carbohydrates such as pasta or buns or candy and such things. So, then I must eat whole grain variants of them. That is what I stick to. Participant no. 7 In terms of diet, I try to eat meat, fish, and vegetables, varied healthy foods, and preferably whole foods like clean meat and fish, less ground meat or mixed ready-made products, and of course eat fruit. Participant no. 11
Meal frequency and portion sizes were important, with some participants adhering to three to four meals daily consumed roughly at the same time points (e.g breakfast, lunch, dinner and evening meal), while others found a somewhat more flexible meal timing beneficial if portion sizes were controlled. Some identified skipping meals as a significant trigger, and one participant avoided going more than five hours without food. Another participant experienced morning muscle paralysis due to inadequate food intake the previous day. This emphasizes the critical role of regular, adequate nutritional intake in managing symptoms. I have experienced that it can be worse if I have not eaten earlier in the day. If I have skipped breakfast and lunch for example, then I come home and eat a big dinner. It can almost not get any worse. So, if I am good at eating “healthy”, little and often, that works the best. That is when I can keep myself best in shape to say it like that. But it is very tempting to eat something tasty occasionally, and a lot. Participant no. 14 One of my problems when starting in a new job is that I have not been good at eating. So eating irregularly absolutely has an effect. (…) I had an evening shift, but I ate when I came home and had previously not eaten much. (…) Then I was going to my day shift the day after and I woke up being a bit paralyzed in my muscles. Participant no. 12
The complex role of added salt and potassium-rich foods
In terms of added salt being a potential trigger, some participants indicated that a combination of high salt content and simple carbohydrates was necessary to trigger an attack, whereas one participant found that foods with a high salt content alone was sufficient. Additionally, another believed that consuming salty foods like chips or popcorn, along with a potassium supplement, could positively contribute to ameliorate an attack. This suggests that salt plays a complex role in both triggering and potentially managing muscle weakness and paralysis, with large individual variability. The absolute trigger is salt. (…) Many years ago, I was invited to my parent's place to eat salted cod or something. I ate it and went straight to training afterwards, which was not a good idea. I developed a severe attack. Another time when I was at Sunday dinner at my parents’, they served reindeer meat and broth. I should not have eaten that. I had a strong reaction to it. So very salty foods or salt combined with white flour is a bad combination. Participant no. 2 Yes, salt can trigger. Chips and things like that. Participant no. 15 I feel that I can become better, if I feel that I am becoming weak, then I can take some potassium supplements and eat some chips. I do not know why though. I normally try to avoid salty foods because it is a trigger for this disease really, but sometimes I believe that chips or popcorn helps a bit really. Participant no. 1
Potassium-rich foods were commonly consumed among participants. While bananas were universally acknowledged by multiple participants as a beneficial source of potassium, coconut water and milk were also recognized for their high potassium content and effectiveness in liquid form. These foods were a deliberate choice to consume to prevent or manage symptoms, particularly if potassium supplements were unavailable during an emerging attack. Since I did not have the tablets that work very slowly, and since I was already feeling so unwell, I needed something in liquid form because we believe that works much better. So I bought one of those large packs of coconut water and drank it throughout the entire car journey. Participant no. 10
Being physical active, exercising regularly and avoiding physical inactivity
All the participants confirmed that hard exercise and rest immediately after exercise could act as a trigger of muscle weakness and paralytic attacks. The informants described various strategies to manage physical activity related symptoms to counter this. These strategies included insight on how to adjust activities and intensity to prevent exercise-related symptoms and incorporating light physical activity as a preventive measure. Many participants acquired this knowledge by trial and error. Those who had overcome the initial obstacles related to exercise and engaged in an active lifestyle noted positive effects on muscle strength, well-being, and a bolstered bodily resilience to triggers. Participants not engaging in an active lifestyle gave insight into constraints in management of symptoms related to physical activity.
Gradually increased strength and tolerance for exercise
Regular exercise was reported to contribute to preventing attacks of muscle weakness and paralysis, and bolster bodily resilience to triggers, as well as providing opportunities for increased muscle strength and endurance. However, the informants initially experienced exercise as a trigger of symptoms. Unfamiliar or new activities were possible triggers of symptoms, regardless of their intensity. Furthermore, lack of energy in the first few days after exercise was described. This was experienced as a barrier to continuing the exercise, but if continued regularly, symptoms became less frequent over the first 2–3 weeks. Several informants described the importance of tolerating a certain level of pain and discomfort in this phase. To ameliorate the symptoms, the informants emphasized the importance of starting easy with low intensity and gradually increasing the duration and intensity. With time and patience, building resilience towards high-intensity exercise was possible. Some described an individually tailored exercise program developed by a physiotherapist as beneficial to build muscle strength. We have always thought that exercise triggers the disease, and it did in the beginning, but when I got over a certain stage, I became a lot better because of the exercise. Participant no. 1 Now I exercise about four times, at least four times a week. Of course, I also have rest days, because it is very important, and I know that the muscles need it. And, I have noticed that it helps a lot because at the beginning I felt that it was so unfamiliar for the muscles, so then I was in a way very ill after exercise, but now I almost do not feel anything after exercising, so it is nice to notice the difference. Participant no. 10 I started exercising last year to maintain muscle strength and I clearly notice that I have become stronger. Therefore, that is fun. Participant no. 6
Warm-up and cool down prevent attacks
Regardless of their overall tolerance level for activity, beginning and ending an exercise session with a warm-up and cool-down activity, respectively for 5 and 15 min, such as cycling, walking, stretching or light household chores were experienced beneficial to ensure a successful exercise session and preventing subsequent symptoms. I never exercise and suddenly just stop and sit down. (…) I always do a cool down exercise at the end such as walking on a treadmill. Yes, I always stretch properly before I end my exercise, and I never sit down when I come home after exercising. Preferably, I go in the shower and keep myself moving by making myself an evening meal or something, then I sit down. Participant no. 2
Regular exercise and avoiding inactivity bolster bodily resilience
Several participants reported significant improvements in their condition by adopting a more active lifestyle. They noted that regular exercise allowed them to occasionally consume foods, such as those high in simple carbohydrates and salt, which previously triggered episodes of muscle weakness or paralysis, or required medication to prevent attacks. This was experienced as a significant improvement from their earlier condition, which many attributed to regular exercise enhancing their body's resilience and reducing their dependence on medication or potassium supplements. By improving my diet and exercising regularly, I can now occasionally allow myself to go out and eat a burger with fries without getting unwell. (…) It used to be a major trigger, but now I can actually do that. It must be because I generally have a better diet and am more active overall. When I was not, my body tolerated much less. Participant no. 2 Then I was able to reduce my use of potassium supplementation, I almost did not use it at all. I managed with two Kaleorid (750 mg Potassium-Chloride) and one Diamox, and I hardly ever experienced weakness. I had the best time when I was in pretty good physical shape, I probably still experienced weakness during the nights, but it was far from as strong and as often. Participant no. 15
Conversely, some participants elaborated on the challenge of maintaining regular exercise. They noted that lapses in routine led to increased weakness, heightened vulnerability to triggers, and a greater reliance on medication and potassium supplements. Cessation of activity for 1–3 weeks could typically lead to a setback. Such periods without exercise increased the vulnerability to symptoms when resuming the exercise. This illustrated the importance of maintaining a certain continuity in exercise and avoiding daily inactivity to prevent attacks from occurring, for instance by incorporating physical activity into daily routines. This included strategies such as changing positions while sitting or lying down, standing up to walk around regularly, engaging in light activity in their homes or exercising several times a week. Sedentary behavior was particularly highlighted as a challenge among participants who had office jobs involving extended periods of sitting down. I also believe staying in shape is important. I sort of notice that if it's been a long time since I've been in regular exercise, there's a barrier you must overcome, a small hurdle, and that hurdle is that you feel bad after you have exercised. You must get past that first step. Participant no. 8 Too little physical activity is a trigger for me. Meaning, if I am too passive for a longer period, I feel that my body becomes weak and tolerates less. Participant no. 12 The disease has never bothered me as much as it does now. (…) These days, I do not exercise, I weigh a lot more than I used to, I eat much less healthy and take less care of myself. That's just how life is sometimes. It has its ups and downs. Now, I rely much more on medication and am completely dependent on potassium supplements. However, for my part, I know in many ways what works to help me feel better, even if I will never be completely well. Participant no. 15
The cumulative effect of triggers
Combined triggers heightened the risk of muscle weakness and paralytic attacks. Participants consistently reported feeling more susceptible to attacks when exposed to multiple triggers simultaneously. For instance, while cold ambient temperatures or a meal containing refined carbohydrates might not trigger an attack on their own, these trigger factors, when combined with inactivity, or physical exertion, substantially increased the likelihood of an attack. This finding emphasizes that the cumulative effect of triggers makes participants more sensitive and vulnerable, thereby playing a critical role in the onset of muscle weakness or paralysis. Now that the weather is cold, I feel, in general, weakened. Especially when I've been sitting for a long time or have little movement, or things like that. Participant no. 3 If I eat pizza and chips and a lot of that in a day and then just lie still on the sofa, it's guaranteed that I'm going to get an attack. Participant no. 10 If I sleep in a cold room, I become ill. Therefore, I must have it warm (20 degrees Celsius) when I sleep. Participant no. 7
To mitigate the risk, participants actively sought to control and stabilize trigger factors in their daily lives, reducing the likelihood of developing weakness or paralysis. Specifically, changes from warm to cold temperatures consistently exacerbated symptoms, making thermal management crucial for the participants. Seasonal variations influenced symptom management, with warmer weather allowing greater dietary flexibility and tolerance for physical exertion. During cold seasons, some participants used warm clothing, baths, showers, and saunas to maintain warmth and muscle relaxation to increase threshold for symptom onset. I tolerate a lot less during the winter, and there are things that I can do in the summer, that I cannot do in the winter, (…) just looking at the time it takes me to hike up a mountain, not just because it is slippery in the winter, but I move slower, I tolerate less during the winter than in the summer. Participant no. 4 Yes, for me it is the cold weather or weather changes. So, it does not need to be the coldness, but during the day in the summer, yes, it is like I almost don’t have the disease at all. Participant no. 5
Discussion
The participants’ narratives highlight the critical role of dietary modifications and consistent physical activity and exercise in the self-management of attacks of muscle weakness and paralysis in HypoPP. Key self-management strategies included maintaining a regular meal pattern with controlled portions of complex carbohydrates while limiting the intake of simple carbohydrates, engaging in regular mild to moderate exercise combined with warm-up and cool-down, and avoiding physical inactivity. However, the impact of potassium- and salt-rich foods remains uncertain, suggesting a nuanced and potentially individualized interaction between these nutrients and symptom management that warrants further investigation. Furthermore, participants highlighted the cumulative effect of triggers, elucidating the complexity of actively managing and regulating these lifestyle factors in daily lives.
Maintaining a regular meal pattern with controlled portions of complex carbohydrates while limiting the intake of simple carbohydrates
Participants in this qualitative interview study frequently reported simple carbohydrates as a trigger of muscle weakness and paralytic attacks, consistent with findings in previous literature. 9 Since there is a proportional link between simple carbohydrates and attacks, patients must be careful with starchy foods and foods with a lot of sugar. There are various strategies for this, but the main finding suggests that it might not be necessary for all patients with CACNA1S-related HypoPP to avoid carbohydrates and follow a low-carbohydrate diet. Several participants in this study describe that it is sufficient to choose complex carbohydrates and unprocessed foods that take longer to digest and therefore give a more gradual rise in blood sugar levels and consequently insulin response. 16 This illustrates that it may not only be the amount of carbohydrates that matters but possible also the type of carbohydrate consumed and the preparation method used.
A regular meal pattern also appears to be an important strategy to avoid excessive amounts of carbohydrate at one time, to maintain stable blood sugar levels and consequently prevent periodic muscle weakness or paralysis. These findings align with current understanding of dietary strategies that mitigate insulin spikes and maintain glucose stability. 17
The participants had varying perceptions and attitudes about the importance and role of potassium-rich foods in preventing and treating symptoms. These conflicting responses may be explained by the fact that many participants regularly take potassium supplements, containing significantly higher levels of potassium compared to the amount found naturally in foods and therefore potentially overshadow any effect of potassium-rich foods. Additionally, understanding this topic requires nutrition literacy beyond the typical level found in the general population. Different experiences regarding salt-rich foods show that this may be an area of individual variation. However, we cannot rule out the possibility that some may have misunderstood the importance of salt in foods with a high amount of both salt and starch, e.g., pommes frites. More studies are therefore needed in this area to clarify the role of salt and potassium-rich foods in symptom management.
Participants expressed a need for structured, evidence-based guidance to navigate dietary management effectively. Balancing dietary restrictions with the enjoyment of food remains a challenge, emphasizing the importance of a holistic approach that addresses both attacks of muscle weakness and paralysis, and overall quality of life. While half had brief consultations with clinical dietitians, many found them unhelpful due to insufficient disease-specific knowledge, leading most to rely on trial and error to develop their own dietary regimens. This highlights a gap in healthcare support and the need for consistent, individualized, and disease-specific dietary counseling.
Being physical active, exercising regularly and avoiding physical inactivity
Hard exercise followed by rest is a well-documented trigger for attacks in individuals with HypoPP, as reported by participants in the current study and confirmed by prior literature. 9 This phenomenon can be attributed to significant potassium shifts during exercise and the subsequent activation of sodium-potassium ATPase pumps in skeletal muscles post-exercise.4,18–21 Participants in this study reported that engaging in moderate physical activity and exercise helped delay or even prevent attacks, but only after their bodies gradually increased tolerance for exercise over a period of 2–3 weeks. Furthermore, regular physical activity was reported to enhance bodily resilience against known triggers. Regardless of the participants’ overall tolerance levels for physical activity, incorporation of warm-up and cool-down activities was critical to ensure a successful exercise session and to minimize post-exercise symptoms. The principle of “Start low and go slow” is well supported in the context of physical activity for neuromuscular disorders. Research suggests that adopting a physically active lifestyle with moderate-intensity activity of sufficient duration (i.e., a physically active lifestyle) may be as effective and impactful as structured physical training in reducing disease burden and improving muscle function in neuromuscular disorders. 22 However, the findings that regular exercise may increase bodily resilience against triggers and the importance of cool-down represents novel insights not previously described in the literature. These findings underscore the importance of structured exercise programs that incorporate not only the type and intensity of exercise but also the preparation and recovery phases. It suggests that warm-up and cool-down routines may help stabilize muscle function by minimizing rapid potassium fluxes, which are known to contribute to symptom exacerbation in HypoPP.4,18,19
Participants in this study described lifelong challenges with physical activity, often rooted in difficult childhood experiences with exercise. Medical advice to engage only in mild to moderate physical activity and avoid overexertion frequently led to negative social consequences, long-term disengagement and anxiety. For those who experienced adverse physical responses to exercise in childhood, transitioning to regular activity was particularly challenging, compounded by a lack of supportive structures. While nearly half of the participants had consulted physiotherapists, many found these sessions unhelpful due to insufficient disease-specific knowledge. Consequently, most relied on trial and error to independently develop their exercise routines. Psychological barriers such as self-doubt, insecurity, and fear of causing harm persisted despite the physical benefits of regular activity, highlighting the need for more structured and supportive approaches in youth to build confidence and encourage lasting engagement with exercise.
Cumulative effects of triggers
The cumulative effect of multiple triggers emerged as a significant factor in the onset of muscle weakness and paralytic attacks in individuals with HypoPP, underscoring the complexity of managing the condition Living with HypoPP requires substantial effort to develop, adapt, and implement strategies to prevent muscle weakness and paralytic attacks and mitigate permanent weakness. Recent research highlights the impaired quality of life experienced by people with HypoPP, which worsens with age. 7 Permanent weakness and fatigue have the most significant negative impact, although paralytic and weakness attacks also are reported to pose considerable challenges to daily life. 7 These findings suggest that individuals with HypoPP could benefit from multidisciplinary care by specialists familiar with the condition, providing comprehensive support and guidance. Unfortunately, such services remain insufficiently available in many areas for rare neuromuscular disorders. 23
Strengths and limitations
A significant strength of this study was that the research group had previously conducted a systematic literature review on the topic. 9 This prior review ensured that the qualitative study was well informed and methodologically robust, addressing specific knowledge gaps identified in the existing literature. The findings from the systematic review provided a strong theoretical foundation and framework for comparing and contrasting the qualitative results, enabling a more comprehensive exploration of the research topic. Additionally, the review equipped the interviewer and research team with a clear understanding of the broader context, enhancing their ability to contextualize and interpret the qualitative findings. This integrative approach strengthened the study's rigor, validity, and credibility.
Even so, in qualitative research, a potential challenge lies in the researcher's role in the data analysis. While Malterud's STC 15 provides a transparent and structured framework, the process is inherently reliant on the researcher's interpretations, which can introduce subjectivity and influence the emphasis placed on certain themes. To address this limitation, the entire research team actively participated in the STC process, reflecting on and documenting analytical choices, and engaging in collaborative discussions of decisions and findings throughout. This approach enhanced the study's credibility and confirmability, in line with Malterud. 15 To ensure dependability and credibility further, a single researcher conducted all interviews to maintain consistency in the approach. Probing questions were used when responses were unclear or overly vague, enabling deeper exploration of participants’ experiences. Additionally, the researcher paraphrased participants’ statements during the interviews to confirm and clarify their intended meaning, thereby aligning interpretations with participants’ perspectives.
Another strength of this study is the convenience sample of participants from various regions of Norway, ensuring representation from diverse families, age groups, and a balanced gender distribution with six men and eight women. Additionally, the use of digital face-to-face interviews proved highly effective in overcoming logistical challenges associated with in-person interviews. This approach facilitated broader participation and enabled the inclusion of eligible individuals who might otherwise have been unable to take part, enhancing the study's inclusivity and geographical reach.
The study, however, recruited only individuals with pathogenic variants in the calcium channel gene, leaving uncertainty about whether individuals with HypoPP due to pathogenic variants in the sodium channel gene SCN4A have similar experiences to adjustments in dietary intake, physical activity, and exercise.
An important consideration is the heterogeneity in phenotype, medication use, and physical activity experience among participants. While this diversity can be a strength in qualitative research, capturing a wide spectrum of perspectives, it may also limit direct comparability of experiences across individuals. Additionally, the natural history of periodic paralysis, particularly the decline in attack frequency with age, 1 may further shape how participants perceive and manage their symptoms over time, whether due to disease progression or lifestyle adaptations.
As with all interview-based studies, findings rely on participants’ recall and self-reported experiences. Although qualitative research provides insights into personal experiences, it does not capture objective measures of symptom progression or management effects. Future longitudinal or interventional studies are needed to complement these findings by tracking clinical outcomes and exploring causal relationships. Despite these limitations, this study offers patient-centered insights into how individuals experience and self-manage attacks of muscle weakness or paralysis, contributing to inform future research and practice.
Conclusion
The findings suggest that patients with CACNA1S-related HypoPP perceive self-management by maintaining a regular meal pattern with controlled portions of complex carbohydrates while limiting the intake of simple carbohydrates, engaging in regular mild to moderate exercise, and avoiding a sedentary lifestyle to reduce their vulnerability to attacks. Furthermore, participants highlighted their experience with the cumulative effect of triggers, a novel finding that elucidates the complexity of proactively managing these factors in daily life.
To enhance self-management and health literacy, it is essential for patients to receive tailored, disease-specific guidance from healthcare providers including physiotherapists and clinical dietitians. While this study contributes to a growing understanding of how diet and physical activity can support HypoPP management, intervention studies with subgroup analysis are needed to assess the effectiveness of specific dietary patterns and physical exercise regimens in preventing attacks and improving long-term outcomes.
Footnotes
Acknowledgments
We express our gratitude to the Neuromuscular Disorders Association of Norway for their collaboration and for disseminating information about the study. Several of the authors are members of the ERN-NMD.
ORCID iDs
Author contributions
All authors have made substantial contributions to the following: The conception and design of the qualitative study, drafting the article or revising it critically, and final approval of the submitted version. NLW conducted and transcripted the interviews. All authors, apart from HD, contributed to the STC.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Norwegian National Advisory Unit on Rare Disorders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.