
Abstract
Introduction:
Limb-girdle muscular dystrophy (LGMD) R4, betasarcoglycanopathy, is a progressive muscle disease that frequently presents in childhood and results in loss of ambulation around 20 years of age. With interventional trials on the horizon it is essential to document functional disease progression using standardized performance outcome assessments (PerfO).
Methods:
We present a prospective longitudinal observational study of individuals recruited through both Nationwide Children's Hospital neuromuscular clinics and through outreach events held in an area with a high incidence of Founder variant (c.452C > G). PerfOs included the NorthStar Assessment for limb-girdle dystrophies (NSAD), Performance of Upper Limb (PUL), timed function tests, and spirometry, as appropriate.
Results:
Forty-six individuals enrolled (aged 3–55 years) with 22 (55%) ambulant. Most PerfOs quantified change over time. We found heterogeneity of functional abilities at all ages. In our cohort, children's performance improved until around age 7, followed by a plateau until around 10–12 years. The ability to rise from the floor was the first milestone lost and was unable to be completed by anyone who took longer than 7.7 s on the 10-meter. Further, performance on select PerfOs were related to skills of functional independence, informing clinical care and data driven trial design.
Conclusion:
There is a great deal of functional heterogeneity. The selected PerfOs measured motor function and disease progression in individuals with LGMDR4, for the benefit of both data driven clinical management and clinical trial design.
Keywords
Introduction
The limb girdle muscular dystrophies (LGMD) are a group of rare degenerative neuromuscular disorders with a heterogenous presentation of clinical features.1,2 The sarcoglycan complex (including alpha, beta, gamma, and delta-sarcoglycan) is part of the dystrophin-associated glycoprotein complex. The sarcoglycan trans-membrane glycoproteins play an important role in the structural stability of skeletal and cardiac muscle fibers and pathogenic variants to any member of the sarcoglycan complex may result in LGMD.3–7 LGMDR4 β-sarcoglycan-related, (previously LGMD2E) is a recessively inherited LGMD subtype identified by a loss of function of the β-sarcoglycan gene (SGCB) and subsequent deficiency of β-sarcoglycan protein production.2,8 LGMDR4 is characterized by muscle atrophy and weakness, with reported symptom onset at ages 5–16 years and loss of ambulation in late teens or early adulthood.9,10 Cardiac disease is most common in individuals who are no longer ambulant but should be monitored in patients of all ages.9,11,12 Previous reports of pulmonary involvement suggest it is less common, reported in around 19% of the population, especially accompanying loss of ambulation.9,12
While spontaneous variants to SGCB in individuals with no documented family history have been reported, there is a higher documented prevalence of LGMDR4 in areas such as Iran, China, Italy, and some regions of the United States of America, which have been suggested to be due to founder variants.9,13–16 One such example are the Plain population of the United States. The Plain communities are groups of individuals with a common religious foundation that live simply, dress plainly, and live in the modern world but remain separate from it. These beliefs resulted in many small endogamous communities across North America. 17 Founder variants in these communities lead to a disproportionate prevalence of many genetic conditions. The Plain Population communities with increased prevalence of LGMDR4, specifically those that carry the c.452C > G variant, have been reported as having a potentially milder phenotype, however these classifications have been largely based on patient reported age of symptom onset and age of loss of ambulation through recall of life events.9,16,18
Development of disease-modifying treatments for LGMDs are accelerating thus accentuating the need for well documented quantification of the functional manifestations of the disease. To date, prospective natural history data is limited, in part, due to do the rarity of the disease, with a reported prevalence of 0.86 × 10−6 cases making it difficult to amass a large data corpus. The aim of our study was to characterize disease progression using standardized clinical outcome assessments (COA), specifically Performance Outcomes (PerfOs), in individuals diagnosed with LGMDR4 across 3 years.
Methods
This study was designed as a prospective observational study and was approved by Nationwide Children's Hospital (NCH) Institutional Review Board, as IRB17–01086. Written informed consent was obtained by subjects and caregivers; written assent was obtained as applicable. Criteria for subject enrollment included a genetically confirmed diagnosis of LGMDR4. Subjects were excluded if there was a known concomitant disease or other pathogenic genetic variant likely to impact performance on functional assessments in the opinion of the investigator.
Subjects were recruited as a sample of convenience either at regularly scheduled visits with the NCH Neuromuscular/Muscular Dystrophy Association clinics, or through community outreach visits to a Plain community with a founder variant (c.452C > G). Individuals recruited through NCH neuromuscular clinics received follow-up functional assessments during their regularly scheduled clinic visits. Those recruited and followed in the Plain community, completed testing locally with physical therapists bringing the appropriate equipment to conduct standardized testing within their community setting. Up to four visits were completed over 3 years. These were both samples of convenience, therefore not all subjects received the same number of visits.
Functional outcome assessments
The expert physical therapists completing the assessments regularly participate in rigorous training and reliability programs required for multisite clinical trials, and several serve as the gold-standard MasterPhysio trainers in international multisite sponsored trials. Subjects completed a battery of testing appropriate to their current ability at each visit. All subjects completed the Performance of Upper Limb v2.0 (PUL) and 9 Hole Peg Test (9HPT), however, the 9HPT was discontinued after the first year as it did not differentiate between ability levels.19,20 Ambulatory individuals completed the North Star Assessment for limb girdle-type muscular dystrophies (NSAD) which includes timed function tests (10 meter walk/run [10m] and time to rise from floor [TTR]), and 100 meter timed test (100m).21–24 Although the NSAD includes items for non-ambulatory subjects, this assessment was not often collected at community-based testing as transferring non-ambulant individuals on a portable exam table was not considered safe. In addition to raw performance in seconds on the 100m, for individuals under the age of 15 years, a comparison to the average time for their age and size value was calculated using a previously published regression equation. 24
Respiratory function
The respiratory function of all subjects able to understand and perform the maneuvers was collected using the Microlab 3500 spirometer, and performed according to the American Thoracic Society criteria modified for neuromuscular disease. Sitting forced vital capacity (FVC) measurements were taken and prediction values were calculated using the Global Lung Function Initiative (GLI) normative reference dataset. 25 Subjects completed a minimum of three FVC attempts and the best effort was used for analysis.
Statistical analysis
Statistical analysis was completed with IBM SPSS Statistics version 29.0.1.0. Demographic and baseline functional data are presented as a single cohort, as well as divided into subjects with the c.452C > G variant and those with other variants. All summary group statistics are presented as median and interquartile range (IQR). A between-group comparison of age at baseline was analyzed using the Mann-Whitney U test. Spearman correlation coefficient is used to present the relationship between performance on PerFOs and other covariates. Linear regression was used to evaluate the impact of age on baseline motor performance. Longitudinal performance is analyzed using Wilcoxon signed rank-sum test and are presented as change in performance from baseline for each follow-up timepoint.
Results
Demographics
Forty-six individuals (54% male) with an average age of 20.2 years (IQR 11.7, 31.4; range 3.0–54.8 years) were enrolled between January 2016 and February 2020 (Table 1).
Demographics at the baseline visit; presented as a full cohort, by variant type, sex, and by ambulatory status.
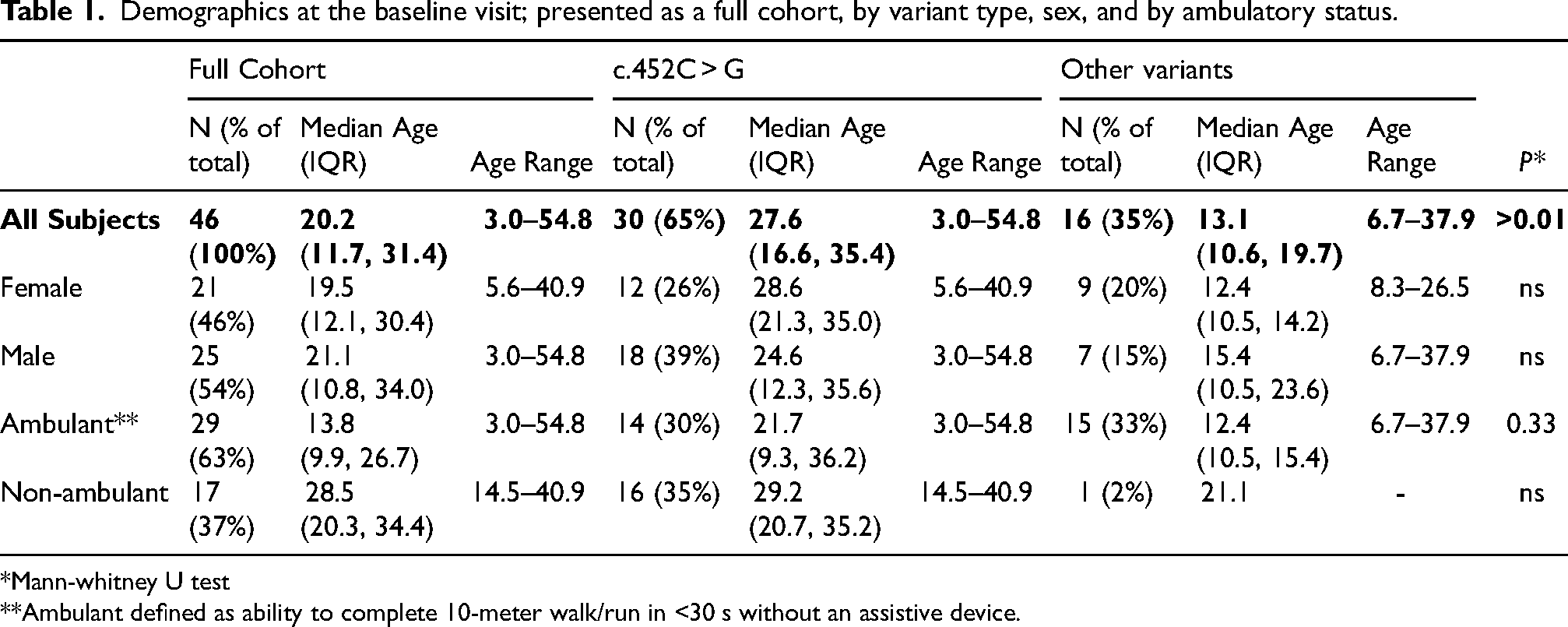
*Mann-whitney U test
**Ambulant defined as ability to complete 10-meter walk/run in <30 s without an assistive device.
Sixty-five percent (N = 30) of those enrolled had a confirmed c.452C > G variant in SCGB; the remaining 16 had other identified variants in SCGB (see Supplemental Table 1). The c.452C > G variant group was, on average, older compared to those with the ‘Other variants’ group (P < 0.01) (Figure 1). All but one individual in the ‘Other variants’ group was ambulant at enrollment whereas the c.452C > G variant group included 17 (52%) individuals who were no longer able to walk.
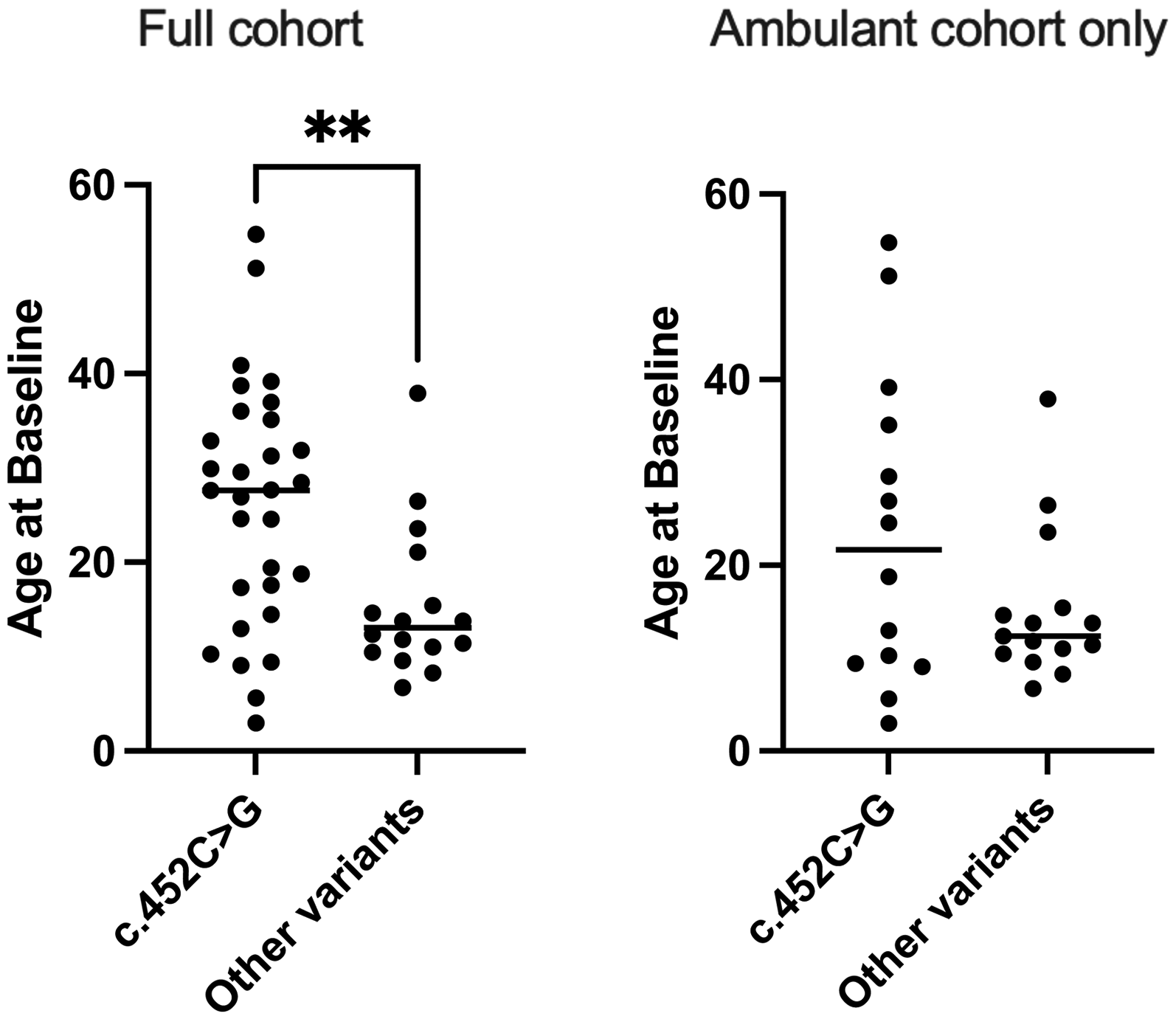
In our cohort, those in the c.452C>G variant group were, on average, older than those with Other variants (Mann-Whitney U test; *p<0.01). Further, a majority of the Other variant group (94%) were ambulant compared to only 52% of those in the c.452C>G group. Consideration of the spread of age and abilities between cohorts is crucial when interpreting PerfO results.
Baseline
The PerfOs quantified functional performance across a wide range of abilities; average baseline performance on all outcomes by variant group are listed in Table 2.
Group average baseline performance on PerfOs presented as a full cohort and by variant subgroup, including median, IQR, range and number of subjects that completed each outcome.
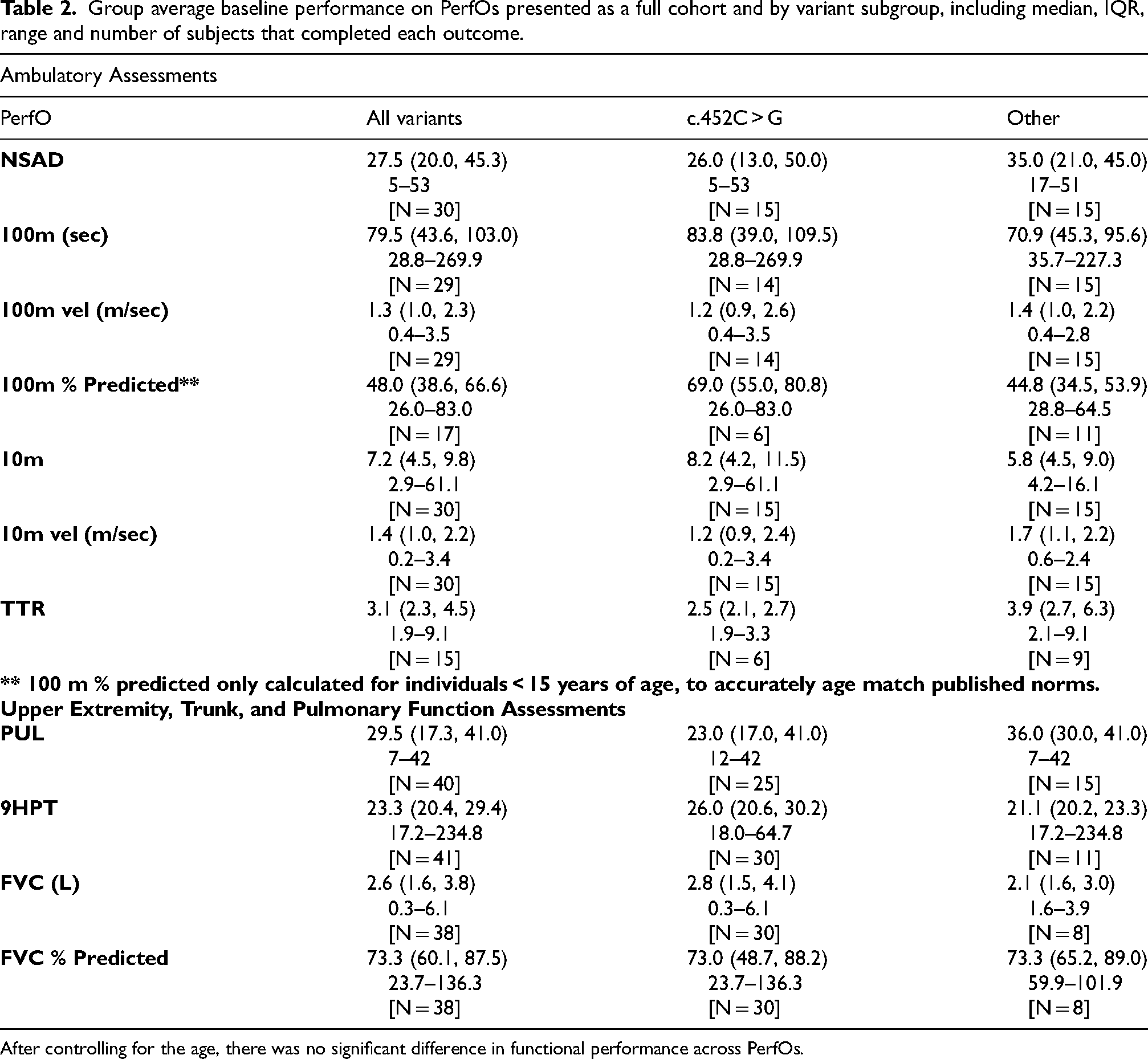
After controlling for the age, there was no significant difference in functional performance across PerfOs.
After controlling for age, there was no significant difference in functional performance between variant groups at Baseline. There was a moderate and significant correlation between age and performance on all outcomes (Figure 2) (rho = 0.53–0.70, P < 0.01) except 9HPT and FVC % predicted (both, P > 0.05); the polarity of the relationship was dependent on the scale used (e.g., it took longer to complete timed items as age progressed while other functional scales like the NSAD decreased in score as subjects increased in age).
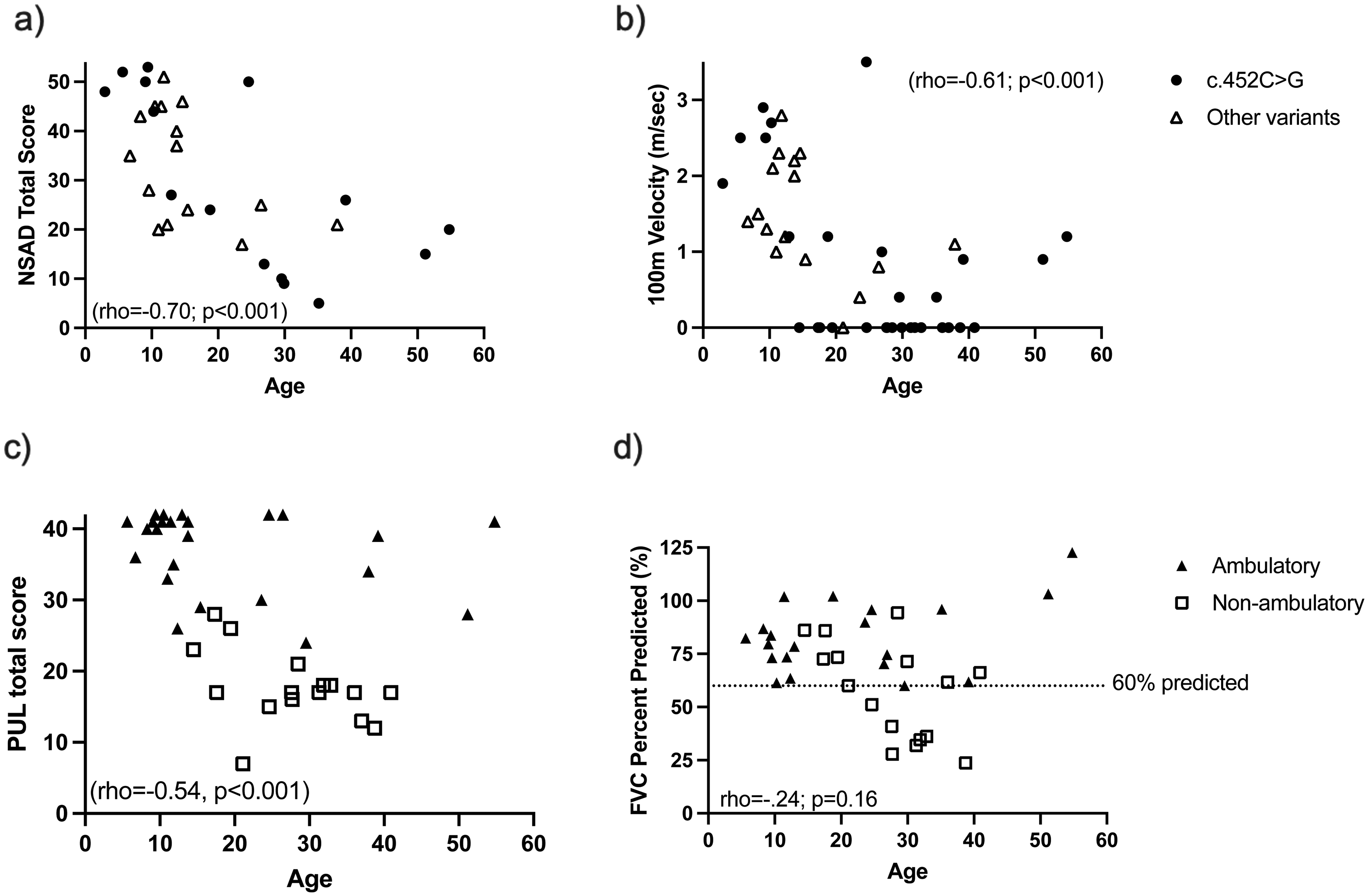
Individual performance at baseline on the a) NSAD and b) 100m, identified by variant subgroup. c) Performance on PUL and d) Pulmonary function (reported as a percent of predicted value) are also depicted at baseline, with individuals identified by ambulatory status. Correlations calcuated using Spearman's rho.
All PerfO were highly and significantly correlated to each other (rho = 0.67–0.91, P < 0.01), except the 9HPT, which was weakly correlated to PUL only (rho = 0.44, P < 0.05). Pulmonary function (FVC % Predicted) was weakly but significantly correlated to PUL only (rho = 0.38; p < 0.05) as no pulmonary function involvement was identified in the ambulatory cohort, with the values for FVC above 60% of predicted for all ambulatory participants (Figure 2(d)). 26 The strongest relationships were between different PerfOs measuring ambulatory performance, with the NSAD and 100m being the strongest (rho = 0.92; p < 0.001).
Performance on assessments of ambulatory PerfOs was variable across the full cohort. Only 15 subjects (33%) were able to complete TTR without furniture or external support, with the average age of those completing this task being 10.8 years (range 3.0–24.6 years). All subjects who independently rose from the floor had a 10m time less than 7.7 s (<1.3 m/s) (Figure 3). Twenty-nine people completed the full 100m timed test between 28.8 s to 269.9 s (0.4–3.5 m/s). For subjects aged 4–15 years (n = 17), a comparison of performance to expected performance of healthy peers demonstrates this cohort was on average 49.2% below the average performance for individuals of matched age and body mass index. The deficits ranged between 17.0% to 76.8% below the matched mean which demonstrated a significant delay even in the mildest subject at baseline.
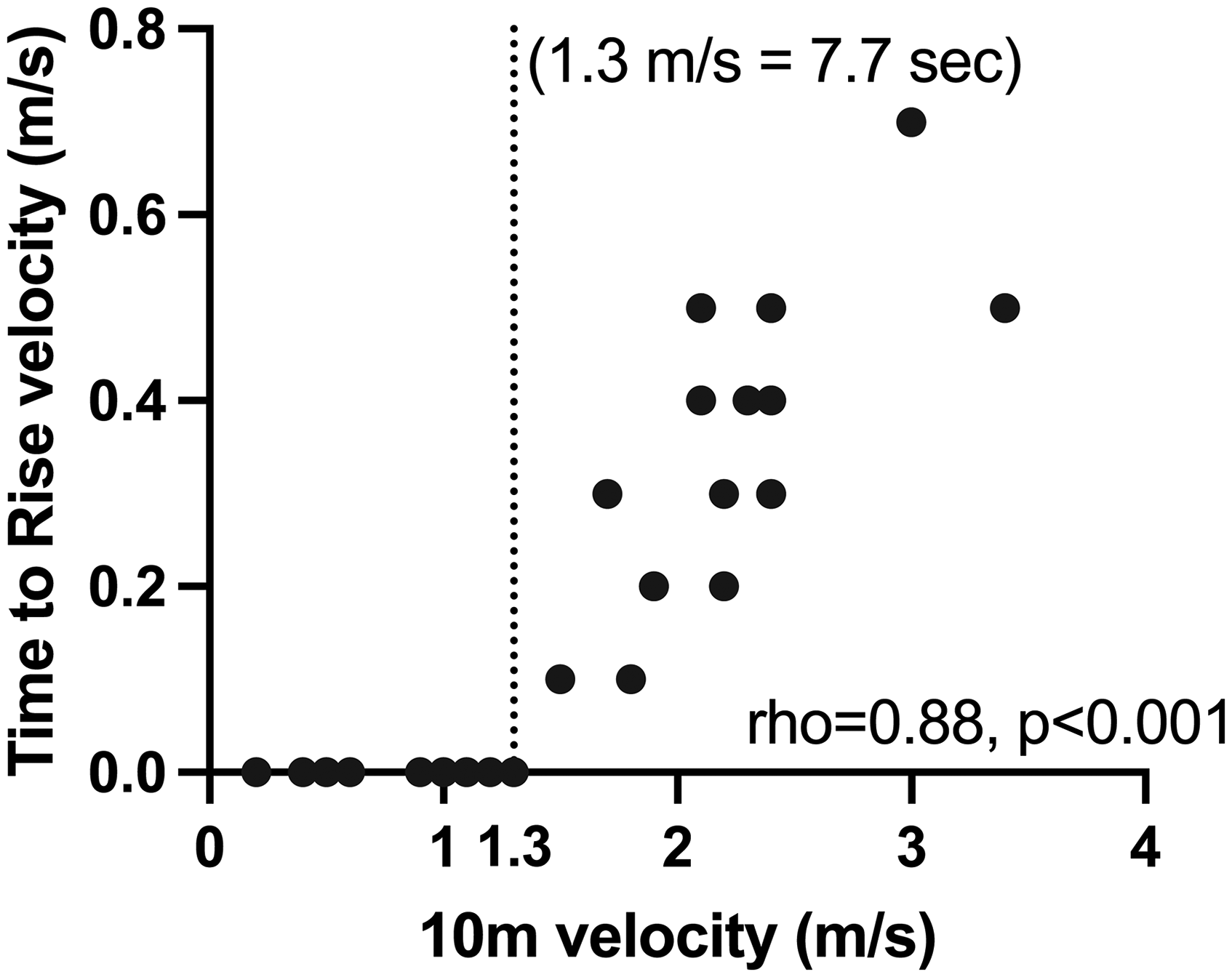
Ten meter (10m) performance is significantly correlated to rise from floor (TTR) velocity and appears to have a predictive value for the loss of that skill. Both cross-sectionally and longitudinally, subjects lost the ability to rise from the ground independently after their 10m velocity fell below 1.3 m/s.
Evaluation of upper extremity function identified a slight ceiling effect (defined as scoring ≥ 38 points out of 42 total) with 15 (38%) subjects scoring within this range. Individuals most likely to achieve a high score on the PUL were younger, (median age 11.4 yrs, range 5.6–54.8 years), ambulatory, and higher functioning overall (median NSAD = 39 ± 11 out of 54 points). Despite this, the PUL differentiated between subjects by ambulatory function in our cohort (median ambulant PUL = 40 points v. median non-ambulant = 17 points; Mann-Whitney U, p < 0.01). While many subjects performed below the average expected for their age, the 9HPT did not discriminate abilities well in this population based on ambulatory status or age as most subjects had a similar time on this test (Mann-whitney U, p = 0.16) until severe upper extremity weakness was present (N = 1, 9HPT time = 234.8 s).
Longitudinal performance
Visits were completed at 6-monthly or yearly intervals over time and included the same battery of testing as at baseline (Month 6, N = 40; Year 1, N = 26; Year 2, N = 24; and Year 3, N = 23 visits), apart from the 9HPT which was excluded following interim analysis at Year 1. The number of longitudinal observations on any given PerfO is variable based on both the ability of the subjects and retention of enrollment. Longitudinal participation was more consistent in the c.452C > G group (94%, 85%, 92%, and 96% of total visits, respective to timepoints above). Average change in performance on PerfOs can be found in Table 3.
Average change in performance from baseline on PerfOs at each timepoint.
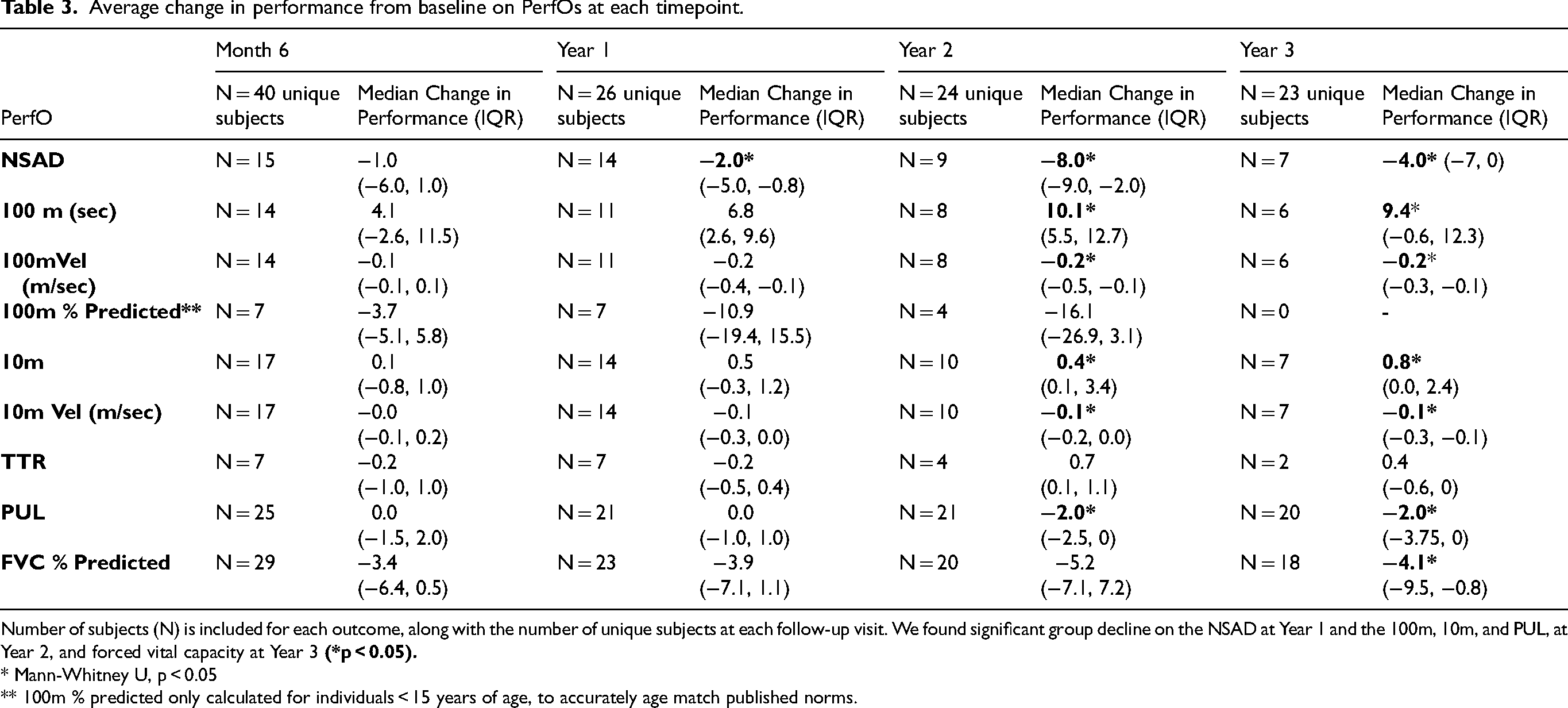
Number of subjects (N) is included for each outcome, along with the number of unique subjects at each follow-up visit. We found significant group decline on the NSAD at Year 1 and the 100m, 10m, and PUL, at Year 2, and forced vital capacity at Year 3
* Mann-Whitney U, p < 0.05
** 100m % predicted only calculated for individuals < 15 years of age, to accurately age match published norms.
Comparison of group performance over specified timepoints demonstrations that no PerfOs in this study reached a statistically significant change in 6-months’ time. The NSAD was the only measure that showed a statistically significant decline (median change = 2 points, p < 0.05) at Year 1. In a 24-month period the NSAD, 100m, 10m and PUL all had a statistically significant change. Time to rise did not show a statistically significant change, likely due to the significant floor effect of this assessment as evidenced by the small number of people capable of completing this item (baseline, N = 15; year 1, N = 7; year 2, N = 4; year 3, N = 2); to note, the 10m velocity cut-off predicting loss of ability to rise from floor persisted through longitudinal analysis and no subject, at any time point, who had a 10m time > 1.3 m/s (or >7.8 sec) was able to rise from the ground independently. One child lost the ability to rise from the floor (10m = 1.2 m/s, this visit) compared to baseline while the others were lost to follow-up. Forced vital capacity did not show statistically significance until the 3 year mark; this is likely attributed to the small number of subjects that have pulmonary deficits.
Individual performance on selected PerfOs over the 3-year period are depicted in Figure 4. Total NSAD score in the ambulatory cohort could be grouped by the ability to complete these individual tasks (i.e., TTR and stand from chair)(Figure 4(a)): those able to achieve both independently had an average NSAD score of 44 points, SD 6.5; those able to rise from a chair but no longer able to TTR, an average NSAD score of 22 points, SD 3.5; and those who had lost the ability to complete both, an average NSAD score of 15 points, SD 5. Additionally, there were fewer patients and study visits (N = 7; 11 visits) where individuals were able to rise from a chair but not the floor, compared to the other groups (36 and 30 total visits throughout the duration of the study), suggesting the ability to rise from a chair may be quickly lost following the loss of independence with TTR. Similarly, individual 100 m performance over 3 years with reported values for functional indicators of gait speed are depicted in Figure 4(b). Considered a functional vital sign, gait speed has been linked to safety and independence within the home and community. 27 Only seven of participants who completed the 100m moved at a speed greater than 1.3 m/s which is the minimum speed considered to safely cross a street. Most of the subjects enrolled maintained their range of functional gait speed, however, four subjects (14%) did lose ambulation over the duration of the study (Figure 4(b)). Three of the four subjects had the lowest NSAD scores at baseline (range, 4–10 points), the slowest 100 m velocity at baseline (range, 0.1–0.5 m/s), and range of PUL scores between 18–24 points. The fourth subject lost the ability to walk between Year 1 and Year 2 visits. This individual's functional trajectory of decline was quicker compared to all others in the study; over two years he lost the ability to rise from the floor and rise from a chair, had a decrease in NSAD score by 28 points and a decrease in PUL score by 18 points, over 2 years. Lastly, total PUL score was grouped by gross functional reaching ability (i.e., overhead, mid-level / could bring hand to mouth, and tabletop activities)(Figure 4(c)): those with ability to reach overhead demonstrated an average PUL score of 36 points, SD 5.7; compared to those reaching within mid-level activities had an average PUL score of 22 points, SD 3.0; and those completing tabletop level movement scored an average of 16 points, SD 3.0.
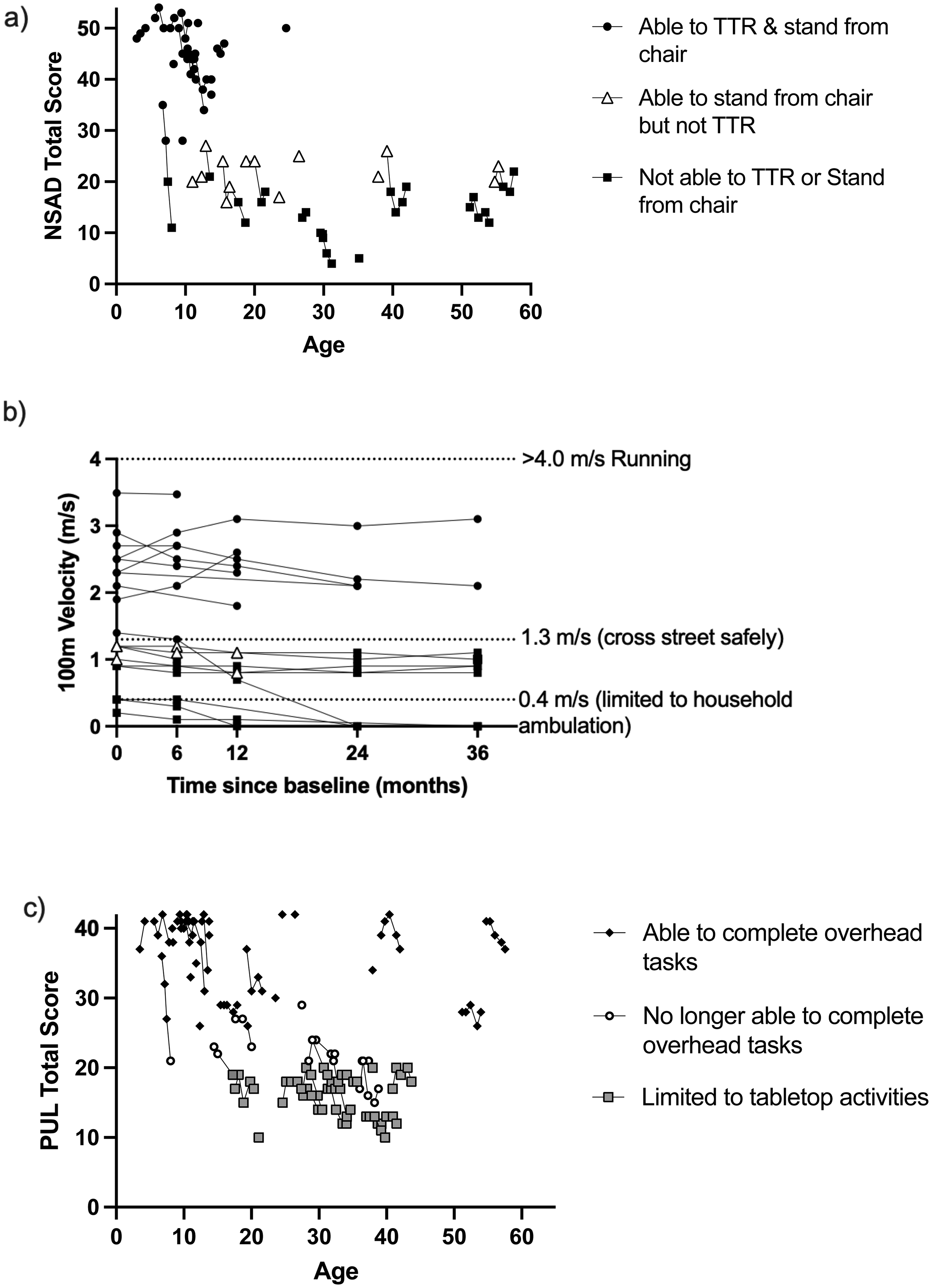
Individual performance on selected PerfOs over time. In the ambulatory cohort, overall performance on the a) the NSAD and b) the 100m are presented by ability to complete certain motor tasks related to functional independence (i.e., TTR and ability to stand from a chair). Upper extremity function in the full cohort, as depicted by performnace on c) PUL, is also related to ability to complete certain activities of daily living (i.e., brush hair, feed self, and type on a computer). These distinctions may help elevate clinical conversations regarding needs for future mobility aides and other assistive tools.
Over the course of the study, only one subject obtained a perfect score on the NSAD at age 6.2 years. Three subjects scored within three points of the max of the scale (> 51 points; ages 5, 9, and 11 years) which could suggest a small ceiling effect in some younger children. Rising from the floor without the use of a Gower maneuver, standing on one's heels, standing on one leg without sway or using compensations, and getting up from the floor through half kneeling were the most difficult items for the higher achieving cohort. Further, participants in this cohort lost the ability to rise from a chair independently as NSAD score reached 20 points (+/- 3 pts). While we found a modest ceiling effect cross-sectionally with the PUL, we found no floor effect over time with all subjects achieving a score of ≥10 points and even the most progressed individuals with those on daytime ventilatory support able to complete many items in the distal dimension of the assessment.
Maturation of individuals with a progressive neuromuscular condition must be considered during analysis as motor function is expected to improve in young children, albeit typically at a slower trajectory than age matched peers. In our sample, we enrolled 17 individuals who were under the age of 15 years at baseline (age range 2.9–14.6 years) and saw that no one had improved scores on their functional assessments after they reached 15 years of age. To examine the impact of maturation on function, we highlight the NSAD and 100m performance of these subjects separately in Figures 5(a&b). Overall we present 46 longitudinal visits from the 17 subjects who were first tested under the age of 15 years. Performance on the 100m trends towards improvement until 6 or 7 years of age (Figure 5(a)), with only one individual reaching the average expected performance (50th percentile) for a healthy peer of a similar age and body type, which was immediately followed by a decline in predicted performance and speed. A similar trend was seen with performance on the NSAD, as the two subjects that improved in total score were under the age of 7 years (Figure 5(b)).
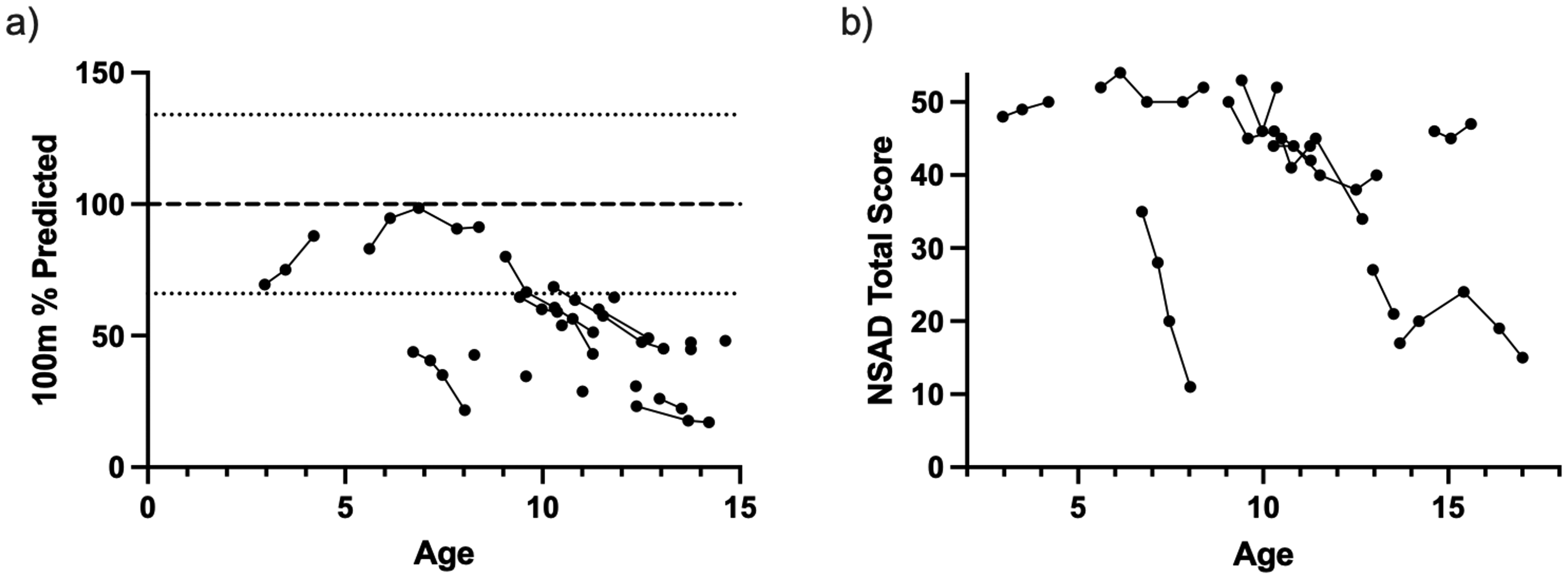
The functional performance of children and adolescents on the a) 100m (depicted as % of the average predicted) and b) NSAD demonstrate slight improvements during earlier years, which is followed by functional decline.
Discussion
This study prospectively characterized the functional performance of individuals with LGMDR4 using standardized PerfOs. These PerfOs include those used in current clinical trials and other ongoing natural history studies. With the exception of the 9HPT, all of the PerfOs quantified disease in LGMDR4, by distinguishing groups based on ambulatory status and measuring change over time. They also characterized onset of weakness in LGMDR4, with lower extremities affected before upper extremities, followed by pulmonary function impairment.
Measurement for disease management is an important concept in the clinic and natural history studies may help provide data to help guide clinicians make data driven recommendations. We know that rising from the floor without support is one of the first skills lost in individuals with a progressive neuromuscular disease. Our finding that no individual with a 10 m greater than 7.8 s (1.3 m/s) was able to rise from the floor independently could be useful when guiding discussion around home and safety modifications. Additionally, the relationship between overall performance on certain PerfOs, such as the NSAD, 100m, PUL and the ability to perform certain functional skills provides further insight into disease progression in LGMDR4 and can inform proactive clinical management and counseling. For example, the ability to rise from the floor and the ability to stand from a chair independently are two skills that are an important component of functional independence. Our findings that average NSAD scores are related to the ability to complete both, one, or none of these skills independently may assist with the clinical planning of future needs. Gait speeds as measured by the 100m can elevate clinical care discussions related to use of mobility aids with the goal of reducing fall risk and maintaining independence within the home and community. Similarly, utility of the PUL can guide discussions related to activities of daily living requiring overhead (i.e., dressing, grooming), mid-level (i.e., teethbrushing, eating), or tabletop (i.e., cell phone, computer use) levels of function.
This data also suggests that proximal upper extremity weakness begins earlier in disease progression in individuals with LGMDR4, compared to other well documented neuromuscular diseases such as Duchenne muscular dystrophy (DMD). In individuals with DMD, the loss of ability to raise arms overhead occurs after the loss of ambulation, while in our cohort, the earliest sign of upper extremity loss of function started at 12 years old. Further, distal hand function appears to be maintained until the late stages of the disease, as supported by the limited floor effect found using the PUL. This information may help clinicians discuss functional expectations and plan the administration of clinical outcomes that can help individuals and families adapt and plan for the future.
Maturational improvements in children with LGMD can make study planning challenging as it is difficult to ascribe improvements to the investigational therapeutic if the child is expected to still be improving due to maturation alone. The running speeds of all the children in our cohort were below the mean for their age and size with the exception of one child, with the c.452C > G variant, at only one time point. The individual's speed at this visit would be considered average based on age and size (50th percentile), but performance compared to peers declined at all subsequent visits. To note, this was the same individual who achieved the only perfect score on the NSAD, also only at one (the same) timepoint. This subject's sibling also had the c.452C > G variant, appeared to be “pre-symptomatic” at enrollment, and was followed beginning at 3 years of age (100-m normative data starts at age 4-years). All the other child and adolescent-aged subjects’ performance fell below the average speed expected for age and body-matched peers (Figure 4).
One of the challenges in clinical trials in LGMDR4 is the heterogeneous presentation. Another outlier with the same c.452C > G variant was 24.6 years of age at enrollment and had an NSAD score of 50 / 54 possible points, ten-meter run time of 2.9 s and time to rise of 1.9 s. Conversely, a different subject of a younger age at baseline (6.7 years) demonstrated the most profoundly quick decline and was of the “Other variants” group. While heterogeneity of trajectories may exist in this young cohort, our study demonstrates that functional abilities can be quantified using existing PerfOs. This understanding of differences in expected disease trajectories is an important consideration for data-driven interventional trial design.
Despite the heterogeneity of trajectories, our study demonstrates that functional abilities can be quantified using existing PerfOs. Overall, the trend for improvement in skills at a young age followed by a plateau in late childhood and decline in early teen through adult years is supported by performance on the NSAD and other timed function tests. This suggests that while young kids with LGMDR4 will gain motor skills and achieve motor milestones following birth, their motor performance is still impacted at a young age and those with LGMDR4 will likely never achieve the performance-level of their peers.
We acknowledge some limitations with our study. The first limitation is that the sample of convenience did not provide us with consistent longitudinal data points on every subject. This resulted in our sample size for each assessment to decrease over time. When looking over our sample we believe the attrition was randomly distributed across variants and severity, not related to a drastic decline in motor function, but have not tested this hypothesis. Additionally, this makes us cautious to calculate effect size and recommend clinical trial sample size from this data set.
We may also be skewed by over-representation of the c.452C > G group, leading to difficulty establishing genotype-phenotype correlations. Previous studies have suggested that individuals with a c.452C > G variant have a milder presentation and later symptom onset. 16 While this designation has been attributed to outcomes that are different from those included in this study (reliant on reported age of loss of milestones, such as loss of ambulation), it is difficult to confirm or refute this with our study, as the c.452C > G variant-grouping was, on average, older and thus showed greater deficit consistent with a progressive disorder. The c.452C > G variant cohort also included many more non-ambulant individuals. It is well known that travel can be difficult for individuals in power wheelchairs, this may have limited the number of non-ambulant individuals willing to come to Columbus, Ohio to be tested. Conversely, we traveled to the Plains community to complete functional testing on the c.452C > G group, therefore limiting burden of travel for the non-ambulatory individuals in this cohort.
Although this is the largest prospective study evaluating PerfOs in LGMDR4 to date, it is still a small sample and easily influenced by heterogeneity of disease leading to outliers; therefore, summary statistics should be interpreted with caution. It is also important to note that the NSAD was only completed in individuals that were able to transfer to a mat table safely; therefore, the interpretability of the utility of the NSAD to measure function and change in those whose disease progression limits independent transfers is limited in this data set.
Conclusion
The PerfOs selected to measure motor function in individuals with LGMDR4 are informative and able to measure changes over time. We also identify a great deal of heterogeneity in motor performance in individuals with LGMDR4, which must be accounted for during future interventional clinical trial design. Further research in a larger, longer prospective cohort is needed.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251339219 - Supplemental material for A prospective observational study assessing the functional disease progression of LGMDR4, betasarcoglycan-related limb girdle muscular dystrophy
Supplemental material, sj-docx-1-jnd-10.1177_22143602251339219 for A prospective observational study assessing the functional disease progression of LGMDR4, betasarcoglycan-related limb girdle muscular dystrophy by Megan A Iammarino, Natalie F Reash, Kiana Shannon, Maggie Dugan, Kelly Lehman, Alayne Meyers, Jerry R Mendell, Lindsay N Alfano and Linda P Lowes in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
We would like to thank the patients and families who committed their time and effort to participate in this study.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MI reports receiving salary support from Saretpa Therapeutics for evaluator training and clinical trial data review. NR reports receiving salary support from Saretpa Therapeutics for evaluator training and clinical trial data review. LA reports royalties for intellectual property in addition to salary support from Sarepta Therapeutics. LL reports royalties for intellectual property in addition to salary support from Sarepta Therapeutics at the time this research was conducted. JRM and LL are employees of Sarepta Therapeutics, but were both employees of Nationwide Children's Hospital at the time of this research study. KS, MD, KL, and AM declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.