
Invited Speakers
Tuesday 15th April 2025
S01Newborn Screening Using Whole Genome Sequencing: The Generation Study
David Bick, MD
Genomics England Ltd., London, UK
Genomics England in conjunction with the National Health Service England (NHSE) has undertaken a Research Ethics Committee approved research study, the Generation Study, to screen 100,000 unselected newborns across England for treatable conditions.
922 genes-conditions pairs were assessed against four principles (https://www.genomicsengland.co.uk/initiatives/newborns) followed by specialist review. 462 genes representing 208 conditions were chosen for the study, including 31 genes associated with neurologic conditions.
The study is currently recruiting from 20 weeks of pregnancy at 27 hospitals (18 trusts). Cord blood is the source of DNA for screening. Where cord blood is unavailable, a heel stick or indwelling line is the source. DNA extraction and short read whole genome sequencing is performed at cores facilities.
A Genomics England purpose-built pipeline selects variants. To maximize positive predictive value, only pathogenic and likely pathogenic variants are sought. A list of ‘include’ variants come from ClinVar (https://www.ncbi.nlm.nih.gov/clinvar/), from QIAGEN Inc. (Hilden, Germany), from Genomics England’s database and from gene specific ‘custom include’ lists. Predicted protein truncating variants in genes where loss of function is the mechanism of disease are also reported. The selected variants are reviewed by a clinical scientist.
‘Condition suspected’ results are passed to pediatric specialists who call the families to engage in treatment. Screen positive cases are confirmed with non-molecular confirmatory tests. Only conditions where NHSE has confirmed that the treatment is available throughout England are included.
To date, 6035 women have been recruited. 3279 newborns have been sequenced. 134 of the sequenced cases were prioritized for review by a clinical scientist. 18 cases have been reported to paediatric specialist for onward care.
Strong international interest in the potential of newborn genome screening has given rise to the International Consortium on Newborn Sequencing (https://www.iconseq.org/). Sharing outcomes across international programs and assuring access to treatment represent long term challenges. As the price of short read and particularly, long read genome sequencing falls, the availability and accuracy of newborn genome screening should improve.
S02Reducing neurogenetic and neurodevelopmental healthcare inequalities in under-represented populations
Professor Emma Baple
Professor of Genomic Medicine, University of Exeter
Recent large-scale genomic sequencing projects have transformed our understanding of genomic variation, and its relevance to health and disease. However, such programmes have limited ability to delineate the mechanistic basis of ultra-rare inherited disease or interpret the clinical significance of ultra-rare genetic variation. Additionally, because the majority of publicly available genomic variation data derives from studies of individuals of European ancestry, we are less able to interpret genetic variants in people from more diverse ethnic backgrounds, who are thus more likely to receive unclear genetic test results or be misdiagnosed. Conversely, due to their individual genomic architectures, detailed genetic and longitudinal clinical studies of inherited disorders present amongst under-represented and genetically isolated populations can help to define the relevance of rare genomic variation to disease.
Our long-running translational research studies of inherited disorders within the Amish communities of North America have provided unique and important insights into the biological basis of monogenic neurodevelopmental and neurodegenerative disorders, and complex inherited diseases. By establishing an interdisciplinary collaborative framework spanning biomedical and social science, healthcare policy makers and other disciplines, we have addressed unmet healthcare inequalities and needs. This work has transformed regional knowledge of the basis and causes of inherited disease, and improved regional healthcare/diagnostic services, clinical management strategies and rare disease policies. Following the Amish paradigm, our more recent collaborative translational genomics research programmes in Pakistan, the Palestinian West Bank and Oman, have enabled the delivery of similar benefits to populations in these regions, as well as families affected by rare disease worldwide.
S03Long-read sequencing as a comprehensive genetic test for rare disease patients
Professor Christian Gilissen
Department of Human Genetics, Radboud University Medical Center, Nijmegen, The Netherlands
More than 50% of families with suspected rare monogenic diseases remain unsolved with routine genetic testing. This diagnostic gap may be partially due to the fact short-read sequencing (SRS) technologies are unable to interrogate complex genome regions, and have difficulties in identifying repeat expansions and (complex) structural variation. Long-read sequencing (LRS) could potentially help bridge this diagnostic gap by capturing variants inaccessible to SRS, facilitating long-range mapping and phasing and providing haplotype-resolved methylation profiling. However, it is still unclear whether LRS is sufficiently accurate to identify small variants, and how well more complicated genetic variants can be detected with LRS, and whether LRS can potentially replace routine standard of care testing. We extensively validated the technical capabilities of LRS by performing benchmarking for 8 high coverage trios. In addition we performed LRS (30× HiFi genomes) for 100 samples with 145 known clinically relevant germline variants that are challenging to detect using short-read sequencing and necessitate a broad range of complementary test modalities in diagnostic laboratories that shows the potential to use a single technology to accurately identify all types of clinically relevant variants. Finally we are currently performing a prospective study using 1,000 clinical samples to determine the concordance of LRS to current standard-of-care (SoC).
S04Newborn Screening for SMA
Laurent Servais, MD, PhD
Professor of Paediatric Neuromuscular Diseases, MDUK Oxford Neuromuscular Center Department of Paediatrics, University of Oxford
Spinal Muscular Atrophy (SMA) is a recessive condition that affects 1 in 14300 newborns. In its more severe and frequent form- it leads to deaths or permanent ventilation between the age of 2 years. All forms are progressive conditions associated with a significant physical burden and a huge economic cost. Since 2017, three treatments – nusinersen, risdiplam and onasemnogene abeparvovec – have been approved by regulatory authorities in the US and Europe. All trials and real-world evidence have demonstrated much greater efficacy when delivered early. This has led to the rapid initiation of several newborn screening (NBS) programs for SMA since 2018. In 2018, a request to consider an SMA NBS was rejected by the UK National Screening Committee (NSC) on the rationale that there was insufficient evidence to suggest that the intervention would do more good than harm. It is currently under re-evaluation. Both the initial submission and the current re-evaluation have been supported unanimously by physicians and patients’ associations. A request for an earlier re-evaluation based on compelling international peer-reviewed evidence was unsuccessful.
It is estimated that nearly all US and a vast majority of European newborns are screened for SMA- through a simple and cheap PCR that detects 96% of patients- as 4% presents with a deletion and point mutation on the other allele that is not detected by PCR. The 20 pilots or state programs published so far have systematically demonstrated an excellent reliability and sensitivity of the method- and a much better prognosis of newborns identified by NBS in comparison with those identified per symptoms. In 2022- Ukraine has launched a national screening in the middle of the war.
Four health economic models have robustly demonstrated that NBS of SMA is a highly cost effective strategy that leads not only to substantial gains of QALYs, but also to substantial economic savings.
In the UK, one child is born every 4 days with SMA. 507 children have been registered in SMA Reach registry from 1st January 2019 to 1st November 2024. Sixteen patients died. None of the 231 SMA1 patients acquired independent walking and the majority of them needed a ventilatory support, a nutritional support or both. This contrasts dramatically with the situation in countries like Belgium or Germany where SMA NBS has been set up as early as 2018.
The 2018 decision to refuse SMA NBS, despite the support of the entire national SMA community and in disregard of international evidence, resulted in the death or the permanent severe disability of more than five hundreds of children, this amount increasing by 7 children per month as NBS is still not in place. It also translates in significant cost and burden on the NHS that could have been avoided by a simple and highly cost-effective test that has been validated in 20 independent studies worldwide.
S05Tailored ASO Therapies: From Genomic Discovery to Human Application – Challenges and Opportunities
Rebecca Schüle, MD
Division of Neurodegenerative Diseases and Movement Disorders, Department of Neurology, Heidelberg University Hospital and Heidelberg Faculty of Medicine
Antisense oligonucleotide (ASO) therapies have emerged as a promising approach for treating genetically defined neurodegenerative diseases, particularly in the context of ultrarare disorders. By modulating gene expression at the RNA level, these therapies enable precision treatments tailored to specific pathogenic variants.
In my talk, I will provide an overview of the translational pathway from genomic discovery to the clinical application of ASO therapies. Using POLR3A-associated spastic ataxia as a model, I will explore the role of deep intronic variants in disease pathogenesis and demonstrate how ASO therapies can be designed to restore normal splicing. The presentation will cover key aspects of both preclinical ASO development and clinical considerations, including trial readiness, patient selection, outcome measures, and trial design.
Additionally, I will highlight the crucial role of academic platforms such as 1M1M – 1 Mutation, 1 Medicine in accelerating the development of RNA-based therapies for ultrarare diseases through interdisciplinary collaboration.
S06Determining ASO-amenability of disease-causing variants
Dr. Marlen Lauffer
Dutch Center for RNA Therapeutics, Leiden University Medical Center, Leiden, The Netherlands
1Mutation 1Medicine
N=1 Collaborative
m.c.lauffer@lumc.nl
About 6-8% of the world’s population is affected by at least one of the 8,000+ rare diseases, the majority of whom are genetic in origin. For less than 5% of the disorders targeted therapies are available, and the incentives remain low to develop therapies in an industry setting. Fortunately, individualized genetic therapies are emerging as promising therapeutics for these individuals, whereby the developments are mainly facilitated by academia and non-profits. Over 25 patients have received variant-specific RNA therapies to date, and a few cases of other bespoke gene genetic interventions have been reported. The field expects exponential growth in these developments in the coming years and an expansion to modalities other than the prominent RNA therapeutics. It will thus become important to understand who are suitable candidates to receive individualized genetic therapies. However, we are still far from being able to routinely assess a variant’s eligibility for genetic interventions or provide informed guidance on potential therapies and their developments.
In 2024, the N=1 Collaborative released the first consensus guidelines for the assessments of genetic variants towards antisense oligonucleotide therapies, one form of an RNA-based therapy. The N=1 Collaborative is a global initiative aimed at standardizing, streamlining, and coordinating individualized therapy developments. Here, I will present the N1C VARIANT guidelines, introduce the guiding principles, and present how these guidelines can be applied to patient cohorts or implemented in diagnostic settings. I will further discuss current developments for establishing guidance to assess genes and diseases for ASO-amenability, plans to expand our guidance to other treatment modalities, and ideas to automate the assessment procedure for seamless integration into diagnostic workflows.
S07From gene to treatment: the end of the beginning
Professor Mary Reilly
Head of division of clinical neurology, UCL
No abstract
S08Advances in imaging metabolism using photoacoustics and Raman spectroscopy
Professor Sarah Bohndiek
University of Cambridge/ Cancer Research UK Cambridge Institute
Spectroscopic imaging represents a new frontier in medical physics that enhances the vision of the clinician and enables measurements of the local concentrations of key biomarkers in tissue. Spectroscopic imaging records spatial information in 2D or 3D, alongside an additional spectral dimension, which encodes chemical information. In photoacoustic imaging, the distinct absorption properties of oxy- and deoxy-haemoglobin can be exploited to infer local blood concentration and oxygenation, while water and lipids can be resolved for analysis of tissue composition. With Raman spectroscopy, the distinctive fingerprints of different molecular building blocks of tissue can be measured, enabling quantification of dynamic processes such as fatty acid synthesis and oxidative phosphorylation.
Here, I will review recent research efforts that aim to quantify metabolic properties of cells and tissues using photoacoustics and Raman spectroscopy, indicating the potential of these technologies for clinical diagnostics and staging of neuromuscular diseases.
Wednesday 16th April 2025
S09Proteomic biomarkers of muscle diseases
Professor Andreas Roos
University Medicine Essen, Duisburg-Essen University, Dept.of Neuropaediatrics
Biomarkers serve as critical indicators of physiological processes, disease progression, and responses to various interventions and treatments. Particularly in diagnostic, prognostic, and predictive applications, biomarkers have proven to be invaluable tools, becoming essential measures across numerous disorders, including muscular diseases. Various biomaterials can be utilized to provide key pathophysiological insights.
With the advent of proteomic profiling, the ability to quantify thousands of proteins in parallel has significantly advanced. In this context, mass spectrometry-based protein analytics has emerged as a state-of-the-art approach for identifying and validating biomarkers, offering comprehensive insights into the manifestation, progression, and treatment response of muscular diseases. A range of biomaterial sources—including muscle biopsies, cultured cells (such as fibroblasts), and body fluids—have been explored to meet the growing demand for biomarkers. Special attention has been given to those that can be monitored in a minimally invasive manner while maintaining significant pathophysiological relevance.
An overview of the past decade of biomarker research in muscular diseases, with a particular focus on a paradigmatic strategy for identifying biomarkers of direct pathophysiological relevance is provided where Myotonic Dystrophy Type 1 serves as a case study, highlighting a targeted approach to biomarker discovery. Additionally, white blood cells are discussed as a promising, less invasive alternative to muscle biopsies for biomarker research.
Finally, as the potential of protein-based biomarkers continues to expand, so do the expectations regarding their informational value. Thus, the balance between justified and unrealistic demands on biomarkers relevant to muscular diseases is discussed.
S10Biomarkers in acquired and genetic neuropathies
Professor Michael Lunn
Clinical Lead in Neuroimmunology, National Hospital for Neurology and Neurosurgery
The modern concept of disease biomarkers has expanded rapidly with the availability of ultrasensitive immunochemistry, imaging techniques with greater resolution and disease specificity, and an expansion in diagnostic genetics. These open the door to using biomarkers for a greater breadth of purposes including diagnostics, natural history, prognosis and following the outcomes of intervention in the clinic and clinical research.
A biomarker is a measurable indicator of some biological state or condition. Biomarkers are often measured and evaluated using biofluids, tissues or imaging modalities to examine normal biological processes, pathogenic processes, or pharmacologic responses to therapeutic interventions. In clinical medicine, whilst group statistics often identify statistically significant category differences it is far more useful when a biomarker has utility for a single individual in following their progress or response to intervention.
This lecture will concentrate on the more recent developments in clinical biomarkers, biofluids and imaging. Well-constructed Rasch-built clinical scales have linearity across the range of measurement, can be responsive and have statistical validity when used to compare individuals or groups. The ability to measure meaningful clinical change in disability, anchors other biological measures which are nearer to the pathogenesis of the disease. The last decade has seen a rapid expansion of fluid biomarkers representing tissue damage. Neurofilament light, now easily measured, remains the benchmark for active axonal damage and has many advantages but also a lack of specificity for disease. More specific biomarkers of damage in peripheral nerve cells are made increasingly viable with ultrasensitive technology and examples will be presented. For slowly progressive disease such as the genetic neuropathies biofluid measures of disease activity probably have a kinetic that is too short, and MRI is increasingly helpful as a tool for prognostication and classifying categories of disease and therapeutic responsiveness over long periods of time.
S11Overlap of neuropathy/myopathy genes
Professor Tanya Stojkovic
Pitié-Salpêtrière Hospital, Paris, France
In the past, before the advent of molecular biology, neuropathies and myopathies were studied separately, with little or no overlap between the two entities.
However, over the last 20 years, numerous genes have been discovered in both myopathies and hereditary neuropathies, and even more since the advent of next generation sequencing. Moreover, overlap between myopathies and neuropathies was well known for mitochondrial genes.
More unexpectedly, several genes involved in myofibrillar myopathies have been associated with predominantly motor neuropathies. This is particularly the case for BAG3, DES and CRYAB genes; although clinical signs reminiscent of those observed in myopathies (i.e., cardiomyopathy, axial muscle involvement…) may appear as the disease progresses. More recently, extracellular matrix proteins have been implicated in motor neuropathies and spinal muscular atrophies, such as VWA1 protein. One of the most important components of the extracellular matrix is represented by collagens, whose role in motor axonal growth is beginning to emerge.
This overlap between myopathies and motor neuropathies are increasingly recognized, especially in genes involved in multisystem proteinopathy, such as VCP, MATR3, SQTMS1, TIA1, leading to nerve, brain, muscle and bone damage in various combination. On the other hand, mutations in genes such as HSPB8 or SPTAN1 known to be responsible for distal motor neuropathy, have now been identified in distal myopathy or a mixed picture sometimes combining a neurogenic and myogenic component, both electromyographically and histologically.
As we make progress with new sequencing techniques (WGS, long read), unexpected phenotypes are arising, involving an already known gene for myopathy in a peripheral neuropathy or vice versa. Di-genism or even oligo-genism could account for a mixed phenotype combining the nerve and muscle, or a polymorphic variant could also be responsible for a phenotype alternating between neuropathy and myopathy.
S12Markers of Disease progression in Pompe disease
Professor Jordi Diaz Manera
Professor of Neuromuscular, Translational Medicine and Genetics, Newcastle University
No abstract
S13MRI Biomarkers in Muscle
Professor John S. Thornton PhD
Neuroradiological Academic Unit, UCL Queen Square Institute of Neurology
University College London
Over the past decade quantitative MRI (qMRI) methods have emerged with validation confirming their potential role as robust, responsive objective measures of progression across many neuromuscular diseases. MRI-obtained muscle fat-fraction and muscle cross-sectional area, indices of disease which can be more responsive than conventional trial endpoints, are now finding application in patient treatment trials. Important recent developments which will facilitate the take-up of qMRI outcome measures include the introduction of deep learning supported automated image segmentation, which significantly reduces the workload overhead in extracting qMRI readouts from the source images, and AI supported accelerated image acquisition technologies, which can significantly reduce imaging times. qMRI methods sensitive to muscle tissue water distributions and microstructure (T2 and diffusion metrics) are also under development. Finally, the potential of moving beyond structural imaging to obtain measures of muscle metabolism accessible to magnetic resonance scanners is likely to become increasingly important.
18th UK Neuromuscular Translational Research Conference
15th and 16th April 2025
Posters, Flash and Platform
Presentations
‡indicates a platform or flash
presentation
Motor Nerve Disorders
MND01Motor Unit Magnetic Resonance Imaging (MUMRI) as a Novel Biomarker in Spinal Muscular Atrophy (SMA)
Matthew G. Birkbeck1,2
, Ian Schofield1, Ian Wilson1, Julie Hall1,3, Chiara M. Bettolo1,4, Volker Straub1,4, Roger G. Whittaker1, Andrew M. Blamire1
1Newcastle University Translational and Clinical Research Institute (NUTCRI), Newcastle University, Newcastle upon Tyne, United Kingdom, 2Northern Medical Physics and Clinical Engineering, Freeman Hospital, Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom, 3Department of Neuroradiology, Royal Victoria Infirmary, Newcastle upon Tyne NHS Foundation Trust, Newcastle upon Tyne, United Kingdom, 4John Walton Muscular Dystrophy Research Centre, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom
matt.birkbeck@newcastle.ac.uk
Background: Spinal muscular atrophy (SMA) an autosomal recessive disease characterised by the loss of the secondary motor neurons leads to profound muscle weakness. Genetic therapies are rapidly advancing SMA trials, however, treatments need to be delivered early in the disease. A sensitive and non-invasive biomarker to monitor treatment response is required. We have developed a technique called motor unit MRI (MUMRI), which non-invasively detects fasciculation, a common symptom of spinal muscular atrophy (SMA). Here, we applied MUMRI in SMA patients and controls to compare fasciculation rates.
Methods: In 10 patients (all SMA III;6 male) and 10 age comparable and sex matched controls; images of the tongue, upper right arm, paraspinal and bilateral lower limbs (thighs & calves) were acquired using 3-point Dixon and MUMRI (pulsed gradient spin echo) MRI sequences. For each body region, muscles were manually delineated, and fat fraction and fasciculation rates were calculated using in-house algorithms.
Results: At group level, fat fraction %, was higher in SMA compared to controls for: upper arm (35.0 ± 25.4 vs. 4.2 ± 1.1, p<0.0001), paraspinal (41.4 ± 31.0 vs. 7.4 ± 4.5, p=0.002), thighs (54.8 ± 23.8 vs. 5.7 ± 1.0, p<0.0001) and calves (29.6 ± 23.5 vs. 4.4 ± 0.9, p=0.0003), but not for the tongue (13.9 ± 3.2 vs. 13.0 ± 3.3, p=0.393). Fasciculation rate (number of signal voids per cm3 muscle tissue per minute, cm-3min-1) was higher in SMA compared to controls for: upper arm (0.28 ± 0.61 vs. 0.002 ± 0.001, p=0.014), paraspinal (0.06 ± 0.06 vs. 0.003 ± 0.005, p=0.001), thighs (0.46 ± 0.57 vs. 0.008 ± 0.005, p=0.002) and calves (0.37 ± 0.58 vs. 0.02 ± 0.02, p=0.001), but not for the tongue (0.17 ± 0.17 vs. 0.05 ± 0.08, p=0.082).
Discussion: We showed significantly higher fat fraction in the paraspinal muscles, a novel finding in SMA III. MUMRI has detected significantly higher fasciculation rates in cervical, thoracic and lumbar innervated muscles, but not bulbar. Although further work in larger cohorts is required, MUMRI is an attractive non-invasive novel biomarker which could be used to monitor progression & response in clinical trials of SMA.
MND02Cardiac Involvement in Adults with Spinal Muscular Atrophy: A Multi-Centre Audit of Cardiac Monitoring and Complications
Dr Calum Byrne
1, Dr Rosa Tanzi1, Dr Mark Specterman2, Dr Clare Galtrey1, Dr Ahaan Kaul 3, Dr James B. Lilleker 3 and Dr Channa Hewamadduma4
1 Atkinson Morley, Regional Neurosciences Centre, St George’s Hospital, Blackshaw Road, Tooting, SW 17 0QT, 2 Department of Cardiology; St George’s Hospital, Blackshaw Road, Tooting, SW17 0QT, 3 Department of Neurology, Northern Care Alliance NHS Foundation Trust, Salford Royal Hospital, M6 8HD, 4 Department of Neurology; Sheffield Teaching Hospitals NHS Foundation Trust; Sheffield, S10 2JF
Calum.byrne@stgeorges.nhs.uk
Background: Spinal muscular atrophy (SMA) is a genetic neuromuscular disorder caused by mutations in the SMN1 gene leading to reduced SMN protein levels. Whilst SMA predominantly affects motor neurons, there is an association of cardiac manifestations. SMN2 modifiers like Risdiplam, which has systemic bioavailability, may impact the cardiovascular system and requires monitoring for QT prolongation.
Aims: Audit of all SMA patients on disease modifying drugs across three regional centres (St George’s, Salford and Sheffield) to assess the outcomes of cardiac monitoring.
Methods: A 24-month retrospective manual review of clinical notes and investigations across centres. Patients were categorised by SMA type and severity; concurrent disease modifying treatment; cardiac symptoms and cardiac investigations. All ECGs were reviewed by a cardiac electrophysiologist.
Results: A total of 78 patients were identified. 71 (91%) had ECGs to review and of these 16 (23%) demonstrated an abnormality. 24% SMA type 2 (mean age 35) and 17% SMA type 3 (mean age 42). ECG abnormalities were 6 LVH criteria; 2 RVH criteria; 2 right bundle branch block; 1 right bundle branch block + left axis deviation; 1 first degree AV block; 3 with T wave inversions; 1 prolonged QTc. 17 (22%) patients required specialist cardiology assessment for their ECG/symptomatology. The patient with long QTc was found to be familial and was not taking Risdiplam. Echocardiograms demonstrated only 2 structural abnormalities: a 19-year-old (SMA type 1) with mild-mod mitral and tricuspid regurgitation and normal biventricular size and function; a 40-year-old (SMA type 2) with impaired right ventricular function and no left to right shunt identified. No arrhythmias were identified on holter monitoring in the 2-year period of notes review.
Conclusion: SMA patients require monitoring for cardiac manifestations. We have demonstrated over a fifth of SMA patients across 3 regional centres exhibit ECG abnormalities and over a 2-year period more than a fifth required a formal Cardiology assessment. With the advent of disease modifying therapy differentiating age-related vs primary SMA-associated cardiac manifestations becomes challenging. No patients on Risdiplam displayed QT prolongation. Cardiac structural abnormalities
MND03The Integration of PROMs and Clinician-reported Data: a Holistic Approach to Characterise Disease Burden and Treatment Impact
Aleks Carver1
, Jess Page1, Elena Karkkainen1, Elzo Cavalcante2, Matthew Madden2, Kate Adcock3, Maria Farrugia4, Gennadiy Ilyashenko5, James Lilleker6, John McConville7, Andria Merrison8, Matt Parton9, Liz Ryburn10, Portia Thorman10, Robert Muni-Lofra1, Mariacristina Scoto2, Chiara Marini-Bettolo1 and the Adult SMA REACH and SMA REACH UK clinical networks.
1The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, United Kingdom, 2Dubowitz Neuromuscular Centre, Great Ormond Street Hospital, London, United Kingdom, 3Muscular Dystrophy UK, London, United Kingdom, 4Institute of Neurological Sciences, Queen Elizabeth University Hospital, Newcastle upon Tyne, United Kingdom, 5TreatSMA, Royal Tunbridge Wells, United Kingdom, 6Manchester Centre for Clinical Neuroscience, Salford & University of Manchester, Newcastle upon Tyne, United Kingdom, 7Ulster Hospital, Belfast, United Kingdom, 8Bristol Neuromuscular Disease Centre & South West Neuromuscular Disease network, Newcastle upon Tyne, United Kingdom, 9Queen Square Centre for Neuromuscular Diseases, University College London, London, United Kingdom, 10SMA UK, Stratford-upon-Avon, United Kingdom.
aleks.carver@newcastle.ac.uk
Background: The UK SMA Patient Registry collects patient-reported outcome measures (PROMs) from individuals living with spinal muscular atrophy (SMA) in the United Kingdom and Ireland. In 2022, PROMs were introduced in the registry to supplement the clinical and genetic data held therein. PROMs capture the perspectives of adults and caregivers of young people living with SMA about the impact of their condition and treatment, their quality of life and activities of daily living. The importance of the patient voice is increasingly recognised and valued.
Aims: Currently, SMA therapies Nusinersen and Risdiplam are available in the UK via managed access agreements (MAAs). The collection of clinical and patient-reported data informs the review of treatment impact by UK regulatory authorities. In collaboration with the clinical networks Adult SMA REACH and SMA REACH UK, the registry aims to collect PROMs data of 100 patients receiving each treatment. PROMs data is then aligned with Adult SMA REACH and SMA REACH clinical data, anonymised, analysed and submitted to regulatory authorities for consideration as part of the treatment MAAs. Methods/Materials: Registration in the UK SMA Patient Registry is patient-initiated through a secure online portal. Patients are invited to complete questionnaires about their condition, including the following PROMs:
EQ-5D
Patient Global Impression of Severity (PGIS)
Patient Global Impression of Improvement (PGII)
SMA Independence Scale (SMAIS-ULM)
Free-text box
PROMs data is then aligned with clinical data collected by the SMA REACH networks.
Results: The registry has 673 participants: 465 adults (≥16 years); 208 paediatric (<16 years).
Since their launch in the registry, PROMs questionnaires have been completed by 254 adults and by the caregivers of 105 paediatric patients, and 2628 patient-reported outcomes have been collected. Findings and analysis from the past 3 years of PROMs data collection will be presented.
Conclusions: The UK SMA Patient Registry represents a well-defined cohort of individuals with SMA and is a valuable tool for the collection of SMA real-world data reported by treated and treatment-naïve patients. The registry’s collection of PROMs continues to support UK SMA data collection and supplements SMA REACH clinical data, assisting in therapy evaluation by regulatory authorities.
‡MND04Repurposing bile acid receptor therapies as treatments for motor neuron disease
Adam Creigh1, Ellis Carter1, Taisha Peplowska1, Lexie Urquhart1, David Jones2,
Helen Devine1
1 Mitochondria Research Group, Newcastle University, Newcastle upon Tyne, UK, 2 Liver Unit, Freeman Hospital, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom; Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, United Kingdom
Helen.devine@newcastle.ac.uk
Background: Amyotrophic lateral sclerosis is a devastating neurodegenerative disease characterised by the loss of motor neurons leading to progressive weakness. There is an urgent, unmet need for disease-modifying therapies for people with ALS as the currently approved drugs only increase lifespan by a few months. Dysregulated energy metabolism is found in both sporadic and familial causes of ALS, suggesting that targeting metabolic homeostasis may be beneficial.
The bile acid receptors, FXR and TGR5, are known regulators of metabolism and bile acids have known neuroprotective effects. Obeticholic acid (OCA) is a potent FXR agonist which is NICE-approved for the treatment of primary biliary cirrhosis (PBC). Here we evaluate the effects of OCA on ALS patient-derived iPSC motor neurons (iPSC-MNs).
Aims: To determine whether repurposed “next generation” bile acid (BA) receptor therapies are promising candidates for clinical trials in MND.
Methods/Materials: We targeted the FXR pharmacologically using OCA in iPSC-derived motor neurons derived from patients with the VCP ALS mutation. We assessed multiple ALS disease phenotypes including cell survival, neurite outgrowth and metabolic function following treatment with OCA alone or in combination with the PPAR agonist bezafibrate which has shown synergistic benefits in PBC.
Results: We found that treatment with OCA improved motor neuron viability and neurite outgrowth in VCP iPSC-MNs. There was also an increase in metabolic function when treated in combination with bezafibrate.
Conclusion: Our data demonstrate that OCA protects motor neurons and therefore repurposing OCA has the potential to increase the therapeutic options for ALS irrespective of whether the disease is sporadic or familial.
MND05Adult SMA REACH: Characterisation of adult patients living with SMA at start of treatment
Elena Karkkainen1
, Jess Page1, Jose Verdu-Diaz1, Aleks Carver1, Grecia Alvarez1, Anisha Thomas1, Stephanie Tanner1, Jassi Michell-Sodhi1, Dionne Moat1, Robert Muni Lofra1, Chiara Marini Bettolo1.
The John Walton Muscular Dystrophy Research Centre, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK.
Elena.karkkainen@newcastle.ac.uk
Background: Spinal Muscular Atrophy (SMA) is a rare motor neuron disease. Disease progression of SMA may be improved by recent disease modifying therapies (DMT) now available for the adult population - Nusinersen and Risdiplam are available for the UK adult population through conditional Managed Access Agreement (MAA). MAA mandates collection of Real-world data (RWD) for final drug approvals in the UK through Adult SMA REACH. Adult SMA REACH is a multi-centre longitudinal observational data collection study that collects RWD during routine clinical visit across 18 different sites in the UK. The study includes patients aged ≥16 years with genetically confirmed 5q SMA.
Aims: The primary aim is to gain a comprehensive understanding of the demographic and clinical landscape of the adult SMA population at the start of treatment.
Methods/Materials: Descriptive analysis was conducted for categorical and continuous variables at baseline. Mean and standard deviation (SD) were summarised for continuous variables. Categorical variables were presented as count and percentage of occurrence. Number of patients for each variable was displayed as count and percentage.
Results: The overall population included 357 SMA patients with near-equal distribution of sex. SMA Type 3 was most common, comprising of 194 participants, followed by SMA Type 2 with 155 participants. SMA Type 1 was rarer with only 3 participants in the total cohort. There was no SMA Type 4 patients included in this analysis. WHO functional status categorised patients as: 35.0% as non-sitters, 45.7% as sitters and 19.3% as walkers at baseline.
The adult SMA population in the UK has a mean age at symptom onset of 3.59 years and mean age at diagnosis of 9.88 years. The adult SMA population had first access to DMT at the age of 34.5 years. Further analysis of physiotherapy assessments will be presented.
Conclusion: This analysis provides a comprehensive baseline characterisation of adults living with SMA in the UK at the start of treatment initiation. The findings empathise the importance of early diagnosis, timely intervention, and robust RWD frameworks to advance SMA care and improve outcomes.
MND06Adult SMA REACH: A real-world data collection study and ready-made infrastructure to support research and improvement initiatives in SMA
Jess Page1
, Elena Karkkainen1, Jose Verdu-Diaz1, Aleks Carver1, Grecia Alvarez1, Anisha Thomas1, Stephanie Tanner1, Jassi Michell-Sodhi1, Dionne Moat1, Robert Muni Lofra1, Chiara Marini Bettolo1.
The John Walton Muscular Dystrophy Research Centre, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK.
Jess.page@newcastle.ac.uk
Background: Adult SMA REACH a Research and Clinical Hub that established a collaborative clinical network in 2020 across 18 clinical sites in the UK, patient advocacy groups, regulators, and industry. It also established a longitudinal observational real-world data (RWD) collection study, collecting clinical data and outcome measures from adult SMA patients in the UK. SMA treatments Nusinersen and Risdiplam are available through Managed Access Agreements (MAA); Adult SMA REACH is responsible for capturing and reporting data to UK regulatory authorities to support their review of drug efficacy. The final data cuts for both MAA’s have now passed and Adult SMA REACH is in a position to grow; as a ready-made infrastructure to inform research questions in the UK, it is already currently supporting a number of initiatives.
Aims: The aims of Adult SMA REACH are to better understand the natural history of adult SMA, evolving phenotypes and the impact of new therapies.
Methods/Materials: Data is collected from clinical sites via a centralised online database. Using innovative data modelling techniques, we created an automated software for data validation, consistency checks, completeness analysis and treatment tracking. This allows us to continuously monitor evolving datasets, maximising the quality of collected data. Anonymised data can be provided to support research following submission of a data request which must receive approval from the steering committee.
Results: Data collected via Adult SMA REACH has supported research related to access to care; analysis of age at diagnosis, prevalence, and mortality; baseline characterisation of adults; and safety/efficacy analyses of available treatments. In addition to this, it is supporting the SMA Care UK initiative which aims to update and implement the Standards of Care for SMA patients. A pregnancy sub-study has also recently been established to characterise the effects of Nusinersen on pregnant women and the infants born to them.
Conclusion: Adult SMA REACH is a valuable infrastructure to support SMA research, ultimately optimising patient care, advancing therapy approvals and broadening the understanding of the disease.
MND07Seizures in patients with Spinal Muscular Atrophy (SMA) – correlation or coincidence?
Shira Rabinowicz1, Mariacristina Scoto1, Giovanni Baranello1, Adnan Manzur1, Francesco Muntoni1, Suresh Pujar2, Marios Kaliakatsos2, Pinki Munot1
1 Dubowitz Neuromuscular Centre, Great Ormond Street Hospital for Children, London, United Kingdom, 2 Clinical Neurosciences, Great Ormond Street Hospital for Children, London, United Kingdom
Background: Spinal Muscular Atrophy was previously considered a solely lower motor neuron disease, with no central nervous system involvement. However, as survival has changed dramatically with disease modifying treatments, the long-term phenotype of SMA patients is evolving, with concerns regarding additional axes of development.
Aim: We describe the incidence and characteristic of epilepsy in patients with SMA, to improve the understanding of this comorbidity.
Methods: We reviewed the charts of SMA patients followed up at the neuromuscular service at Great Ormond Street Hospital with concurrent diagnosis of seizures for demographics, clinical data and investigation results.
Results: we found four SMA patients who experienced seizures, first seizure at a median age of 6.5 years (range 2.5-12 years). Two patients with SMA1 and one patient with SMA2 had suspected focal seizures, and a patient with SMA 3 had suspected generalized seizures. Out of the patients with suspected focal seizures, one had semiology and EEG consistent with self- limited epilepsy with autonomic seizures, and one may be in keeping with self-limited epilepsy with centrotemporal spikes (although EEG was not done at sleep). One patient had bilateral temporal discharges in awake and sleep and general slowing of background.
For the three patients with likely focal seizures, brain MRI showed: atrophy (1), ventriculomegaly (1) and white matter and central tegmental signal hyperintensity (1). The patient with suspected generalized seizure had a normal exam.
SMA treatment at first seizure was: salbutamol, with an additional seizure after induction of Nusinersen (1), newly introduced Risdiplam post Nusinersen (1), 2-years post Nusinersen and Zolgensma (1) and treatment naïve (1). Two patients were initially treated with anti- seizure medications, and two were offered SOS benzodiazepines.
Conclusion: a few patients with SMA had seizures, 2/4 had SMA type 1. While seizures are common in the general population and some manifestations may be of common epilepsies, the comorbidity with the diagnosis or the newly introduced treatments is an issue for further research.
MND08Compassionate treatment for Spinal Muscular Atrophy with viral gene therapy – a single centre experience from India
Ramya Ramesh Babu1,2
, Madhuri Maganthi1, Ilin Kinimi 3, Dipanjana Datta4, Lakshmi K.S1, Joanne Ng5, Ann Agnes Mathew1,2.
1 Paediatric Neuromuscular services, Department of Paediatrics, Bangalore Baptist Hospital, Bangalore, India, 2 Synapse Neurocentre and Child Development Centre, Bangalore, India, 3 Manipal Hospital, Old Airport Road, Bangalore, 4 Institute of Child Health, Kolkata, India, 5 Gene transfer technology group, UCL EGA Institute for Women’s Health, London.
ramya.babu@nhs.net
Background: Spinal Muscular Atrophy (SMA), a monogenic autosomal recessively inherited disorder causes progressive muscle weakness. Onasemnogene abeparvovec (OA), a single dose gene replacement therapy (GT) was FDA-approved in May 2019 for the treatment of SMA.
Aims: This study describes the functional outcomes and safety profile of OA among 27 SMA affected children from a single centre in India.
Methods: 21/27 received OA through a global compassionate access programme and the remaining through crowdfunding between January 2021 and November 2022.
Their clinical details, serial motor assessments (using Hammersmith Infant Neurological Examination-2 [HINE-2] and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders [CHOP-Intend]) and laboratory parameters (platelets, liver enzymes and troponin I) were collected at baseline and latest till 12 months post GT. Oral steroid (Prednisolone) was initiated 24hours prior to scheduled dosing.
Results: 27 symptomatic SMA subjects (SMA1=13, SMA2=13, SMA3=1) received OA at our centre. The mean age of administration of GT was 12.2 months among SMA1 and 17.6 months among SMA2 cohort. Two SMA1 on long term ventilation succumbed at 2.5 months (de-escalation of care on parental request) and 10 months after GT (sudden respiratory failure). Among SMA1, the mean HINE-2 score improved by 2 and CHOP-Intend by 12 points from the baseline. The increase in mean motor scores were higher in the SMA2 cohort than SMA1 (HINE-2 by 4, CHOP-Intend by 12). The six-minute walking distance significantly improved in the SMA3 subject (250 metres from a baseline of 90 metres).
10/27 had thrombocytopenia, 1/27 had elevated Troponin I and all (100%) had transaminitis. The mean duration of steroid treatment was 21.36 weeks and 25.18 weeks among SMA1 & SMA2 respectively. One patient (SMA3) had subacute liver failure and received intravenous steroids.
Discussion: The functional outcomes were better in SMA2 than SMA1. SMA1 infants in our study received OA at a later age than SMA1 in other studies. We noticed a better recovery of transaminitis with early increment of steroids based on serial monitoring of liver enzymes. GT can be safely administered in resource limited settings with good functional outcomes while adhering to the standards of care.
Neuromuscular Junction Disorders and Channelopathies
NMJ&C01SCN4A loss of function zebra fish model : insights into congenital myopathy
Flavie Ader1
,2,3, Alan Pitman1, Emma Matthews4, Dan Osborn1
1 Cardiology and Genetics Research Institute, St George's University of London, Cranmer Terrace, London. SW17 0RE, 2 Sorbonne Université- DMU BioGem-Unité Fonctionnelle de Cardiogénétique et Myogénétique Moléculaire et cellulaire, Service de Biochimie Métabolique, APHP-Hôpital Universitaire Pitié Salpêtrière, Paris, France, 3 Université Paris Cité, UFR de Pharmacie, 4 av de l’observatoire, 75006 Paris, France, 4 Neurosciences and Cell Biology Research Institute, St George's University of London, Cranmer Terrace, London. SW17 0R
flavie.ader@aphp.fr
Background: SCN4A is a gene encoding for the muscular sodium channel. Bi-allelic loss of function (LOF) of SCN4A was identified as a cause of congenital myopathy. To date, no in vivo model recapitulates congenital myopathy due to SCN4A-LOF, and thus few hypotheses exist on the patho-mechanisms leading to this disease.
Aims: We have turned to the zebrafish to provide an in vivo model to assess SCN4A-LOF association with congenital myopathy.
Methods/Materials: We have used a CRISPR-mediated multiguide approach knockdown (scn4ab-KD) to generate the disease model, using 3 guide RNAs.
Results: The CRISPR mediated knockdown approach shown a cutting efficiency >79% confirmed by next generation sequencing and 10-20% of remaining expression of scn4ab transcript (qPCR and RNASeq data at 3 days port fertilization dpf). Early stages (3-5 dpf) data shown that death rate was similar between scn4ab-KD (0%, n=138) compared to controls (3% n=196), but rate of heart oedema was significantly higher in scn4ab-KD (21%, n=138) compared to controls (11%, n=196, p=0.008) at 3 dpf. No obvious morphological or muscle structure changes by birefringence (n=15 per condition) were observed. Cartilage staining revealed a tend for higher width/length ratio in scn4ab-KD (1.13+/- 0.05, n=16) comparing to control (1.08+/-0.07, p=0.1, n=10) at 5dpf.
Regarding the functional phenotyping, the scn4ab KD fishes presented a significant reduction of the distance moved (8437+/-5324mm, n=12) comparing to the control (13993 mm+/-4842mm, p=0.01, n=12) at 28dpf. Scn4ab-KD heartbeat always seated above controls from 5 to 28dpf (p= 0.001; scn4ab n=14 vs. control n=11 at 13dpf).
The molecular phenotyping (RNAseq at 3 dpf) evidenced 76 significantly upregulated genes and 33 significantly downregulated genes including unc45b, a myosin chaperone (confirmed by qPCR). Treatment of 2 dpf scn4ab-KD embryos by dichlorphenamide (0.5mg/mL) and acetazolamide (1mM) shown an increase of unc45b transcription level in preliminary data.
Conclusion: Scn4ab-KD model presents a progressive muscular defect in parallel as myosin profile changes, which could be linked with unc45b down-regulation. Interestingly, unc45b-LOF is associated with congenital myopathy and cardiac dysfunction. Our model is the first presenting a functional muscular defect and could provide useful new insights into the pathomechanisms of congenital myopathy, and could be used for drug testing.
NMJ&C02Pre-clinical trial of DOK7-AAV treatment for AChR deficiency CMS
Yin Yao Dong
, Leslie Jacobson, Richard Webster
Nuffield Department of Clinical Neurosciences, University of Oxford
Yin.dong@ndcn.ox.ac.uk
Background: Genetic variants resulting in the loss of muscle nicotinic acetylcholine receptor (AChR) surface expression is the most common cause of congenital myasthenic syndromes (CMS). Patients tend to respond well to cholinesterase inhibitor treatments like pyridostigmine, but long-term use at high doses can lead to loss of effectiveness. Salbutamol can restore the response to pyridostigmine, and lead to some further improvements. After treatment these patients tend to remain relatively stable, a significant number of them are still disabled to some extent even on optimised treatment.
We previously showed in our well-established mouse model of AChR deficiency CMS that high dose pyridostigmine leads to disruption of AChR clustering and neuromuscular junction (NMJ) structure. AChR clustering is normally mediated through the MUSK-DOK7 pathway, and previous studies have shown that DOK7-AAV treatment can lead to increased AChR clustering and enlarged NMJ.
Aims: Test whether DOK7-AAV can improve the myasthenic features of our mouse model of AChR deficiency CMS.
Method/materials: We test three doses of DOK7-AAV (2x1013, 6x1013 and 1x1014 vg/kg) in mice treated with 7mg/kg/day pyridostigmine, and compared them with untreated mice, those treated with pyridostigmine only, and those treated with pyridostigmine and salbutamol (45mg/kg/day). Mice weight and strength was tracked by fortnightly hang tests over six months. Electromyography was carried out on mice at the end of the study, and NMJ morphology was assessed by confocal microscopy posthumously. AAV biodistribution and DOK7 expression was assessed by digital-droplet-PCR
Results: DOK7-AAV at 6x1013 and 1x1014 vg/kg doses improved mice strength in comparison to pyridostigmine only treated mice, and untreated mice, but not significantly more so than pyridostigmine/salbutamol co-treated mice. The two higher doses of DOK7-AAV also significantly increased NMJ size, significantly more than all other groups.
Conclusions: DOK7-AAV treatment in combination with pyridostigmine improved AChR deficiency CMS, but not significantly more than pyridostigmine/salbutamol co-treatment.
NMJ&C03Usefulness of ColabFold and AlphaMissense for diagnosing congenital myasthenic syndromes?
Yin Yao Dong
1, 2
, Finlay Ryan-Phillips1, Leighann Henehan3, Sithara Ramdas2,4, Jacqueline Palace1,3, David Beeson1
1 Nuffield Department of Clinical Neurosciences, University of Oxford, 2 MDUK Neuromuscular Centre, Department of Paediatrics, University of Oxford, 3 Neurology Department, Oxford University Hospitals, 4 Department of Paediatric Neurology, Oxford University Hospital
Yin.dong@ndcn.ox.ac.uk
Background: Congenital myasthenic syndromes (CMSs) are caused by variants in >30 genes with increasing numbers of variants of unknown significance (VUS) discovered by next-generation sequencing. Establishing VUS pathogenicity requires in vitro studies that slow diagnosis and treatment initiation. The recently developed protein structure prediction software AlphaFold2/ColabFold has revolutionized structural biology; such predictions have also been leveraged in AlphaMissense, which predicts ClinVar variant pathogenicity with 90% accuracy. However, few reports have tested these tools on rigorously characterized clinical data.
Aims: Evaluate the accuracy of ColabFold and AlphaMissense for predicting the pathogenicity of missense variants in CHRN genes.
Methods/materials: Utilizing a dataset of 61 clinically validated CHRN variants, (1) we evaluated the possibility of a ColabFold metric (either predicted structural disruption, prediction confidence, or prediction quality) that distinguishes variant pathogenicity; (2) we assessed AlphaMissense’s ability to differentiate variant pathogenicity; and (3) we compared AlphaMissense to the existing patho-genicity prediction programs AlamutVP and EVE.
Results: Analyzing the variant effects on ColabFold CHRN structure prediction, prediction confidence, and prediction quality did not yield any reliable pathogenicity indicative metric. However, AlphaM-issense predicted variant pathogenicity with 63.93% accuracy in our dataset — a much greater proportion than AlamutVP (27.87%) and EVE (28.33%).
Conclusions: Emerging in silico tools can revolutionize genetic disease diagnosis, but improvement, refinement, and clinical validation are imperative prior to practical acquisition.
NMJ&C04SLC25A1 associated Congenital Myasthenic Syndrome – A case series
Jane Kung
1
, Emma Clement1, Jacqueline Palace2, Sithara Ramdas2, Leighann Henehan2, Yin Dong2, Iain Horrocks2, Maria Vanegas3, Sespoina Mandelenaki3, Hugh Lemonde3, Heinz Jungbluth3, Pinki Munot1
1 Great Ormond Street Hospital, London, UK, 2 John Radcliffe Hospital, Oxford, UK, 3 Evelina Children’s Hospital, London, UK
jane.kung@gosh.nhs
Background: Congenital myasthenic syndromes (CMS) are a clinically and genetically heterogeneous group of disorders caused by mutations which lead to impaired neuromuscular transmission. The SLC25A1 gene encodes the mitochondrial citrate transporter, a protein that belongs to the solute carrier family 25 (SLC25). This transporter is primarily involved in moving citrate and other tricarboxylates across the mitochondrial membrane.
Mutations in SLC25A1 have primarily been associated with combined D-2- and L-2-hydroxyglutaric aciduria, a rare metabolic disorder with early onset severe disease but a milder CMS phenotype has also been described.
Aims: We aim to describe the clinical phenotype of six individuals with SLC25A1 associated CMS.
Methods/Materials: Participants with SLC25A1 disorder were identified from clinician CMS database. Data was retrospectively collected from records on clinical presentation, investigations, treatment efficacy on 6 individuals (age 4-45 years; 50% female).
Results: We describe six cases from five families. The median age at presentation was 6.8 months (range 0.3 – 18 months) and at diagnosis 9.1 years (range 4 – 34 years).
Clinical features include ptosis, seen in all. Seizures were noted in 4/6 (67%). All had learning difficulties. 4/6 (67%) were ambulant. Fatigue was a prominent feature in those ambulant
.
Ataxia or balance issues was seen in 2/6 (33%). No respiratory difficulties were seen in any. Paediatric Intensive Care Unit (PICU) admission in two, for seizures and cardiorespiratory arrest.
Biochemical abnormality in urine (L-2-hydroxyglutaric aciduria) was seen in three cases, not tested in one. Neuromuscular transmission studies were abnormal in two, not performed in one and yet to be performed in two. Brain MRI was abnormal in one, pending review in another. Genetic confirmation in all was by genome sequencing.
Three responded to treatment with pyridostigmine, two are awaiting treatment and one not trialled.
Conclusion: We demonstrate that SLC25A1 associated CMS can present early with symptoms involving the brain such as epilepsy and learning difficulties. Targeted investigation and treatment should be incorporated early into SLC25A1 diagnosis and management.
NMJ&C05Rituximab in Juvenile Myasthenia Gravis: A single-centre case series
Emma Scott1, Louise Hartley2, O Martineau1,
Munot P
1
1Dubowitz Neuromuscular Centre, Great Ormond Street Hospital, London WC1N 3JH UK, 2Department of Paediatric Neurology, The Royal London Hospital, London E1 1BB, United Kingdom
Background: Juvenile myasthenia gravis (JMG) is a rare autoimmune disorder marked by weakness due to autoantibodies targeting the neuromuscular junction, most commonly acetylcholine receptor (AChR) and muscle-specific kinase (MuSK) antibodies. Refractory cases present therapeutic challenges despite standard treatments. Rituximab, a B-cell-depleting monoclonal antibody, has emerged as a potential therapy in adult myasthenia gravis, yet its paediatric applications remain underexplored.
Aim: To describe the efficacy and tolerability of Rituximab in eight girls with antibody-positive JMG
Methods: This case series includes 8 girls (ages 8–16 years) with refractory JMG treated at a single centre with Rituximab after failing conventional therapies, including corticosteroids and immunosuppressants. Baseline and follow-up assessments included Myasthenia Gravis Activities of Daily Living (MG-ADL) scores, corticosteroid doses, and adverse events.
Results: Five girls with AChR antibodies and three with MuSK antibodies were included. 6/8(75%) girls demonstrated significant clinical improvement. MG-ADL scores decreased significantly, with the greatest reduction observed in MuSK-positive patients. Steroid-sparing effects were achieved in 6 cases, with three Musk patients benefitting the most. Pharmacological remission was achieved in 6 patients (3 AChR-positive, 3 MuSK-positive). In the remaining, one was refractory with no response and one had an allergic response and infusion was abandoned. Rituximab was well-tolerated in the remaining. Redosing was needed in all that responded.
Conclusion: Rituximab was effective and well-tolerated in this series with refractory JMG, including both AChR- and MuSK-positive cases. These findings highlight its potential as a targeted therapy for antibody-mediated JMG.
NMJ&C06Profile time course of motor unit regeneration and stability following administration of Smn-upregulating therapeutics
I Partlova1,2
L H Comley1,2, L M Murray1,2
1 Centre for Discovery Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom, 2 Euan McDonald Centre for Motor Neuron Disease Research, University of Edinburgh, Edinburgh, United Kingdom
I.Partlova@sms.ed.ac.uk
Background: Despite the availability of therapeutic options for SMA, impactful deficits persist in affected patients even after pre-symptomatic treatment. A hallmark of motor unit pathology in SMA involves the loss of motor neurons and disruption of neuromuscular junctions (NMJs).
Aims: To determine what deficits remain following treatment with an Smn up-regulating drugs over time and how to develop combinational therapeutics to target such deficits.
Methods: Here we have analysed NMJ recovery following early (PD2) administration of Nusinersen in the SMNΔ7 mouse model. We have employed the mouse cranial muscles which facilitate whole mount analysis of a group of differentially vulnerable motor units. The analysis was conducted on cranial muscles aged P6, P12 and P18 – analysing parameters including axon number, endplate number and motor unit size. Additionally, analysis of sprouting, poly innervation, endplate size and maturity was conducted to provide a comprehensive picture of regeneration and stability of the NMJ following early Nusinersen in the SMNΔ7 mouse model.
Results: Treatment with Nusinersen significantly improved innervation of endplates at the NMJ compared to untreated littermates, even in the most vulnerable muscles. The vast majority of endplates were fully occupied at all time points analysed following treatment. However, there was an underlying loss of endplates in the most vulnerable muscles, which could mask denervation. Numbers of intramuscular axons innervating the most vulnerable muscles were also reduced from the P6 time point onwards. The loss of axons coupled with stabilisation in endplate innervation gave rise to a profound increase in motor unit size, which could have implications for the health of the remaining axons over time. This work suggests that Nusinersen treatment rescues some but not all parameters of neuromuscular pathology in this mouse model of SMA, and reveals important deficits in motor unit recovery following an increase in SMN levels .
Conclusion: This study emphasizes the regenerative potential of motor neurons following Smn restoration but stresses that recovery is incomplete. This is particularly highlighted in the progressive decline of axon number, which increases the motor unit size over time.
‡NMJ&C07Mexiletine versus lamotrigine in Non-Dystrophic myotonias – a randomised, double-blinded, cross-over trial
Vinojini Vivekanandam
1
,2, Iwona Skorupinska1, Louise Germain1, Dipa Jayseelan1, Emma Matthews3, Richard Barohn4, Michael P McDermott5, Michael G Hanna1,2
1The National Hospital for Neurology and Neurosurgery, Queen Square, 2CNMD, Queen Square UCL Institute of Neurology, 3Neurosciences and Cell Biology Research Institute, St George’s University of London, 4University of Missouri, 5University of Rochester Medical Center
Background: Non-dystrophic myotonias are genetic conditions that cause significant morbidity and impairment of quality life in a young cohort. Myotonia is experienced as stiffness, cramps, falls, fatigue and pain. There is currently no cure or disease-modifying treatment for Non-dystrophic myotonias. Sodium channel blockers are used for symptomatic relief. Symptomatic treatments are life-altering for affected patients. A previous international, multi-centre randomised, placebo-controlled study as well as subsequent studies, have shown that mexiletine is effective in reducing myotonia and improving quality of life. Mexiletine has been the mainstay of treatment for the last 20 years. Lamotrigine has more recently been shown to be effective in a randomised controlled trial. This poses clinical equipoise regarding the most effective and first line treatment of myotonia.
Aims: We performed a phase III, randomised, double-blinded, cross-over, non-inferiority trial to compare lamotrigine and mexiletine head-to-head.
Methods: Participants had genetically confirmed symptomatic Non-dystrophic myotonia. Participants were randomised to receive either mexiletine for 8 weeks followed by lamotrigine for 8 weeks, or lamotrigine followed by mexiletine with appropriate washout. The primary outcome measure was the interactive voice response diary (IVR-diary) stiffness score (0-9 scale) and non-inferiority was assessed with a predefined margin of 0.5.
Results: Sixty participants were enrolled. We were not able to show that lamotrigine was non-inferior to mexiletine. The mean mexiletine-lamotrigine difference in IVR-diary stiffness score was -0.09 (95% CI -0.58 to 0.39). However, improvements from baseline in stiffness scores and all secondary outcome measures were comparable between mexiletine and lamotrigine - the mean IVR stiffness score reduced from 5.3 at baseline, to 2.52 with mexiletine and 2.62 with lamotrigine. The most common adverse event was indigestion/reflux with both treatments. No serious adverse events were seen.
Conclusion: Importantly, improvements in all outcome measures from baseline were comparable between lamotrigine and mexiletine. As such, lamotrigine is a key consideration in the treatment algorithm of Non-dystrophic myotonias. We discuss a treatment approach considering the trial results, local economics, patient needs and pharmacokinetics.
NMJ&C08A novel mouse model of fast channel congenital myasthenic syndrome: Initial characterisation
Richard Webster, Yin Dong
Nuffield Department of Clinical Neurology, University of Oxford, UK
richard.webster@imm.ox.ac.uk
Background: Congenital Myasthenic Syndromes (CMS) are a heterogenous group of disorders affecting neuromuscular transmission and are characterised by fatigable muscle weakness. One of the most severe subtypes in the UK is Fast Channel CMS (FCCMS) that is largely resistant to current treatments. FCCMS is caused by genetic variants in muscle nicotinic acetylcholine receptor (AChR) genes that reduce channel activity, leading to failed neurotransmission. In the UK, it is most commonly caused by the CHRNE p.Pro141Leu variant either homozygously, or compound heterozygous with a variant that reduces AChR expression. No animal model of FCCMS has been reported.
Aims: Here we describe the initial characterisation of an FCCMS mouse model created by MRC GEMM program who inserted the p.Pro141Leu variant into mouse Chrne (εP141L).
Results: Homozygous εP141L model mice were generated at expected ratios from heterozygous parents. Their initial growth profile was identical to heterozygous and wildtype (WT) littermates and showed no phenotype. However, by postnatal day 14 (P14) all model mice began to grow more slowly, from P15 pups lost weight and rapidly declined. Pups were culled by P17 as the humane endpoint for 15% weight loss was reached. At P17 model mice averaged 6.1 g, ∼79 % of WT littermates (n=7). Initial fluorescence microscopy of P16 diaphragms revealed neuromuscular junction morphology indistinguishable from age-matched WT, with robust staining for AChR.
Electrophysiological characterisation of neurotransmission on P15-17 model diaphragms (n=7) showed dramatically reduced miniature end plate potential (mEPP) amplitude, frequency and EPP amplitude compared to WT (n=4) but enhanced quantal content. mEPPs had prolonged duration but reduced area. The size and duration of mEPPs in model mice is analogous to neurotransmission utilising foetal AChR. Interestingly, heterozygous mice (n=3) also had modestly reduced mEPP amplitude and EPP amplitude but mEPP frequency, quantal content and mEPP duration was unchanged compared to WT.
Conclusion: We conclude that this model of FCCMS generated viable mice that demonstrates measurable deficit in neurotransmission. Further studies will determine if current and novel therapies for FCCMS can modify the disease phenotype. Development of this model will aid in our search for better therapies for this difficult to treat neuromuscular disorder.
Dystrophy (Pre-clinical)
D01The role of CRISPR/Cas9 in revolutionizing Duchenne muscular dystrophy treatment: opportunities and obstacles
Ahsan Ali, Md Yakeen Rahman, Danish Sheikh
ahsan.ali.md@outlook.com
https://pubmed.ncbi.nlm.nih.gov/39583121/
Background: Duchenne muscular dystrophy (DMD) is a severe X-linked disorder impacting approximately 1 in 3,500 male births globally. It is characterized by progressive muscle wasting and premature mortality, caused by mutations in the dystrophin gene. Current treatments remain largely palliative, emphasizing the urgent need for innovative curative therapies. CRISPR/Cas9 gene-editing technology presents a revolutionary opportunity to address the genetic root cause of DMD.
Aims: This study reviews the transformative potential of CRISPR/Cas9 for DMD treatment, assessing advancements in preclinical models and addressing obstacles for clinical application.
Methodology & Theoretical Orientation: The review synthesizes data from key scientific publications focusing on CRISPR-mediated dystrophin restoration, as well as advancements in related gene-editing technologies such as base and prime editing. Specific emphasis is placed on developments in delivery systems, such as lipid nanoparticles and exosome-based platforms, and improvements in gene-editing fidelity through high-accuracy Cas variants.
Results: Preclinical models demonstrate CRISPR/Cas9’s ability to restore dystrophin expression and improve muscle function. Notable challenges include optimizing delivery systems for broad muscle targeting and ensuring the safety and efficacy of long-term applications. High-fidelity Cas9 variants and novel delivery systems show promise in overcoming these barriers.
Conclusion & Significance: CRISPR/Cas9 offers a groundbreaking approach to treating DMD by addressing its genetic cause. While significant strides have been made in preclinical settings, transitioning to human applications requires overcoming hurdles in delivery, precision, and long-term safety. Continued innovation in genome-editing technology could redefine DMD treatment and provide a model for addressing other genetic disorders.
Keywords: CRISPR/Cas9, Duchenne muscular dystrophy, gene editing, gene therapy, preclinical models
Biography: Ahsan Ali is a dedicated 5th-year medical student at Plymouth University, Peninsula Medical School, with a passion for genetic medicine and innovative therapies. His academic journey has been marked by a keen interest in molecular biology and translational research. Collaborating with esteemed peers and mentors, Ahsan has focused on understanding the transformative potential of CRISPR/Cas9 technology in addressing rare genetic disorders like Duchenne muscular dystrophy. His work synthesizes cutting-edge developments in gene-editing tools and delivery mechanisms to provide actionable insights into clinical translation. Beyond his academic pursuits, Ahsan actively participates in science communication and aspires to contribute to the broader field of personalized medicine.
Image Example:

Figure 1: Abstract representation of muscle tissue comparison between healthy individuals and those affected by Duchenne Muscular Dystrophy (DMD). On the left, the healthy muscle tissue is depicted as evenly aligned, organized lines symbolizing intact muscle fibers. On the right, the DMD-affected muscle tissue shows irregular, broken lines, representing the disorganized and degenerating muscle fibers characteristic of DMD progression
D02Advanced modelling of human muscle stem cell transplantation using deep neural networks and 3D engineered skeletal muscles
SungWoo Choi1,2
, Kevin Cheng1,2, Francesco Saverio Tedesco1,2,3
1.The Francis Crick Institute, London UK, 2.Department of Cell and Developmental Biology, University of College London, London UK, 3.Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health & Great Ormond Street Hospital for Children, London UK.
Presenting author: sungwoo.choi.16@ucl.ac.uk
Corresponding author: f.s.tedesco@ucl.ac.uk
Background: Several animal models of muscular dystrophy have been utilised to evaluate safety and efficacy of skeletal myogenic cell transplantation for cell therapies. Whilst the complexity of in vivo models provides anatomical and immunological similarities to humans, results obtained in animal models (including large animals) have so far not predicted the limited efficacy observed in clinical studies. This limitation has been attributed to several factors, including: 1) the high regenerative capacity of murine models; 2) lack of species specificity due to xenogenic barriers; 3) limited scalability of performing screens for therapies due to ethical concerns.
Aims: In this study, we aimed to develop an in vitro model of human myogenic cell transplantation into isogenic human engineered muscles, coupled with automated image analysis pipelines to quantify critical variables necessary for successful myogenic transplantation as well as contractile properties of host tissues.
Methods: To this aim, we transplanted fluorescently labelled myogenic stem/progenitor cells into acutely injured, isogenic engineered skeletal muscles. Migration of transplanted cells was initially monitored using stereomicroscopy for 10 days post-transplantation. Subsequently, the contribution of transplanted cells to host muscles was analysed using custom deep learning segmentation algorithms to perform instance segmentation of nuclei and myotubes.
Results: This revealed that the donor cells were able to effectively migrate and spread throughout the host engineered muscle as well as generate highly striated, donor-derived muscle fibres fused with host fibres. To assess the functional contribution of donor cells, we stimulated artificial muscles with electrical stimuli. The contractile property of muscles was evaluated using an analysis pipeline combining neural network-based image segmentation and optical velocity analysis. Contractility analysis revealed that engineered skeletal muscles transplanted with donor cells demonstrated significantly increased contractile properties suggesting functional integration of donor cells.
Conclusions: To conclude, we developed automated pipelines for the analysis of morphological features and contractility in human bioengineered muscles. We provide proof-of-concept results that suggest that transplantation of muscle stem cells onto artificial muscles facilitates contribution of donor cells to the contractile apparatus of host muscles to enhance contractile strength. This platform is automated and disease- and treatment-agnostic, which can potentially allow for application in future screens for cell and gene therapies within this humanised system.
D03Dissecting the composition of the extracellular matrix in sarcoglycanopathies
James Clark1, Esther Fernández-Simón1, Elisa Villalobos Villegas1, Rasya Gokul Nath1, Alexandra Monceau1, Panos Katsikis1, Catherine Collins1, Priyanka Mehra1, Lidia Matias Valiente1, Zoe Laidler1, Andrew Galloway1, Dan Cox1, Pawel Palmowski2, Andrew Porter2, Jordi Diaz Manera1
1 John Walton Muscular Dystrophy Research Centre, Newcastle University, Newcastle, UK, 2 Newcastle University Protein and Proteome Analysis, Newcastle University, Newcastle, UK
James.clark4@newcastle.ac.uk
Background: Sarcoglycanopathies are a group of genetic disorders affecting the sarcoglycan complex, a vital component in sarcolemmal stability, preventing muscle damage. Characterised by a progressive weakening of the muscles, primarily in the limb girdles, these recessive disorders are variable in severity but have a meaningful impact on patient quality of life and longevity. The extracellular matrix (ECM) is central in the protection and repair of muscle under normal circumstances. The aberrant deposition of fibrotic tissue leads to stiffness and contractures in patients. Drugs are being developed with the aim of controlling this fibrosis. Antifibrotic drugs may be useful in managing the symptoms of muscular dystrophies, here we investigate the effects of the antifibrotic drug Nintedanib on the ECM in a sarcolgycan mouse model.
Aims: To elucidate changes in the protein of the ECM in the disease state using a murine sarcoglycan alpha knockout (SGCA -/-). Determine the effect of Nintedanib, an antifibrotic drug, on the effect of fibrosis in the model.
Methods/Materials: 6 individuals from each condition, wildtype (WT), SGCA -/- with no treatment (NT) or SGCA -/- with Nintedanib treatment (TR) were used in the study. Muscle was harvested from the animals and decellularized using a series of washes and detergents. The decellularized material was submitted to mass spectrometry analysis to determine protein content. ECM proteins in the three groups were compared, and significantly altered ECM proteins were identified for additional investigation.
Results: We identified 58 significantly differentially expressed matrisomal proteins between the SGCA -/- mice and the WT. Nintedanib treatment meant that 39 (67%) of these ECM proteins no longer showed a significant overexpression compared to the WT group. Treatment also appears to significantly increase the expression of some proteins that regulate or reduce ECM production.
Conclusion: Nintedanib alters the protein composition of the ECM in SGCA -/- mice. It decreases the overexpression of some ECM proteins and promotes ECM regulatory proteins, an additional mechanism reducing the fibrotic phenotype seen in sarcoglycanopathies, a hallmark of many muscular dystrophies. Understanding how the disease affects matrix proteins and adjusting the composition may prove useful in managing symptoms of muscular dystrophies.
D04A CCG expansion in ABCD3 causes oculopharyngodistal myopathy in individuals of European ancestry
Riccardo Curro2,1
, Sarah J Beecroft3,4, Stefano Facchini2,1, Macarena Cabrera-Serrano3, Igor Stevanovski5,6, Sanjog Chintalaphani5,6, Hasindu Gamaarachchi5,6,7, Ben Weisburd8, Chiara Folland3,4, Gavin Monahan3,4, Carolin K Scriba3, Lein Dofash3,4, Mridul Johari3,4, Bianca R Grosz9,10, Melina Ellis9,10, Liam G Fearnley11,12, Rick Tankard13, Justin Read14,15, Ash Merve16, Natalia Dominik1, Elisa Vegezzi17, Ricardo P Schnekenberg2,1, Gorka Fernandez18, Marion Masingue18, Diane Giovannini19, Martin Delatycki14,15, Elsdon Storey20, Mac Gardner21, David Amor14,15, Garth Nicholson9,22, Steve Vucic10,23, Robert D Henderson24,25, Thomas Robertson26,27, Jason Dyke28,29, Vicki Fabian28, Frank Mastaglia30, Mark R Davis31, Marina Kennerson9,10,22, Ros Quinlivan32, Simon Hammans33, Liam Carroll33, Arianna Tucci34, Melanie Bahlo11,12, Catriona A McLean35,36, Nigel G Laing3,30, Tanya Stojkovic18, Ira Deveson5,6, Paul J Lockhart14,15, Phillipa J Lamont37, Michael C Fahey38, James Lilliker43, Robert Pitceathly1, Pedro Machado1, Stefen Brady40, Mary M Reilly1, Volker Straub41, Giselle Bonne59, Henry Houlden1, Michael G Hanna1, Enrico Bugiardini1, Gianina Ravenscroft3,4 for the OPDM study group,
Andrea Cortese1,2
,
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, United Kingdom, 2Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy, 3Harry Perkins Institute of Medical Research, Nedlands, WA, Australia, 4Centre for Medical Research, University of Western Australia, Nedlands, WA, Australia, 5Genomics Pillar, Garvan Institute of Medical Research, Sydney, NSW, Australia, 6Centre for Population Genomics, Garvan Institute of Medical Research and Murdoch Children's Research Institute, Sydney, New South Wales, Australia, 7School of Computer Science and Engineering, University of New South Wales, Sydney, NSW, Australia, 8Program in Medical and Population Genetics, Broad Institute of MIT and Harvard, Cambridge, MA, USA, 9Northcott Neuroscience Laboratory, ANZAC Research Institute, Sydney, NSW 2139, Australia, 10Faculty of Medicine and Health, University of Sydney, Sydney, NSW 2006, Australia, 11Population Health and Immunity Division, The Walter and Eliza Hall Institute of Medical Research, 1G Royal Parade, Parkville, VIC 3052, Australia, 12Department of Medical Biology, The University of Melbourne, 1G Royal Parade, Parkville, VIC 3052, Australia, 13Department of Mathematics and Statistics, Curtin University, Perth, Western Australia, Australia, 14Bruce Lefroy Centre, Murdoch Children’s Research Institute, Parkville, VIC, Australia, 15Department of Paediatrics, University of Melbourne, Royal Children’s Hospital, Parkville, VIC, Australia, 16Department of Neuropathology, National Hospital for Neurology and Neurosurgery, London, United Kingdom, 17IRCCS Mondino Foundation, Pavia, Italy, 18Nord/Est/Ile-de-France Neuromuscular Reference Center, Institute of Myology, Pitié-Salpêtrière Hospital, APHP, Paris, France, 19CHU Grenoble Alpes, Grenoble Institut Neurosciences, INSERM, U1216, Université Grenoble Alpes, Grenoble, France, 20Neurology Department, The Alfred Hospital, Melbourne VIC, Australia, 21The Laboratory for Genomic Medicine, University of Otago, Dunedin, New Zealand, 22Molecular Medicine Laboratory, Concord Repatriation General Hospital, Sydney, NSW 2139, Australia, 23Brain and Nerve Research Centre, Concord Repatriation General Hospital, Sydney, NSW 2139, Australia, 24Department of Neurology, Royal Brisbane & Women's Hospital, Herston, QLD, Australia, 25UQ Centre for Clinical Research, Herston, QLD, Australia, 26Pathology Queensland, Royal Brisbane and Women’s Hospital, Herston, QLD, Australia, 27School of Biomedical Sciences, The University of Queensland, St Lucia, QLD, Australia, 28PathWest Neuropathology, Royal Perth Hospital, Perth, WA, Australia, 29School of Medicine and Pharmacology, University of Western Australia, Crawley, WA, Australia, 30Perron Institute for Neurological and Translational Science, Nedlands, WA, Australia, 31Neurogenetics Unit, Diagnostic Genomics, PathWest, Nedlands, WA, Australia, 32Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health & MRC Centre for Neuromuscular Diseases, London, United Kingdom, 33Wessex Neurological Centre, University Hospital Southampton, Southampton, United Kingdom, 34William Harvey Research Institute, Faculty of Medicine and Dentistry, Queen Mary University of London, London, United Kingdom, 35Department of Medical Biology, The University of Melbourne, Parkville, Victoria, Australia, 36Department of Anatomical Pathology, Alfred Hospital, Melbourne, Victoria, Australia, 37Neurogenetics Unit, Royal Perth Hospital, Perth, WA, Australia, 38Department of Paediatrics Monash Children's Hospital, Victoria, Australia, 39Manchester Centre for Clinical Neurosciences, Salford Royal Hospital, Northern Care Alliance NHS Foundation Trust, Manchester, United Kingdom, 40Oxford Muscle Service, John Radcliffe Hospital, Level 3, West Wing, Oxford OX3 9DU, United Kingdom, 41John Walton Muscular Dystrophy Research Centre Newcastle University Translational and Clinical Research Institute and Newcastle Hospitals NHS Foundation Trust Newcastle upon Tyne, United Kingdom
andrea.cortese@ucl.ac.uk
Background: Oculopharyngodistal myopathy (OPDM) is an inherited myopathy manifesting with ptosis, dysphagia and distal weakness. Pathologically it is characterised by rimmed vacuoles and intranuclear inclusions on muscle biopsy. In recent years CGG • CCG repeat expansion in four different genes were identified in OPDM individuals in Asian populations. None of these have been found in affected individuals of non-Asian ancestry.
Aims: aim of this study was to identify the cause of OPDM in patients of European ancestry
Methods: genotype arrays, short and long read sequencing, muscle pathology, RNAseq and fluorescence in situ hypbrididization (FISH).
Results: In this study we describe the identification of CCG expansions in ABCD3, ranging from 118 to 694 repeats, in 35 affected individuals across eight unrelated OPDM families of European ancestry. ABCD3 transcript appears upregulated in fibroblasts and skeletal muscle from OPDM individuals, suggesting a potential role of over-expression of CCG repeat containing ABCD3 transcript in progressive skeletal muscle degeneration.
Conclusions: The study provides further evidence of the role of non-coding repeat expansions in unsolved neuromuscular diseases and strengthens the association between the CGG • CCG repeat motif and a specific pattern of muscle weakness.
D05Myostatin is a marker of disease severity in Facioscapulohumeral dystrophy
J. Dumonceaux1
, S. Sohn 1, P. Jones2, S. Arbogast3*, D. Laoudj-Chenivesse4 and V. Mariot1
1NIHR Biomedical Research Centre, University College London, Great Ormond Street Institute of Child Health and Great Ormond Street Hospital NHS Trust, London, UK, 2University of Nevada, Reno, School of Medicine, Department of Pharmacology, 1664 N. Virginia St., Reno, NV 89557, United States, 3PhyMedExp, Université de Montpellier, INSERM, CNRS, Montpellier, France, 4PhyMedExp, Université de Montpellier, INSERM, CNRS, Montpellier, Department of Clinical Physiology, CHU of Montpellier, Montpellier, France
j.dumonceaux@ucl.ac.uk
Background: Facioscapulohumeral muscular dystrophy (FSHD) is primarily caused by aberrant expression of the toxic transcription factor DUX4. Recent advances have led to the development of therapeutic strategies targeting DUX4, including small molecules, antisense oligonucleotides, and gene therapy vectors, with 2 clinical trials currently underway. However, a significant challenge in the FSHD field is the difficulty in measuring DUX4 expression in patient biopsies, which complicates both disease monitoring and therapy development. While circulating biomarkers could provide a quantitative and robust measure of disease severity and therapeutic efficacy, none are currently available.
Aims: This study aimed to evaluate myostatin (MSTN) as a potential biomarker for FSHD disease severity and therapeutic monitoring.
Methods: We used the ACTA1-MCM;FLExDUX4/+ mouse model, which exhibits chronic and mosaic DUX4 expression, and develops an FSHD-like pathology over time. Mstn expression was measured at the mRNA level in muscle and protein level in blood. We then analyzed serum MSTN levels in FSHD patients and healthy controls, followed by larger analysis of serum from 51 FSHD patients using ELISA. The correlations between MSTN levels and clinical severity scores were evaluated.
Results: In mice expressing DUX4, Mstn expression was significantly lower at both the mRNA and circulating protein levels compared to controls, with further decreases observed as the disease progressed. In FSHD patients, MSTN levels were approximately two-fold lower than in healthy controls. In the larger patient cohort, MSTN levels strongly inversely correlated with clinical severity scores, with the clinical severity showing the most robust correlation (p = 9 × 10−1).
Conclusion: Our findings suggest that MSTN could be a reliable biomarker for FSHD disease severity and progression.
‡D06Cellular mapping of DMD transcript in human myogenic cells and skeletal muscle by RNA in situ hybridization and multiphoton imaging
Alessandra Ferlini1
, Martina Mietto1, Silvia Montanari1, Maria Sofia Falzarano1, Riccardo Scodellaro2, Frauke Alves2
1 Unit of Medical Genetics, Department of Medical Sciences, University of Ferrara, Ferrara, Italy; 2 Translational Molecular Imaging, MPI for Multidisciplinary Sciences, Max Planck Institute, Göttingen, Germany.
fla@unife.it
Background: Duchenne muscular dystrophy (DMD) is a severe X-linked neuromuscular rare disease (1 in 5000 males) due to pathogenic variations in the dystrophin (DMD) gene, which lead to the reduction or absence of dystrophin protein (DYS). Several gene corrective strategies are ongoing to restore dystrophin protein, and some published results highlight success and failure.
Aims: Despite many therapies target RNA and/or are related to the gene transcription, the precise mechanisms underlying DMD transcript dynamics and spatial expression are unknown, so we aimed at exploring these processes in DMD cells and muscle biopsies.
Methods/Materials: We used RNAscope assay and multiphoton imaging to characterize DMD gene transcription dynamics and spatial localization in DMD myogenic cells and skeletal muscles.
Results: We showed a dramatic decrease of DMD mRNA in the cytoplasmic fraction, while a massive amount of DMD transcript is retained in the nucleus (up to 90%) and co-localized with nucleoli. This leads to severe unbalanced transcript spatial distribution with poor or absent mRNA availability in cytoplasm. Multiphoton imaging was combined to RNAscope assay (Figure 1) to further define the muscular spatial localization of both collagen and DMD transcripts. (A) shows an image of RNAscope exons 37-42 probe on DMD muscle tissue, B) reports the Second Harmonic Generation (SHG) signal scattered by collagen in the same biopsy, (C) depicts the output of the elastic registration procedure of (A) and (B). Red squares in (A), (B) and (C) highlight the same regions of interest, whose zoom is (D), (E) and (F), respectively. We preliminary demonstrated that, using artificial intelligence (AI), collagen-related morphological properties differently correlate to mutated DMD transcripts localization in DMD muscle biopsies.
Conclusion: Our data provide evidence that the DMD mature transcript export fails and both heterogenous RNA (hnRNA) and mRNA accumulate in the nucleus. The combined RNAscope-multiphoton imaging approach allowed to define a changed collagen morphology associated with the mutated transcript and might be used as a novel ex-vivo or even in-vivo RNA-imaging biomarker tool.
Figure 1

‡D07Investigating the role of EGFR signalling in muscle dystrophies: Implications for Duchenne muscular dystrophy
E. Fernández-Simón*
1, Ainoa Tejedera-Villafranca2, Xiomara Fernández-Garibay2, James Clark1, Alexandra Monceau1, Elisa Villalobos1, Dan Cox1, Javier Ramón Azcón2,3, Juan M. Fernández-Costa2, Jordi Diaz Manera1
1 John Walton Muscular Dystrophy Research Centre, Institute of Genetic Medicine; Newcastle University, UK, 2 Institute for Bioengineering of Catalonia (IBEC), The Barcelona Institute of Science and Technology (BIST); C/Baldiri Reixac 10-12, E08028 Barcelona, Spain, 3 Institució Catalana de Recerca i Estudis Avançats (ICREA); Passeig de Lluís Companys, 23, E08010 Barcelona, Spain.
*Esther.fernandez-simon@newcastle.ac.uk
Background: The degeneration of muscle in muscular dystrophies involves complex interactions among different cell types. Fibroadipogenic progenitor cells (FAPs) support muscle regeneration under healthy conditions; however, in muscle dystrophies, FAPs contribute to fibrosis and adipogenesis, promoting the increase of fibrotic and fat tissue.
Aim: This study aims to investigate the dysregulation of molecular pathways, specifically epidermal growth factor (EGF) signaling, in Duchenne muscular dystrophy (DMD) muscle samples compared to healthy controls. The study further explores the roles of EGF and EFEMP1 signaling in FAPs and myoblasts in vitro.
Materials&Methods: Datasets from single-nuclei RNA sequencing (snRNAseq) of DMD muscle samples were analyzed to identify alterations in molecular pathways. In vitro experiments were conducted to assess the effects of EGF and EFEMP1 on FAPs and myoblasts, including their impact on myotube size, fibrotic differentiation, and muscle strength.
Results: The analysis revealed that EGF signaling is upregulated in DMD muscle, driven by increased expression of the ligands EGF and EFEMP1. EFEMP1, which is secreted by FAPs in DMD, was found to increase myotube size without enhancing muscle strength. In contrast, EGF promoted fibrotic differentiation in FAPs and induced the formation of smaller, proliferative myotubes in myoblasts, contributing to a fibrotic and dysfunctional muscle phenotype. The observed differences in cellular effects between the two ligands were attributed to different receptor interactions, with EGF activating both EGFR and ErbB2, while EFEMP1 selectively maintained ErbB4 in an inactive state, potentially amplifying the signaling effects of EGF.
Conclusions: This study highlights alterations in EGF signaling in DMD and uncovers new molecular interactions involving EGF and EFEMP1. These findings contribute to understanding the cellular mechanisms underlying muscle degeneration and provide potential targets for therapies aimed at mitigating muscle dystrophy progression.
D08A spatial transcriptomic approach to understanding Duchenne Muscular Dystrophy
Rasya Gokul Nath1
, Elisa Villalobos1, James Clark1, Priyanka Mehra1, Panos Katsikis1, Catherine Collins1, Esther Fernandez-Simon1, Alexandra Monceau1, Mojgan Reza1, Zoe Laidler1, Jose Verdu-Diaz1, Rachel Queen2, Jordi Diaz-Manera1
1.The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, UK, 2.Biosciences Institute, Newcastle University, NE1 3BZ
rasya.gokul-nath@newcastle.ac.uk
Background: Duchenne Muscular Dystrophy (DMD) is a genetically inherited, X-linked neuromuscular disease caused by mutations in dystrophin encoding DMD gene. It is characterized by severe and progressive muscle wasting leading to irreversible disability. Early-stage DMD patients present with symptoms such as difficulty taking the stairs, imbalance, and a waddling gait. The muscle fibers are progressively lost in the later stages and replaced by fibrotic and adipose tissue. It causes severe weakness and a loss of ambulation. The disease progression further affects the cardiorespiratory function in the patients, ultimately resulting in their death in the third or fourth decade of their life.
Aim: To investigate the histopathological changes happening in muscle tissue across different stages of the disease and map the molecular markers with these changes in DMD samples at spatial resolution.
Methods: We employed spatial transcriptomics technology on muscle biopsies of DMD patients (n=2, for early, middle, and middle-to-advanced DMD stage each) and healthy controls (n=3). Using our previously published single-nuclei RNA-sequencing dataset, we applied a deconvolution strategy to study the spatial cell-type localization in the samples. We first used the gene expression profiling in snRNA-seq dataset to annotate the cell types present in the data using an R package, Seurat. With this as reference, we utilised Cell2location tool to deconvolute the spots in the spatial transcriptomic dataset and find the contribution of the identified cell types to the gene signature in each spot.
Results: We estimated the overall cell-type proportions and their spatial localization across the different stages of DMD and control samples. We also identified the different FAPs subtypes and estimated their relative proportions in the spatial transcriptomic dataset.
Conclusion: This study will help demonstrate the cellular and spatial complexity in the different stages of DMD progression, which could offer novel opportunities for therapeutic intervention.
D09AAV-Mediated DUX4 Knockdown in Facioscapulohumeral Muscular Dystrophy: Therapeutic Benefits and Challenges for Long-Term Efficacy
V. Mariot1
,
S. Sohn1*, S. Reid1*, M. Bowen2, C. Hudon1, E. Corbex1, B. Morel2, C. Hourde2,3 and J. Dumonceaux1
1NIHR Biomedical Research Centre, University College London, Great Ormond Street Institute of Child Health and Great Ormond Street Hospital NHS Trust, London, UK, 2Laboratoire Interuniversitaire de Biologie de la Motricité LIBM, EA 7424, Savoie Mont Blanc University, F-7300, Chambéry, France, 3Université Grenoble Alpes, Inserm, LBFA, 38000 Grenoble, France
Virginie.mariot@ucl.ac.uk
Background: Facioscapulohumeral muscular dystrophy (FSHD) is characterised by the aberrant expression of the toxic transcription factor DUX4 in skeletal muscle, leading to progressive muscle degeneration. Therapeutic strategies targeting DUX4 inhibition are promising, with AAV-mediated delivery emerging as a key approach. However, the regenerative nature of skeletal muscle poses a challenge to AAV-based therapies, as muscle fibre turnover can diminish AAV transduction efficiency and the persistence of therapeutic transgenes over time.
Aims: This study aimed to evaluate the efficacy and durability of AAV-mediated DUX4 inhibition using an AAV vector carrying a short hairpin RNA targeting DUX4 (shDUX4) in a mouse model of FSHD. The goal was to assess this approach's short- and long-term therapeutic impact and identify potential limitations.
Methods: The ACTA1-MCM; FLExDUX4/+ mouse model, which replicates key features of FSHD, was used. Mice received a single administration of AAV-shDUX4 (MyoAAV 2A capsid), and therapeutic efficacy was assessed one month and 10 months post-treatment. Outcomes included molecular analyses, histopathological evaluation, and functional assessments using force-velocity-endurance (FOvE) tests. The persistence of AAV genomes and DUX4 knockdown efficacy were also evaluated over time.
Results: One month after AAV-shDUX4 administration, significant improvements were observed in DUX4-associated pathological features, including reduced molecular markers of toxicity, improved muscle histology, and enhanced functional FOvE parameters. However, by 10 months post-treatment, these therapeutic benefits had largely diminished. Most pathological markers remained uncorrected, and muscle force showed no sustained improvement. The decline in therapeutic effect is correlated with reduced DUX4 knockdown and a loss of AAV genomes, which is likely due to muscle fiber turnover and AAV genome dilution.
Conclusion: AAV-mediated shDUX4 therapy offers significant short-term benefits for FSHD by effectively suppressing DUX4 expression. However, the long-term therapeutic efficacy is limited by muscle fibre regeneration and associated AAV genome loss. These findings underscore the need for strategies to enhance the durability of AAV-based therapies to achieve sustained benefits in FSHD treatment.
D10Analysis of the DNA methylation of FAPs in Duchenne muscular dystrophy
Lidia Matias-Valiente1
, Jordi Diaz-Manera1,2,3
1John Walton Muscular Dystrophy Research Center, University of Newcastle, Newcastle upon Tyne, UK, 2Neuromuscular Diseases Unit, Neurology Department, Hospital de la Santa Creu i Sant Pau and Biomedical Research Institute Sant Pau (IIB Sant Pau), Barcelona, Spain, 3Centro de Investigaciones Biomédicas en Red en Enfermedades Raras (CIBERER), Madrid, Spain
lidia.matias-valiente@newcastle.ac.uk
Background: Duchenne muscular dystrophy (DMD) is a devastating degenerative disease of skeletal muscles caused by loss of Dystrophin, a key protein to maintain muscle integrity. The absence of this protein causes progressive muscle degeneration, aggravated by chronic inflammation, reduced regenerative capacity of muscle stem cells and muscle replacement by fibro-adipogenic tissue, which is one of the major pathological features of skeletal muscle in DMD patients, driven by the differentiation of fibro-adipogenic progenitors cells (FAPs) into profibrotic or adipogenic cells. The role that epigenetic changes play in FAPs differentiation potential has not been explored yet. We have recently identified differences in the expression of non-coding RNAs including both microRNAs (miRNAs) and small nuclear RNAs (snRNAs) between DMD and control FAPs isolated from muscle and cultured in vitro, suggesting that they might play a role in the different biological behaviour of these cells.
Aim: We hypothesize that epigenetic mechanisms, particularly DNA methylation, influence the altered function and plasticity of FAPs in DMD patients contributing to their differentiation into fibrotic and adipogenic cells. Thus, the main goal of this project is to perform a comprehensive analysis of the DNA methylation patterns in FAPs isolated from DMD patients and compare it with control FAPs to deepen our understanding of their potential role regulating FAPs behaviour in the process of muscle degeneration in DMD.
Methods/Materials: Firstly, we will analyse the overall differences in DNA methylation patterns between FAPs isolated from muscle biopsies of DMD patients and age and gender matched healthy controls using an ELISA assay. To specifically identify which genes are hypermethylated or hypomethylated in dystrophic condition, we will perform genome-wide methylation profiling using Illumina Infinium BeadArrays. By RT-qPCR and Western Blot, we will also study the expression levels of DNMT and TET enzymes, which are responsible of the methylation process.
Results and Conclusions: Characterizing this process may provide valuable insights into how molecular mechanisms regulating FAPs function and potentially lead to the identification of novel therapeutic targets to slow the progression of this disease.
D11Unlocking adipogenesis: Role of MicroRNAs in differentiation of fibro-adipogenic precursors in Duchenne muscular dystrophy
Priyanka Mehra1, Elisa Villalobos1, Panos Katsikis1, Mandy Peffers2, Jordi Diaz Manera1
1John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom, 2 Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, United Kingdom
P.Mehra2@newcastle.ac.uk
Background: Duchenne muscular dystrophy (DMD) is a genetic disease characterized by degeneration of muscle fibres and their replacement with fatty-fibrotic tissue. The primary cells responsible for this fibrotic and fat tissue expansion are fibro-adipogenic precursor cells (FAPs), which are mesenchymal stem cells capable of differentiating into fibroblasts or adipocytes. The molecular mechanisms governing the cell fate of FAPs remain poorly understood. Recent studies have highlighted the role of microRNAs in regulating adipogenesis; however, their role in FAPs adipogenic differentiation remains unclear.
Aim: To identify and characterize microRNAs involved in the differentiation of FAPs from patients with DMD and control individuals.
Methods: Total RNA was extracted from FAPs (n=4, DMD and control) cultured in adipogenic differentiation media for three days, followed by small-RNA sequencing. Differential gene expression analysis was conducted on the obtained results. A comprehensive literature review was performed to identify microRNA targets and elucidate their role in adipogenesis. Sequencing results were validated using qRT-PCR. MicroRNAs that were differentially expressed in DMD FAPs compared to control FAPs in both adipogenic and basal media were further characterized. Their expression was evaluated at various time points during adipogenesis using qRT-PCR. Additionally, the impact of the microRNAs on adipogenesis was assessed by treating FAPs with microRNA mimics and evaluating their effect on the expression of adipogenic markers using qPCR.
Results: We observed significant differences in microRNA expression (>2-fold change, FDR < 0.05) between DMD and control FAPs cultured in both adipogenic and basal media. Specifically, hsa-miR-196a-5p and hsa-miR-10a-5p exhibited >5-fold decrease in expression in DMD FAPs compared to controls. Further characterization revealed that the expression of hsa-miR-196a-5p gradually reduces during adipogenic differentiation of FAPs. Additionally, treatment of DMD FAPs with hsa-miR-196a-5p mimic resulted in a decrease in the expression of adipogenic markers after three days of differentiation, suggesting hsa-miR-196a-5p may regulate adipogenic differentiation of FAPs.
Conclusion: These findings demonstrate that microRNA expression differs between DMD and control FAPs, and that microRNA expression in FAPs changes upon adipogenic induction. This suggests the presence of epigenetic regulation of FAPs behavior in DMD, which is maintained when cells are isolated from the tissue and cultured in-vitro.
D12Single nuclei RNA-seq to unravel the molecular mechanisms of Facioscapulohumeral Muscular Dystrophy
Mohi-Uddin Miah1, Asmita Saha1, Raul Fulea1, Catherine Collins1, Rasya Gokul Nath1, Sam Fitzsimmons1, Ariele Barreto Haagsma1, Michela Guglieri1, Chiara Marini Bettolo1, Jordi Diaz Manera1, Volker Straub1, Giorgio Tasca1.
1John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom.
m.miah4@newcastle.ac.uk
Background: Facioscapulohumeral muscular dystrophy (FSHD) is one of the most prevalent muscular dystrophies, affecting 1 in 20,000 people. It is marked by progressive and asymmetric weakness and atrophy predominant in facial, shoulder girdle and upper arm muscles. FSHD is driven by the abnormal activation of the DUX4 retrogene in skeletal muscle. Abnormal DUX4 expression disrupts muscle cell function through processes like apoptosis, oxidative stress, and inflammation, yet its full impact remains incompletely understood, with limited in vivo validation.
Aims: This study aims to understand the biological pathways involved in FSHD by single-nuclei RNA sequencing (snRNA-seq) on human skeletal muscle biopsies. Through this approach, we intend to identify disease-specific gene signatures and dysregulated pathways. This can ultimately inform new biomarkers for disease monitoring and discovery of new therapeutic targets.
Method/Materials: Skeletal muscle biopsy samples have been collected from healthy individuals and FSHD patients, followed by single-nuclei RNA sequencing performed to comprehensively explore the transcriptomic landscape of individual muscle cells. FSHD muscles are stratified according to their muscle magnetic resonance signal, in either muscles showing active (STIR+) or inactive (STIR -) disease.
Results: Preliminary analyses have shown an increased prevalence of slow-twitch myonuclei, alongside endothelial cells and fibro-adipogenic progenitor cells (FAPs) in FSHD patients compared to healthy individuals.
Conclusion: This study is the initial step towards understanding the molecular and cellular mechanisms driving FSHD using a multi-omic approach. Preliminary findings indicate a higher amount of slow-twitch myonuclei and FAPs, which implies a shift in cell-type in the disease. By integrating single-nuclei and spatial transcriptomics, this research intends to understand disease-specific biomarkers at different stages and aid in treatment development.
D13Normalising to functional muscle volume as a proportion of bodyweight eliminates age- and genotype-associated differences in serum myostatin in a canine model of Duchenne muscular dystrophy
Dominique O. Riddell1
, Natasha L. Hornby1, John C.W. Hildyard1, Rachel C.M. Harron1, Dominic J. Wells2, Richard J. Piercy1
1Comparative Neuromuscular Diseases Laboratory, Department of Clinical Science and Services, Royal Veterinary College, London, NW10TU, UK, 2Department of Comparative Biomedical Sciences, Royal Veterinary College, London, NW10TU, UK
driddell@rvc.ac.uk
Background: Inhibiting myostatin (MSTN) signalling has been proposed as an approach to treatment of Duchenne muscular dystrophy (DMD). However, patients and canine models of DMD have low serum MSTN concentrations, leading to speculation that MSTN inhibition might be ineffective in this disorder. Low circulating MSTN in DMD has been attributed to downregulation of muscle MSTN expression, but here we hypothesised that it is caused, instead, by reduced functional skeletal muscle volume as a proportion of bodyweight.
Aims: To assess the influence of muscle atrophy and fibrosis on WT and DE50-MD dog serum MSTN concentrations and to examine normalisation strategies for serum MSTN quantification. Further we examine muscle MSTN mRNA and protein expression in DMD and control dogs.
Methods/Materials: Male dogs (from a total cohort of DE50-MD: up to N=16; WT: up to N=14) were studied longitudinally at 3-monthly intervals between 3- and 18-months of age. At each timepoint we obtained serum, mRNA and picrosirius red fibrosis fraction from biopsied vastus lateralis muscle, MRI-derived pelvic limb and lumbar muscle volumes, and bodyweight. Vastus lateralis, biceps femoris and semitendinosus muscle samples were collected postmortem in a subset of 18-month dogs (N=3-4). MSTN protein was quantified by ELISA and MSTN mRNA by RT-qPCR.
Results: Serum MSTN concentration was lower in DE50-MD dogs than WT at all ages, while no difference was seen between genotypes in muscle MSTN mRNA. Normalisation of serum MSTN concentration to muscle volume eliminated differences between genotypes, while normalisation to non-fibrotic muscle volume as a proportion of bodyweight eliminated differences between genotype and age groups. MSTN protein and mRNA expression did not differ between genotypes within the 3 muscle groups analysed postmortem.
Conclusion: MSTN expression within muscle was unaffected by genotype, at both RNA and protein level: low serum MSTN concentrations in DE50-MD dogs can instead be accounted for by the reduced functional muscle mass as a proportion of bodyweight. If the same occurs in DMD patients, inhibition of MSTN signalling might remain a possible treatment approach.
D14Variability in the efficacy of antisense oligonucleotide treatment among DMD patients: correlation between genome and transcriptome
Konstantina Tetorou
1,2, Francesco Muntoni1,2, Rachele Rossi1,2
1 The Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, UK, 2 National Institute for Health Research, Great Ormond Street Institute of Child Health Biomedical Research Centre, University College London, London.
konstantina.tetorou.18@ucl.ac.uk
Background: Duchenne muscular dystrophy (DMD), a lethal neuromuscular disease affecting children, is caused by mutations, mostly deletions, in the DMD gene. Currently, genetic therapies such as antisense oligonucleotides (AONs) are showing positive results in clinical studies, albeit with substantial inter-patient variability, the reasons for which remain unclear. Recently, it was observed that DMD mature transcripts seem to have a preferential nuclear localization in DMD patients and dystrophic animal models compared to healthy controls and animals, respectively. Recent data on the spliceosomal machinery and processes suggest that the spliceosome utilizes unannotated intronic splice sites with a high level of kinetic variability in intron removal. Moreover, in some cases, pre-mRNA molecules still containing introns, especially from large genes or when spliceosome processivity decreases, have been demonstrated to escape from the nucleus. These phenomena impact the amount of the transcript available for AONs, affecting their efficacy.
Aims: This project aims to elucidate the role of splicing in individual variability to AON treatment in DMD patients. Specifically, it seeks to determine whether patients with different deletion breakpoints exhibit dissimilar mature and non-mature DMD transcript localization and different expression levels of the DMD transcript. Additionally, this study aims to evaluate, for the first time, the fidelity of AON-mediated splicing using post-treatment RNA-seq analysis.
Methods/Materials: We extracted RNA from myogenic cells of 25 DMD patients, both in-vitro treated and non-treated with AON, to perform DMD-targeted long-read RNA profiling. The same cells were also used for nuclear and cytoplasmic RNA extraction, followed by qPCR using 5’ and 3’ DMD-specific TaqMan probes.
Results: Methods for nucleus/cytoplasm RNA extraction were optimized, and the RNA analysis showed minimal contamination between cellular subfractions. The targeted long-read RNA sequencing revealed the expected isoform expression and confirmed the fidelity of AON-mediated splicing.
Conclusions: This study represents the first attempt to investigate DMD transcript characteristics among different patients to better understand the inter-patient variability observed in genetic therapy clinical trials. Our results contribute to the understanding of one important challenge of AON treatment.
D15Screening of exon-skipping antisense oligonucleotide bioconjugates on Duchenne muscular dystrophy human and mouse models
Torres-Masjoan, L.1, *, Aghaeipour, A.1, Coulson. D.2, Frommer. J.2, Aguti, S.1, Privolizzi, R.1, D Zhou, H.3, 4, Muntoni, F.1, 4, 5, and TransNAT consortium
1Neurodegenerative Diseases, UCL Queen Square Institute of Neurology, London, UK, 2Department of paediatrics, Oxford University, Oxford, UK, 3Genetics and Genomic Medicine Research and Teaching Department, UCL Great Ormond Street Institute of Child Health, London, UK, 4National Institute for Health Research, UCL Great Ormond Street Institute of Child Health, London, UK, 5The Dubowitz Neuromuscular Centre, Molecular Neuroscience Section, Developmental Neurosciences Research and Teaching Department, UCL Great Ormond Street Institute of Child Health, London, UK
l.masjoan@ucl.ac.uk
Background: Duchenne muscular dystrophy (DMD) is a severe neuromuscular disorder that causes progressive muscle weakness and premature death. Most of the cases are caused by frame-shifting mutations on the dystrophin gene (DMD) resulting in the depletion of functional dystrophin. One therapeutical approach for the treatment of DMD is the use of exon-skipping antisense oligonucleotides (ASOs) to restore the reading frame of the DMD gene leading to the production of shorter but functional dystrophin. To date, four ASOs have been approved by the U.S. Food and Drug Administration. However, their treatment efficacy remains low and there is a current need of developing new ASOs with improved uptake, endosomal escape and target engagement by modifying their structure.
Aims: This study, which is part of the UKRI funded interdisciplinary consortium TransNAT, aims at developing and testing new ASOs conjugated to different moieties, including lipids, vitamins and polyamines, on various DMD models.
Methods/Materials: Immortalized human skeletal muscle cells and hiPSCS-derived cardiac muscle cells carrying a deletion of exon 52 of DMD, were treated with the bioconjugates, and exon-skipping and dystrophin protein restoration were assessed by RT-qPCR and western blot (WES). In parallel, the intracellular localization of the bioconjugates was assessed by miRNAscope. The lead candidates will be administered to a new humanized inducible mdx52 mouse model (h52floxedDMD), where exons 49-53 are humanized, and exon 52 is flanked by two loxP sequences.
Results: While some lipid-conjugates showed cytotoxicity on immortalized myotubes, we observed exon-skipping on immortalized myoblasts and hiPSCs-derived cardiomyocytes by lipid-bioconjugates. We also detected ASOs on treated cells, and, in combination with endosomal markers’ immunodetection, this will serve as a platform to understand the intracellular trafficking of ASOs until they reach their pre-mRNA target. Finally, we validated the elimination of exon 52 upon Cre expression on h52floxedDMD mouse embryonic stem cells and are running preliminary exon-skipping experiments on them for further validation of the model.
Conclusion: With this study, we expect to gain a better understanding on the role of different chemical modifications of ASOs on their endocytosis, intracellular trafficking, and treatment efficacy to, ultimately, design safer and more efficient ASOs-based therapies for DMD.
‡D16Studying and modelling Duchenne muscular dystrophy pathology and therapies with next-generation human stem cell-based models
Tugce Torun
1,2*, Moustafa Khedr1,2*, Sumitava Dastidar1,2, Louise Moyle1, Hidetoshi Hoshiya1, Katrin Neumann3, Yulia Lomonosova1,2, Matthew Wood4,5,6, Francesco Muntoni7, Konstantinos Anastassiadis3, Francesco Saverio Tedesco1,2,7*
1Department of Cell & Developmental Biology, University College London, London WC1E 6DE, UK;, 2The Francis Crick Institute, London NW1 1AT, UK;, 3Technische Universität Dresden, 01307 Dresden, Germany,, 4Department of Paediatrics, University of Oxford, Headington, Oxford OX3 7TY, UK, 5Institute of Developmental and Regenerative Medicine, University of Oxford, IMS-Tetsuya Nakamura Building, Old Road Campus, Roosevelt Drive, Headington, Oxford OX3 7TY, UK, 6MDUK Oxford Neuromuscular Centre, South Parks Road, Oxford OX3 7TY, UK, 7Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health & Great Ormond Street Hospital for Children, London, UK.
*Equal contribution
**Correspondence: f.s.tedesco@ucl.ac.uk
Presenter: tugce.torun.19@ucl.ac.uk
Background: Duchenne muscular dystrophy (DMD) is caused by a deficiency of the dystrophin protein, resulting in progressive skeletal muscle wasting and weakness, often with concurrent cardiac involvement. Although less obvious in infants, DMD cardiac pathology worsens over time and becomes life-threatening. Unfortunately, research into DMD striated (i.e., cardiac and skeletal) muscle pathophysiology is often restricted by limited access to primary samples (e.g., human heart tissue) and suboptimal animal models.
Aims: Given the limitations of current disease models in capturing the complex interplay of cardiac and skeletal involvement in DMD, this study establishes a novel platform using human iPSCs and tissue-engineered models, including a novel isogenic cell line engineered with a dystrophin-reporter cassette (RC). With this platform, we aim to investigate human dystrophin expression dynamics, DMD pathogenesis and response to therapies in vitro.
Methods/Materials: Isogenic DMD and healthy control iPSCs were differentiated into cardiac and skeletal myogenic lineages and then combined with biomaterials into the engineered heart (EHT) and skeletal muscle (ESMT) tissues. The electrophysiological behaviour of EHTs and ESMTs was analysed with a pillar-based contraction recorder. Proof-of-principle response to therapy was performed using antisense oligonucleotides (ASO) to induce exon skipping and re-framing of the dystrophin transcript.
Results: Molecular analyses of cardiac markers (cTNI, MHY6/7) revealed enhanced tissue maturation in EHTs compared to conventional monolayer cultures. Notably, DMD EHTs exhibited a reduction in the cardiomyocyte population (cTNT+cTNI+), accompanied by an increase in the non-cardiac cell population. Analysis of excitation-contraction coupling demonstrated contraction abnormalities in DMD EHTs, resembling disease-associated defects described in vivo. Following the delivery of ASO, dystrophin expression in DMD EHTs increased over time, measured using the new RC. Additionally, using the same RC, we tracked dystrophin protein localisation live in cell cultures. While healthy control cardiomyocytes expressed dystrophin at the cell edges in long-term cultures (≥Day 30), DMD cardiomyocytes showed reduced dystrophin expression.
Conclusion: DMD 3D-engineered striated muscles recapitulated key disease hallmarks and showed partial dystrophin restoration after ASO treatment, expanding the toolkit of novel organoid-like platforms in DMD pre-clinical research.
D17Biomechanical regulation in Duchenne muscular dystrophy: the role of stiffness in adipogenic differentiation of human adipogenic precursors
Elisa Villalobos
1
, Priyanka Mehra1, James Clark1, Panos Katsikis1, Jordi Diaz-Manera1
1 John Walton Muscular Dystrophy Research Centre (JWMDRC), Institute of Genetic Medicine, Newcastle University, Newcastle, UK
Elisa.Villalobos@newcastle.ac.uk
Background: Duchenne Muscular Dystrophy (DMD) is an X-linked disorder caused by mutations in the Dystrophin gene, leading to muscle degeneration and fibro-fatty tissue accumulation. Fibro-adipogenic progenitors (FAPs) play a crucial role in muscle degeneration by differentiating into fibroblasts and adipocytes. External factors, such as tissue stiffness, can affect FAP survival and differentiation. However, the impact of tissue stiffness on FAP differentiation in DMD remains unclear. This study aims to investigate how stiffness influences FAP fate in DMD and identify key proteins involved in mechano-transduction.
Methods: Human fibro/adipogenic progenitors (FAPs) and human pre-adipocytes (SGBS) were seeded in different stiffness (0.2 - 46 kPa). We use FAPs control and from muscles with DMD. Differentiation into fibroblast was evaluated after treatment with TGF-ß1 (3d) and differentiation into adipocytes was evaluated after treatment with adipogenic media (3, 5, 10d). Collagen I, Fibronectin, α-SMA and FABP4 and PPARγ (adipogenesis) were evaluated by western blot, as key differentiation markers. Further, targeted proteomic assay was done in FAPs after adding adipogenic media (1d) to assess involvement of protein kinases regulating the process of differentiation. Key mechano-transduction regulators were evaluated by Immunofluorescence and western blot.
Results: We identified decreased cell survival in cells (SGBS and FAPs) at soft surfaces, this effect was greater in FAPs DMD. Increased levels of adipogenic markers (FABP4 and PPARγ), were observed in SGBS and FAPs at stiffer surfaces. The effect of differentiation was less clear in fibrosis. Diminished levels of FAK(Tyr397) and different distribution pattern of vinculin were identified in DMD FAPs in basal conditions. Results from the proteomic analysis identified WNK1 and PRAS40 as relevant kinases involved in adipogenic differentiation.
Conclusions: Our results suggest higher tissue stiffness (muscle and adipose tissue), common in ageing, metabolic and neuromuscular diseases, could promote ectopic accumulation of fat by increasing the adipogenic commitment on FAPs and pre-adipocytes. Changes in vinculin and FAK could potentially explain changes in cell survival in different genotypes. The identification of targets such as, WNK1 and PRAS40 will allow us to further dissect these pathways and work on strategies to tackle adipogenesis in muscle.
Dystrophy (Clinical)
DC01The Newcastle Distal and Myofibrillar Myopathy Cohort
Ariele Barreto Haagsma1
, Doaa Salman1, Carla Bolano Diaz1, Marianela Schiava1, Tara Reeves1, Pietro Riguzzi1, Goknur Kocak1, Maha Elseed1, Elizabeth Harris1, Ana Töpf1, Judith Hudson2, Robert Muni Lofra1, Emma Grover1, Emma-Jayne Robinson1, Michelle McCallum1, Jassi Michell-Sodhi1, Dionne Moat1, Karen Wong1, Peter Waldock1, Julie Walsh1, Stephanie Tanner1, Jordi Diaz-Manera1, Michela Guglieri1, Chiara Marini Bettolo1, Volker Straub1, Giorgio Tasca1
1 The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, UK, 2 Northern Molecular Genetics Service, Biomedicine East Wing, Newcastle upon Tyne, UK
ariele.barreto-haagsma@newcastle.ac.uk
Background: Distal and myofibrillar myopathies (DM and MFM) are umbrella terms for rare diseases showing significant overlap.
Aims: to describe the features of the MFM and DM population followed at the John Walton Muscular Dystrophy Research Centre.
Methods/Materials: This retrospective single-centre study included patients with either a myopathological diagnosis of MFM or a clinical diagnosis of DM. Demographic, genetic, clinical, and respiratory data were collected from July 1995 to April 2024. Variables assessed included disease causing variants, age at onset, first symptoms, and ambulatory status.
Results: The cohort included 127 patients. Sixty-four patients fulfilled the criteria for MFM (mean age 49.26 ± 14.62 years, 68.8% male) and eighty-four for DM (mean age 47.32 ± 15.39 years, 63.1% male). Twenty-one patients (16.5% of the whole cohort) matched the criteria for both. Seventy-eight percent of the patients were molecularly diagnosed. In DM, the most frequent causative gene was GNE (29.8%), while variants in TTN or DES were found in 59.4% of MFM patients. Age at onset did not significantly differ between the MFM and DM subgroups (mean 40.89 ± 14.64 years versus 37.26 ± 14.41 years, p = 0.169). TTN variants were significantly associated with respiratory symptoms and DES variants with cardiac symptoms at onset. Both these genes were also significantly associated with lower sitting forced vital capacity values at initial assessment.
Conclusion: This service evaluation provides an initial cross sectional characterization of the DM/MFM cohort followed at the John Walton Muscular Dystrophy Research Centre. The next steps will be the collection of retrospective longitudinal, muscle biopsy and MRI data.
DC02Standards of Diagnosis and Care for the Sarcoglycanopathies
Holly Borland1, Claudio Bruno2, Kristl Claeys3, Marta de Antonio Ferrer4, Filipe Di Pace5, Meredith James1, Nicholas Johnson6, Lea Leonardis7, Leonela Luce1, Najoua Miladi8, Isabelle Richard9, Dorianna Sandona10, Beril Talim11, Giorgio Tasca1, Conrad Weihl12, Stephan Wenninger13, Jordi Diaz-Manera1
1The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon, Tyne, United Kingdom, 2 Paediatric Neurology and Neuromuscular Disorders Unit, IRCCS Istituto Giannina Gaslini, Genoa, Italy, 3Department of Neurology, University Hospitals Leuven, Leuven, Belgium, 4Servei de Cardiologia, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 5Department of Neurology, Hospital das Clinicas da Faculdade de Medicina da Universidade de Sao Paulo, Sao Paulo, Brazil, 6Department of Neurology, Virginia Commonwealth University, Richmond, Virginia, USA, 7Department of Neurology, Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia, 8University of Tunis El Manar, 2092 El Manar 1, Tunis, Tunisia, 9Généthon, INSERM U951, INTEGRARE Research Unit, Évry, France, 10Department of Biomedical Sciences, University of Padova, Via U. Bassi 58/B, 35131 Padova, Italy, 11Department of Pediatrics, Pathology Unit, Hacettepe University Faculty of Medicine, Ankara, Turkey, 12Department of Neurology, Washington University School of Medicine, St Louis, MO, USA, 13Department of Neurology, Friedrich-Baur-Institute, LMU Clinics Munich, Munich, Germany
h.borland2@newcastle.ac.uk
Background: Sarcoglycanopathies are a group of autosomal recessive muscular dystrophies caused by pathogenic variants in one of the four sarcoglycan genes. The disease is characterised by proximal muscle weakness which begins during childhood and progresses quickly, with early loss of ambulation. Clinical signs include calf hypertrophy and scapular winging. HyperCKaemia is common. MRI shows a pattern of fat replacement; muscle biopsy often shows dystrophic changes. Current management is focused on a multidisciplinary approach, involving neuromuscular care, physiotherapy, cardiorespiratory exercises, and surgery where required. To ensure quality patient care and clinical outcomes, it is essential that this management is delivered in a standardised manner. Provision of standards of care will allow patients to receive internationally-recognised diagnoses, management, and follow-up.
Aims: The focus of this workshop was to align experience from around the world, provide data-driven recommendations for the clinical care of individuals with the diagnosis of a sarcoglycanopathy, and identify unmet needs.
Methods/Materials: Patient representatives and multidisciplinary experts from around the world in the fields of basic science, translational research, and clinical care met during the 282nd European Neuromuscular Centre (ENMC) International Workshop to develop a standard of diagnosis and care for the sarcoglycanopathies.
Results: Clinical presentation of the sarcoglycanopathies is heterogeneous, so the goal was to capture a more robust understanding of trajectories across variants to further inform future care. A diagnostic algorithm was proposed, including common clinical presentations, differential diagnoses, and expected presentation of immunohistochemistry and MRI results across subgroups. Recommendations for a gold standard set of clinical outcome assessments was suggested, along with a corresponding minimum acceptable dataset. Recommendations for monitoring of cardiac and respiratory manifestations should begin when individuals lose ambulation or become symptomatic. A standardised definition of ‘ambulatory’ was proposed; the ability to complete the 10-meter timed test (10m) in less than 30 seconds. Additional topics included recommendations for exercise, anaesthesia, emergency care, paediatric-to-adult care transition, clinical trial opportunities, and drug discovery programmes.
Conclusion: A standard of care guideline for the sarcoglycanopathies is in development to be published for use globally. Endocrinological and nutritional aspects of care were identified as areas that would benefit from further understanding.
DC03The International Clinical Outcome Study for Dysferlinopathy II: validation of motor outcome measures in a new patient cohort
Holly Borland1, Heather Hilsden1, Meredith K. James1, Heather Gordish Dressman2, Laura E. Rufibach3, John. W. Day4, Jerry R Mendell5, Roberto Fernandez Torron6, Matt Harms7, Alan Pestronk8, John Vissing9, Urvi Desai10, Madoka Yoshimura11, Jin-Hong Shin12, Tahseen Mozaffar13, Tanya Stojkovic14, Elena Pegoraro15, Jorge Bevilacqua Rivas16, Montse Olive17, Carmen Paradas18, The Jain COS Consortium, Volker Straub1
1The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, UK, 2Center for Translational Science, Division of Biostatistics and Study Methodology, Children’s National Health System; Paediatrics, Epidemiology and Biostatistics, George Washington University, DC, USA, 3The Jain Foundation, Seattle, Washington USA, 4Department of Neurology and Neurological Sciences, Stanford University School of Medicine, CA, USA, 5Abigail Wexner Research Institute, Nationwide Children’s Hospital, Columbus, OH USA, 6Neuromuscular Area, Biodonostia Health Research Institute, Neurology Service, Donostia University Hospital, Spain, 7Department of Neurology, Irving Medical Center, Columbia University, NY, USA, 8Department of Neurology, Washington University School of Medicine, St Louis, MO, USA, 9Copenhagen Neuromuscular Center, Department of Neurology, Rigshospitalet, University of Copenhagen, Denmark, 10Carolinas MDA Care Center, Atrium Health, Charlotte, NC, 11Department of Neurology, National Center Hospital, National Center of Neurology and Psychiatry, Tokyo, Japan, 12Laboratory of Molecular Neurology, Pusan National University Yangsan Hospital, 13Department of Neurology, MDA ALS and Neuromuscular Center, University of California, Irvine, CA, USA, 14Institut de Myologie, Groupe Hospitalier Pitié-Salpêtiere, Paris, France, 15Department of Neuroscience, University of Padova, Italy, 16Departamento de y Neurología Neurocirugía Clínica, Clínica Dávila, 17Neuromuscular Disorders Unit, Neurology Department, Hospital de la Santa Creu i Sant Pau, 18Neuromuscular Unit, Department of Neurology, Hospital U. Virgen del Rocío/ Instituto de Biomedicina de Sevilla
h.borland2@newcastle.ac.uk
Background: The International Clinical Outcome Study for Dysferlinopathy (COS) was the first multi-country natural history study in dysferlinopathy with the aim to characterise disease presentation and improve clinical trial readiness. In the absence of validated disease specific motor assessment scales, The North Star Assessment for limb girdle type muscular dystrophies (NSAD), was developed and validated in the COS I cohort. The Performance of Upper Limb (PUL 2.0) was assessed in COS I and found to be suitable to measure upper limb function in dysferlinopathy. The extension study, COS II, recruited 203 participants (119 new) from 16 sites in nine countries with the aim to validate the findings from COS I in an expanded cohort.
Aims: The aim was to validate the NSAD and PUL in the new COS II participants to determine the reliability of these clinical outcome assessments in patients with dysferlinopathy.
Methods/Materials: We examined the psychometric performance of the NSAD and PUL in the new COS II participants using Rasch Unidimensional Measurement Model (RUMM). Psychometric evaluation of 117 available assessments evaluated NSAD and PUL performance in seven areas: targeting, response categories, fit, reliability, dependency, stability and unidimensionality using RUMM2030 software.
Results: NSAD and PUL demonstrated unidimensional construct of functional motor performance and upper limb motor performance respectively, high reliability with a PSI of 0.96 and 0.95 respectively. A potential ceiling effect existed for the strongest/ asymptomatic subjects in both scales. 27/29 items of the NSAD and 19/22 items of the PUL demonstrated ordered response categories, meaning the scoring categories for each item are logical and appropriate for dysferlinopathy. No items of NSAD with fit residuals outside ±2.5 but three on the PUL. The items fit well together to make use of the total score appropriate. Differential item functioning analysis, indicative of whether person factor influences the probability of scoring, was not present for gender on either scale.
Conclusion: This study validated previous COS data COS, confirming that the NSAD and PUL are suitable measurements for use in dysferlinopathy. Ongoing analysis is underway examining the psychometric properties of these scales and responsiveness to change in functional ability over time.
‡DC04Mitochondrial characterisation of myotonic dystrophy type 1 human skeletal muscle
Valeria Di Leo1,2
, Laura Girard-Cote3,4, Marie-Pier Roussel5, Conor Lawless1,2, Tiago Bernardino-Gomes1,2,6, George O. T. Merces7,8, Grainne Gorman1,6, Elise Duchesne4,5 & Amy E. Vincent1,2.
1Wellcome Centre for Mitochondrial Research, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, UK; 2NIHR Newcastle Biomedical Research Centre, Newcastle upon Tyne Hospitals NHS Foundation Trust and Newcastle University, Newcastle upon Tyne, England; 3Department of Health Sciences, Université du Québec à Chicoutimi, Québec, Canada; 4Neuromuscular Diseases Interdisciplinary Research Group (GRIMN), Saguenay-Lac-St-Jean Integrated University Health and Social Services Center, Saguenay, QC, Canada; 5Department of Fundamental Sciences, Université du Québec à Chicoutimi, Quebec, Canada; 6NHS Highly Specialised Service for Rare Mitochondrial Disorders, Royal Victoria Infirmary, Newcastle Upon Tyne, UK; 7Biosciences Institute, Innovation, Methodology and Application (IMA) research Theme, Faculty of Medical Sciences, Newcastle University, UK; 8Image Analysis Unit, Faculty of Medical Sciences, Newcastle University, UK.
Valeria.Di-Leo@newcastle.ac.uk
Background: Myotonic dystrophy type 1 (DM1) is a rare neuromuscular disorder with dominant autosomal inheritance due to CTG triplet repeats expansion in the DMPK gene. At present, resistance exercise training has been proven the best option to ameliorate physical capabilities, such as skeletal muscle (SKM) weakness, and to increase muscle strength by triggering SKM hypertrophy. A significant knowledge gap is around mitochondrial involvement in DM1 pathology and related exercise physiology.
Aims: The aim of this study is to characterise SKM mitochondria from DM1 patients before and after 12-week resistance exercise training.
Methods/Materials: SKM biopsies were collected from quadriceps of DM1 patients (men, n=11; women, n=9) before and after resistance exercise training and compared to sex- and age-matched controls. Immunofluorescence was used to preliminary test the oxidative phosphorylation (OXPHOS) defects in SKM. A deeper characterisation of mitochondrial function will be performed with MACSima technology.
Results: The 12-week resistance exercise training increased mitochondrial mass and partially rescued mitochondrial OXPHOS deficiency in complex I and/or complex IV in DM1 patients. Exercise-induced effects observed in mitochondria are independent of the number of CTG triplet repeats, phenotype classification and sex. Undergoing experiments are employing spatial single cell analysis on SKM to assess proteins levels and to compare mitochondrial signalling pathways in both OXPHOS deficient and normal fibres before and after exercise training.
Conclusion: A deeper understanding of SKM mitochondrial functions in DM1 patients is necessary to underpin the role of novel factors in DM1 pathology and to identify novel therapeutic targets for the cure of DM1 patients.
DC05The DMD Hub Site Feasibility and Clinical Trial Database
Emma Heslop1, Phillip Cammish1, Jess Elliott1, Ellie Drummond1, Marta Zancolli3, Chloe Perry4, Alex Johnson5, Emily Reuben5, Alessandra Gaeta5, Volker Straub2 and
Michela Guglieri2
1 John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, UK, 2 John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK, 3 The Dubowitz Neuromuscular Unit, UCL Great Ormond Street Institute of Child Health, London, UK, 4 The Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry, UK, 5 Duchenne UK, London, UK
michela.guglieri@newcastle.ac.uk
Background: The DMD Hub is a collaboration between the John Walton Muscular Dystrophy Research Centre and Duchenne UK. In January 2025, the DMD Hub launched the Site Feasibility and Clinical Trial Database, a unique tool designed to facilitate clinical trial operations in the UK.
Aims: The database aims to streamline trial feasibility assessment, share information on the pipeline of trials in DMD, track trial activity at DMD Hub sites and record patient recruitment data, ultimately reducing timelines, supporting trial efficiency and improving patient access to DMD trials.
Methods: The central online secure platform allows clinical sites to manage detailed profiles of their experience, capabilities and available facilities. This supports timely and accurate responses to feasibility questionnaires requested from industry and contract research organizations (CROs), reducing the administrative burden on site staff. By providing sponsors with accurate and up-to-date site information, the database will accelerate the identification of suitable trial sites in turn reducing setup timelines. Sites can regularly update their profiles, ensuring ongoing relevance and accuracy. The two-way flow of information within the secure environment enables sites to receive up to date information on trials in the pipeline, helping them to plan and address potential capacity issues.
Results: The database is currently being piloted as a 12-month project. During this period, data collected will support feasibility assessments for companies seeking trial sites for DMD in the UK. At the pilot’s conclusion, a comprehensive review will assess its effectiveness in site selection, timeline reduction, and alleviating staff workload. Feedback will guide decisions on establishing the database as a long-term resource for the DMD community.
Conclusion: The DMD Hub Site Feasibility and Clinical Trial Database has the potential to significantly benefit the DMD community by reducing administrative burdens for site staff, accelerating trial setup, and improving patient access to clinical trials. This initiative is a critical step toward ensuring efficient trial execution and expanding research opportunities for DMD patients in the UK and will help ensure the UK remains competitive and sponsors continue to select UK sites to run DMD trials.
DC06DMD Hub: An established clinical trial accelerator network delivering tools and services to sites, patients and industry in the UK
Emma Heslop1
, Alessandra Gaeta2, Alexandra Johnson2, Emily Reuben2, Phillip Cammish1, Megan McNiff1, Pietro Riguzzi1, Francesco Muntoni3, Anne-Marie Childs4, Volker Straub1, Michela Guglieri1
1John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK, 2Duchenne UK, London, UK, 3The Dubowitz Neuromuscular Unit, UCL Great Ormond Street Institute of Child Health, London, UK, 4Leeds Teaching Hospital, Leeds, UK
Emma.Heslop@newcastle.ac.uk
Background: The DMD Hub (www.dmdhub.org), a collaboration between Duchenne UK and the John Walton Muscular Dystrophy Research Centre at Newcastle University, has established a UK Clinical Trial Accelerator Network (CTAN) to efficiently deliver Duchenne muscular dystrophy (DMD) clinical trials.
Aim: The DMD Hub CTAN ensures that clinical trials in DMD continue to be conducted in the UK, facilitating timely and effective trial setup and delivery.
Methods: The DMD Hub model was developed by incorporating key elements, including:
Building workforce capacity.
Establishing effective communication infrastructure.
Harmonising costings and trial setup processes.
Promoting fair and equitable patient recruitment.
Providing training and educational resources for staff.
Adapting to challenges to ensure sustainability.
Results: The established network offers a suite of tools and services for stakeholders, including patients, clinical sites, contract research organisations, and industry. Acting as a national, central coordinating body, it enables early engagement with sites, facilitates study and site feasibility, streamlines trial setup, and enhances recruitment to clinical studies. For sponsors, this centralised approach accelerates setup and delivery timelines, supported by site engagement, patient insights into trial design, and robust site feasibility. Sites benefit from improved processes, reduced duplication of effort, and increased trial opportunities. Patients gain greater access to clinical trial opportunities and effective recruitment processes.
Conclusion: The success of the DMD Hub model extends beyond DMD; in early 2024, the Becker Muscular Dystrophy Hub was launched, and DMD Hub tools have informed models for other rare diseases in recently funded national and international initiatives. A nationally coordinated, inclusive approach tailored to stakeholder needs has demonstrated the ability of the DMD Hub to improve clinical trial delivery and serve as a blueprint for other disease areas.
DC07Liver involvement in Myotubular and Centronuclear Myopathy: Review of one year’s data collected by the MTM & CNM Patient Registry
Lucy Hickson1, Julie Bohill1, Anando Sen1, Erin Ward2, Anne Lennox3, Michael W. Lawlor4, Heinz Jungbluth5,6, Alan H. Beggs7, Robert J. Graham8, Marcel Heidemann9, Marie Wood2, Mark Ward2, Jess Page1, Belinda Cowling10, Tmirah HaselKorn11, Nicol C. Voermans12, A Reghan Foley13, Eirini Kyrana14, Chiara Marini Bettolo1, Anil Dhawan,14. James J. Dowling15
1 The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK, 2 MTM-CNM Family Connection, Massachusetts, USA, 3 Myotubular Trust, London, UK, 4 Diverge Translational Science Laboratory and Medical College of Wisconsin, Milwaukee, WI, USA, 5 Department of Paediatric Neurology – Neuromuscular Service, Evelina Children’s Hospital, Guy’s & St Thomas’ NHS Foundation Trust, London, UK, 6 Randall Centre for Cell and Molecular Biophysics, Muscle Signalling Section, Faculty of Life Sciences and Medicine (FoLSM), King’s College London, London, UK, 7 The Manton Center for Orphan Disease Research, Boston Children's Hospital, Harvard Medical School, Boston, USA, 8 Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children’s Hospital, Boston, USA, 9 Independent consultant, Berlin, Germany, 10 Dynacure, Illkirch, France, 11 Astellas Gene Therapies, USA, 12 Department of Neurology, Donders Institute for Brain, Cognition and Behavior, Radboud University Medical Center, Nijmegen, The Netherlands, 13 Neuromuscular and Neurogenetic Disorders of Childhood Section, NINDS, National Institutes of Health, Bethesda, MD, USA, 14 Paediatric Liver, GI and Nutrition Centre and Mowat Labs, King’s College Hospital NHS Foundation Trust, London, UK, 15 Division of Neurology, Program for Genetics and Genome Biology, Hospital for Sick Children, Toronto, Canada
Lucy.Hickson@newcastle.ac.uk
Background: Centronuclear myopathies (CNMs) represent a group of rare, inherited congenital muscle disorders for which no cure is currently available. The most common form, X-linked myotubular myopathy (XLMTM), has an estimated incidence of 1 in 50,000 male births and is often associated with a severe clinical presentation. The International Myotubular and Centronuclear Myopathy Patient Registry is a database that collects both clinical and patient-reported data from affected individuals, both deceased and living.
In recent years, three clinical trials—ASPIRO, Unite-CNM and TAM4MTM—were discontinued early due to liver-related severe adverse events. These adverse events have brought increased attention to liver-related issues, including pre-existing liver dysfunction in XLMTM and CNM patients, which may heighten the risk of complications during treatment.
Aims: This project aimed to draw on the expertise of the Liver Working Group to create a tailored questionnaire and deepen understanding of the liver-related challenges faced by the CNM community.
Methods: Spearheaded by MTM-CNM Family Connection and the Myotubular Trust, the project brought together leading researchers from academia and industry, as well as patient advocates, to establish the Liver Collaborative Working Group. This group partnered with the MTM & CNM Patient Registry to design and launch a liver health questionnaire. The survey, integrated into the existing online registry platform, seeks to gather detailed information on liver health from both affected individuals and carriers.
Results: To date, 187 responses have been collected. As the working group continues to respond to emerging knowledge on liver dysfunction in CNM and XLMTM, new questions are being added to capture additional information, including dietary habits and results from liver tests. Preliminary findings have been gathered and analysed.
Conclusion: Insights gained from the liver health questionnaire will help to better understand liver dysfunction in CNM and XLMTM patients. The data will inform clinical management and contribute to the design of safer and more effective clinical trials for future therapies.
DC08Advancing Neuromuscular Research: Achievements and Future Directions for The John Walton Muscular Dystrophy Research Centre Patient Registries
Sam McDonald
, Julie Bohill
1
, Aleks Carver
1
, Lucy Hickson
1
, Helen Walker
1
, Chiara Marini-Bettolo
1
and Volker Straub
1
1 The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
Sam.mcdonald@newcastle.ac.uk
Background: Patient registries are secure databases where individuals with a specific rare condition can voluntarily provide their information to aid research efforts. The John Walton Muscular Dystrophy Research Centre (JWMDRC) manages 3 international and 3 national registries for patients with rare neuromuscular disorders. By collecting data from over 4500 combined participants, the registries can support ongoing efforts to further understand these rare conditions.
Aims: The registries endeavour to serve many functions, providing recruitment support for clinical studies, disseminating useful and disease specific information to patients and gathering longitudinal natural history data. They also support enquiries from external organizations and act as a communication platform connecting patients, healthcare professionals, and the research community.
Methods: Patients initiate registration for all JWMDRC registries through a secure online portal, providing informed consent. They complete a questionnaire about their condition, which includes details such as clinical diagnosis, genetic confirmation, current and optimal motor function, and ventilation status. Additionally, most registries ask questions on patient perceptions and experiences, which are collected using disease relevant PROM questionnaires.
Results: The registries have provided data and support to many research projects with help from responsive and engaged patient cohorts.
Conclusion: The John Walton Muscular Dystrophy Research Centre Patient Registries have built strong relationships with patient and scientific communities and can rapidly respond to research needs. The registries have had a positive impact on the neuromuscular field, contributing to the advancement of research and improvement of patient care.
DC09A comprehensive education and training programme for healthcare professionals in care and research for Duchenne muscular dystrophy developed from DMD Care UK and the DMD Hub
Megan McNiff1
, Cathy Turner1, Emma Heslop1, Alex Johnson2, Adam Kerr1, Sam Geuens3, Volker Straub1, Michela Guglieri1, 1 The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University, and the Newcastle upon Tyne Hospitals NHS Foundation Trust, UK, 2 Duchenne UK, UK, 3 Neuromuscular Reference Center Children, UZ Leuven, Belgium
megan.mcniff@newcastle.ac.uk
Background: The DMD Hub and DMD Care UK, as successful partnerships between the John Walton Muscular Dystrophy Research Centre and Duchenne UK, have pioneered the facilitation of expert care and clinical research across the UK for patients with Duchenne muscular dystrophy (DMD). However, recent work has shown that we need to address remaining discrepancies in care provision and access to clinical trials across the UK.
Key barriers to this include gaps in awareness and a lack of appropriate levels of understanding about latest standard of care guidelines and clinical research in DMD among health care professionals (HCPs). Knowledge of DMD care requirements is often limited to neuromuscular specialists, whilst others responsible for crucial care delivery may be less informed.
Aims: The DMD Hub and DMD Care UK aim to address the lack of access to expert care and clinical research, caused in part by gaps in awareness, which carries significant consequences for patients. We are developing a comprehensive, single, and reliable source of up-to-date, and accredited education and training for all aspects of DMD care and clinical research.
Methods/Materials: Content has been built on the outputs and expertise of the well-established DMD Care UK and DMD Hub projects, translating these into high-quality, expert-delivered resources for HCPs. This is delivered online via a learning management system and annual face-to-face workshops, and based on prioritised needs identified by the DMD Care and DMD Hub networks.
Results: We present here the first phase and plans for next steps of this programme that targets different learning needs from primary HCPs to tertiary specialists. Content will initially focus on physical aspects of multi-disciplinary care, e.g. cardiac care, as well as research topics such as gene therapy. We plan to expand to important and often overlooked components of DMD, such as psychosocial needs in care and clinical trial participation. Although the programme is UK-based, it will be available for use by healthcare practitioners in other countries with the only limitation being that content is delivered in English.
Conclusion: This educational programme will provide HCPs with bespoke, accessible, expert training across different aspects of DMD care and research.
‡DC10iPSC-based advanced models of LMNA-related congenital muscular dystrophy for the development of gene therapy strategies
Daniel Moore1,2, Cherry Tsz Yan Wong1,2, Valentina Lionello1,2, Heather Steele-Stallard1, Luca Pinton1,3, Salma Jalal1,2, Jean-Marie Cuisset4, Gisèle Bonne5, Peter Zammit3,± and Francesco Saverio Tedesco1,2,6,±,*
1 Department of Cell & Developmental Biology, University College London, London WC1E 6DE, UK;, 2 The Francis Crick Institute, London NW1 1AT, UK;, 3 Randall Centre for Cell & Molecular Biophysics, King’s College London, SE1 1UL London, UK;, 4 Centre de Référence des maladies neuromusculaires Nord/Est/Ile de France, Service de N europédiatrie, Hôpital Roger Salengro, CHRU Lille, Lille, France, 5 Sorbonne Université, INSERM, Institut de Myologie, Centre de Recherche en Myologie, Paris, France;, 6Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, UK.
Presenting author: daniel.moore.18@ucl.ac.uk
±Senior authors
*Correspondence: f.s.tedesco@ucl.ac.uk
Background: Laminopathies are a group of incurable muscular dystrophies caused by mutations in the LMNA gene. LMNA encodes the lamins A/C, which assemble to form the nuclear lamina: a structure primarily responsible for mechanical stabilisation of the nucleus, while also regulating chromatin organisation and gene expression. Mutations in the LMNA gene disrupt the nuclear lamina, rendering the nucleus prone to mechanical damage and rupture. Nuclear abnormalities are often found in mechanically active tissues such as cardiac and skeletal muscle, with LMNA-related congenital muscular dystrophy (L-CMD) being one of the most severe laminopathies. To date laminoapthies remain incurable, with research into disease mechanisms and therapeutic strategies hindered by lack of effective, humanised model systems.
Aims: We used induced pluripotent stem cells (iPSC) to recapitulate hallmark laminopathy skeletal myonuclear shape phenotypes and transcriptomic changes, as well as to develop genetic therapies using antisense oligonucleotide (AON)- and CRISPR-based technologies.
Methods/Materials: We used three patient-derived iPSC lines which harbour different L-CMD-causing LMNA mutations. These cells were differentiated into skeletal myogenic cells in vitro, and disease-associated phenotypes were assessed. CRISPR and AON genetic correction strategies were applied to the cells and assessment of phenotypic amelioration was performed, alongside computational predictions of lamin proteins resulting from those genetic interventions.
Result: iPSC-derived, LMNA-mutant muscle cells recapitulated myonuclear morphological abnormalities in 2D and 3D model platforms and have reduced LAMIN B1 levels. Transcriptomic analysis revealed enrichment of pro-apoptotic and inflammatory pathways. Alphafold structure prediction of internally truncated LAMIN A/C proteins suggested stable lamin species. These species were confirmed at RNA and protein levels in an LMNA-mutant line using a CRISPR-based exon removal strategy. Furthermore, the use of CRISPR-based methodologies specifically and precisely corrected the same LMNA mutation. These approaches ameliorated disease-associated morphological phenotypes in exon-skipped cells and restored phenotypes comparable to healthy controls in corrected cells.
Conclusions: iPSC-based models of laminopathies effectively recapitulate disease-associated phenotypes. These models can be utilised as a platform for the development of gene therapy approaches for laminopathies.
DC11From Genomes to Phenomes: Discovering DMPK Repeat Expansions in Genomics England as a Gateway for Future PheWAS
Rezbieara Rahman1,
Professor Elijah Behr2, Dr. Marta Futema2 and Dr. Emma Matthews1
1 City St. George’s University of London, Neuroscience and Cell Biology Research Institute, 2 City St. George’s University of London, Cardiovascular and Genomics Research Institute
rrahman@sgul.ac.uk
Background: Myotonic Dystrophy Type 1 (DM1) is an autosomal dominant disorder caused by an expansion of a CTG repeat sequence in the DMPK gene. Healthy individuals typically carry 5-37 repeats, while those in the premutation range (38-49 repeats) may be asymptomatic, risk intergenerational repeat expansion. Pathogenic expansions (>50 repeats) lead to DM1’s multisystemic manifestations and noted for its remarkable variability. Despite well-established clinical features, the population-level impact of DMPK expansions, particularly across different genetic ancestries, remains underexplored.
Aims: Leveraging the Genomics England (GEL) Research Environment with extensive whole-genome sequencing (WGS) data, we aim to (1) identify DMPK repeat expansions in GEL data, classifying them into cohorts, (2) compare repeat length distributions across ancestries, and (3) establish a genotype-phenotype dataset linking individuals to phenotypes using Human Phenotype Ontology (HPO) terms. Thus, laying the groundwork for a future phenome-wide association study (PheWAS) utilising this data. This research represents the start of the first application of an HPO-based PheWAS in a DM1 context.
Methods/Materials: We analysed 80,110 GEL whole-genome sequencing samples for DMPK expansions using Expansion Hunter, categorising participants into normal (<37 repeats), premutation (38-49 repeats), and pathogenic (>50 repeats) cohorts. Statistical analyses assessed ancestry-based patterns in repeat distributions.
Results: Among 80,110 genomes, we identified 78 participants with pathogenic expansions, 183 with premutation alleles, and 79,849 with normal repeat lengths. Significant ancestry-based differences were observed in comparisons between pathogenic vs. normal cohorts (p=0.038) and normal vs. premutation cohorts (p=0.003), p<0.05. Preliminary findings indicate that European ancestry may have a higher prevalence of DM1 and are more likely to have larger DMPK expansions than other populations, however this requires further validation.
Conclusion: This study identified significant ancestry-related differences in DMPK expansions, illustrating the role of ancestry in DM1 genetic epidemiology. Additionally, a robust HPO-linked database is being developed to support the planned PheWAS. Thus, paving the way for the first HPO-based PheWAS in a DM1 context, enabling the exploration of how DMPK expansions influence diverse traits. This will broaden our understanding regarding DM1 clinical phenotypes, disease progression, and undiagnosed cases, ultimately informing potential clinical approaches and management.
DC12Relationships between functional outcome measures and instrumented gait assessment in Facioscapulohumeral muscular dystrophy: preliminary findings
Robert Muni-Lofra 1, Emma Robinson 1, Philip Brown 3, Pete Waldock 1, Heather Hunter 3, Samantha Fitzsimmons 1, Meredith James 1, Lisa Alcock 2, Giorgio Tasca 1
1 John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University, Integrated Laboratory Medicine, Newcastle Upon Tyne Hospitals NHS Foundation Trust, UK, 2 Translational and Clinical Research Institute, Newcastle University, 3 The Newcastle Hospitals NHS Foundation Trust
Robert.muni-lofra@newcastle.ac.uk
Background: Facioscapulohumeral muscular dystrophy (FSHD) is a hereditary neuromuscular condition characterised by progressive muscle weakness affecting facial, shoulder and pelvic girdle muscles. The involvement of trunk and lower limb muscles leads to limitations in gait and balance including reduction in comfortable walking speed. This may be associated with reduced hip flexion, knee extension and ankle dorsiflexion strength.
Evaluating mobility limitations is usually restricted to clinical observations and scales. These approaches are susceptible to subjectivity and lack sufficient sensitivity to detect progression or evaluate therapeutic response. As such, objective markers of functional mobility are required.
Aims: To explore relationships between functional mobility and gait in FSHD.
Methods/Materials: Eleven participants with FSHD (age range: 30-74y, 5 males) were recruited in the natural history of neuromuscular disorders study.
A functional assessment was carried out using the North star assessment for limb girdle type muscular dystrophies (NSAD). Subscale scores were calculated for 1) lower limb strength and function (including sit to stand and standing on tiptoes) 2) general mobility (such as standing, squatting, and running).
Participants completed up to 4x 10-metre intermittent walks across an instrumented walkway (GAITRite, 240Hz) using usual orthotic and walking aids as required. Temporal spatial outcomes (step velocity, length, time and width) were extracted as mean values (all steps). Gait variability (consistency between steps) and asymmetry (absolute difference between right and left limbs) were also calculated.
Spearman rho correlations were used to investigate relationships (strength, direction and significance) between clinical and instrumented measures of mobility.
Results: Strong correlations were identified between functional mobility (General mobility and lower limb mobility sub scores) and gait (mean step velocity, step length, step and stance time, rho= 0.75-0.96, p<0.008). Similarly, functional mobility were strongly correlated with gait variability (step, stance and swing time, and step width; rho= 0.77-0.93, p<0.005). There were no significant correlations between Functional scores and gait asymmetry.
Conclusion: Reduced functional mobility was associated with impaired gait, higher temporal gait variability and lower step width variability. Preliminary evidence from a small cohort of patients with FSHD suggests that temporal spatial gait characteristics are clinically valid measures of functional mobility.
DC13The impact of losing the ability to sit to stand on social participation in people with dysferlinopathy: Clinical Outcome study for dysferlinopathy
Robinson E1
, James M.K
1
, Hilsden H
1
, Rufibach L2, Roper W.M3, Holsten S4, Lowes L.P5, De Monts C6, Yochai C7, Pardo A8, Ogasawara y9, Rudolph K10, Webber J11, Montiel Morillo E12, Birnbaum S13, Rojas J14 Mi Young K15, Nitollama P16, Mastellaro S 17, Mayhew A.G
1,
Straub V
1
, The Jain COS Consortium on behalf of the Jain Foundation2.
1 John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, The Newcastle upon Tyne Hospitals NHS Foundation Trust and Newcastle University, UK, 2 The Jain Foundation, Seattle, Washington, USA, 3 Department of Neurology, Washington University School of Medicine, St Louis, MO, USA, 4 Carolinas Neuromuscular Centre, Carolinas HealthCare System, Charlotte, NC, USA, 5 Nationwide Children’s Hospital, Columbus, OH, USA, 6 Department of Neurology and Neurological Sciences, Stanford University School of Medicine, Stanford, CA, USA, 7 Pediatric Neuromuscular Division, Columbia University Irving Medical Centre, New York, NY, USA, 8 Neuromuscular Area, Donostia University Hospital, Donostia-San Sebastian, Spain, 9 Department of Physical Rehabilitation, National Centre Hospital, National Centre of Neurology and Psychiatry Tokyo, Japan, 10 Copenhagen Neuromuscular Centre, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark, 11 Neurorehabilitación, Clínica Dávila, Santiago, Chile, 12 Physical medicine and rehabilitation, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 13 Institut de Myologie, Groupe Hospitalier Pitié-Salpêtrière, Paris, France, 14 Neuromuscular Unit, , Hospital U. Virgen del Rocío/Instituto de Biomedicina de Sevilla, Seville, Spain, 15 Pusan National University Yangsan Hospital, Yangsan, Republic of Korea, 16 Department of Neurology, MDA ALS and Neuromuscular Centre, University of California – Irvine, Orange, CA, USA, 17 Department of Neuroscience, University of Padova, Padova, Italy;
Emma-jayne.robinson@nhs.net
Emma.Robinson2@newcastle.ac.uk
Background: Individuals with limb girdle muscular dystrophy (LGMD) R2/2B (dysferlinopathy) lose the ability to stand up from a seated position (STS) without help prior to loss of ambulation. Clinically, individuals report this impacts their ability to socialise or to work, however there are no studies evaluating this.
Aims: To examine the impact of the loss of STS on social participation in individuals with dysferlinopathy.
Methods/Materials: We examined the baseline visit data of 205 participants in the Clinical Outcome study for Dysferlinopathy, a two-year, 16-site natural history study. Data analysed included scores of STS from the North Star assessment for limb-girdle type muscular dystrophies (NSAD), responses to the participant-reported Activity limitations for patients with upper and/or lower limb impairments (ACTIVLIM) and participant-reported responses to the Quality of Life in Genetic Neuromuscular Disease Questionnaire (QOLgNMD). The Chi square test for association (χ2) was used to test for a relationship between clinician-reported ability to STS and participant-reported ability to complete activities requiring STS with social participation. A small focus group (n=5) was carried out and analysed to explore the impact of losing the ability to STS. Both strands of data were merged for any convergence or divergence in results.
Results: Statistically significant associations were found between the following variables:clinician-reported ability to STS (NSAD) and patient-reported ability to get on/off a toilet, in/out of a car (ACTIVLIM), how often getting to the toilet restricted activities outside the home and how often participants felt able to leave the house alone (QOLgNMD). Loss of ability to STS was associated with reduced social participation, which can be detected by deterioration on NSAD or ACTIVLIM STS items. Conclusion: The use of equipment or support from others is helpful in managing difficulties with STS, which enables people with dysferlinopathy to remain socially active. Clinicians should proactively instigate early referrals to equipment and wheelchair providers after any deterioration on NSAD or ACTIVLIM STS scores, regardless of ambulatory status.
DC14Association between cardiac function and loss of ambulation in adults with Duchenne muscular dystrophy
Marianela Schiava1
, John P Bourke1, Jordi Díaz-Manera1, Anna Johnson2, Maha A Elseed1, Giorgio Tasca1, Kadhim Kadhim2, Volker Straub1, Chiara Marini Bettolo1, Michela Guglieri1.
1John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK, 2Newcastle Hospitals NHS Foundation Trusts, Newcastle upon Tyne, UK.
Background: Cardiomyopathy is a common co-morbidity in individuals with Duchenne muscular dystrophy (DMD) and has become the leading cause of death in DMD. With improved Standards of Care in DMD, leading to delayed in LOA and increased life expectancy, concerns have been raised that better-preserved skeletal motor function could aggravate the course of DMD-related cardiomyopathy by putting added stress on the heart.
Aims: The aim of this retrospective study was exploring the association between motor function, assessed as age at loss of ambulation (LOA) and late stage cardiomyopathy in adults with DMD, treated with including glucocorticoids and ACE inhibitors, according to the Standards of Care.
Methods: This is a retrospective study from a single highly specialized muscular dystrophy centre in the UK. The relationship between Left Ventricular ejection fraction percentage (LVEF%) and age at LOA was assessed by multiple linear regression analysis. As sensitivity analyses, additional models were created to consider the effect of respiratory dysfunction and genotype.
Results: Eighty four individuals (> 16 years old) with DMD were included. A positive correlation between later age at LOA and higher LVEF in adulthood was observed (linear regression estimate 1.49, 95% CI: 0.13–2.84, p=0.03). Sensitivity models excluding cardioprotective genotypes (absence of Dp116 isoform) and mild motor phenotypes (out of frame deletions amenable to exon 44 and 45 skipping) confirmed this association while models including age at respiratory impairment did not improve the model. Individuals who lost ambulation before age 11.92 (ROC AUC 0.73, 95% CI: 0.60–0.85) reached a LVEF <40% 5.21 years earlier than those who lost ambulation after that age (adjusted restricted mean survival time 19.08 vs 24.29 years, p<0.001).
Conclusion: The results may reduce concerns that prolonged ambulation is deleterious to longer-term cardiac function in DMD. This message is relevant in the era when potent disease-modifying treatments, such as gene therapy, advanced exon skipping, and antifibrotic molecules, are either under development or at the stage of clinical testing.These findings may suggest that prolonging ambulation does not impact cardiac function adversely in advance stages of DMD.
DC15Comorbidities and adverse events in FSHD: experience from the Resolve cohort
Iwona Skorupinska
a
, Enrico Bugiardinia, Louise Germaina, Jose M.S. Mengibara, Anna Ubialia, Russell Butterfieldb, Elena Carraroc, Nuran Dilekd, Bakri Elsheikhe, Kiley Higgsf, Katy Eichingerd, Nicholas Johnsong, Leann Lewisd, Doris G. Leungh, William B. Martensd, Michael McDermottd, Karlien Muli, Sabrina Sacconij, Valeria Sansonec, Perry Shiehk, Kathryn Wagnerh#, Michaela Walkerf, Leo H. Wangl, Rabi Tawild, Jeff Statlandf, and the ReSolve Investigators of FSHD CTRN.
a Queen Square Centre for Neuromuscular Diseases, UCL, London, United Kingdom, b University of Utah, UT, United States of America, c Centro Clinico NeMO Milano, Milan, Italy, d University of Rochester Medical Center, NY, United States of America, e The Ohio State University, OH, United States of America, f University of Kansas Medical Center, KS, United States of America, g Virginia Commonwealth University, VA, United States of America, h The Johns Hopkins School of Medicine, Kennedy Krieger Institute, Baltimore, MD, United States of America, i Radboud University, Nijmegen, Netherlands, j Nice University, Nice, France, k University of California, Los Angeles, CA, United States of America, l University of Washington, WA, United States of America
#Current affiliation: F. Hoffmann-La Roche, Basel, Switzerland
Iwona.skorupinska@nhs.net
Background: Facioscapulohumeral muscular dystrophy (FSHD) is the third most prevalent type of muscular dystrophy. While the treatment landscape is evolving there remains limited information regarding comorbidities associated with FSHD.
Aims: This study aims to assess comorbidities, concurrent medication use, and adverse events in a large cohort of FSHD patients whose inclusion criteria align with those used in clinical trials (Resolve study).
Methods: Data on comorbidities were obtained through self-reported history questionnaires. Medications were categorized by their intended use, and adverse events were documented over the two-year follow-up period of the study.
Results: A total of 235 participants were enrolled in the Resolve study, of whom 56% were male and 44% female, with a mean (range) age of 50.3 (19-75) years. The most frequently reported comorbidities included pulmonary (19%), cardiovascular (14%), hearing (20%), and vision problems (19%). Nine percent of participants required a breathing device, while 5% used hearing aids. Supplements (37%), analgesics (30%), and cardiovascular medications (23%) were the most commonly used treatments. Notably, 25% of analgesic usage was related to FSHD-associated pain. Over the course of the study, 63 participants (27%) experienced at least one adverse event, with the most common being falls (11%), musculoskeletal issues or injuries (17%), and blood draw-related effects like bruising (5%).
Conclusions: Patients with FSHD primarily have cardiorespiratory comorbidities. High rates of supplement and analgesic use were observed among participants who are potential candidates for clinical trials. Adverse events were primarily musculoskeletal, with falls being frequently reported during the study period. Additionally, psychological problems, including depression, were notably prevalent (23%).
‡DC16An exercise challenge system to define a universal proteomic signature of muscle injury in adult inherited myopathy and it’s use in a controlled clinical trial setting
MPG Stemmerik1, B Barthel2, SV Frølich1, NAM Receveur1, AW Slipsager1, JM Donovan2, J MacDougall2, AJ Russell2,
J Vissing1
1Department of Neurology, University of Copenhagen, 2Edgewise Therapeutics, Boulder, CO, USA
John.Vissing@regionh.dk
Background: Several inherited muscular dystrophies exhibit an enhanced injury response to exercise. However, current understanding of how circulating biomarkers of muscle injury are defined in different disorders is poorly understood.
Aims: We used an exercise intervention in adults with myopathy to characterize proteomic signatures of injury and then used this signature to assess the protective effects of a selective fast skeletal muscle myosin inhibitor, sevasemten.
Methods: We studied healthy volunteers, Becker muscular dystrophy (BMD), Limb-girdle muscular dystrophy types 2I (LGMD2I), and 2L (LGMD2L) using high intensity cycling and leg strength exercise to stress muscles. Blood samples were collected before and up to 24hrs after exercise and analyzed with SOMAscan 7K proteomics.
Results: In individuals with BMD and LGMD2I, we identified a signature of 26 proteins elevated at baseline and further elevated with exercise vs healthy individuals. Signature protein concentrations increased with time with most peaking at 2-4 hrs post injury. Proteins were predominantly enriched or exclusive to skeletal muscle. Finally, we used this injury signature to track muscle injury responses in a placebo-controlled exercise study with the sevasemten. We performed a 16-wk double-blind study in BMD, LGMD2I, and McArdle’s disease (McA; n=9, 9 and 3, respectively). After an exercise challenge, participants were randomized to sevasemten daily or placebo (2:1). At wk12, participants underwent a second exercise challenge. Sevasemten was well tolerated with no change in exercise parameters (pVO2 or 1RM) between 1st and 2nd exercise challenge. In BMD, sevasemten significantly reduced the injury signature by -41% (p<0.0001 vs. placebo). Post-exercise signature was also reduced. McA participants on sevasemten exhibited normalization of resting and post-exercise signature.
Conclusion: We have attempted to better define a signature of muscle injury in a selection of individuals with adult myopathy and successfully used this signature in a clinical trial setting to provide evidence of protective effects of sevasemten.
DC17A prospective, multicentric natural history study in paediatric TTN-related Congenital Myopathies - the TREATIN study: design and baseline characteristics
Gianpaolo Cicala1,2
, Amy Wolfe1,2, Maria Vanegas3, Teishel Joefield2, Jennie Sheehan3, Chris Clark1,2, Sniya Sudhakar1, Jessica Bilby1, Alex Schofield3, Francesco Muntoni1,2,5, Heinz Jungbluth3,4, Giovanni Baranello1,2,5, Anna Sarkozy1,2
1Great Ormond Street Hospital for Children NHS Foundation Trust, London, UK, 2Dubowitz Neuromuscular Centre, Institute of Child Health, University College London, London, UK, 3Department of Paediatric Neurology – Neuromuscular Service, Evelina London Children’s Hospital, Guy’s & St Thomas’ NHS Foundation Trust, London, UK, 4Randall Centre for Cell and Molecular Biophysics, Muscle Signalling Section, Faculty of Life Sciences and Medicine (FoLSM), King’s College London, 5UCL NIHR GOSH Biomedical Research Centre
Gianpaolo.cicala@gosh.nhs.uk
Background: Biallelic pathogenic TTN gene variants cause a form of congenital myopathy (TTN-CM) with mostly neonatal/paediatric onset and a wide range of associated histopathological features. Reliable natural history data and informative biomarkers are currently lacking. A natural history study for paediatric patients with TTN-CM started at Great Ormond Street and Evelina Children’s Hospitals, London, in January 2024, aiming to describe motor and respiratory function trajectories and identify suitable assessment tools to detect significant changes over time, with 6-monthly assessments for up to 18 months.
Aims: To describe TREATIN study design and baseline characteristics of recruited patients.
Methods/Materials: TTN-CM patients aged 0-18 years were recruited and seen at baseline. Patient demographics, clinical history, neurological examination, physiotherapy outcome measures (CHOP-INTEND, HINE2, motor function measure (MFM), 2 and 6-minute walking tests (2MWT, 6MWT), rise from floor, 4-stair climb, grip myometry, contracture assessment and spinal posture), lung function (LF) assessment including FVC, PEF, MIP/MEP and SNIP, muscle imaging (US and MRI) and self-reported questionnaires (MFI and Paeds FACIT) were collected.
Results: 21 patients had been recruited by November 2024. Mean age at baseline was 9.75 years (range 1.5-16.6 years). Time of presentation ranged from prenatal (19%), birth (23%) and post-neonatal (58%). At baseline, 67% of patients were ambulant, 47% had scoliosis, 33% needed respiratory and 28.5% feeding support. 14.2% had cardiac involvement The MFM32, completed in 16 patients, had a median total score of 74% (IQR: 59.3-86.9%). Domain 2 of the MFM, “proximal and axial function”, had the highest median score of 88% whilst domain 1, “standing and transfers”, scored the lowest (median score 54%; IQR: 31.2-73.9%). Baseline muscle US and MRI was performed in 7 and 15 patients, respectively, and 14 patients completed the full LF assessment. Detailed analysis of results is in progress.
Conclusion: This study will provide, for the first time, detailed natural history data of children with TTN-CM and improve trial readiness for this important emerging neuromuscular disorder.
DC18Identifying prognostic biomarkers in a large cohort of patients with dysferlinopathy
Bolano-Diaz C1
, Verdu-Diaz J1, James MK1, Hilsden H1, Jain COS Consortium2, Volker S1, Diaz-Manera J1.
1The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Central Parkway, Newcastle upon Tyne, UK, 2The Jain Foundation, Seattle, Washington, USA
Carla.bolano-diaz@newcastle.ac.uk
Background: Limb girdle muscular dystrophy-dysferlin related (LGMDR2) is an inherited muscle disease with a complex clinical spectrum, marked by variability in severity and progression, even within families. This complicates tailored care and clinical trial design. While some clinical and imaging factors have been identified to predict worse outcomes, they fail to explain all variability.
The Clinical Outcome Study for Dysferlinopathy (COS), the largest natural history study on LGMDR2, followed over 400 patients for 3 to 10 years, generating a vast dataset. Traditional statistics struggle to analyse its multidimensional variables, but artificial intelligence has shown promise in addressing these challenges effectively.
Aims: Identify prognostic biomarkers in a large cohort of patients with LGMDR2.
Methods: The COS 1 dataset was used, including demographic, clinical, genetic, and imaging of 188 patients. First, a machine learning (ML)-based pipeline was created to optimize data quality. Later, an ML-based model with nested-cross validation was built to identify relevant prognostic features and predict disease progression. Finally, AI explainability techniques were used to understand how these factors influenced progression.
Results: The North Star Ambulatory Assessment (NSAD) scale was used to measure disease progression. A regression line was fitted to each patient’s trajectory, and a model was built to predict the slope of these lines. Out of 70 included variables, seven were selected as the most relevant, without compromising the model’s accuracy (mean square error 3.65±2.36). Final variables included age, disease duration, baseline NSAD, creatinine phosphokinase, body mass index (BMI), forced vital capacity and six-minute walk test velocity.
The first 10 years of disease duration were closely associated to a steeper decline, followed by a plateau. Faster disease progression was linked to BMI values outside the normal range, whereas baseline NSAD scores above 45/54 related to a slower progression.
Conclusions: Seven relevant variables were identified to predict disease progression. Ten years of disease duration is a clear threshold, with patients plateauing past this point. Next steps include incorporating MRI data and developing separate models for early and late stages. These results are encouraging in our journey towards understanding LGMDR2 and improving patient care and clinical trial readiness.
Mitochondrial Disease
MD01Loss of the mitochondrial protease YME1L in the muscle leads to myofiber-type switch and metabolic dysfunction
Sebastian Kallabis2, Marcus Krüger2, Thomas Langer3,
Sofia Ahola1
1 Department of Metabolism and Systems Science, University of Birmingham, B15 2TT, UK, 2 CECAD, Centre of Excellence for Ageing Research, University of Cologne, Germany, 3 Max Planck Institute for Ageing Research, Cologne, Germany
s.ahola@bham.ac.uk
Background: Mitochondrial dysfunction, characterized by impaired oxidative phosphorylation and increased oxidative stress, plays a central role in the development of muscle diseases. Mitochondrial failure to meet the high energy demands of muscle tissue contributes to a range of muscle diseases, including mitochondrial myopathies, which are marked by muscle weakness, exercise intolerance, and progressive muscle degeneration. Mitochondrial metabolism is crucial in normal muscle development and differentiation, but the regulation of these processes is not well characterized. Mitochondria are the cellular hub of metabolism and control the utilization of different energetic substrates and the metabolic rate of the cell. Mitochondrial mass and protein composition match the metabolic demand of the cell and mitochondrial proteases have an important task regulating the mitochondrial protein machinery. YME1L is a mitochondrial inner membrane protease governing the mitochondrial proteome and fusion process and loss of YME1L leads to mitochondrial fragmentation. Muscle-specific YME1L KO mice are insulin hypersensitive and glucose intolerant due to systemic downregulation of insulin production. YME1L rewires mitochondrial metabolism in response to nutrition starvation and hypoxia. This signalling is mediated by the inhibition of mTORC1 complex that via regulating the lipid composition in mitochondrial membranes, activates YME1L. Once activated, Yme1l degrades import machinery complexes, and lipid transfer proteins and activates glutamine utilization allowing reductive carboxylation.
Aims: Determine the role of Yme1l-mediated mitochondrial remodelling in muscle differentiation and development
Methods/Material: We utilized Yme1l KO mice and C2C12 myoblast cell lines to study the role of mitochondrial metabolism in muscle differentiation. We analysed the fiber type composition from adult mice and performed a single fiber proteome to analyse the fiber-specific changes upon metabolic remodelling.
Results: Loss of YME1L leads to systemic metabolic alterations and muscle dystrophy mimicking mTORC1 hyperactivation phenotype and ageing. Oxidative muscles are more sensitive to metabolic remodelling in YKO muscles and show altered fiber type. Our C2C12 data shows that YME1L is needed for myotube differentiation and metabolic switch.
Conclusions: Mitochondrial protease YME1L is required to mediate mTORC1 signalling in muscle development and in adulthood.
MD02Modifier variants in metabolic pathways are associated with an increased penetrance of Leber’s Hereditary Optic Neuropathy
Eszter Sara Arany1, Catarina Olimpio2, Ida Paramonov3, Rita Horvath2#
1 Faculty of Medicine, Imperial College London, London, UK, 2Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK, 3Centro Nacional de Análisis Genómico (CNAG), Barcelona, Spain
Background: Leber’s hereditary optic neuropathy (LHON) is a debilitating mitochondrial disease characterized by acute or subacute painless bilateral vision loss, typically manifesting in the second or third decade of life. Despite being the most prevalent mitochondrial disorder, the precise pathophysiological mechanisms underlying LHON remain poorly understood, with only 50% of men and 10% of women with a disease-causing variant showing visual symptoms. Nuclear modifier genes have been long suspected to affect phenotype severity, however, previous studies have not identified specific cellular pathways implicated in disease penetrance. In recent years, autosomal recessive variants in nuclear genes were recognised to cause the typical LHON phenotype. This was proposed as a new autosomal recessive disease mechanism for LHON (arLHON). The association between nuclear variants and the phenotype makes the nuclear pathways disrupted in arLHON the strongest candidates to act as mitochondrial LHON (mLHON) modifiers.
Aims: The aims of the study were to identify specific biological pathways that are involved in modifying the penetrance of LHON.
Methods: In this study we systematically investigated a large cohort of symptomatic and asymptomatic patients carrying one of the three primary mitochondrial variants. We used various bioinformatics tools to identify relevant pathways.
Results: We identified several pathogenic variants amongst the affected individuals that were consistently linked to metabolic and complex I related pathways, mirroring those disrupted in arLHON. Our findings are consistent with the presence of a second hit in specific biological pathways impairing ATP production. We propose that in addition to the primary mitochondrial variant related complex I insufficiency, disruption in these nuclear pathways drives the clinical manifestation of LHON. Genes involved in these same pathways also emerge as exciting candidates for future association with arLHON.
Conclusion: The present study deepens our understanding of LHON’s pathophysiology and provides a new framework for identifying novel disease-modifying targets.
MD03Clinical and Biomarker Profiles in Primary Mitochondrial Diseases: insights for Diagnosis and Future Clinical Trials
Ignazio Giuseppe Arena1
, Emma Harrison1, Thiloka Ratnaike1, Katherine Schon1, Catarina Olimpio1, Zoe Golder1, Elizabeth Ashby1, Charlotte Addy1, Heather Biggs1, Jelle van den Ameele1,2, Patrick Yu Wai Man1, Rita Horvath1, Patrick Chinnery1.
1 Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK
ia454@cam.ac.uk
Background: Primary Mitochondrial Diseases (PMDs) are a diverse group of neurometabolic disorders, primarily caused by defects in the oxidative phosphorylation system (OXPHOS). The clinical manifestations of PMDs are highly variable, with differences in age of onset, severity, and disease progression.
Since the first pivotal description dating to the late 1980s, considerable progress has been made in understanding the genetic underpinnings of these diseases. Numerous studies have documented patient cohorts, aiding in the classification of the various mitochondrial syndromes identified so far. However, the overlap of symptoms and the complexity of the mechanisms driving this heterogeneity continue to complicate the diagnosis and management of PMDs. While no disease-modifying treatments currently exist for PMDs, establishing a genetic diagnosis is crucial for providing accurate genetic counseling to patients and families. Furthermore, it can help pave the way for the development of targeted clinical trials, informed by a deeper understanding of the disease. In this perspective, it is also crucial to find appropriate biomarkers to aid in the assessment and monitoring of PMD patients.
Aims: The aim of this study is to describe the clinical features of a cohort of patients affected by PMDs. Specifically, we aim to examine the phenotypic features of mitochondrial disorders from an unbiased perspective, seeking to identify distinguishing clinical features and comparing them with known and new blood-based biomarkers to find relevant associations.
Methods: We will approach this topic presenting the main mitochondrial syndromes presented by our cohort and focusing on the main symptoms/signs reported, and finally exploring the role of targeted functional biomarkers within the same cohort, which may offer insights into disease mechanisms and assist in the development of future clinical trials.
Results: 12 patients with nuclear and 58 mitochondrial mutations were assessed. Preliminary analysis of all patients (n=27) with m.3243A>G mutation indicates that some biomarkers, particularly neurofilaments, are organ-specific and related to the severity of the disease. The idea is that through the combination of these different biomarkers valuable information can be obtained in the diagnostic evaluation and monitoring of PMDs.
Conclusion: By delineating the clinical and biomarker profiles, we propose to enhance the understanding of mitochondrial diseases supplying possible improved diagnostic strategies in the differentiation from other inherited similar neurological condition and providing hopefully reliable markers for future clinical trials strategies.
MD04Deciphering the mechanisms of mitochondrial stress
Danielle Brister1,2,3
, Jack Collier1,2, Rita Horvath1,2
1Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK CN2 1TN, 2School of Clinical Medicine, University of Cambridge, Cambridge, UK CN2 1TN, 3Christ’s College, University of Cambridge, Cambridge, UK CB2 3BU
dlb56@cam.ac.uk
Background: Mitochondrial disease is a group of heterogenous disorders caused by mitochondrial dysfunction, which can activate the integrated stress response (ISR) involving expression of the transcription factor ATF4. Directly inhibiting oxidative phosphorylation triggers ATF4 expression via the OMA1-DELE1-HRI axis. How defective mitochondrial protein translation, a common cause of mitochondrial disease, is sensed and transmitted to the nucleus to activate stress responses remains unclear and appears to be somewhat independent of OMA1 and DELE1.
Aims: To uncover how defects in mitochondrial protein synthesis activate the integrated stress response.
Methods/Materials: We will perform a genome-wide CRISPR interference (CRISPRi) screen to identify genes involved in the integrated stress response. Mitochondrial stress and ATF4 activation will be induced by exposing our CRISPRi/ATF4 reporter HEK293T cell line to doxycycline which inhibits mitochondrial translation. After treatment, high-throughput sequencing of sgRNAs will be followed by data processing using the MAGeCK-iNC pipeline to identify genes that modulate the mitochondrial stress response. Negative control sgRNAs targeting non-essential genes and positive control sgRNAs known to activate the ISR will be included to ensure the quality and consistency of the screen. Top candidate genes will be validated using small interfering RNA knockdowns along with western blot and qPCR to confirm their role in the ISR activation. Access to mitochondrial disease patient cells will allow us to further explore the role of hits in disease.
Results: We have optimized treatment of HEK293T cells with doxycycline over a time-course and with different dosages, and have established oligomycin and chloramphenicol treatment protocols to offer additional mitochondrial triggers of the ISR. All conditions induce ATF4 expression within 24 hours. Using the genome-wide CRISPRi screen, we anticipate identifying key genes and pathways involved in modulating the ISR and ATF4 triggered by impaired mitochondrial protein translation.
Conclusion: This screen will provide valuable insights into the molecular mechanisms governing cellular responses to mitochondrial dysfunction. Additionally, it could provide potential pathway targets for therapeutic intervention in mitochondrial diseases linked to stress response dysregulation.
MD05The role of mtDNA release as a signalling molecule in mitochondrial myopathies
Emily Cross1, Marton Szabo1, Rhianna Yung1, Daniel Lagos1, Rita Horvath1
1Department of Clinical Neurosciences, University of Cambridge
Ec912@cam.ac.uk
Background: Mitochondria are responsible for various cellular processes including energy production, regulation of metabolism, and signalling stress. Mitochondrial dysfunction disrupts these systems, activating cellular stress and downstream effects like cell death. One specialized function of the mitochondria is their ability to respond to cellular demands by fusion and fission. Mitophagy is a form of mitochondrial fission whereby mitochondria degrade damaged components through the endo-lysosomal system. The vesicular components can be degraded internally or shuttled to the plasma membrane for cellular release via exocytosis. Various severities of mitochondrial stress confer these two pathways, although it is not fully understood which triggers the selection of one over the other. Several models studying these mechanisms have done so in the context of various inflammatory diseases, like Parkinsons’ disease. However, the role of the mitochondrial maintenance pathways and the release of mitochondrial content has been poorly described in the context of primary mitochondrial disease.
Aims: To assess the release of mitochondrial content into the cytosolic and extracellular spaces in acute and chronic models of mitochondrial stress and disease and the downstream effects.
Methods/Materials: To model acute mitochondrial stress, C2C12 myoblasts were treated with 5 nM Rotenone or 50 nM Antimycin-A for 48 hours. For a chronic model of mitochondrial disease, m.3243A>G myoblasts and POLG fibroblasts were treated in glucose or galactose media for 48 hours. From media, extracellular vesicles (EVs) were extracted using ultracentrifugation and assessed using immunoblotting and qPCR. Cells were assessed using immunofluorescence, immunoblotting, and RT-qPCR. Serum samples from control and mitochondrial disease patients were analysed for cytokine signatures using a multiplex panel.
Results: C2C12 myoblasts feature complex I-specific EV release and increased levels of mitochondrial DNA present in the cytosol, with decreased mtDNA in complex III inhibition. Primary m.3243A>G myoblasts exhibit cytosolic release of mtDNA with metabolic stress. Patient serum samples with different mitochondrial diseases show increased mtDNA, cytokines GDF-15 and IL-6, with potential IFN-y inhibition.
Conclusions: The release of mitochondrial content differs depending on the type of mitochondrial stress and signals stress response in skeletal muscle. In primary muscle cell models of mitochondrial disease, metabolic stress triggers mtDNA release and could potentially modulate the downstream inflammatory response.
MD06Understanding negative selection of mtDNA variants in the blood
Imogen G. Franklin1,2
, Paul Milne3,4, Jordan Childs1, Isabel Barrow1,3, Barbara Kronsteiner6, Susanna Dunachie6, Conor Lawless1,3, Gráinne S Gorman1,3,5, Yi Shiau Ng1,3,5, Matthew Collin3,4+, Oliver Russell13+, Sarah J. Pickett1,2+
1Mitochondrial Research Group, Newcastle University, Newcastle upon Tyne, UK, 2Biosciences Institute, Newcastle University, Newcastle upon Tyne, UK, 3Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, UK, 4Haematopoiesis and Immunity Laboratory, Newcastle University, Newcastle upon Tyne, UK, 5NHS Highly Specialised Service for Rare Mitochondrial Disorders, Newcastle upon Tyne NHS Foundation Trust, Newcastle upon Tyne, UK, 6Peter Medawar Building for Pathogen Research, Nuffield Dept. of Clinical Medicine, University of Oxford, UK,
+ denotes equal contributions
g.franklin2@newcastle.ac.uk
Background: Mitochondrial (mt)DNA disorders are a clinically heterogenous group of multisystemic diseases. One of the most prevalent pathogenic variants is m.3243A>G, which is associated with a highly varied phenotypic profile, making prediction of disease prognosis difficult. As mtDNA is a multi-copy genome, the proportion of mtDNA molecules that carry a pathogenic variant can vary - this is known as heteroplasmy. Unlike post-mitotic tissues, m.3243A>G heteroplasmy in the blood decreases with age; understanding what drives this decline is likely to give an invaluable insight into disease prognosis and may help to identify therapeutic targets.
Aims: To understand the negative selection of mtDNA variants in the blood.
Methods/Materials: Single cells and bulk populations were isolated via FACS for mtDNA and transcriptome sequencing, extracellular markers analysed using flow cytometry, and PBMCs stimulated in vitro with cell trace violet to assess proliferation.
Results and conclusions: By investigating m.3243A>G level within 15 immune populations from 26 affected individuals (18–66yrs; 11 male, 15 female), we observed enhanced mutation loss in six cell subtypes; this included all cells investigated within the T-cell compartment. Single cell analysis in six individuals supported these findings; all T-cell subsets exhibit a shift towards low mutation level cells compared to progenitor, myeloid and B-cell groups. This shift is more marked in memory compared to naïve T-cells and follows consistent trends between patients throughout T-memory cell differentiation. Notably, this pattern was also observed in patients with the m.8344A>G variant, which remains stable in whole blood with age. Flow cytometry data revealed m.3243A>G patients to have a lower proportion of T-cells than controls and higher expression of exhaustion marker PD-1, suggesting that m.3243A>G is important in blood homeostasis. Further in vitro studies indicated abnormal proliferative behaviours in patient samples. Parallel sequencing of mtDNA and the transcriptome in single cells revealed high levels of cellular stress and abnormal interleukin signalling in T-cells with high m.3243A>G levels. This work identifies a critical vulnerability of T-cells to pathogenic mtDNA, revealing a key role for mitochondrial function in maintaining T-cell homeostasis, potentially linked to cellular stress, enhanced T-cell exhaustion, and an altered proliferative response to stimulation.
MD07Investigating cellular responses to mitochondrial dysfunction in mitochondrial myopathies
T. Bernardino Gomes1,2,3
, V. Di Leo1, C. Warren1, A. Khan1,4, I. Barrow5, D. M. Turnbull1, G. S. Gorman3,5,6, C. Lawless1, A. E. Vincent1,2
1Mitochondrial Research Group, Translational and Clinical Research Institute, Newcastle University, UK, 2John Walton Muscular Dystrophy Research Centre, Newcastle University, Centre for Life, Newcastle Upon Tyne, NE1 3BZ, UK, 3NHS Highly Specialised Service for Rare Mitochondrial Disorders of Adults and Children, Directorate of Neurosciences, Newcastle upon Tyne Hospitals NHS Foundation Trust, UK, 4Centre for Doctoral Training in Cloud Computing and Big Data, Newcastle University, UK, 5Newcastle NIHR Biomedical Research Centre, Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK, 6Wellcome Centre for Mitochondrial Research, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne NE2 4HH, UK
Background: Mitochondrial diseases affect approximately 1 in 8,000 adults in the North East of England, often causing disabling muscle weakness, fatigue, and exercise intolerance. The unfolded protein response (UPR) and metabolic remodelling are implicated in both ageing and mitochondrial dysfunction; however, these pathways remain poorly characterised in the skeletal muscle of patients with mitochondrial myopathy. Understanding these pathways could reveal key disease mechanisms and inform targeted therapies.
Aims: This study investigated protein markers across pathways linked to mitochondrial biology and disease to uncover how muscle fibres respond to mitochondrial dysfunction at the cellular level.
Methods/Materials: Skeletal muscle biopsies from 19 patients with mitochondrial myopathy, caused by either single large-scale deletions (SLSD) or myopathic mtDNA maintenance disorders (MMD), were analysed using an Imaging Mass Cytometry (IMC) panel of 25 protein markers. These included markers of the UPR, oxidative phosphorylation (OXPHOS), mitochondrial dynamics, and one-carbon metabolism. Based on IMC data for the OXPHOS markers MT-ND4, MT-CYB, MT-CO1 and MT-ATP8, fibres were classified as deficient or non-deficient for complexes I, III, IV and V, respectively. Subsequently, Generalised Linear Mixed Models (GLMM) were used to compare deficient and non-deficient fibres with regards to other panel markers. Muscle tissues from 10 healthy controls were also investigated.
Results: The analysis included 48,472 individual fibres from patient tissues and 22,925 from control tissues. The GLMM analysis revealed a significant fold change (FC) increase in several protein markers in OXPHOS-deficient fibres, most prominently in MT-ATP8-deficient fibres, including TFAM (1.41), DLAT (1.65), HSPA9 (2.16), and HSPD1 (2.10). In contrast, C1QBP (1.31) was highest in MT-CYB-deficient fibres. Additionally, combined deficiencies in MT-ND4, MT-CO1, and MT-ATP8 affected 41.5% of patient fibres, whereas MT-CYB deficiency was rarer and co-occurred with other deficiencies in ∼8%.
Conclusion: The results suggest that accumulation of OXPHOS dysfunction is associated with increased markers of mitochondrial biogenesis (TFAM), metabolic remodelling (DLAT), and mitochondrial proteostasis and UPR (C1QBP, HSPA9, and HSPD1). This study represents the most comprehensive analysis of these markers in human tissues at the single-fibre level, helping to address the knowledge gap and informing the development of targeted, disease-specific treatments for mitochondrial myopathy.
MD08Bioinformatics Methods to Improve Diagnostic Rates for Primary Mitochondrial Disease in Lily Precision Diagnostics Project
Renata Kabiljo1
,2
, William L Macken1,2,3, Tamara Hill1, Jamie Leighton4, Charlotte Alston4,5, Robert W Taylor4,5, Robert McFarland4,5, Charulata Deshpande6, Suzie Walker7, Victoria Nesbitt8,9, Monika Olahova4,14,, Carl Fratter9, Katie Waller10, Maria E O’Hanlon10, Liz Curtis10, Alison Maguire11, Kathrine Schon12, Rita Horvath12, Patrick Chinnery12, Adelina Romano1, Robyn Labrum 2,13, Michael G Hanna1,2, Robert D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, 5NHS Highly Specialised Service for Rare Mitochondrial Disorders, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, 6Manchester Centre for Genomic Medicine, St Mary’s Hospital, Manchester, 7Diagnostic Discovery, Genomics England Limited, One Canada Square, London, 8Department of Paediatrics, Medical Sciences Division, Oxford University, Oxford, 9NHS Highly Specialised Service for Rare Mitochondrial Disorders, Oxford University Hospitals NHS Foundation Trust, Oxford, 10The Lily Foundation, Warlingham, Surrey, 11International Mito Patients (IMP), 12Medical Research Council Mitochondrial Biology Unit, University of Cambridge, Cambridge, 13Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 14Department of Applied Sciences, Faculty of Health and Life Sciences, Northumbria University, Newcastle upon Tyne, UK
r.kabiljo@ucl.ac.uk
Background: The Lily Precision Diagnostics Project aims to improve diagnostic rates for patients with suggestive phenotypes of Primary Mitochondrial Disease (PMD) who remain undiagnosed after NHS testing. This initiative tackles diagnostic challenges through enhanced bioinformatics pipelines, expanded gene panels, and emerging sequencing technologies, including long-read sequencing.
Aims: To utilize advanced bioinformatics methods and sequencing technologies to uncover missed diagnoses in PMD patients and improve understanding of disease mechanisms.
Methods/Materials: Enhanced bioinformatics pipelines incorporate state-of-the-art mitochondrial variant callers to accurately detect heteroplasmic variants, alongside specialized tools to identify and quantify mitochondrial deletions and duplications. Long-read sequencing enables phasing of both nuclear and mitochondrial variants, offering critical insights into complex cases. Comprehensive annotation and filtering techniques are applied to patient data to improve diagnostic yield.
Results: The project successfully identifies previously undetected heteroplasmic variants and structural rearrangements in mitochondrial DNA. Long-read sequencing facilitates the phasing of complex nuclear and mitochondrial variants, addressing diagnostic gaps. These advancements have improved the detection and interpretation of challenging cases, providing clarity for patients who had remained undiagnosed through standard testing approaches.
Conclusion: By integrating cutting-edge bioinformatics tools, long-read sequencing, and comprehensive analysis pipelines, the Lily Precision Diagnostics Project provides tools to significantly enhance the diagnostic accuracy for PMD. This approach not only improves patient outcomes but also contributes to a deeper understanding of mitochondrial disease mechanisms.
MD09Full gene deletion of COXFA4 causes cytochrome c oxidase deficiency and paediatric mitochondrial disease
Jamie K. Leighton
1, Lucie S. Taylor1,2, Alfredo Cabrera-Orefice3, Jean-Hubert Caberg4, Doriana Misceo5, Eirik Frengen5, Monika Oláhová1,6, Charlotte L. Alston1,2, Ilka Wittig3 and Robert W. Taylor1,2
1 Wellcome Centre for Mitochondrial Research, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, NE2 4HH, UK, 2 NHS Highly Specialised Service for Rare Mitochondrial Disorders, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, NE1 4LP, UK, 3 Functional Proteomics Group, Institute for Cardiovascular Physiology, Goethe University Frankfurt, 60590, Frankfurt am Main, Germany, 4 Department of Human Genetics, CHU de Liège, Domaine Universitaire du Sart-Tilman, 4000 Liège, Belgium, 5 Department of Medical Genetics, Oslo University Hospital and University of Oslo, 0450 Oslo, Norway, 6 Department of Applied Sciences, Faculty of Health & Life Sciences, Northumbria University, Newcastle upon Tyne, UK
j.k.leighton2@ncl.ac.uk
Background: Cytochrome c oxidase (COX; complex IV) is the terminal enzyme of the mitochondrial respiratory chain. COX comprises 14 protein subunits which originate from both the mitochondrial and nuclear genome. Complex IV assembly is centred around three catalytic core subunits and requires multiple distinct assembly factors. Previously assigned to complex I, the conversation surrounding NDUFA4 over the past decade has cumulated in the reassignment of the protein as a subunit of complex IV, alongside a proposed new name of COXFA4. COXFA4 variants causing human COX deficiency have previously been described in two unrelated families (PMID: 23746447, 38674434). Previously, we have presented two families with COXFA4 splicing variants, here we present two further unrelated families, each with an affected proband presenting with complex IV deficiency and harbouring homozygous allele mediated deletions encompassing COXFA4 (NC_000007.13).
Aims: To characterise the clinical and functional nature of whole gene deletions in COXFA4 leading to human COX deficiency and mitochondrial disease phenotypes.
Methods/Materials: Whole cell lysates, obtained from patient and age-matched control skeletal muscle and fibroblast biopsies, were subjected to SDS-PAGE and immunoblotting to assess steady-state levels of mitochondrial oxidative phosphorylation (OXPHOS) proteins and COXFA4 protein. Blue-Native (BN)-PAGE and high-resolution MS-based complexome profiling were applied to patient and control cell lines to assess mitochondrial OXPHOS complexes assembly.
Results and conclusions: While some data remain preliminary, biochemical assessment of respiratory chain enzyme activities in patient fibroblasts and skeletal muscle reveals a reduction in complex IV activity. SDS-PAGE immunoblotting alongside complexome profiling has demonstrated undetectable steady-state levels of patient COXFA4 protein. BN-PAGE investigations suggest a reduction in complex IV holoenzyme assembly and proteomic investigations highlight COXFA4 as a dynamic subunit of complex IV with a high turnover rate. The precise consequence of rare COXFA4 variants in patient cells remains under ongoing proteomic investigation. Extending this work will unravel the function of COXFA4 within mammalian cells, providing diagnostic clarity for these families.
‡MD10The Lily Precision Diagnostics Project for mitochondrial disease; A framework for boosting diagnostic rates for rare genetic disorders
William L Macken
1,2,3, Renata Kabiljo1,2, Jamie Leighton4, Charlotte Alston4,5, Monika Winter4,6, Robert W Taylor4,5, Robert McFarland4,5, Charulata Deshpande7, Suzie Walker8, Victoria Nesbitt9,10, Carl Fratter10, Katie Waller11, Maria E O’Hanlon11, Liz Curtis11, Alison Maguire12, Kathrine Schon13, Rita Horvath13, Patrick Chinnery13, Adelina Romano1, Robyn Labrum 2,14, Michael G Hanna1,2, Robert D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, 5NHS Highly Specialised Service for Rare Mitochondrial Disorders, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, 6Department of Applied Sciences, Faculty of Health and Life Sciences, Northumbria University, Newcastle upon Tyne, 7Manchester Centre for Genomic Medicine, St Mary’s Hospital, Manchester, 8Genomics England Limited, One Canada Square, London, 9Department of Paediatrics, Medical Sciences Division, Oxford University, Oxford, 10NHS Highly Specialised Service for Rare Mitochondrial Disorders, Oxford University Hospitals NHS Foundation Trust, The Churchill Hospital, Oxford, 11The Lily Foundation, Warlingham, Surrey, 12International Mito Patients (IMP), 13Medical Research Council Mitochondrial Biology Unit, University of Cambridge, Cambridge, 14Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London.
w.macken@ucl.ac.uk
Background: Diagnostics rates for suspected primary mitochondrial disorders (PMDs) have improved significantly over the last decade and the NHS now offers comprehensive molecular testing based on next generation sequencing. However, a diagnosis remains elusive for many patients. Barriers include the need to bioinformatically process and manually interrogate both mitochondrial DNA (mtDNA) and nuclear DNA (nDNA), the continuously growing number of genes with a phenotypic association, and the need to consider the vast array of phenocopies of mitochondrial syndromes. The Lily Foundation is the UK’s largest patient organisation supporting individuals impacted by PMD and is dedicated to improving the diagnostic pathway for PMDs in the UK.
Aims: 1. To improve the diagnostic rates for complex patients after routine NHS testing through bioinformatic innovations and emerging omic techniques. 2. To accelerate introduction of advance technologies in the NHS.
Methods/Materials: In partnership with the Lily Foundation, we have co-developed a 12 centre NIHR portfolio-adopted study with nationwide coverage. We placed emphasis on ease of recruitment through e-consenting and a straightforward phenotyping database. A central clinical and bioinformatic team assess and triage cases into (1) data reanalysis through bespoke bioinformatic pipelines, (2) advanced omic analysis (long read or RNA sequencing) or (3) functional validation. New diagnoses are formally interpreted and reported via the NHS Highly Specialised Services for PMD and reported back to clinicians. We also run two parallel initiatives (1) application of bespoke nDNA and mtDNA pipelines to undiagnosed mitochondrial cases in the National Genomic Research Library and (2) Iterative PPI on diagnostic experiences via the Lily IMPACT initiative.
Results: In the first five months we have recruited over 20 patients. We have identified diagnoses in both known disease associated and novel genes. Identification of new genetic conditions has also led to diagnoses in other individuals outside of the study. We have developed early pipelines for enhanced omics. Lily-PPI initiatives have led to the development of a qualitative study on diagnostic experience for PMD patients.
Conclusions: Collaborations harnessing academic expertise, the diagnostic NHS environment, and patient organisations can meaningfully boost diagnostic rates, and establish pathways for better omic technologies and improved patient experience.
MD11Long Read sequencing as a single diagnostic assay for suspected primary mitochondrial disease
William L Macken
1,2,3, Renata Kabiljo1,2, Aine Moylett1,2,4, Jessica Williams4, Alexander Ingell4, Elizabeth Scotchman4, Kathryn Oprych1,2, Chiara Pizzamiglio1,2, Enrico Bugiardini1,2, Esra Erdil1,2, Micol Falabella1, Natalie Chandler4, Cathy Woodward 2,4, Yogen Patel2,4, Robyn Labrum 2,4, Mary M Reilly1, James Polke2,4, Michael G Hanna1,2, Robert D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London.
w.macken@ucl.ac.uk
Background: The diagnosis of primary mitochondrial disorders (PMDs) currently relies on separate next generation sequencing (NGS) of both nuclear and mitochondrial DNA (nDNA, mtDNA). This sequential approach is time consuming and has several technical shortcomings. Over the last three years major improvements in the accuracy and cost effectiveness of long read sequencing (LRS) have for the first time made it possible to consider use of this technology in diagnostics.
Aims: 1. To conduct a pilot study investigating the practicality of introducing LRS into the diagnostic space. 2. To compare the utility of Pacific Biosciences (PacBio) and Oxford Nanopore Technologies (ONT).
Methods/Materials: We extracted high molecular weight DNA using the Qiagen MagAttract kit according to manufacturer instructions. We undertook full whole genome sequencing on a representative sample of known positive PMD patients including a single large scale mtDNA deletion, a single large scale mtDNA duplication, a maintenance defect including mtDNA deletions, a small indel, and dual pathogenic mtDNA variants using PacBio Revio and an ONT Promethion device.
Results: Both technologies delivered deep mtDNA coverage which was improved by the addition of an enzymatic treatment step to increased mtDNA linearisation. A larger DNA input size was required for PacBio sequencing than ONT, however this was ameliorated but the introduction of new SPRQ chemistry. Both technologies facilitated excellent resolution of single large-scale rearrangements and single molecule phasing of SNVs when compared with NGS. The PacBio ‘out of the box’ pipeline delivered accurate SNV calling. Raw ONT data required additional bioinformatic manipulation to remove false InDels. Calling of multiple heteroplasmic mtDNA deletions was challenging for both technologies and required bespoke re-engineering of NGS tools.
Conclusions: Both technologies are close to being ready for introduction into the clinical sphere and exhibit improved variant calling over NGS especially for large scale rearrangements. However, robust and maintained bioinformatic pipelines from industrial partners is required before NHS environments can support their use.
MD12Outcomes of a national specialised multi-disciplinary team meeting to aid diagnosis in complex primary mitochondrial disease cases
Áine Moylett1,2,4, William L Macken1,2, Esra Erdil1,2, Chiara Pizzamiglio1,2, Enrico Bugiardini1,2, Renata Kabiljo1,2, Amanda Lam1,2, Kathryn Oprych1,2, Cathy Woodward2,4, Yogen Patel2,4, Padraig Flannery2,4, Robyn Labrum2,4, James Polke2,4, Michael G Hanna1,2, Robert D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London.
a.moylett@nhs.net
Background: Primary mitochondrial diseases (PMDs) are a group of clinically heterogenous, multi-system disorders. Diagnosis of PMDs often involves input from several healthcare disciplines and interpretation of clinical, biochemical, histological, and genetic information. With the expansion of genomic testing, variants in PMD genes are increasingly identified in the NHS. At our centre, this has led to an increase in the identification of VUSs, incidental findings of mtDNA variants, often at low level, and unanticipated diagnoses of PMDs. Interdisciplinary collaboration with support from expertise in PMDs is needed to determine the most appropriate investigations to maximise diagnosis.
Aims: Formation of a national MDT meeting for complex PMD genomic findings to improve diagnose and counselling and to support non-mitochondrial clinicians.
Methods / Materials: The NHS Highly Specialised Service for Rare Mitochondrial Disorders started a local MDT meeting for complex PMD cases in May 2024. Due to increased demand, the MDT was expanded to include national and international cases.
Results: The first complex MDT meeting began in May 2024. Since its inception, 13 local and 22 national and international cases have been discussed. Case specific strategies were determined following discussion between clinicians and clinical scientists. Testing enzyme levels, genetic testing in other tissue types, proteomic and functional follow-up has all been employed to resolve VUS classification. 3 cases have had VUS classifications upgraded, through testing ubiquinone levels in muscle, increasing the genotype-phenotype corelation of the variant. 10 cases are undergoing further functional work to inform variant classification. Patients have been recruited to research studies including gene agnostic approaches, RNA sequencing and long read sequencing, identifying disease causing variants which would not have been detected through routine diagnostic testing. Additionally, 4 cases with mitochondrial DNA variants were determined to be incidental findings, leading to improved counselling for families. The variation in follow-up investigations to achieve better resolution of variants, or find an alternative diagnosis emphasises the need for multi-disciplinary collaboration for diagnosis of PMDs.
Conclusion: The formation of this national MDT meeting has led to improved diagnosis and outcomes for patients through personalised investigations, demonstrating the utility of a multi-disciplinary approach for complex PMD cases.
‡MD13RTN4IP1 is essential for the final stages of mitochondrial complex I assembly and coenzyme Q biosynthesis
Monika Oláhová1,2
, Rachel M. Guerra3, Jack J. Collier1,4, Juliana Heidler5,6,7, Kyle Thompson1, Chelsea R. White3, Paulina Castañeda-Tamez5,6, Alfredo Cabrera-Orefice5,6, Robert N. Lightowlers8, Zofia M. A. Chrzanowska-Lightowlers8, Ilka Wittig5,6,9, David J. Pagliarini3,10,11 and Robert W. Taylor1,12
1 Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, UK, 2 Department of Applied Sciences, Faculty of Health & Life Sciences, Northumbria University, Newcastle upon Tyne, UK, 3 Department of Cell Biology and Physiology, Washington University School of Medicine, St. Louis, MO 63110, USA, 4 Department of Clinical Neurosciences, John Van Geest Centre for Brain Repair, University of Cambridge, Cambridge, UK, 5 Center for Functional Proteomics, Faculty of Medicine, Goethe University, 60590 Frankfurt am Main, Germany, 6 Institute for Cardiovascular Physiology, Faculty of Medicine, Goethe University, 60590 Frankfurt am Main, Germany, 7 University Clinic of Vascular Surgery, Innsbruck Medical University, Anichstr. 35, A-6020 Innsbruck, Austria, 8 Mitochondrial Research Group, Biosciences Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, UK, 9 German Center for Cardiovascular Research (DZHK), Partner site RheinMain, Frankfurt, Germany, 10 Department of Biochemistry and Molecular Biophysics, Washington University School of Medicine, St. Louis, MO 63110, USA, 11 Department of Genetics, Washington University School of Medicine, St. Louis, MO 63110, USA, 12 NHS Highly Specialised Service for Rare Mitochondrial Disorders, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
monika.winter@northumbria.ac.uk
Background: A biochemical deficiency of mitochondrial complex I (CI) underlies ∼30% of cases of primary mitochondrial disease, yet the inventory of molecular machinery required for CI assembly remains incomplete. We previously characterised patients with isolated CI deficiency caused by segregating variants in Reticulon-4-Interacting Protein 1 (RTN4IP1), encoding a mitochondrial NAD(P)H oxidoreductase. Pathogenic variants in the RTN4IP1 gene have been associated with optic atrophy and multisystem mitochondrial disease, yet the mechanistic role of this protein in mitochondrial function is not clearly understood.
Aims: To further investigate the molecular function of the poorly-characterised mitochondrial protein RTN4IP1.
Methods/Materials: To investigate the molecular functions of RTN4IP1 we used patient-derived primary fibroblasts and generated a tractable model cell system (U2OS) lacking RTN4IP1 using CRISPR/Cas9 technologies. Immunoblotting, proteomic and targeted lipidomic analysis, high-resolution complexome profiling and respirometry were used to assess the biological role of this orphan mitochondrial protein.
Results: Characterisation of RTN4IP1-deficient cells showed a marked decrease in the steady-state levels of fully assembled mitochondrial CI and its subunits, suggesting that RTN4IP1 is a bona fide CI assembly factor. Stable overexpression of RTN4IP1 restored the levels of most downregulated CI subunits in the RTN4IP1 knockout cell line closer to wild type levels, demonstrating that defective RTN4IP1 causes CI-deficiency. Complexome profiling of both, patient fibroblasts and RTN4IP1-knockout cells revealed accumulation of unincorporated late-stage CI ND5-module and impaired N-module production. In addition to its’ role in CI assembly, targeted lipidomic analysis revealed that loss of RTN4IP1 function also leads to defects in coenzyme Q biosynthesis pathway.
Conclusion: In summary, our data reveal that RTN4IP1 plays an essential role in both the terminal stages of mitochondrial CI assembly and in coenzyme Q metabolism, and that pathogenic RTN4IP1 variants impair both functions in patients with mitochondrial disease.
MD14Muscle DNA Whole Genome Sequencing identifies mtDNA deletion signatures with diagnostic implications for genetic and acquired myopathies.
KB Oprych1,2
, WL Macken1, 2, 3, R Kabiljo1,2, A Moylett1,2,4, J Williams4, C Pizzamiglio1,2, E Bugiardini1,2, E Erdil1,2, M Falabella1, C Woodward 2,4, Y Patel2,4, R Labrum 2,4, MM Reilly1, J Polke2,4, MG Hanna1,2, RDS Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London.
k.oprych@ucl.ac.uk
Background: Mitochondria-related muscle dysfunction is reported in aging, inclusion body myositis (IBM), genetic myopathies and mitochondrial myopathies. Histological changes (including COX negative fibres and ragged red fibres) and molecular changes (depletion in mtDNA copy number and accumulation of mtDNA deletions) are seen across these conditions and may result in diagnostic uncertainty, particularly in atypical clinical presentations. There is preliminary evidence that mitochondrial disease, IBM and aging may have discriminatory hallmarks in the patterns of mtDNA deletions. However, studies to date may be biased by PCR enrichment and are limited by small numbers of samples and genes studied.
Aims: To identify mutational signatures between primary, acquired, and age-related mtDNA deletions.
Methods: Genomic DNA was extracted from fresh frozen muscle samples and PCR-free whole genome sequencing undertaken. Mitochondrial DNA reads were extracted and studied using the MitoSALT bioinformatic tool. Results were compared with clinical gold standard sequencing (next generation sequencing on long range PCR-enriched mitochondrial DNA).
Results: An apparent abundance of large deletions was observed with PCR-enriched samples. In addition, discrete differences were demonstrated in deletion patterns between age-related, non-mitochondrial and mitochondrial myopathies including number of deletions seen, deletion break points and degree of mtDNA ablation.
Conclusions: Mitochondrial DNA deletion signatures may offer a new diagnostic tool for undiagnosed myopathies and evidence towards or against pathogenicity in the classification of variants of uncertain significance. Age related mitochondrial dysfunction can be discriminated from true primary muscle disease by whole genome sequencing and deletional analysis.
‡MD15Results from the first longitudinal magnetic resonance imaging and spectroscopy study in primary mitochondrial myopathies
Chiara Pizzamiglio1,2
, Marzena Arridge3, Amy McDowell3, Jasper Morrow1, Gita Ramdharry1, Michael G. Hanna1,2, John S Thornton3, Robert D.S. Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, UK, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, Queen Square Centre for Neuromuscular Diseases, The National Hospital for Neurology and Neurosurgery, London, UK, 3Neuroradiological Academic Unit, UCL Queen Square Institute of Neurology, London, UK
c.pizzamiglio@ucl.ac.uk
Background: Primary mitochondrial myopathies (PMM) are genetic disorders with defects of the oxidative phosphorylation affecting predominantly the skeletal muscles. Currently, there are no disease modifying therapies for PMM. One difficulty to clinical trials in PMM is the lack of reliable and reproducible biomarker that can capture the disease severity and progression.
Aims: This is the first study aiming to examine the biomarker validity of MRI quantified muscle fat fraction (FF), cross-sectional area (CSA), diffusion, and phosphorous magnetic resonance spectroscopy (31P-MRS) measures of thigh muscles before, during, and after a knee extension/flexion exercise with tailored ankle weight, in PMM.
Methods/Materials: We did a prospective observational cohort study of genetically confirmed PMM patients. Age and sex-matched healthy subjects (HS) were also recruited. Assessments were done at baseline and 12 months. The MRI session consisted of quantitative MRI (FF, CSA, diffusion) of the thighs bilaterally, and surface-coil 31P-MRS of the left thigh. For each session of the 31P-MRS, we fitted a mono-exponential function to the recovery curve (averaged over two runs on a day) to obtain the time constant (TC) of phosphocreatine (PCr) resynthesis.
Results: Thirty subjects were recruited (10 HS, 10 m.3243A>G and 10 single deletion of mitochondrial DNA). All patients had muscle involvement (fatigue and/or muscle weakness). At baseline, the CSA of both thighs was reduced in PMM vs. HC (p=0.035). The FF did not show any difference in PMM vs. HC. However, on dividing the PMM participants into the 2 sub-groups, the FF was increased in subjects with single deletion (p=0.034) but not in the 3243 group. The longitudinal analysis did not show any significant reduction of the CSA, however there was an increase in thigh FF over 1 year in the PMM group (p=0.04). The diffusion sequence did not show any difference in the mean diffusivity and fractional anisotropy between PMM and HC. With regards to the 31P-MRS, the TC of PCr recovery is significantly longer in PMM vs. HC (p<0.01).
Conclusion: Muscle involvement is heterogeneous within the PMM group. MRI and 31P-MRS might be valuable PMM biomarkers and might be useful to better stratify participants for clinical trials.
MD16Use of computerised neurocognitive assessments in adults with mitochondrial disease as a clinical trial outcome measure
Pogoryelova O1-
3
, Smeitink J4, Renkema H4, Barrow I1-3, Barton F1, Lyon R1, Newman J1-3, Moe A.1-3, Ng Y.S1-3, Gorman G.1-3
1 Wellcome Centre for Mitochondrial Research. Translational and Clinical Research Institute. Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne NE2 4HH, UK, 2 Newcastle NIHR Biomedical Research Centre, Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK, 3 NHS Highly Specialised Service for Rare Mitochondrial Disorders of Adults and Children, Directorate of Neurosciences, Newcastle upon Tyne Hospitals NHS Foundation Trust, 4 Khondrion BV, Nijmegen, The Netherlands
o.pogoryelova@nhs.net
Background: Primary mitochondrial diseases (PMD) often affect tissues with high energy demands, such as the brain, muscles, and heart. While cognitive impairment and neurodegeneration can be present in some forms of PMD, they do not occur in all cases. Despite the widespread prevalence of these symptoms in certain forms, only supportive management is available for most PMDs. Recent clinical research has focused on improving cognitive performance in affected individuals, but the variety of neurocognitive assessments used across studies introduces significant heterogeneity. Therefore, an accurate, standardized assessment tool is crucial to monitor cognitive deficits and evaluate novel therapies effectively.
Aims: This study aims to assess the suitability of computerized cognitive assessments for clinical research in PMD and to capture variability and confounding factors influencing performance.
Methods/Materials: The study includes two cohorts: prospectively recruited Newcastle cohort and data from the KHENERGYZE clinical trial, for this study we used data from the trial screening assessments. Adult patients with genetically confirmed PMD underwent cognitive assessments using the Cogstate battery and Test of Attentional Performance, with paper-based assessments (Addenbrookes and Montreal Cognitive Assessment) as comparators. Fatigue, anxiety, and depression were also assessed.
Results: Newcastle cohort comprises 45 patients, KHENERGYZE cohort has 27 patients. Both cohorts showed similar disease burden and a significant prevalence of fatigue. Cogstate assessment outcomes were statistically indistinguishable between the two cohorts. Computerized assessments revealed attention deficits and slower processing speeds in a significant portion of the patients, highlighting the importance of reaction time in cognitive impairment in PMD.
Conclusion: Computerized cognitive assessments are valuable for detecting mild to moderate cognitive impairment in PMD and correlate well with traditional methods, supporting their use in clinical research. The use of two independent cohorts allowed better overview of variability in performance and reproducibility of the statistical correlations. The study also highlights the prevalence of fatigue in PMD.
MD17Heterogeneity of Mitochondrial Disease: Implications for Clinical Trials and Patient Care
Dr Naomi Thomas
, Professor Robert McFarland, Professor Grainne Gorman, Dr Yi Ng, Dr Jane Newman, Dr Oksana Pogoryelova
Affiliations (all authors)
1.Wellcome Centre for Mitochondrial Research. Translational and Clinical Research Institute. Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne NE2 4HH, UK 2.Newcastle NIHR Biomedical Research Centre, Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK, 3.NHS Highly Specialised Service for Rare Mitochondrial Disorders of Adults and Children, Directorate of Neurosciences, Newcastle upon Tyne Hospitals NHS Foundation Trust
naomi.thomas@newcastle.ac.uk
Background: Mitochondrial diseases are a heterogeneous group of disorders, characterised by diverse clinical phenotypes even within the same genotype. Involvement of multiple organ systems results in significant disease burden and comorbidity.
Aims: Understanding this complexity is critical not just for clinical care, but also for tailoring clinical research; we aim to address this issue.
Methods/Materials: To explore the extent and impact of this heterogeneity, we analysed data from the MitoCohort. This is a natural history study and patient registry of over 2000 patients with mitochondrial disease, collected from patients seen by the NHS Highly Specialised Services. It integrates patient and clinician-reported data, including the Newcastle Mitochondrial Disease Adult Scale (NMDAS - a standardised tool for assessing disease burden) and pathology results.
We also independently collected medication records for the last 500 patients visiting the Newcastle-Upon-Tyne mitochondrial clinic, to establish the extent of polypharmacy.
Results: By systematically characterising the heterogeneity of mitochondrial disease, and ensuring the full spectrum of disease burden is accounted for, we emphasise the importance of patient-centred approaches in both clinical care and research: particularly for clinical trial design. Within the mitochondrial disease population, the majority are often precluded by from participating in conventionally designed clinical trials, because eligibility criteria fail to reflect the complex nature of the condition. Trials may fail to meet outcome measures for failing to anticipate complicating factors.
Conclusion: We suggest mitigations in trial design to allow wider inclusion and improve success in achieving trial outcomes.
The strategy of carefully defining and adapting to the specific needs and complexities of individuals within the target population is applicable to trials design for other rare or clinically diverse disorders. Ensuring the design of an intervention reflects the population it is intended for should result in both better patient representation, and higher chances of success.
MD18Avoidance of tissue sampling for primary mitochondrial disease investigation may lead to sub optimal diagnostic rates
Jessica Williams1,2,4, William L Macken1,2, Aine Moylett1,2,4, Renata Kabiljo1,2, Kathryn Oprych1,2, Elizabeth Scotchman4, Cathy Woodward2,4, Yogen Patel2,4, Robyn Labrum2,4, James Polke2,4, Michael G Hanna1,2, Robert D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 2NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 3North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 4Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London.
jessica.williams102@nhs.net
Background: In the era of whole genome sequencing the investigation of primary mitochondrial disorders is increasingly undertaken using blood DNA in the absence of tissue samples.
While this less invasive approach has obvious advantages, it may result in suboptimal diagnostic rates. As blood cells have a high rate of turnover, deleterious mtDNA variants may be selected against and become absent from blood cells especially in older patients.
In addition, blood samples are less amenable to mitochondrial functional investigations than blood samples.
Aims: To investigate the potential for overlooked diagnoses if tissue samples are not collected.
Methods and Materials: We audited patients attending the NHS Highly Specialised Service for Rare Mitochondrial Disorders over a 1 year period and collected data regarding whether a diagnosis would have been missed if an invasive tissue sample was not available for analysis.
Results: 12.9% of PMD patients had a muscle-specific variant absent from other tissues which would have been missed without a diagnosis. This is in comparison to the estimates rate of 11.5% of muscle specific mutations. 2 cases were noted in which ubiquinone levels was normal in blood but low in muscle tissue leading to the upgrade of a VUS to likely pathogenic. Additionally, a case in which a POLG variant would have been incorrectly classified as a VUS without the identification of depletion through a muscle biopsy. Finally, 30 cases in which high levels of multiple deletions were identified in the absence a variant in a nuclear gene which could have been in appropriately dismissed as a non PMD case.
Conclusions: While non-invasive approaches have clear advantages, there is potential for diagnostic inaccuracy, and wasted expense if a one size fits all approach is taken and tissue samples are no longer gathered.
‡MD19Improving diagnosis of mtDNA disease using MitoHPC: preliminary results from 70,254 rare disease participants in the 100,000 Genomes Project
Ji-Ming Yang
1,2, Renata Kabiljo3,4, William L Macken3,4,5, Sinan Shi2, Michael G Hanna3,4, Robert D S Pitceathly3,4 Patrick F Chinnery1,2, Katherine R Schon6,7
1Medical Research Council Mitochondrial Biology Unit, University of Cambridge, Cambridge, 2Department of Clinical Neurosciences, University of Cambridge, Cambridge, 3Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 4NHS Highly Specialised Service for Rare Mitochondrial Disorders, The National Hospital for Neurology and Neurosurgery, London, 5North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, 6Department of Medical Genetics, University of Cambridge, Cambridge, 7East Anglian Clinical Genetics, Cambridge University Hospitals NHS Foundation Trust, Cambridge
jmy30@cam.ac.uk
Background: Pathogenic mitochondrial DNA (mtDNA) variants are individually rare and can cause a variety of single organ or multi-system disorders. Testing for mtDNA variants has traditionally relied on highly specialist laboratories, whilst mtDNA genes have not been routinely analysed in whole genome sequencing (WGS) and whole exome sequencing (WES) data. MitoHPC is a pipeline which can accurately identify mtDNA variants and heteroplasmy fractions from WGS data. In previous sequencing-based studies, analysing mtDNA has shown a diagnostic uplift in specific disorders. However, mtDNA analysis has not been performed systematically across a large rare disease cohort.
Aims: 1. To improve the diagnostic rates for rare disease patients in the 100,000 genomes project. 2. To guide which mtDNA genes should be included on virtual panels for different clinical indications in rare disease patients.
Methods/Materials: The MitoHPC pipeline was applied in 70,254 rare disease participants and family members who had WGS data in the 100,000 Genomes Project. They were recruited from Genomic Medicine Centres in England between 2015-2018. DNA was extracted from blood. Variants were filtered using against MITOMAP confirmed and ClinVar (likely) pathogenic variants.
Results: MitoHPC ran efficiently for 69,942/70,254 samples (99.6%) on the High Performance Computing Cluster in the Genomics England Trusted Research Environment. 666 participants were identified with a MITOMAP confirmed variant and/or ClinVar (likely) pathogenic variant at heteroplasmy ≥ 5%. The commonest pathogenic variants were m.1555A>G, m.14484T>C, m.11778G>A and m.3243A>G. 24 families with previously diagnosed mtDNA disease were successfully identified. To date, we have contacted the clinicians for 45 families with suspected new diagnoses. Diagnostic categories of these patients include retinal disorders, inherited optic neuropathy, congenital hearing impairment, hypertrophic cardiomyopathy, intellectual disability, epilepsy, hereditary dystonia, and hereditary ataxia.
Conclusions: MitoHPC provided a reliable and computationally efficient way of identifying heteroplasmic and homoplasmic mtDNA variants from WGS data. There were new mtDNA diagnoses across multiple diagnostic categories. Diagnostic panels should be reviewed to ensure that all appropriate mtDNA genes are included in the analysis.
This research was made possible through access to data and findings in the National Genomic Research Library via the Genomics England Research Environment.
MD20AAV-based liver-targeted gene therapy for MNGIE: proposal for a clinical trial
Jelle van den Ameele
1,2, Emma Cutting2, Kerry Dresser2, Ignazio Giuseppe Arena2, Emma Harrison2, Heather Biggs2, Caterina Garone3,4, Ramon Marti5
1 MRC Mitochondrial Biology Unit, University of Cambridge, Cambridge, UK, 2 Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK, 3 Department of medical and surgical sciences, Alma Mater Studiorum University of Bologna, Italy, 4 UOC Neuropsichiatria dell'età pediatrica, IRCCS Istituto delle Scienze Neurologiche di Bologna, Italy, 5 Vall d’Hebron Research Institute, Universitat Autònoma de Barcelona, and Biomedical Network Research Centre on Rare Diseases (CIBERER), Instituto de Salud Carlos III, Barcelona, Catalonia.
Jv361@cam.ac.uk
Background: Mitochondrial NeuroGastroIntestinal Encephalomyopathy (MNGIE) is an autosomal recessive disease caused by loss-of-function mutations in TYMP, the gene encoding the enzyme thymidine phosphorylase (TP). TP deficiency leads to systemic accumulation of the nucleosides thymidine (dThd) and deoxyuridine (dUrd). This results in an imbalanced pool of mitochondrial deoxyribonucleoside triphosphates (dNTPs), causing mtDNA maintenance defects, eventually leading to a defect of oxidative phosphorylation and the clinical phenotype.
MNGIE is an ultra-rare, fatal, but in principle treatable neurodegenerative condition. The most debilitating symptoms are severe gastrointestinal dysmotility, cachexia, myopathy and neuropathy, with median age of death ∼35years. Current treatment options are hematopoietic stem-cell (HSCT) or liver transplantation (LT), which restore normal TP activity in blood-/liver-cells, to reduce circulating dThd/dUrd levels and stabilise or improve symptoms. However, these procedures are associated with significant limitations, risks and mortality in affected individuals who often have multiple MNGIE-related co-morbidities.
Aims: We have previously obtained evidence that administration of the TYMP coding region using a liver-targeted AAV2/8-vector is effective at reducing dThd/dUrd levels and preventing some neurological and motor dysfunction in mouse models of MNGIE. We aim to bring this gene-therapy to patients through pre-clinical toxicity and biodistribution studies, a natural history study, and a Phase I/II clinical trial to test safety and biochemical efficacy (dThd/dUrd levels).
Methods and Results: We have partnered with the UKRI/LifeArc Innovation Hubs to develop GMP vector manufacturing, conduct pre-clinical toxicity/biodistribution studies, prepare regulatory applications, and complete all requirements to obtain approval and funding for a clinical trial. Patient and public involvement has already been instrumental to project development, supported by the Lily Foundation. An international multicentre retrospective natural history study is currently in set up, to better characterize the clinical phenotype and evaluate biomarkers, including in patients after LT/HSCT.
Conclusion: MNGIE is an ultra-rare and fatal condition, but the most obvious and trial-ready gene therapy candidate among all mitochondrial diseases. We are currently removing the remaining obstacles between proof-of-concept and clinical translation of a gene therapy for MNGIE.
Peripheral Neuropathy
PN01Natural history of Cerebellar ataxia, neuropathy, and vestibular areflexia syndrome (CANVAS)
Riccardo Currò1,2
, Nehzat Koohi3,4, Ferran Prados5,6,7, Gorka Fernandez-Eulate8, Chiara Pisciotta9, Amanda Heslegrave10,11, Elisa Vegezzi12, Ilaria Quartesan2, Alexander Rossor1, Michael Lunn1,13, Gita Ramdharry1,13, Tarek Yousry14, Henrik Zetterberg10,11,15, Diego Kaski3,4, David Gosal16, Davide Pareyson9, Paola Giunti17, Tanya Stojkovic8, Marios Hadjivassiliou18, Sheng-Han Kuo19,20, Henry Houlden1, Mary M Reilly1,13, Andrea Cortese1,2
r.curro@ucl.ac.uk
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, United Kingdom, 2Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy, 3Department of Clinical and Movement Neurosciences, UCL Queen Square Institute of Neurology, London, United Kingdom, 4The Ear Institute, University College London, London, United Kingdom, 5Queen Square Multiple Sclerosis Centre, Department of Neuroinflammation, UCL Institute of Neurology, London, United Kingdom, 6Centre for Medical Image Computing (CMIC), Department of Medical Physics and Biomedical Engineering, University College London, London, United Kingdom, 7e-Health Center, Universitat Oberta de Catalunya, Barcelona, Spain, 8Nord/Est/Ile-de-France Neuromuscular Reference Center, Institute of Myology, Pitié-Salpêtrière Hospital, APHP, Paris, France, 9Unit of Rare Neurological Diseases, Department of Clinical Neurosciences, Fondazione IRCCS Instituto Neurologico Carlo Besta, Milan, Italy, 10Department of Neurodegenerative Disease, UCL Institute of Neurology, London, United Kingdom, 11UK Dementia Research Institute, University College London, London, United Kingdom, 12IRCCS Mondino Foundation, Pavia, Italy, 13Queen Square Centre for Neuromuscular Diseases, National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, United Kingdom, 14Neuroradiological Academic Unit, Queen Square Institute of Neurology, University College London, London, United Kingdom, 15Institute of Neuroscience and Physiology, Goteborgs Universitet, Goteborg, Sweden, 16Manchester Centre for Clinical Neurosciences, Salford Royal NHS Foundation Trust, Manchester, United Kingdom, 17Ataxia Centre, Department of Clinical and Movement Neurosciences, UCL Queen Square Institute of Neurology, London, United Kingdom, 18Academic Department of Neurosciences, Sheffield Teaching Hospitals NHS Trust and University of Sheffield, Sheffield, United Kingdom, 19Department of Neurology, Columbia University Irving Medical Center, New York, United States, 20Initiative for Columbia Ataxia and Tremor, Columbia University Irving Medical Center, New York, United States
r.curro@ucl.ac.uk
Background: Cerebellar ataxia, neuropathy, and vestibular areflexia syndrome (CANVAS) is caused by biallelic AAGGG repeat expansions in RFC1 and is recognized as one of the most common causes of ataxia and sensory neuropathy worldwide. Retrospective studies investigated the role of the repeat expansion size and of serum Neurofilament Light Chain (NFL) as markers of disease severity. However, no reliable markers of disease progression are currently available.
Aims: We aim to establish an international cohort of CANVAS patients and to follow them up longitudinally.
Methods/Materials: At each visit, a set of clinical scales designed for ataxic disorders (Scale for Assessment and Rating of Ataxia-SARA: International Cooperative Ataxia Rating Scale–INAS) or for sensory neuropathies (Charcot-Marie-Tooth Examination Score-CMTES; Sensory Ataxia Rating Score-SEARS) will be administered. Change-sensitive items will be combined in a new composite, disease-specific grading system. 3D-T1 brain and cervical spine MRI will be performed for volumetric analyses. Serum and blood RNA tubes will be collected for quantification of axonal damage biomarkers (e.g. NFL, peripherin) and for expression studies. Video-oculography and 3D-motion capture will be carried out to gather quantitative data on vestibular function and gait. Long-read sequencing will be performed on a subset of patients to investigate the role of repeat interruptions as genetic modifiers.
Results: Currently, we have enrolled 36 CANVAS patients and collected detailed history, clinical examination, and clinical scales in all of them. Biospecimens for serum biomarkers and RNA studies are available in 28 patients. Diagnostic MRI has been carried out in 16 patients and vestibular testing in 32.
Conclusion: This natural history study aims to provide a deeper understanding of CANVAS-RFC1 disease and its progression. Integrating quantitative clinical, biological, and digital biomarkers will offer greater sensitivity and reliability in identifying biomarkers for early-stage disease, crucial for informing the design and for potential success of future clinical trials. In parallel, we will carry out a genome-wide association study to identify genetic modifiers in CANVAS-RFC1 disease, for which we have already collected 650 DNA samples thanks to an international collaboration.
73
PN02Biallelic variants in ARHGAP19 cause a progressive inherited motor-predominant neuropathy – an update
Natalia
Dominik
1#, Stephanie Efthymiou1#§, Christopher J. Record1, Xinyu Miao2,51, Renee Lin1, Jevin M. Parmar3, Annarita Scardamaglia1, Reza Maroofian1, Gabriel Aughey4, Abigail D. Wilson4, Simon Lowe4, Riccardo Curro1,5, Ricardo P. Schnekenberg1, Shahryar Alavi1, Leif Leclaire2,51, Yi He2,51, Kristina Zhelcheska1, Yohanns Bellaiche6, Isabelle Gaugué6, Mariola Skorupinska1, Liedewei Van de Vondel7,8, Sahar I. Da'as9, Valentina Turchetti1, Serdal Güngör10, Gavin Monahan3, Ehsan Ghayoor Karimiani,1,11, Yalda Jamshidi11, Phillipa J. Lamont12, Camila Armirola Ricaurte13,14, Haluk Topaloglu15, Albena Jordanova13,14,16, Mashaya Zaman17, Selina H. Banu17, Wilson Marques18, Pedro José Tomaselli19, Busra Aynekin1, Ali Cansu20, Huseyin Per21, Ayten Güleç21, Javeria Raza Alvi22, Tipu Sultan22, Arif Khan23,24, Giovanni Zifarelli25, Shahnaz Ibrahim26, Grazia M. S. Mancini27, M. Mahdi Motazacker28, Esther Brusse27, Vincenzo Lupo29, Teresa Sevilla30,31, A. Nazlı Başak32, Seyma Tekgul32, Robin J. Palvadeau32, Jonathan Baets7,8,33, Yesim Parman34, Arman Çakar34, Rita Horvath35,36, Tobias B. Haack37,38, Jan-Hendrik Stahl39,40, Kathrin Grundmann-Hauser37,38, Joohyun Park37,38, Stephan Züchner41,42, Nigel G. Laing3, Lindsay Wilson1, Alexander M. Rossor43, James Polke44, Fernanda Barbosa Figueiredo45, André Luiz Pessoa46, Fernando Kok45, Antônio Rodrigues Coimbra-Neto47, Marcondes C. França Jr47, Gianina Ravenscroft3, Sherifa Ahmed Hamed48, Wendy K. Chung49, Daniel P. Osborn50, Michael Hanna1, Andrea Cortese1,5, Mary M. Reilly1#, James E. C. Jepson4#, Nathalie Lamarche-Vane2,51#, Henry Houlden1#
Natalia Dominik n.dominik@ucl.ac.uk
1Department of Neuromuscular Disease, UCL Queen Square Institute of Neurology, London, WC1N 3BG, UK, 2Department of Anatomy and Cell Biology, McGill University, Montréal, QC H3A 0C7, Canada, 3Harry Perkins Institute of Medical Research, Centre for Medical Research, University of Western Australia, Perth, Western Australia, Australia, 4Department of Clinical and Experimental Epilepsy, UCL Queen Square Institute of Neurology, London, UK, 5Department of Brain and Behavioral Sciences, University of Pavia, 27100 Pavia, Italy, 6Institut Curie, Université PSL, Sorbonne Université, CNRS UMR3215, INSERM U934, Genetics and Developmental Biology, 75005 Paris, France, 7Translational Neurosciences, Faculty of Medicine and Health Sciences, University of Antwerp, Antwerp, Belgium, 8Laboratory of Neuromuscular Pathology, Institute Born-Bunge, University of Antwerp, Antwerp, Belgium, 9Department of Human Genetics, Sidra Medicine, Doha, Qatar, 10Inonu University, Faculty of Medicine, Turgut Ozal Research Center, Department of Pediatric Neurology, Malatya, Turkey, 11Molecular and Clinical Sciences Institute, St. George's, University of London, SW17 0RE, UK, 12Royal Perth Hospital, Perth, WA, 6000, Australia, 13Molecular Neurogenomics group, VIB Center for Molecular Neurology, VIB, Antwerp, Belgium, 14Molecular Neurogenomics group, Department of Biomedical Sciences, University of Antwerp, Antwerp, Belgium, 15Department of Pediatric Neurology, Hacettepe University, Ankara, Turkey, 16Department of Medical Chemistry and Biochemistry, Medical University-Sofia, 1431, Sofia, Bulgaria, 17Department of Pediatric Neurology, Dr M.R. Khan Shishu (Children) Hospital and ICH, Mirpur, Dhaka, Bangladesh, 18Department of Neurosciences, School of Medicine of Ribeirão Preto, University of São Paulo, São Paulo, Brazil, 19Clinical Hospital of Ribeirão Preto, Department of Neurosciences and Behaviour Sciences, University of São Paulo, Ribeirão Preto, Brazil, 20Department of Pediatric Neurology, Faculty of Medicine, Farabi Hospital, Karadeniz Technical University, Trabzon, Turkey, 21Department of Pediatric Neurology, Erciyes University, Kayseri, Turkey, 22Children's Hospital & the Institute of Child Health, Lahore, Pakistan, 23Pediatric Neurology, Neuropedia Hospital, Dubai, ARE, 24Pediatric Neurology, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai, ARE, 25CENTOGENE GmbH, Am Strande 7, 18055 Rostock, Germany, 26Department of Pediatrics and Child Health, Aga Khan University, Karachi, Pakistan, 27Department of Clinical Genetics, ErasmusMC University Medical Center, Dr.Molewaterplein 40, 3015GD Rotterdam, The Netherlands, 28Laboratory of Genome Diagnostics, Department of Human Genetics, Amsterdam UMC, University of Amsterdam, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands, 29Rare Neurodegenerative Diseases Laboratory, Centro de Investigación Príncipe Felipe (CIPF), 46012 Valencia, Spain, 30Hospital Universitari i Politècnic La Fe & IIS La Fe, Neuromuscular Diseases Unit, Department of Neurology, Valencia, Spain, 31Universitat de València, Valencia, Spain. Centro de Investigación Biomédica en Red de Enfermedades Raras (CIBERER), Spain, 32Suna and İnan Kıraç Foundation, Neurodegeneration Research Laboratory (NDAL), Research Center for Translational Medicine (KUTTAM), Koç University School of Medicine, Istanbul, Turkey, 33Neuromuscular Reference Centre, Department of Neurology, Antwerp University Hospital, Antwerp, Belgium, 34Department of Neurology, Istanbul Medical School, Istanbul University, Istanbul, Turkey, 35Department of Clinical Neurosciences, School of Clinical Medicine, University of Cambridge, Cambridge Biomedical Campus, Cambridge, UK, 36Department of Clinical Neurosciences, John Van Geest Centre for Brain Repair, School of Clinical Medicine, University of Cambridge, Cambridge, UK, 37Center for Rare Disease, University of Tübingen, Tübingen, Germany, 38Institute of Medical Genetics and Applied Genomics, University of Tübingen, Tübingen, Germany, 39Department of Epileptology, Center of Neurology, University of Tübingen, Germany, 40Hertie Institute for Clinical Brain Research, University of Tübingen, Tübingen, Germany, 41John P. Hussman Institute for Human Genomics, University of Miami, Miami, FL, USA, 42Dr. John T. Macdonald Foundation Department of Human Genetics, University of Miami, Miami, FL, USA, 43Centre for Neuromuscular Diseases, Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, UK, 44Neurogenetics Laboratory, The National Hospital for Neurology and Neurosurgery and the North Thames Genomics Laboratory Hub, London, UK, 45Mendelics Genomic Analysis, São Paulo, SP, Brazil, 46Universidade Federal Do Ceara - UFC and Hospital Infantil Albert Sabin, Fortaleza, Brazil, 47Department of Neurology, School of Medical Sciences, University of Campinas (UNICAMP), Campinas, SP, Brazil, 48Department of Neurology and Psychiatry, Faculty of Medicine, Assiut University, Assiut, Egypt, 49Department of Pediatrics, Boston Children's Hospital, Harvard Medical School, Boston, MA, USA, 50Genetics Sections, Molecular and Clinical Sciences Institute, St George's University of London, Cranmer Terrace, London, SW17 0RE, UK, 51Cancer Research Program, Research Institute of the McGill University Health Centre, Montréal, QC H4A 3J1, Canada.
#Contributed equally
Introduction: Charcot-Marie-Tooth Disease is a clinically and genetically heterogeneous group of hereditary neuropathies. Despite progress in genetic sequencing, around a quarter of patients remain unsolved.
Aims: To describe ARHGAP19-neuropathy and identify potential therapeutic targets.
Methods: By using next-generation-sequencing, we identified 16 recessive variants in the RhoGTPase activating protein 19 gene (ARHGAP19) causing motor-predominant neuropathy in 25 individuals from 20 unrelated families. The ARHGAP19 protein acts as a negative regulator of the RhoA GTPase and we used various approaches to model these variants; in-vitro GTPase-activating-protein (GAP) assays to assess if the GAP activity is affected by overexpression of proteins carrying ARHGAP19, complemented by an in-vivo Drosophila melanogaster model to test for movement, lifespan and neuromuscular junction integrity, an in-vivo Danio rerio model to test for locomotion and morphological changes; in silico approach to gain an understanding of protein structure changes and its implications.
Results: In-vitro biochemical and cellular assays revealed that patient variants impair the GTPase-activating protein (GAP) activity of ARHGAP19 and reduce ARHGAP19 protein levels. Parallel in-vivo studies in Drosophila and zebrafish models demonstrate a conserved role for ARHGAP19 orthologs in regulating locomotor capacity, the length and branching of motoneuron axons in zebrafish. Transcriptomics provided evidence that pathways associated with motor proteins and cell cycle are impacted.
Conclusions: Taken together, our findings establish ARHGAP19 variants as a cause of inherited neuropathy acting through a loss-of-function mechanism. ARHGAP19 is a GAP with activity towards RhoA, and the downstream effectors are exciting potential new targets for therapy. Efforts are ongoing to identify potential small molecule drugs by use of high-throughput Drosophila melanogaster drug screen to modify the disease progression.
PN03An Evaluation of Participant Acceptability of the CMT Functional Outcome Measure (CMT-FOM)
Magdalena M Dudziec1, Mariola Skorupinska1 Gita Ramdharry1, Luke O’Donnell1, Matilde Laurá1, Michael E Shy3, David N Herrmann2, Mary M Reilly1
1Centre for Neuromuscular Diseases, Dept of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London UK, 2Department of Neurology, University of Rochester, Rochester, NY, United States, 3Department of Neurology and Center for Molecular Medicine and Genetics, University of Iowa, USA.
m.dudziec@ucl.ac.uk
Background: Functional impairments of both upper and lower limbs are experienced by people with Charcot-Marie-Tooth Disease (CMT). The 13-item, performance-based CMT-FOM is used by trained clinicians in natural history research to assess function. Despite the measure being increasingly commonly used, little is known about participant acceptability and completion rates of each item within it.
Aims: To evaluate participant acceptance and item completion of the CMT-FOM in a cohort of participants enrolled in the Inherited Neuropathy Consortium 4 Gene and Accelerate Clinical Trials in Charcot-Marie-Tooth Disease (ACT-CMT) studies.
Methods: The 13 items of the CMT-FOM were analysed. Descriptive analysis was used to illustrate the percentages of completion of each item.
Results: Baseline data from 91 participants was analysed (female n=42 (46%); mean age: 45 years, range: 18–73). Disease types were: CMT1A (n=51, 57.1%) CMT1B (n=13, 14.3%), CMT2A (n=10,11 %), CMT1X (n=10, 11%) and CMT2F (n=6, 6.6%). All participants completed the Foot Posture Index. The Timed Up and Go, Stair climb,10m Walk and 6 Minute Walk Tests were completed by all but one participant. Several participants were too weak to elicit results in strength measures. Within these, handgrip was completed by 88/91 (96.7%), plantar flexion by 77/91 (84.6%) and dorsiflexion by 64/91 (70.3%). 78/91 (85.7%) completed the 30 second chair stand. Balance ability was measured in three conditions. 83/91 (91.2%) completed eyes open, 76/91 (83.5%) eyes closed and 66 /91 (72.5%) single leg stance with eyes closed. In upper limb dexterity measures, 88/91 people (96.7%) completed the Functional Dexterity Test with 90/91 (98.9%) completing the 9-Hole Peg Test. In all cases, disease symptoms prohibiting function prevented completion.
Conclusions: The CMT-FOM was acceptable to participants at baseline measurements. The inability to complete measures was reflective of the functional limitations caused by CMT. Baseline data will be analysed alongside follow-up visits to observe changes over time and with greater measure familiarity.
PN04Histopathological findings from muscle and nerve biopsies in patients with Strachan’s syndrome
Caroline Kramarz1
, Thomas O Millner2, Ashirwad Merve2, Stephanie Carrington1, William L Macken1,3, Matteo Zanovello1,4, Cathy E Woodward5, Heba Morsy1, Aisling Carr1, David Gosal6, Tim Lavin6, Robert DM Hadden7, Robert DS Pitceathly1,3, Mary M Reilly1, Alexander M Rossor1
1Department of Neuromuscular Diseases, Queen Square UCL Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, UK, 2Division of Neuropathology, The National Hospital for Neurology and Neurosurgery, London, UK, 3NHS Highly Specialised Service for Rare Mitochondrial Disorders, Queen Square Centre for Neuromuscular Diseases, The National Hospital for Neurology and Neurosurgery, London, 4UCL Queen Square Motor Neuron Disease Centre, Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, 5Neurogenetics Unit, Rare and Inherited Disease Laboratory, North Thames Genomic 6Laboratory Hub, London WC1N 3BH, UK, 7Salford Royal Hospital, Northern Care Alliance NHS Foundation Trust, Manchester
Department of Neurology, King's College Hospital, London, UK.
c.kramarz@ucl.ac.uk
Background: Strachan's syndrome is characterised by a triad of optic, auditory and painful sensory peripheral neuropathies. The cause of the syndrome is attributed to nutritional deficiencies and typically presents acutely or sub-acutely following systemic illness, weight loss, or dietary restriction such as veganism. The syndrome is more prevalent among Black British individuals, often of Jamaican descent, and an underlying genetic predisposition has been suggested. Despite its recognition since the late 19th century, there remains limited awareness of its pathophysiology and clinical features.
Aims: This study aimed to collect and analyse the histopathological findings in cases of Strachan’s syndrome in UK patients to better characterise its clinical and pathological features.
Methods: We identified 30 UK patients diagnosed with Strachan’s syndrome through a specialist peripheral nerve service and compiled detailed clinical histories. Nerve and muscle biopsies were performed on several patients to investigate underlying pathological changes. Findings from these biopsies were analysed alongside clinical data to identify common patterns or abnormalities.
Results: Six patients underwent quadriceps muscle biopsy which showed ragged red fibres, reduced COX (cytochrome c oxidase) activity and excess lipid content. Six patients underwent sural nerve biopsy during the acute phase of disease which showed active axonal degeneration with loss of large and small myelinated fibres. In three cases, there was widespread perivascular, inflammatory cell infiltrate in the epineurium, suggesting vasculitis and led to some patients receiving immunosuppressive treatment.
Conclusion: Similar histological findings have been identified in nerve biopsies performed in other endemic neuropathies, notably the Cuban epidemic of optic and peripheral neuropathy in 1990. It is unclear why there are signs of inflammation seen on nerve biopsy. This may be due to a secondary immune response from ischaemia or oxidative stress induced by nutritional deficiencies.
The muscle biopsy findings provide direct evidence of mitochondrial failure as the final common pathway in Strachan’s syndrome.
‡PN05Transcriptional insights into a highly prevalent equine motor axonopathy
Victoria O’Hara1
, Abdulaziz Almuhanna1, Sarah Salisbury3, Justin Perkins2, Stephen D Cahalan1, Androniki Psifidi2,3, Diego Robledo3, Richard J Piercy1
1 Comparative Neuromuscular Disease Laboratory, Royal Veterinary College, London, UK, 2 Clinical Services and Sciences, Royal Veterinary College, London, UK, 3 Roslin Institute, The University of Edinburgh, UK
vohara4@rvc.ac.uk
Background: The left equine recurrent laryngeal nerve (RLn), spanning ∼250 cm, offers a valuable model for studying human length-dependent axonopathies due to its susceptibility to recurrent laryngeal neuropathy (RLN), a common distal axonopathy. The length of the equine RLn offers a more relevant model for human disease compared to the relatively much shorter axons in rodent models. Despite this potential, the molecular mechanisms underlying RLN remain poorly understood. Since the cell bodies of the RLn reside in the nucleus ambiguus (nAmb), we hypothesized that single-nucleus RNA sequencing of this region could reveal transcriptional alterations linked to RLN.
Aims: To identify disease-associated transcriptional changes in the nAmb neuronal cell bodies and elucidate mechanisms underlying RLN as a distal axonopathy.
Methods/Materials: Bilateral RLns from 5 Warmblood geldings were histologically assessed for disease severity by examining left to right axon count ratios. The brainstems from these animals were snap frozen, and the left and right nAmb regions were resected. nAmb nuclei were isolated and sequenced with the 10x Genomics Chromium platform, generating 191,398 high-quality nuclei. Cell populations were identified using marker genes from other species. Differential expression was analysed with EdgeR and Gene Ontology (GO) enrichment was performed using DAVID.
Results: Seventeen distinct cell clusters were identified, including two neuron populations. Cell type proportions remained consistent across mild and severe cases, indicating that disease does not stem from alterations in population. One neuronal cluster displayed stress-related signals in all samples. Differential expression analysis between mild and severely-affected horses revealed pathways linked to cellular stress in glial cells, with GO enrichment showing stress responses and regulation of cell death (FDR = <0.001 and 0.007 respectively). Response to xenobiotic stimulus (FDR<0.001) was upregulated in the stressed neuron population when comparing left to right nAmb. Further focus on receptor-ligand interactions and validation via RNAScope in-situ hybridisation is ongoing.
Conclusion: This study identifies stress-related transcriptional signatures in RLN, implicating glial disruptions in axonal degeneration. These findings support RLN as a model for studying human length-dependent neuropathies.
PN06Using Social Media to Engage with People Living with CANVAS, to Guide Rehabilitation Research
Ramdharry, G.M.
1,2, Male, A.3,4, Koohi, N.3,4, Curro R.2, Kaski, D.3,4, Cortese, A.1,2,Reilly, M.M.1,2
1Queen Square Centre for Neuromuscular Diseases, National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, UK, 2Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London WC1N 3BG, UK, 3Department of Clinical & Movement Neurosciences, University College London Queen Square Institute of Neurology, London WC1N 3BG, UK, 4The Ear Institute, University College London, London WC1X 8EE, UK
g.ramdharry@ucl.ac.uk
Background: Patient and Public Involvement (PPI) is a requirement of many research funders to ensure "research being carried out 'with' or 'by' members of the public rather than 'to', 'about' or 'for' them". Engagement helps to understand issues and identify research topics.
Aims: Here we present the method and results of a focused PPI activity that will be used to inform a research program for people with Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS). This was a first step to consult people with CANVAS on strategies they use to address the problem of poor balance and falls.
Methods/Materials: There is no specific UK charity for CANVAS, but there is a dedicated Facebook page: RFC-1 CANVAS International Support Group. The group administrators gave permission for three questions to be posted on their Facebook page:
1) What have you found improves your balance?
2) What do you do, or use, to prevent falls?
3) Have you received physiotherapy or physical therapy for your condition, and did it help?
Free text responses were tabulated and coded using thematic analysis.
Results: Seventy of 568 members responded (12%).
Question 1) Sixty-nine responses were grouped into three main themes. ENVIRONMENTAL STRATEGIES: extra lighting (19%), walking aids (9%). REHABILITATION-BASED STRATEGIES: balance/vestibular training (17%), strengthening exercise (16%), aerobic training (7%). BEHAVIORAL STRATEGIES: light-touch balance (7%), avoiding fatigue and stress (7%), using visual reference-points (3%), keeping head still (3%).
Question 2) There were 47 responses under two themes. ENVIRONMENTAL STRATEGIES: walking aids (28%), changes to home (19%). BEHAVIORAL STRATEGIES: holding objects/others (25%), avoiding perturbations (6%), using visual reference-points (6%).
Question 3) Twenty-seven people responded, with 70% having received physiotherapy, and 63% finding it helpful.
Conclusions: This information will guide development of falls management and rehabilitation programs for people with CANVAS. More in-depth, in-person engagement is required with people with a definite RFC-1 confirmed diagnosis.
‡PN07Proposing a Model of Falls and Balance Performance for People with Inherited Peripheral Neuropathy
Ramdharry, G.M.
1,2, Dudziec, M.2, Tropman, D.3, Reilly, M.M.1,2
1Queen Square Centre for Neuromuscular Diseases, National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, UK, 2Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, UK, 3Clinical Engineering, Royal Free Hospital, London, UK
g.ramdharry@ucl.ac.uk
Background: Inherited peripheral neuropathies (IPN) are a heterogeneous group of conditions that includes mixed motor-sensory neuropathies, distal motor neuronopathies and sensory neuropathies. Falls events in IPN cohorts, are reported between 50% - 86%, impacting balance confidence.
Aims: In this study, we explore relationships between falls, postural stability and presenting sensory-motor impairments to describe a preliminary model of falls and balance performance. This model can then guide targeted rehabilitation interventions.
Methods/Materials: This was a cross-sectional study of people with IPN. Quantitative measures were obtained of lower-limb muscle strength (dynamometry) and sensory impairment (monofilaments, biosthesiometer). Static balance was assessed using gold-standard static posturography (center of pressure (COP) velocity). Forward and lateral reach tests were used to measure dynamic balance. A Romberg's Quotient was calculated to ascertain visual dependency. Falls events were recorded prospectively over six-months with weekly postcards. Balance confidence was assessed using the Falls Efficacy Scale. Regression analysis was used to explore the relationships between impairments and balance, balance and falls, and falls and balance confidence.
Results: Thirty-two people with a range of genetic sub-types and motor-sensory presentation of IPN were recruited. A mean of 8.84 falls were recorded over 6-months. A three-level model is presented
(1) Static stability measures (COP velocity) were significantly related to ankle-dorsiflexor strength (β=-0.35, 0.009) and Romberg's Quotient (β=0.51, P=0.014). Forward-reach distance was significantly related to knee-extensor strength (β=0.73, P=0.009), and lateral-reach related to ankle-evertor strength (β=0.73, 0.009).
(2) Highly significant relationships were found between falls events and COP velocity (eyes-open, feet-together β=5.51. P=0.009; eyes-closed, feet-apart β=3.72, P=0.009) and forward-reach distance (β=-0.012, P<0.000).
(3) Falls frequency related to reduced balance confidence (β =0.02, P=0.013).
Conclusions: Targeting lower limb strength and visual dependency with rehabilitation interventions, such as exercise and orthotics, could improve static and dynamic balance, so reducing falls frequency and increasing balance confidence for people with IPN.
PN08Functional Investigation of RFC1 Expansions using iPSC-Derived Inducible Sensory Neurons
Ricardo Schnekenberg1,
Riccardo Currò1, Arianna Ghia1, Yichen Qiu1, Gabrielle Lignani1, Henry Houlden1,2, James Jepson1, Mary Reilly 1,2, Andrea Cortese1,2
1UCL Institute of Neurology, London,
2
Queen Square Centre for Neuromuscular Diseases, London
r.schnekenberg@ucl.ac.uk
Background: CANVAS is a recessively inherited condition caused biallelic intronic repeat expansions in RFC1. Through in vitro, cellular and Drosophila models we previously showed that RFC1 intronic expansions appear to lead to loss of RFC1 function. However, the exact molecular mechanisms linking the presence of the pathogenic repeat expansion to reduced RFC1 function remain elusive. Possible reasons of this limitation encompass the cell-specific variability of RFC1 expression as well as the selective vulnerability of sensory neurons compared to other cell types.
Aims: Here we aimed to develop a highly robust inducible sensory neuron platform that can be used for investigating disease models in sensory neuronopathies such as CANVAS. We then benchmarked it on CANVAS IPSC lines along with heterozygous and homozygous corrected isogenic cell lines where the pathogenic repeat was selectively excised.
Methods/Materials: Expanded RFC1 alleles were deleted via CRISPR/Cas9-editing in two patient-derived iPSC lines to achieve isogenic control lines with monoallelic or biallelic corrections. Patient lines, isogenic lines and control lines were differentiated to sensory neurons through PiggyBac-mediated integration of a cassette that forces expression of neuronal transcription factors Ngn2 and Brn3a in response to doxycycline. Phenotypes were assessed using RNAseq, immunofluorescence, protein studies and multi-electrode arrays.
Results: Induced neuronal cells were successfully differentiated up to 3 months, with neuronal morphology similar between disease and isogenic control lines. Sensory neuronal identity was confirmed by Tuj1+, MAP2+ and BRN3a+ staining. Principal component analysis (PCA) of transcriptomic data along 6 timepoints shows progressive maturation along both PC1 and PC2 axes. Multielectrode array data show electrical activity starting 14 days after induction.
Conclusion: We report an iPSC-based platform that can generate induced neurons that are transcriptionally and neurophysiologically compatible with sensory neurons which can be used for mechanistic research and drug testing in RFC1/CANVAS and other types of sensory neuropathies.
PN09Foot Ulceration in Patients with Charcot-Marie-Tooth Disease: Assessing Access to Podiatry Services
Mariola Skorupinska1
, Gita Ramdharry1, Alexander M. Rossor1, Matilde Laurá1, Mary M. Reilly1
1Centre for Neuromuscular Diseases, Dept of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London UK,
mariola.skorupinska@nhs.net
Background: Patients with Charcot-Marie-Tooth (CMT) disease and related disorders are at increased risk of developing foot ulcers, leading to considerable health challenges. Timely and effective podiatry care is essential for preventing and managing these complications. However, limited information exists regarding patient satisfaction and their perspectives on the accessibility and efficacy of podiatry services.
Aims: To assess patient satisfaction and perceptions of podiatry services, focusing on accessibility, effectiveness, and their role in preventing and treating foot ulcers in the United Kingdom (UK).
Methods: An audit was conducted using a questionnaire completed by CMT patients attending our genetic neuropathy clinics.
Results: A total of 92 patients with CMT and related disorders participated (56% female; mean age: 48 years, range: 18–79). Of these, 9% (8/93) had active ulcers at the time of the study. Most participants, 79 (86%) were diagnosed with CMT, with the majority (46/79) having CMT1A caused by PMP22 duplication. Another 10 patients (11%) had hereditary sensory neuropathy (HSN), with 60% (6/10) having HSN1 due to SPTLC1/SPTLC2 variants. Of the respondents, 60% (56/93) had been advised to attend podiatry services, but only 35% (33/93) were able to access services. The main factors affecting access to podiatry care were lack of primary healthcare provider referrals (42%) and lack of appointment availability (37%), while other barriers included long waiting times (18%) and limited local services (17%). A small number (7 patients) attended private podiatry services. Among those who accessed podiatry services, 78% (47/60) reported improvements in foot health and overall well-being.
Conclusion: This study highlights significant gaps in podiatry service delivery for patients with CMT and related conditions. It emphasises the need for enhanced access to podiatry care and better patient education on the benefits of these services for preventing and managing foot ulcers. These findings offer valuable direction for improving podiatry service provision.
Other Diseases
OD01PIGG variants cause a neurodevelopmental disorder with secondary cerebral folate deficiency
Dania B. Hammadi1
, Robert McFarland1,2, Robert W.Taylor1,2 and Charlotte L. Alston1,2
1Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, 2NHS Highly Specialised Services for Rare Mitochondrial Disorders, Royal Victoria Infirmary, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne
d.b.h.hammadi2@ncl.ac.uk
Background: Paediatric neurometabolic disorders are genetically and phenotypically heterogeneous, complicating diagnosis. Inherited glycosylphosphatidylinositol (GPI) deficiencies result from variants in any of the 22 genes involved GPI anchor biosynthesis, including PIGG, which encodes an ethanolamine phosphate transferase. PIGG adds an ETNP molecule to the second mannose of the GPI backbone, essential for specific protein expression. Bi-allelic PIGG variants are known to cause a paediatric neurodevelopmental disorder characterised by seizures, delayed development and cerebral atrophy. A measurable decrease in cell surface expression of GPI-anchored proteins in patient fibroblasts is reported to be a useful diagnostic marker to support pathogenicity of novel PIGG variants. We describe a female patient who presented at 12 months of age with cerebral folate deficiency (CFD), seizures, developmental delay, and myopathy. At 15 years, folinic acid supplementation has reportedly improved her symptoms, though no genetic diagnosis was established.
Aims: To identify the genetic basis of the patient's phenotype and explore its relationship to the folinic acid treatment.
Methods/Materials: Trio whole exome sequencing (WES) of blood DNA from the patient and her parents was undertaken, followed by variant prioritisation based on inheritance pattern, variant allele frequency, predicted variant impact, and known disease associations. Immunofluorescent microscopy was used to investigate the expression of folate receptor 1 (FOLR1) in patient fibroblasts.
Results: Compound heterozygous loss-of-function PIGG variants were identified: c.1332+1G>T and c.2624_2625del, p.Leu875* (NM_001127178.3), in addition to a homozygous missense variant, c.434C>T, p.(Thr145Met) in FOLR2 (NM_000803.5). No variants were identified involving FOLR1, the main cause of CFD. FOLR1 and FOLR2 encode GPI-anchored folate receptors that mediate 5-methyltetrahydrofolate (5-MTHF) transport. FOLR1 is predominantly expressed in epithelial cells, particularly in the choroid plexus, the primary site of 5-MTHF transport into the brain, whereas FOLR2 is more highly expressed in myelopoietic cells and during early development, including in the placenta. Immunofluorescence imaging of patient fibroblasts revealed decreased expression of FOLR1 compared to control fibroblasts, consistent with defective attachment of the receptor to the GPI-anchor.
Conclusion: To our knowledge, this is the first report of PIGG dysfunction causing decreased expression of FOLR1, leading to CFD, and provides support for therapeutic folinic acid in similar patients.
OD02A Novel Cause of Rhabdomyolysis: Two Cases of Syndromic Ciliopathy Caused by a Homozygous Variant in the POC5 Gene
E Erdil
1,2, S Lin3,4, J Spillane1,2, R Howard1,2, Y Patel2,5, R Kabiljo1,2, R Labrum2,5, R Quinlivan1, M G Hanna1,2, W L Macken1,2,6, R D S Pitceathly1,2
1Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London, UK, 2The National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Foundation Trust, London, UK, 3Manchester Centre for Genomic Medicine, Saint Mary’s Hospital, Manchester University NHS Foundation Trust, Manchester, UK, 4UCL Institute of Ophthalmology, University College London, London, UK, 5Rare and Inherited Disease Laboratory, North Thames Genomic Laboratory Hub, Great Ormond Street Hospital for Children NHS Foundation Trust, London, UK, 6North East Thames Clinical Genetics, Great Ormond Street Hospital for Children NHS Foundation Trust, London, UK
esra.erdil@nhs.net
Background: To date a number of genetic causes of rhabdomyolysis have been described. These include metabolic myopathies, mitochondrial myopathies, calcium related disorders (RYR1) and muscular dystrophies. However, the true burden of mongenic rhabdomyolysis is likely to be underestimated and other causes are likely.
Aims: To describe two syndromic cases of rhabdomyolysis in which a novel genetic cause was identified.
Methods/Materials: Following the tentative identification of POC5 as a morbid gene we undertook reanalysis of NGS data and identified two cases with homozygous variants and rhabdomyolysis. We conducted a case review for each with a focus on the neuromuscular element of the phenotype.
Results: Patient 1 is a female with suspected acquired myotonia, presenting with severe cramps, muscle rippling, and rhabdomyolysis episodes in her 30s. EMG showed nerve hyperexcitability, myokymia, and neuromyotonic discharges. Rapidly firing neurogenic units have been found during cramps. Nerve excitability studies were consistent with depolarisation. Extensive antibody testing was negative. Two muscle biopsies were performed: the first showed non-specific vacuoles, and the second revealed Type 2 fibre atrophy no evidence of an inflammatory myopathy. Creatine kinase levels ranged from 400s to 1200 U/L. She also has Polycystic Ovary Syndrome, hypothyroidism, hyperlipidaemia, mild concentric hypertrophy, large hands, thin scalp hair, and brittle nails. Patient 2 developed exercise-induced cramps from age 13, with one episode of suspected rhabdomyolysis and CK> 10,000 U/L. Cramps are triggered by activity and cold weather, but not by fever, infection, or fasting. Lower limb MRI showed no sign of myopathy. A muscle biopsy revealed fast fibre atrophy, uneven oxidative staining, occasional well defined core lesions, aligning with rhabdomyolysis and limited physical activity. Cardiac evaluation showed borderline concentric hypertrophy. She developed retinal dystrophy in adulthood and died suddenly at 32 due to acute pancreatitis and multiorgan failure, with high triglycerides.
Conclusions: Recessive variants in POC5 are associated with a rhabdomyolysis, endocrinopathy/metabolic syndrome and retinal dystrophy.
OD03ATG12 variants impair autophagy and cause a neurodevelopmental disorder
James Lambton1
, Charlotte L. Alston1,2, Fumi Suomi3,4, Magali Prigent5,6, Aliza Imam7, Thomas J. McCorvie8, Daniel Warren9, Emma Hobson7, Helen McCullagh10, Doriana Misceo11, Anna Bjerre12, Marie F. Smeland13,14, Claus Klingenberg14,15, Eirik Frengen11, Swati Naik16, Gavin Ryan16, Annapurna Sudarsanam17, Katie Foster18, Pradeep Vasudevan19, Rajib Samanta20, Robert McFarland1,2, Jack J. Collier21, Wyatt W. Yue8, Renaud Legouis5,6, Thomas G. McWilliams3,4, Monika Oláhová1,22 and Robert W. Taylor1,2
1 Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK, 2 NHS Highly Specialised Rare Mitochondrial Disorders Service, Newcastle upon Tyne Hospitals NHS Foundation Trust, NE1 4LP, Newcastle upon Tyne, UK, 3 Translational Stem Cell Biology & Metabolism Program, Research Programs Unit, University of Helsinki, 00290, Helsinki, Finland, 4 Department of Anatomy, Faculty of Medicine, University of Helsinki, 00290, Helsinki, Finland, 5 Institute for Integrative Biology of the Cell (I2BC), Université Paris-Saclay, CEA, CNRS, 91190, Gif-sur-Yvette, France, 6 INSERM U1280, 91198, Gif-sur-Yvette, France, 7 Yorkshire Regional Genetics Service, Chapel Allerton Hospital, Leeds Teaching Hospitals NHS Trust, LS7 4SA, Leeds, UK, 8 Biosciences Institute, Faculty of Medical Sciences, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK, 9Department of Radiology, Leeds Teaching Hospitals NHS Trust, Leeds, LS1 3EX, UK, 10 Department of Paediatric Neurology, Leeds Teaching Hospitals NHS Trust, LS1 3EX, Leeds, UK, 11Department of Medical Genetics, Oslo University Hospital and University of Oslo, 0450, Oslo, Norway, 12 Department for Specialised Paediatrics, Oslo University Hospital, 0450, Oslo, Norway, 13 Department of Paediatric Rehabilitation, University Hospital of North Norway, 9019, Tromsø, Norway, 14 Department of Clinical Medicine, Faculty of Health Sciences, UiT-The Arctic University of Norway, Tromsø, Norway, 15 Department of Paediatrics and Adolescence Medicine, University Hospital of North Norway, Tromsø, Norway, 16West Midlands Clinical Genetics Unit, Birmingham Women’s and Children’s Hospital, B15 2TG, Birmingham, UK, 17Department of Neurology, Birmingham Women’s and Children’s Hospital, B15 2TG, Birmingham, UK, 18Department of Radiology, Birmingham Children’s Hospital, B4 6NH, Birmingham, UK, 19Department of Clinical Genetics, University Hospitals Leicester NHS Trust, Leicester Royal Infirmary, LE1 5WW, Leicester, UK, 20Department of Paediatric Neurology, University Hospitals Leicester NHS Trust, Leicester Royal Infirmary, LE1 5WW, Leicester, UK, 21Department of Clinical Neuroscience, University of Cambridge, Cambridge Biomedical Campus, CB2 0QQ, Cambridge, UK, 22Department of Applied Sciences, Faculty of Health and Life Sciences, Northumbria University, NE1 8SG, Newcastle-upon-Tyne, UK
j.lambton@newcastle.ac.uk
Background: Autophagy is an essential developmental and homeostatic process, defined by the endolysosomal degradation of intracellular components and pathogens. Dysfunctional autophagy is implicated in complex human disease yet reports of congenital autophagy disorders were considered exceedingly rare until a recent report of several unrelated families with bi-allelic variants in ATG7, complementing the report of two individuals harbouring ATG5 variants, both of which encode core autophagy effectors. Congenital disorders of autophagy present with delayed development, cerebellar malformation, ataxia and hypotonia. ATG12 is another key effector of autophagy.
Aims: To expand our understanding of congenital disorders of autophagy and their associated neurological phenotypes.
Methods/Materials: Whole genome and whole exome sequencing was used to identify patient harbouring ATG12 variants. AlphaFold Multimer was used to model potential structural changes to ATG12. Western blotting determined steady state protein levels patient derived primary fibroblasts. Autophagy function was assessed using autophagy flux immunoblot analysis, cargo sequestration assays and transmission electron microscopy. a yeast model of the identified ATG12 variants was generated and used to characterise the effects of these variants in-vivo via immunoblot and immunofluorescence.
Results: We report five affected individuals from four families harbouring bi-allelic ATG12 variants with complex neurological phenotypes overlapping those of ATG5 and ATG7 patients, including congenital ataxia, hypotonia, developmental delay and seizures with cerebellar vermis hypoplasia evident on neuroradiological imaging. Three of the four unrelated families harbour the same p.Tyr120Ser ATG12 variant (Refseq; NM_004707.4). Structural modelling implicated a potential disruption of the important ATG12-ATG5-ATG16N-ATG3 complex. Biochemical analyses of patient-derived primary fibroblasts from members of two affected families confirmed the loss of stable ATG5-ATG12 dimer and altered autophagic flux, supported by ultrastructural studies showing abnormal accumulation of autophagic structures. Yeast complementation studies demonstrated that equivalent missense ATG12 variants were unable to fully recover autophagy in Atg12 null yeast.
Conclusion: Our findings underscore the pivotal role of efficient autophagy for human neural integrity and emphasise the importance of this emerging group of congenital autophagy disorders with associated neurological phenotypes, thus expanding the understanding of adaptive homeostasis in human health and disease.
OD04Investigating the mechanisms underlying ATG7-related neurological disease
James Lambton1
, Jack J. Collier2, Fumi Suomi3,4, Agata Rozanska5, Thomas G. McWilliams3,4, Majlinda Lako5, Monika Oláhová1,6 and Robert W. Taylor1,7
1 Mitochondrial Research Group, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK, 2 Department of Clinical Neuroscience, University of Cambridge, Cambridge Biomedical Campus, CB2 0QQ, Cambridge, UK, 3 Translational Stem Cell Biology & Metabolism Program, Research Programs Unit, University of Helsinki, 00290, Helsinki, Finland, 4 Department of Anatomy, Faculty of Medicine, University of Helsinki, 00290, Helsinki, Finland, 5 Biosciences Institute, Faculty of Medical Sciences, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK, 6 Department of Applied Sciences, Faculty of Health and Life Sciences, Northumbria University, NE1 8SG, Newcastle-upon-Tyne, UK, 7 NHS Highly Specialised Rare Mitochondrial Disorders Service, Newcastle upon Tyne Hospitals NHS Foundation Trust, NE1 4LP, Newcastle upon Tyne, UK
j.lambton@newcastle.ac.uk
Background: The key catabolic process of autophagy relies on several core autophagy (ATG) genes, very few of which have been directly associated with disease. We recently described a cohort of twelve patients from five unrelated families with damaging bi-allelic ATG7 variants effecting the core ATG5-ATG12 and LC3 conjugation systems (PMID: 34161705). All ATG7 patients presented with developmental delay, atrophy of the corpus callosum, cerebellar hypoplasia and ataxia. Patient-derived fibroblasts showed undetectable or markedly decreased ATG7 protein levels, with complete loss or severe depletion of autophagic flux.
Aims: To investigate the effect of loss of ATG7 on neural differentiation, development and function.
Methods/Materials: Induced pluripotent stem cell (iPSC) ATG7 knockout models were generated using CRISPR/Cas9 gene editing and differentiated into neuron-astrocyte co-cultures. Immunoblot analysis of autophagy related proteins was performed alongside morphological analysis of co-cultures. Immunofluorescence analysis of neuron and astrocyte markers, autophagy adapter protein p62, and cleaved caspase-3 was undertaken. Functional characterisation of co-cultures was performed by calcium imaging using Fluo-4.
Results: The ATG7-/- neural model recapitulates the biochemical phenotypes of ATG7 null patients, showing increased p62 accumulation and complete loss of autophagy flux, while ATG7+/- co-cultures had reduced autophagy flux, with no p62 accumulation. ATG7-/- and ATG7+/- co-cultures showed decreased neurite branching and loss of neuronal cell body cluster area, indicating decreased neuronal network complexity and neuronal cell death compared to wild-type. Immunofluorescence analysis demonstrated increased astrocyte differentiation in the ATG7+/- co-cultures, while ATG7-/- cultures had increased cleaved caspase-3 positive astrocytes. Interestingly, minimal p62 positive neurons were observed. Functional calcium imaging demonstrated that both ATG7-/- and ATG7+/- neurons were able to respond to a glutamate stimulus, however, they showed impaired recovery compared to the wild-type.
Conclusion: Loss of ATG7 results in severe autophagy impairment but does not prevent differentiation of iPSCs into neurons and astrocytes. In the absence of autophagy, both neurons and astrocytes can survive, with neurons potentially undergoing selection throughout differentiation, for neurons able to clear autophagy substrates in the absence of canonical autophagy. In contrast, after differentiation astrocytes appear more susceptible to cell death than neurons, potentially modulating calcium handling in ATG7-/- and ATG7+/- neurons.
OD05Cellular Trafficking Disorders Presenting with Neuromuscular Phenotype
Dr Rajesh Madhu
Alder Hey Hospital
rajesh.madhu@alderhey.nhs.uk
Background: Cellular trafficking disorders are a group of genetic diseases that are being recognised more frequently with the increasing use of genomic sequencing tests. This group of disorders are characterized by defects in protein and lipid transport within cells. While traditionally associated with systemic and metabolic abnormalities, emerging evidence suggests that these disorders can also present with prominent neuromuscular features.
Aims: This retrospective audit aimed to investigate the characteristics of cellular trafficking disorders presenting with a neuromuscular phenotype, and to explore the underlying pathomechanisms.
Methods/Materials: We conducted a retrospective analysis of patients with genetically confirmed cellular trafficking disorders, who presented with neuromuscular symptoms such as muscle weakness, atrophy, and neuropathy. Clinical evaluation, genetic testing, and muscle biopsies were performed to characterize the disorders.
Results: Our results showed that cellular trafficking disorders can present with a wide range of neuromuscular manifestations, often mimicking traditional neuromuscular diseases. We identified more than 30 children presenting with various neuromuscular phenotypes highlighting the importance of further knowledge needed in these rare disorders among clinical teams
Conclusion: This study expands our understanding of cellular trafficking disorders and highlights their potential to present with neuromuscular phenotypes. Our findings have significant implications for diagnosis, treatment, and management of these disorders, and underscore the need for a multidisciplinary approach to patient care.
OD06A case of Multiple acyl-coenzyme A dehydrogenase deficiency (MADD) induced by Sertraline
Marion Masingue
1, Isabelle Ackermann-Bonan2, Amélie de Colnet3, Clément Pontoizeau3, Stéphanie Gobin4, Yves Fromes2, Teresinha Evangelista5
1Reference Center for Neuromuscular Diseases North/East/Île-de-France, Institute of Myology, Pitié-Salpêtrière Hospital, Paris, France, 2Nuclear Magnetic Resonance Laboratory, Neuromuscular Investigation Center, Institute of Myology, Pitié-Salpêtrière Hospital, Paris, France, 3Department of Biochemistry, Unit of Metabolic Biochemistry, Necker-Enfants Malades Hospital, Paris, France, 4Department of Molecular Genetics, Necker-Enfants Malades Hospital, Paris, France, 5Department of Neuropathology, Functional Unit of Neuromuscular pathology and Department of Neuromyology, Institute of Myology, EURO-NMD coordination, Pitié-Salpêtrière Hospital, APHP Sorbonne University, Paris, France.
Marion.masingue@aphp.fr
Background: Multiple acyl-coenzyme A dehydrogenase deficiency (MADD) is a rare inherited disorder of fatty acid beta-oxidation.. Recently, studies have implicated sertraline in MADD-like presentations [1,2].
Aims: We report the case of a 42-year-old patient presenting with exercise intolerance and biochemical MADD-like profile under sertraline treatment.
Methods/Materials: The patient was addressed in myopathy consultation and underwent clinical examination, grip-test, ENMG,functional muscle MRI, muscle biopsy, acylcarnitine profile, urinary organic acid chromatography, and genetic analysis of beta-oxidation genes.
Results: The patient has experienced shortness of breath and painful exercise intolerance since the age of 41, which occurred either immediately with physical activity or later (the next day). She had a history of bipolar disorder and was on sertraline for two and a half years. No change in sertraline dosage had been made at the time the symptoms began.
The clinical examination and ENMG were normal. The grip test revealed resting and post-exercise hyperlactatemia. Functional MRI showed T2 STIR hyperintensities in the lower limbs and abnormalities in dynamic phosphorus spectroscopy, indicating increased lipid degradation products, a high basal metabolism, and delayed recovery. Muscle biopsy showed lipid storage: all muscle fibres exhibited lipid droplets visible with Oil-Red-O staining. The analyses of plasma acylcarnitines and urinary organic acids revealed mild anomalies consistent with a MADD-like profile.
Genetic analysis were negative.
She was supplemented by Riboflavin and gradually discontinued sertraline. 10 days after sertraline discontinuation, she experienced a significant improvement of her symptoms and returned to her previous state.
One month after sertraline discontinuation analyses of plasma acylcarnitines had normalized.
Monitoring of urinary organic acids under treatment are pending.
Conclusion: This case comprehensively illustrates the muscular toxicity of sertraline and the favorable outcome after treatment discontinuation. This toxicity must be well-recognized given the current high prescription rate of sertraline.
References:
1. Sunebo S, Appelqvist H, Häggqvist B, Danielsson O. Multiple Acyl-Coenzyme A Dehydrogenase Deficiency Is Associated with Sertraline Use - Is There an Acquired Form? Ann Neurol 2024 Oct; 96(4): 802-811. doi: 10.1002/ana.27030. Epub 2024 Aug 2. PMID: 39092677.
2. Ingoglia F, Tanfous M, Ellezam B, Anderson KJ, Pasquali M, Botto LD. MADD-like pattern of acylcarnitines associated with sertraline use. Mol Genet Metab Rep 2024 Sep 16; 41: 101142. doi: 10.1016/j.ymgmr.2024.101142. PMID: 39318848; PMCID: PMC11421287.
‡OD07Cartography of transcriptomic changes in muscle biopsies of patients with late-onset pompe disease
Alexandra Monceau1, James Clark1, Eduard Gallardo2,3,4, Montse Olivé2,3,4, Aurelio Hernández-Lain3,5, Carmen Paradas6,7, Eloy Rivas6,7, Cristina Domínguez-González3,5, George Papadimas8, Constantinos Papadopoulos8, Margarita Chrysanthou-Piterou8, Anna Kostera-Pruszczyk9, Biruta Kierdaszuk9, James Lilleker10,11, Mark E. Roberts11, Olimpia Musumeci12, Panos Katsikis1, Priyanka Mehra1, Antonio Toscano12, Giorgio Tasca1, Jordi Díaz-Manera1
1 The John Walton Muscular Dystrophy Research Centre, Newcastle University Translational and Clinical Research Institute, Newcastle Upon Tyne NHS Trust, Newcastle Upon Tyne, United Kingdom, 2 Institut d’Investigació Biomèdica Sant Pau (IIB SANT PAU), Sant Quintí 77-79, 08041 Barcelona, Spain, 3 Center for Biomedical Network Research on Rare Diseases (CIBERER), Instituto de Salud Carlos III, Madrid, Spain, 4 Servei de Neurologia, Unitat malalties neuromusculars, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, 5 Department of Neurology, Neuromuscular Unit, Instituto de Investigación imas12, Hospital 12 de Octubre, Madrid, Spain, 6 Neurology Department, Neuromuscular Disorders Unit, Instituto de Biomedicina de Sevilla, Hospital U. Virgen del Rocío, CSIC, Universidad de Sevilla, Sevilla, Spain, 7 Center for Biomedical Network Research on Neurodegenerative Disorders (CIBERNED), Instituto de Salud Carlos III, Madrid, Spain, 8 Department of Neurology, Eginition Hospital, Medical School, National and Kapodistrian University of Athens, Athens, Greece, 9 Department of Neurology, Medical University of Warsaw, Warsaw, Poland, 10 Division of Musculoskeletal and Dermatological Sciences, Centre for Musculoskeletal Research, School of Biological Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, The University of Manchester, Manchester, United Kingdom, 11 Muscle Disease Unit, Manchester Centre for Clinical Neurosciences, Northern Care Alliance NHS Foundation Trust, Salford, UK, 12 Unit of Neurology and Neuromuscular Diseases, Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy.
alexandra.monceau@newcastle.ac.uk
Background: Late-onset Pompe disease (LOPD), or glycogen storage disease type II (GSDII), is a genetic disorder caused by acid alpha-glucosidase (GAA) deficiency, an enzyme essential for lysosomal glycogen breakdown. GAA deficiency leads to glycogen accumulation within lysosomes, impairing cellular and muscular function. Muscle biopsies in LOPD show a mix of normal-appearing fibers and others with varying levels of glycogen accumulation and autophagic vacuoles.
Aims: This study aimed to map transcriptomic changes in LOPD muscle fibers, differentiating between control fibers, apparently normal Pompe fibers, and glycogen-loaded Pompe fibers. A secondary objective was to compare LOPD and McArdle disease, another GSD, to identify shared and distinct molecular features.
Methods: Spatial transcriptomic analyses were performed on muscle sections using the GeoMx Digital Spatial Profiler, with anti-laminin and anti-LC3B staining to identify muscle membranes and lysosomes, respectively. 93 ROIs were analysed, including 9 from controls, 35 from non-vacuolated Pompe muscle (Pompe NV), 32 from vacuolated Pompe muscle (Pompe V), and 17 from McArdle muscle. A total of 5,069 genes expressed in at least 5% of ROIs were examined.
Results: Transcriptomic profiling revealed distinct molecular differences between Pompe NV and Pompe V fibers. Pompe NV fibers displayed upregulated genes involved in metabolism, including pyruvate metabolism, TCA cycle, and fatty acid oxidation, compensating for glucose shortages. Enhanced expression of genes related to autophagy, mitochondrial biogenesis, stress responses, and MAPK signalling was also observed. In contrast, Pompe V fibers exhibited metabolic exhaustion and upregulation of genes associated with collagen formation and cell death. Additionally, we found 20 axon guidance-related genes, associated with increased occurrence of centrally nucleated fibres, particularly in vacuolated regions, suggests neurogenic changes and muscle reinnervation. Comparative analysis with McArdle disease revealed 174 shared dysregulated genes related to stress responses, extracellular matrix remodeling, apoptosis, and calcium homeostasis, highlighting convergent mechanisms of muscle dysfunction in both disorders.
Conclusion: This study underscores early transcriptomic adaptations in non-vacuolated Pompe fibers, including metabolic reprogramming, mitochondrial dysfunction, and neuromuscular remodeling, as key processes in LOPD progression. Insights into shared and unique pathways between LOPD and McArdle disease may guide future therapeutic strategies for glycogen storage disorders.
‡OD08Biallelic variants in the muscle isoform of Dystonin cause a severe congenital myopathy with contractures and cardiomyopathy
Pinki Munot1
, Maureen Jacob,2, Heike Kölbel3, , Robert Kopajtich2,4, Philip Harrer2,4, Melanie T. Achleitner5, Andreas Hahn6, Anne Schänzer7, Joachim Weis8, Caroline Sewry1,9,10, Rahul Phadke1, Rivka Sukenik-Halevy11,12, Reza Maroofian13, David Goméz-Andrés14, Louise C Wilson15, Gisèle Bonne16, Isabelle nelson16, Véronique Manel17, Ulrike Schara-Schmidt3, Juliane Winkelmann2,4,18, Andreas Roos3,19,20, Johannes A. Mayr5, Felix Distelmaier21, Matias Wagner2,4,22
*Authors 1&2 contributed equally to the work, 1Dubowitz Neuromuscular Centre, Great Ormond Street Hospital, London WC1N 3JH UK, 2Institute of Human Genetics, Klinikum rechts der Isar, Technical University of Munich, School of Medicine and Health, Munich, Germany, 3Department of Neuropediatrics and Neuromuscular Centre for Children and Adolescents, Childreńs University Hospital Essen, University of Duisburg-Essen, Essen, Germany, 4Institute of Neurogenomics, Helmholtz Munich, Neuherberg, Germany, 5University Children's Hospital, Salzburger Landeskliniken (SALK), Paracelsus Medical University, 5020 Salzburg, Austria, 6Department of Child Neurology, Justus-Liebig-University Giessen, Giessen, Germany, 7Institute of Neuropathology, Justus Liebig University Giessen, Germany, 8Institute of Neuropathology, RWTH Aachen University Hospital, Aachen, Germany, 9Wolfson Centre for Neuromuscular Disorders, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry, United Kingdom, 10Cellular Pathology, Salford Royal Hospital NHS Foundation Trust, Northern Care Alliance. Manchester M6 8HD. UK, 11Genetic Institute, Meir Medical Center, Kfar Saba, Israel, 12School of Medicine, Faculty of Medical and Health Sciences, Tel Aviv University, Tel Aviv, Israel, 13Centre for Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London WC1N 3BG, UK, 14Department of Pediatric Neurology, Vall d'Hebron University Hospital, Vall d'Hebron Hospital Campus, Barcelona, Spain, 15Department of Clinical Genetics, Great Ormond Street Hospital, London, UK, 16Sorbonne Université, Inserm, Institut de Myologie, Centre de recherche en myologie, Paris, France - Filière de santé maladies rares neuromusculaires, Filnemus, 17Service de Médecine Physique et Réadaptation Pédiatrique, L'Escale, Hôpital Femme-Mère-Enfant, Hospices Civils de Lyon, Groupement Est, 69500 Bron, France, 18Munich Cluster for Systems Neurology (SyNergy), Munich, Germany, 19Department of Neurology, Heinrich Heine University Düsseldorf, Düsseldorf, Germany, 20Division of Neurology, Department of Medicine, Children' s Hospital of Eastern Ontario Research Institute, The Ottawa Hospital, and Brain and Mind Research Institute, University of Ottawa, Ottawa, Canada, 21Department of General Pediatrics, Neonatology, and Pediatric Cardiology, Medical Faculty and University Hospital Düsseldorf, Heinrich-Heine-University, Düsseldorf 40225, Germany, 22Division of Pediatric Neurology, Developmental Medicine and Social Pediatrics, Department of Pediatrics, Dr. von Hauner Children's Hospital, Ludwig-Maximilian University (LMU) Munich, Munich, Germany.
Background: The Dystonin gene (DST) encodes three tissue-specific isoforms. In contrast to DST-a (“Hereditary Sensory Autonomic Neuropathy VI”) and DST-e (“Epidermolysis bullosa simplex 3”), the muscle isoform DST-b has not yet been associated with a monogenic disease.
Methods: Next Generation sequencing in patients with congenital myopathy, accompanied by RNA and proteome analyses from patient derived fibroblasts with a variant affecting DST-b as well as histological and electron microscopic examinations of available muscle tissue from patients.
Results: We present a case series of 18 patients from 13 unrelated families in which 8 homozygous variants in the largest exon of DST, expressed in the muscle isoform DST-b, could be identified. None of these variants have been previously reported in the literature and all were classified as pathogenic.
Affected individuals range from 1 month to 26 years with severe prenatal onset myopathy with congenital distal more than proximal arthrogryposis at birth. Additionally, the infants had axial weakness, hypotonia and dilated cardiomyopathy. 9/18 patients required CPAP-ventilation and had feeding difficulties. 6/18 individuals died in the first three years of life. In the remaining, there was a spontaneous improvement of symptoms over time and survival to adulthood has been observed in a few. CK was normal in all. Muscle biopsies were available in 6/18 and were done early between 3 weeks and 3 years of age.These showed focal myofibrillar disruption and some nuclei had an undulating membrane. Available neurophysiology and Muscle MRI showed myopathic changes.
RNA sequencing from various tissues revealed that transcripts encoding the DST-b isoform are expressed at high levels in skeletal muscle and heart tissue as well as cultured fibroblasts with lower expression in kidney tissue and no expression in the brain. RNA sequencing from patient derived fibroblasts showed significantly reduced expression of DST and proteomics from patient derived fibroblasts revealed significantly lower levels of DST due to a complete absence of the muscle-specific isoform, while all other isoforms were present in normal amount.
Conclusion: Biallelic variants affecting the DST-b isoform lead to an early onset congenital myopathy with contractures, hypotonia and dilated cardiomyopathy.
Diagnostics and Cross-cutting Therapies
DCC01Immunohistochemical fibre typing of frozen muscle biopsies and the significance of variations of the Fast 2X subtype
D. Chambers
1,2, Y. M. Lim1, R. Phadke1, K. Frontzek1, C. Sewry2,3
1 Division of Neuropathology, UCL Queen Square Institute of Neurology and National Hospital for Neurology and Neurosurgery, University College Hospitals NHS Foundation Trust, London, UK, 2 Dubowitz Neuromuscular Centre, UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 3 Wolfson Centre for Neuromuscular Disorders, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry, United Kingdom
sejjdpc@ucl.ac.uk
Background: Myosin Heavy Chains (MyHC) are an integral part of muscle structure and function but are subject to distributional, developmental and pathological variability. Within a clinical setting MyHC-I (Slow), MyHC-II (Fast) and developmental isoforms are assessed routinely but the sub-types MyHC-IIA and MyHC-IIX are not investigated and may be important to aid in diagnosis across a range of neuromuscular disorders.
Aims: The primary aim of the study is to assess the normal expression of Fast-IIX myosin across different age groups and how aberrant that expression may be in patients presenting with fatigue and other disease states.
Methods/Materials: To ensure consistency only quadriceps muscle samples were prepared with immunofluorescence and immunohistochemical techniques utilising antibodies including clone 6H1, specific to MyHC-IIX fibres, and digitally captured to prepare whole slide images for analysis using QuPath with a CellPose extension. A total of 80 samples were analysed comprising pathologically defined groups: minimal change (n=32), fatigue (n=35), myopathic (n=11) and dystrophic (n=2) cohorts.
Results: An average of 6925 (range 357 to 118550) fibres per sample were analysed with the minimal change cohort demonstrating positivity in all age groups (youngest 2 weeks) with an average of 16.23%. The dystrophic samples exhibited the least expression of MyHC-IIX fibres, 3.89%, followed by the myopathic samples, 6.42%. In comparison to the minimal change samples the fatigue cohort showed lower expression, 16.23% and 12.73% respectively, however the maximum abundance demonstrated more variance; 50.13% to 26.60%.
Conclusion: These results confirm the reduction of MyHC-IIX fibres in muscular dystrophies and myopathies, expand upon the current knowledge and provide the basis for an automated script to aid in diagnostic interpretation. This has already contributed to a baseline of MyHC-IIX expression that may be useful in future studies and potentially the diagnostic pathway. In particular the expression of MyHC-IIX has been demonstrated in samples taken during the neonatal period and whilst this young age was not represented in the samples presenting with myopathy or fatigue, lower overall expression across all ages was observed indicating a potential relationship. Additionally, several samples with minimal pathology but presenting with rhabdomyolysis demonstrated a significantly lower or higher expression which is being investigated
‡DCC02Advancing Splicing Variant Analysis in Hereditary Neuropathies and Other Neuromuscular Disorders with Targeted Long-Read RNA Sequencing
Alessandro Bertini1,2
, Ricardo Parolin Schnekenberg2, Ilaria Quartesan3, Stefano Facchini2, Riccardo Currò2,3, Arianna Manini4, Arianna Ghia2, Enrico Bugiardini2, Matilde Laurà2, Mary M Reilly2, Henry Houlden2, Andrea Cortese2,3
1 Unit of Rare Neurological Diseases, Department of Clinical Neurosciences, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy, 2 Department of Neuromuscular Diseases, UCL Queen Square Institute of Neurology, London WC1N 3BG, UK, 3 Department of Brain and Behavioral Sciences, University of Pavia, 27100 Pavia, Italy, 4 Neurology Unit, Foundation IRCCS Ca' Granda Ospedale Maggiore Policlinico, Dino Ferrari Center, Neuroscience Section, Department of Pathophysiology and Transplantation (DEPT), University of Milan, Via Francesco Sforza 35, 20122, Milan, Italy.
Alessandro.bertini@unimi.it
Background: Short-read whole-genome sequencing (srWGS) has significantly increased the identification of non-coding variants, underscoring their role in hereditary disorders. However, without functional validation, interpreting these variants remains challenging. Amplicon-based long-read RNA sequencing (Amp-lrRNAseq) represents a cost-effective method to analyze splicing in full-length transcripts while preserving phasing.
Aims: This study aimed at taking advantage of Amp-lrRNAseq to predict the impact of non-coding variants on transcript processing in selected patients.
Methods: Variants were identified in four patients with hereditary neurological disorders through short-read WGS and prioritized based on phenotype relevance and computational predictions of splicing disruption. Targeted long-read sequencing (LRS) of full-length transcripts was performed on patient-derived fibroblasts or whole blood. Quantitative PCR (qPCR) was used to assess the impact of the identified variants on gene expression.
Results: In a patient with Charcot–Marie–Tooth type 2, we identified a homozygous GDAP1 variant (c.311-23A>G), previously reported in the literature. We were able to confirm how the mutation activates a cryptic splice site in intron 2, causing the inclusion of 22 intronic nucleotides into exon 2. We also validate previous observations of aberrant splicing caused by a known heterozygous POLR3A mutation (c.1909+22G>A) in a spastic ataxia patient. In a patient presenting with Behr syndrome (spastic ataxia, visual loss, and peripheral neuropathy), a novel homozygous deletion in OPA1 (c.4_5+2del) resulted in skipping of the final coding exon, with reduced OPA1 expression in patient fibroblasts. Lastly, a patient with early-onset myopathy carried a biallelic PYROXD1 variant (c.85-5A>G) that promotes inclusion of four intronic nucleotides, likely introducing a premature stop codon (p.Gln29fs).
Conclusion: Targeted long-read sequencing of full-length transcripts clarifies how genetic variants disrupt splicing and lead to disease, offering a cost-effective, versatile option for variants that match the clinical phenotype but lack definitive
DCC03Genetic landscape of congenital myopathies and muscular dystrophies in the UK: a comprehensive analysis of diagnostic outcomes of next generation sequencing analysis over a 10-Year Period (2014-2023)
Gianpaolo Cicala
1,2
, Jo Mccauley3, Rachael Mein4, Cheryl Walsh3, Francesco Muntoni
1
, Anna Sarkozy
1
, 1 The Dubowitz Neuromuscular Centre, University College London, and MRC Centre for Neuromuscular Diseases, Neurosciences Unit, Great Ormond Street Hospital, London, UK, 2 Pediatric Neurology, Università Cattolica del Sacro Cuore, Rome, Italy, 3 Genetics Laboratory, Synnovis Analytics, Guy's Hospital, London, UK, 4 Genomics Unit, NHS England, Wellington House, London, UK.
Gianpaolo.cicala@gosh.nhs.uk
Background: Congenital myopathies (CM) and congenital muscular dystrophies (CMD) are rare, clinically and genetically heterogeneous neuromuscular conditions characterized by muscle weakness, with onset at birth or in the first few months of life. Recently, next-generation sequencing (NGS) has significantly enhanced diagnostic capabilities and transformed the diagnostic process for rare conditions.
Aims: This study aims to provide insights into genetic aetiology of CM and CMD and describe genotypic prevalences assessed in the Highly Specialized Service (HSS) at the Dubowitz Neuromuscular Centre in London, UK, studied with a NGS panel. We also provide an outcome analysis for NGS testing at our Service for the last 10-years.
Methods/Materials: All patients referred to the HSS for NGS analysis of CM and/or CMD gene panels in the years 2014-2023 were included.
Results: 1927 patients were included, for a total of 2352 genetic analyses. We identified 553/1927 (28.7%) unrelated individuals with a genetic diagnosis of CM or CMD, with pathogenic variants in 49 different genes. Of these, 345 had a diagnosis of CM and 208 of CMD. The most common CMs were related to variants in RYR1 (23.8%), followed by TTN (10.7%), MTM1 (10.4%), NEB (8.7%), SELENON (7.5%), ACTA1 (6.7%), and DNM2 (4.6%) genes. Pathogenic changes in further 27 CM genes were also identified.
The most common CMDs were due to variants in COL6A1 (20.7%), LAMA2 (15.4%), COL6A2 (13.5%), COL6A3 (7.2%), GMPPB (6.7%), POMGnT1 (6.3%), FKRP (6.3%) and LMNA (4.8%) genes. Pathogenic changes in further 16 CMD genes were also identified.
1354 patients remained undiagnosed. Of these, 78 patients (5.7%) carried a heterozygous pathogenic change in a recessive gene, and 419 patients (31%) carried a VUS, with variants in RYR1 (16.9%), NEB (14.%) and TTN (12.8%) genes being the most frequent ones.
Conclusion: This work provides a comprehensive review of outcome of NGS in CM and CMD patients in the UK, highlighting the complex molecular aetiology of these rare conditions. We also underline the relative higher frequency of CM, with RYR1-CM being the most common subtype. This data will help diagnosis and counselling of families with this group of conditions.
DCC04Multi-tier genomic newborn screening for Rare Diseases and its impact on therapies: the EU-IHI Screen4Care project
Alessandra Ferlini
1, Fernanda Fortunato1, Alice Margutti1, Rita Selvatici1,2, Emanuele Agolini3, Silvia Ottombrino3, Antonio Novelli3, Enrico Bertini3, Aldona Zygmunt4, Michela Zuccolo5, Matt Rodesch5, Maria Martinez Fresno6, Moshe Einhorn7, Sergi Beltran8, Leslie Matalonga8, Andreas Clemens9, Stefaan Sansen10, Kathrin Freyler11, Janbernd Kirschner11
1University of Ferrara, Unit of Medical Genetics, Ferrara, Italy; 2Consorzio Futuro in Ricerca, Ferrara, Italy; 3Bambino Gesù Pediatric Hospital, Medical Genetics & Genomics Platform, Roma, Italy; 4Pfizer Inc., Collegeville, Pennsylvania, Collegeville, United States; 5F.Hoffmann-La Roche AG, Basel, Switzerland; 6Illumina Ltd, UK; 7Genoox LTD, Tel Aviv-Yafo, Israel; 8Centro Nacional de Análisis Genómico (CNAG) Barcelona, Spain; 9Novartis Pharma AG, Basel, Basel-Stadt, Suisse; 10Sanofi, Diegem, Machelen, Belgium; 11University of Freiburg, Department of Neuropediatricand Muscle Disorders, University of Freiburg, Germany
fla@unife.it
Background: The Screen4Care (S4C) is a research project funded by EU-IHI with the aim of shortening the path to diagnosis for rare diseases (RDs) through genetic and genomic newborn screening (gNBS).
Aims: We will carry on gNBS in up to 25.000 infants in Italy, Germany, and France (other countries oncoming). To do that, we have designed a clinical, genetic, and operational pipeline. A process to select the treatable rare diseases (RDs) to be screened was codified and dedicated screening tools were designed.
Methods/Materials: We adopted a mandatory criterion which is treatability, and other specific criteria providing cut off-narrowed scores which are mendelian inheritance, natural history knowledge, clinical utility, and amenability of NGS to prioritize the gene list to be screened. These genes have been enriched in a capture-based panel (TREAT) which has been designed and technically validated. Due to the capability of TREAT panel of detecting CNVs, via an innovative, locus-specific, design, and new algorithms, both small and copy number variants will be identified.
Results: The TREAT-panel (first tier) includes 245 genes associated with the following phenomics: 106 metabolic, 33 blood and coagulation, 29 endocrine, 26 immunological, 25 neurological and neuromuscular, 9 renal, 6 mendelian syndromes, 4 cardiological, and 7 other phenotypes (see Figure 1). We plan to carry on also a pivotal trial based on WGS-NBS (second tier) to compare/integrate TREAT panel output. Early symptomatic infants resulted negative at the gNBS will be studied by diagnostic WGS (third tier). Clinical, operational and bioinformatic pipelines were designed (Figure 2), NBS sequencing will be carried in a single Hub (OPBG, Italy) and the 24 European Reference Networks (ERNs) will be involved in the diagnostic and care follow-up of positive babies. Impact on RDs will be high allowing detection at birth and therefore early access to therapies in 245 RDs, including 25 neuromuscular conditions as Duchenne muscular dystrophy and 5q-spinal muscular atrophy.
Conclusion: Babies enrolment has started the 3rd of December 2024 (ClinicalTrial.Gov NCT06549218). The S4C goal is to design and validate a multi-tier, sustainable, ethical, and cost-effective gNBS strategy to be translated into diverse health systems.
Funding:
This work has been funded by the EU-IHI Screen4Care project, grant number No 101034427
Figure 1

Figure 2
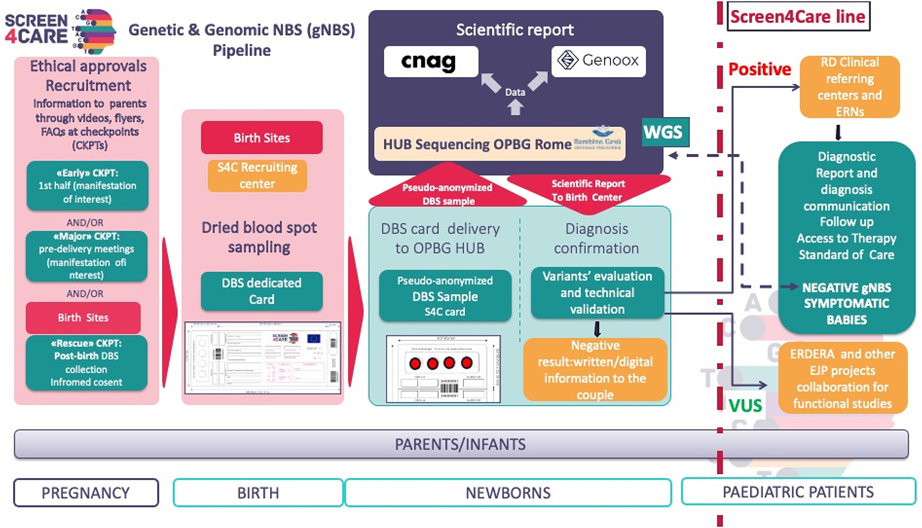
DCC05Familial case of Bethlem myopathy caused by the insertion of an ALU element in COL6A2
Leonela Luce1
, German Demidov2, Jennifer Duff1, Vicente Yépez3, Adam McFarlane1, Alba Segarra Casas1,4, Panos Katsikis1, Steven Laurie5,6, Marianne de Visser7, Anneke van der Kooi7, Volker Straub1, Ana Töpf1
1John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK, 2Universitätsklinikum Tübingen– Institut für Medizinische Genetik und angewandte Genomik, Tübingen, Germany, 3School of Computation, Information and Technology, Technical University of Munich, Munich, Germany, 4Genetics Department, Institut de Recerca Sant Pau (IR SANT PAU), Hospital de la Santa Creu i Sant Pau, Genetics and Microbiology Department, Universitat Autonoma de Barcelona, Barcelona, Spain, 5Centro Nacional de Análisis Genómico, C/Baldiri Reixac 4,08028, Barcelona, Spain, 6Universitat de Barcelona (UB), Barcelona, Spain, 7Department of Neurology, Amsterdam University Medical Centers, Location AMC, Neuroscience Institute, University of Amsterdam, 1107 AZ, The Netherlands.
Leonela.Luce@newcastle.ac.uk
Background: Ullrich congenital muscular dystrophy and Bethlem myopathy (BM) are a spectrum of diseases caused by molecular alterations in COL6A1, COL6A2, COL6A3 or COL12A1. BM is the milder end of the spectrum as patients present mild symptoms and remain ambulant till adulthood. Alu elements are retrotransposons of ∼300bp and their retrotransposition around the genome generates insertions and/or deletions that can be disease causing. Only scarce reports have linked Alu elements to the development of neuromuscular disorders. Here, we present a three-generation familial case of BM, where six affected members presented onset of symptoms in childhood, slow progressive proximal muscle weakness of upper and lower limbs, joint contractures, difficulty walking, and a typical collagenopathy pattern on muscle CT.
Aims: Our aim was to identify the disease-causing molecular alteration and fully understand the pathomechanism behind it.
Methods/Materials: A DNA sample from the index case was initially analysed by whole exome sequencing. No single nucleotide nor indel variants in the COL6 and COL12 genes were identified. Exome data was then analysed applying a pipeline for copy number and structural variants as part of the Solve-RD project. Candidate variants were segregated. Collagen6 immunostaining and RNAseq was performed on patient's fibroblasts.
Results: Re-analysis of exome data detected a large heterozygous insertion in exon 10 of COL6A2, and its exact size and complete sequence was determined by PCR-sanger sequencing. The variant consists of an insertion of ∼321bp between positions c.989_990 (hg19:chr21:47536717), 10bp before the 3’ end of exon 10. Two key elements of the inserted sequence indicate that it stems from an Alu element: a target site duplication and the conserved A5TACA6 motif. The insertion co-segregates with the presence of clinical symptoms, while it is absent in non-affected family members. RNAseq analysis identified an alternative transcript (∼10%), lacking exon 10 and absent in control samples, leading to an in-frame deletion. Proband’s fibroblast showed a collagen6 immunostaining pattern similar to BM control.
Conclusion: We confirmed the clinical diagnosis of BM by the insertion of an Alu element in COL6A2. To our knowledge, this constitutes the first report of a COL6-related myopathy caused by an Alu mobile element.
DCC06Mainstreaming Genomics in Neurology – Nurse-Led Neurogenetics Clinic Service Evaluation of Neuromuscular Patient Cohort
Mark Philipp McQueen-Mencias1
, Dr. Frances Elmslie1 Dr. Emma Matthews1,
1St George’s University Hospitals NHS Foundation Trust
Background: An innovative nurse-led neurogenetics clinic was set up in St George’s University Hospitals NHS Foundation Trust. The aim of the service is to improve the diagnosis and health outcomes of patients with rare neurogenetic diseases. The objective is to mainstream genomics in neurology by providing equitable access to genetic testing, education, and counselling, signposting to hospital and community services, and to promote clinical research. The nurse-led neurogenetics clinic initially focused on neuromuscular disorders and complex epilepsies.
Aim: To assess the activity of the nurse-led neurogenetics service from referral to reporting of genetic result. The primary focus is on patients with a background of neuromuscular diseases such as neuropathy, muscle disorders, motor neurone disease (MND), and spinal muscular atrophy (SMA).
Methods: Service evaluation of the nurse-led neurogenetics clinic between March 2022 to March 2024.
Results: There were 654 referrals to the nurse-led neurogenetics clinic in total between March 2022 and March 2024. 282 patients were seen by the neurogenetics CNS with a background of neuropathy, muscle disorders, MND, and SMA. 244 patients consented to genetic or genomic testing and 138 participated to the National Genomic Research Library. There were 78 cases with an identified causative genetic variant. 9 patients are receiving disease-specific treatment.
Conclusion: The nurse-led neurogenetics service demonstrates a service model that effectively mainstreams genomics and genetic testing in neurology improving equitable access to genetic testing and informing management.
DCC07RNA analysis as diagnostic tool in patients with congenital myopathy and muscular dystrophy
Juliane S Müller1,
Marco Savarese2, Victoria Lillback2, Vicente A. Yepez3, Anna Esteve-Codina4, Luke Perry1, Pinki Munot1, Adnan Manzur1, Jo McCauley5, Chloe Flett1, Rahul Phadke1, Karl Frontzek1, Ana Töpf6, Francesco Muntoni1, Anna Sarkozy1
1The Dubowitz Neuromuscular Centre, University College London, and Great Ormond Street Hospital, London, UK, 2Folkhälsan Research Center, University of Helsinki, Helsinki, Finland, 3Technical University of Munich, Garching bei München, Germany, 4CNAG-CRG, Centre for Genomic Regulation, Barcelona, Spain, 5Synnovis LLP, Guy’s Hospital, London, UK, 6John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK.
j.mueller@ucl.ac.uk
Background: Despite the increased use of Whole Genome and Whole Exon Sequencing, many patients with Congenital Myopathy (CM) or Congenital Muscular Dystrophy (CMD) still do not receive a definite genetic diagnosis. These patients are thought to carry pathogenic variants in novel, yet uncharacterised disease genes, or deep intronic, structural or splicing variants in known genes that were not detected by routine diagnostic procedures.
Aims: To use RNA analysis to complement the routine genetic analysis in patients with CM and CMD referred to the Dubowitz Neuromuscular Centre in London.
Methods/Materials: We investigated 35 patients with suspected CM or CMD who remained without a confirmed genetic diagnosis after standard diagnostic testing, and patients where genetic testing returned a variant of unknown significance (VUS) that could alter splicing. 14 patients were suspected to have a recessive Titinopathy, and 4 to have LAMA2 related muscular dystrophy with absence of laminin 211 on muscle biopsy. The remaining patients carried VUSs in other genes (e.g. DMD, COL6A1, COL6A2, NEB). RNA was extracted from skeletal muscle biopsies and analysed by RT-PCR or RNA sequencing (RNASeq).
Results: RNA analysis contributed to establishing the genetic diagnosis in 20 of the 35 patients. RT-PCR demonstrated aberrant splicing and thus supported variant pathogenicity in 10 cases. Through RNASeq we confirmed the pathogenicity of 2 homozygous intronic pathogenic variants (TNNT3 and TTN), identified missing second pathogenic TTN variants in 5 patients and disease-causing variants in 3 patients in MTM1, LAMA2 and TTN/SRPK3, respectively. Outcomes of splice altering variants on a molecular level ranged from exon skipping, inclusion of intronic sequences, leaky splicing, to the introduction of pseudo-exons through the activation of cryptic splice sites.
Conclusion: This work showcases the important role of RNA analysis in skeletal muscle from patients with unsolved CM and CMD. Through RNA work we were able to diagnose patients where the pathogenic variants were previously missed and clarify the role of VUSs. This work also highlights the key role of the muscle biopsy to provide material for the RNA analysis, as many relevant CM or CMD disease genes are not expressed in blood or skin fibroblasts.
DCC08A UK Platform for Nucleic Acid Therapy for Rare Diseases – the UPNAT consortium
Ella F Whittle1
, Kylie-Ann Montgomery1,2, Alice Davidson3, Mina Ryten4, Carlo Rinaldi5, Nick Lench6, Catherine Ryan1, Francesco Muntoni1, Haiyan Zhou1 and on behalf of the UPNAT consortium
1Great Ormond Street Institute of Child Health, University College London, London, United Kingdom, 2Department of Neuromuscular Diseases, Queen Square Institute of Neurology, UCL, London WC1N 1PJ, UK, 3Institute of Ophthalmology, University College London, London, UK, 4Department of Genetics and Genomic Medicine, Great Ormond Street Institute of Child Health, University College London, London, UK /UK Dementia Research Institute at The University of Cambridge, Cambridge, United Kingdom / Department of Medical Genetics, NIHR Cambridge Biomedical Research Centre, University of Cambridge, Cambridge, UK, 5Institute of Developmental and Regenerative Medicine (IDRM), Department of Paediatrics, University of Oxford, 6MRC Nucleic Acid Therapy Accelerator, Research Complex at Harwell, UK
e.whittle@ucl.ac.uk
Introduction: Nucleic acid therapeutics (NATs) offer great potential to treat rare diseases by targeting specific genetic causes. The rise in NAT clinical trials and approved therapies highlights their role in research to transform new ideas into new treatments and unique opportunities for preclinical and clinical studies, in which the UK has a high level of expertise.
Aims: UPNAT is the UK Platform of Nucleic Acid Therapy for rare diseases, funded by the MRC and the NIHR, and is part of the Rare Disease Research UK Platform (https://rd-research.org.uk/). Its aim is to advance NAT development for patients with rare disease in the UK.
Methods: UPNAT is developing a UK framework for NAT delivery by creating essential resources and establishing a national network comprising scientists, clinicians, geneticists, patient advocates, charities, industry partners, and regulatory bodies. Key collaborators include NIHR Biomedical Research Centres, the UKRI Nucleic Acid Therapeutics Accelerator (NATA) Hub, Genomics England, and Genetics Alliance UK.
Results: Three working groups have been created to support NAT development:
Target Selection: This group is formulating guidelines for selecting genetic variants, target genes, applicable disease conditions and suitable patients for NAT in the UK and piloting the implementation of these guidelines in the highly specialised NHS services. A pilot study with Great Ormond Street Hospital is underway. A draft guideline structure has been shared for expert input, and UPNAT has contributed to finalising the recently published N1C variant guidelines.
Preclinical Development on individualized ASO therapy for ultra-rare diseases: Collaborating with academic groups and international NAT consortia, the team is exploring effective pathways for developing individualised genetic therapies at scale.
Clinical Translation: The team is streamlining clinical translation and regulatory approval by establishing data-sharing initiatives, offering education and training opportunities for the next generation of clinicians and researchers, and by facilitating the creation of a NAT adverse event registry.
Conclusion: By fostering collaboration and resource sharing, UPNAT seeks to accelerate NAT development for rare disease patients in the UK and contribute to international efforts advancing these therapies.
‡DCC09Evaluation of MRI muscle-water T2 as a biomarker in four distinct subtypes of Charcot-Marie-Tooth disease
Nick Zafeiropoulos
1,2
, Jasper M Morrow1, Carolynne M Doherty1, Stephen Wastling1, Evelin Milev2, Tina Banks2, Sachit Shah3, Mariola Skorupinska1, Menelaos Pipis1, Amy McDowell1, Luke O'Donnell1, Alex M Rossor1, Matilde Laurá1, Francesco Muntoni1, Tarek Yousry1, Mary M Reilly1 and John S Thornton1
1UCL Queen Square Institute of Neurology, University College London, London, United Kingdom, 2Great Ormond Street Hospital, London, United Kingdom, 3National Hospital for Neurology and Neurosurgery, London, United Kingdom
Background & Aims: The aim of this work was to investigate calf-level muscle water T2 (T2m) as a MRI biomarker for the assessment of the inherited neuropathy Charcot-Marie-Tooth disease. Here we present a first evaluation of T2m and apparent fat fraction (ffa) determined in a subset of participants in our recent studies which demonstrated that muscle fat fraction is a responsive outcome measure in adults with CMT1B, CMT2A and CMTX1 and a younger cohort with CMT1A.
Methods: T2m and the associated relaxometry-yielded fat fraction (ffa) were obtained from CPMG multi-echo data using a multi-component (corresponding to the muscle and fat tissue compartments) slice-profile compensated extended phase graph (EPG) signal model fitted pixel-wise to the data using maximum likelihood estimation (MLE). T2m, ffa, the B1 field error factor (B1f), overall amplitude (α) and Rician noise SD (σN) were estimated. For comparison, mean cross-sectional muscle fat-fraction was determined independently by 3-point Dixon MRI (ffd). Corrections were applied to both ffd (fat multi-peak spectrum) and ffa for magnetization transfer and T1 effects.
Results: T2m and ffa for all patients were significantly higher than for controls. Longitudinal changes seen in individuals were significant for T2m in 1A patients but not for any other category at the group level. ffd distributions were qualitatively similar, showing significant correlation with ffa, and to a lesser degree with T2m.
Conclusion: T2m increases were seen in calf muscles of children and adolescents with CMT1A when their ffa in these muscles were normal suggesting it is an early biomarker of disease. Greatest T2m was seen in subtypes (CMT1B and CMT2A) which have the fastest clinical progression suggesting T2m is a biomarker of disease activity. Unlike previous reports of significant ffd changes with larger group sizes, here no significant longitudinal changes were observed for any subtypes for ffa at the group level; for T2m longitudinal increase was observed in 1A patients. The distribution of T2m changes within the subtypes was visually distinct, and there was evidence in individual participants of T2m decrease as well as increase. This may support the hypothesis for its sensitivity to early or transient disease activity.
AUTHOR INDEX
Achleitner Melanie T. (‡OD08) S62
Ackermann-Bonan Isabelle (OD06) S61
Adcock Kate (MND03) S9
Addy Charlotte (MD03) S40
Ader Flavie (NMJ&C01) S13
Aghaeipour A. (D15) S26
Agolini Emanuele (DCC04) S65
Aguti S. (D15) S26
Ahola Sofia (MD01) S38
Alavi Shahryar (PN02) S52
Alcock Lisa (DC12) S35
Ali Ahsan (D01) S17
Almuhanna Abdulaziz (‡PN05) S55
Alston Charlotte (‡MD10) S44, (MD08) S43
Alston Charlotte L. (MD09) S44, (OD01) S57, (OD03) S59
Alvarez Grecia (MND05) S10, (MND06) S11
Alves Frauke (‡D06) S21
Alvi Javeria Raza (PN02) S52
Amor David (D04) S19
Anastassiadis Konstantinos (‡D16) S27
Arany Eszter Sara (MD02) S39
Arbogast S. (D05) S20
Arena Ignazio Giuseppe (MD03) S40, (MD20) S51
Arridge Marzena (‡MD15) S48
Ashby Elizabeth (MD03) S40
Aughey Gabriel (PN02) S52
Aynekin Busra (PN02) S52
Azcón Javier Ramón (‡D07) S21
Başak A. Nazlı (PN02) S52
Babu Ramya Ramesh (MND08) S12
Baets Jonathan (PN02) S52
Bahlo Melanie (D04) S19
Banks Tina (‡DCC09) S68
Banu Selina H. (PN02) S52
Baple Emma (S02) S3
Baranello Giovanni (DC17) S38, (MND07) S11
Barohn Richard (‡NMJ&C07) S16
Barrow I (MD16) S48
Barrow I. (MD07) S42
Barrow Isabel (MD06) S42
Barthel B (‡DC16) S37
Barton F (MD16) S48
Beecroft Sarah J (D04) S19
Beeson David (NMJ&C03) S14
Beggs Alan H. (DC07) S32
Behr Professor Elijah (DC11) S34
Bellaiche Yohanns (PN02) S52
Beltran Sergi (DCC04) S65
Bernardino-Gomes Tiago (‡DC04) S30
Bertini Alessandro (‡DCC02) S64
Bertini Enrico (DCC04) S65
Bettolo Chiara M. (MND01) S8
Bettolo Chiara Marini (D12) S24, (DC01) S28, (DC14) S36, (MND05) S10, (MND06) S11
Bevilacqua Jorge (DC03) S29
Bick David (S01) S2
Biggs Heather (MD03) S40, (MD20) S51
Bilby Jessica (DC17) S38
Birkbeck Matthew G. (MND01) S8
Birnbaum S (DC13) S35
Bjerre Anna (OD03) S59
Blamire Andrew M. (MND01) S8
Bohill Julie (DC07) S32, (DC08) S32
Bohndiek Sarah (S08) S6
Bolano-Diaz C (DC17) S38
Bonne Gisèle (‡DC10) S33, (‡OD08) S62
Bonne Giselle (D04) S19
Borland Holly (DC02) S28, (DC03) S29
Bourke John P (DC14) S36
Bowen M. (D09) S22
Brady Stefen (D04) S19
Brister Danielle (MD04) S41
Brown Philip (DC12) S35
Bruno Claudio (DC02) S28
Brusse Esther (PN02) S52
Bugiardini E (MD14) S47
Bugiardini Enrico (‡DCC02) S63, (D04) S19, (DC15) S36, (MD11) S45, (MD12) S46
Butterfield Russell (DC15) S36
Byrne Calum (MND02) S9
Caberg Jean-Hubert (MD09) S44
Cabrera-Orefice Alfredo (‡MD13) S46, (MD09) S44
Cabrera-Serrano Macarena (D04) S19
Cahalan Stephen D (‡PN05) S54
Cammish Phillip (DC05) S30, (DC06) S31
Cansu Ali (PN02) S52
Carr Aisling (PN04) S54
Carraro Elena (DC15) S36
Carrington Stephanie (PN04) S54
Carroll Liam (D04) S19
Carter Ellis (‡MND04) S10
Carver Aleks (DC08) S32, (MND03) S9, (MND05) S10, (MND06) S11
Casas Alba Segarra (DCC05) S66
Castañeda-Tamez Paulina (‡MD13) S46
Çakar Arman (PN02) S52
Cavalcante Elzo (MND03) S9
Chambers D. (DCC01) S63
Chandler Natalie (MD11) S45
Cheng Kevin (D02) S18
Childs Anne-Marie (DC06) S31
Childs Jordan (MD06) S42
Chinnery Patrick (‡MD10) S44, (MD03) S40, (MD08) S43
Chinnery Patrick F (‡MD19) S50
Chintalaphani Sanjog (D04) S19
Choi SungWoo (D02) S18
Chrysanthou-Piterou Margarita (‡OD07) S61
Chrzanowska-Lightowlers Zofia M. A. (‡MD13) S46
Chung Wendy K. (PN02) S52
Cicala Gianpaolo (DC17) S38, (DCC03) S64
Claeys Kristl (DC02) S28
Clark Chris (DC17) S38
Clark James (‡D07) S21, (‡OD07) S61, (D03) S19, (D08) S22, (D17) S27
Clemens Andreas (DCC04) S65
Clement Emma (NMJ&C04) S13
Coimbra-Neto Antônio Rodrigues (PN02) S52
Collier Jack (MD04) S41
Collier Jack J. (‡MD13) S46, (OD03) S59, (OD04) S60
Collin Matthew (MD06) S42
Collins Catherine (D03) S19, (D08) S22, (D12) S24
Colnet Amélie de (OD06) S61
Comley L H (NMJ&C06) S15
Corbex E. (D09) S22
Cortese A. (PN06) S55
Cortese Andrea (‡DCC02) S64, (D04) S19, (PN01) S51, (PN02) S52, (PN08) S56
Coulson D. (D15) S26
Cowling Belinda (DC07) S32
Cox Dan (‡D07) S21, (D03) S19
Creigh Adam (‡MND04) S10
Cross Emily (MD05) S41
Cuisset Jean-Marie (‡DC10) S33
Currò Riccardo (‡DCC02) S64, (PN01) S51, (PN08) S56
Curro R. (PN06) S55
Curro Riccardo (D04) S19, (PN02) S52
Curtis Liz (‡MD10) S44, (MD08) S43
Cutting Emma (MD20) S51
Díaz-Manera Jordi (‡OD07) S61, (DC14) S36
Da'as Sahar I. (PN02) S52
Dastidar Sumitava (‡D16) S27
Datta Dipanjana (MND08) S12
Davidson Alice (DCC08) S68
Davis Mark R (D04) S19
Day John. W. (DC03) S29
De Monts C (DC13) S35
Delatycki Martin (D04) S19
Demidov German (DCC05) S66
Desai Urvi (DC03) S29
Deshpande Charulata (‡MD10) S44, (MD08) S43
Deveson Ira (D04) S19
Devine Helen (‡MND04) S10
Dhawan Bettolo Anil (DC07) S32
Diaz Carla Bolano (DC01) S28
Diaz-Manera J. (DC17) S38
Diaz-Manera Jordi (D08) S22, (D10) S23, (D17) S27, (DC01) S28, (DC02) S28
Dilek Nuran (DC15) S36
Distelmaier Felix (‡OD08) S62
Dofash Lein (D04) S19
Doherty Carolynne M (‡DCC09) S68
Domínguez-González Cristina (‡OD07) S61
Dominik Natalia (D04) S19, (PN02) S52
Dong Yin (NMJ&C04) S14, (NMJ&C08) S16
Dong Yin Yao (NMJ&C02) S13, (NMJ&C03) S14
Donovan JM (‡DC16) S37
Dowling James J. (DC07) S32
Dresser Kerry (MD20) S51
Dressman Heather Gordish (DC03) S29
Drummond Ellie (DC05) S30
Duchesne Elise (‡DC04) S30
Dudziec M. (‡PN07) S56
Dudziec Magdalena M (PN03) S53
Duff Jennifer (DCC05) S66
Dumonceaux J. (D05) S20, (D09) S22
Dunachie Susanna (MD06) S42
Dyke Jason (D04) S19
Efthymiou Stephanie (PN02) S52
Eichinger Katy (DC15) S36
Einhorn Moshe (DCC04) S65
Elliott Jess (DC05) S30
Ellis Melina (D04) S19
Elmslie Frances (DCC06) S67
Elseed Maha (DC01) S28
Elseed Maha A (DC14) S36
Elsheikh Bakri (DC15) S36
Erdil E (MD14) S47, (OD02) S58
Erdil Esra (MD11) S45, (MD12) S46
Esteve-Codina Anna (DCC07) S67
Evangelista Teresinha (OD06) S61
Fabian Vicki (D04) S19
Facchini Stefano (‡DCC02) S64, (D04) S19
Fahey Michael C (D04) S19
Falabella M (MD14) S47
Falabella Micol (MD11) S45
Falzarano Maria Sofia (‡D06) S21
Farrugia Maria (MND03) S9
Fearnley Liam G (D04) S19
Ferlini Alessandra (‡D06) S21, (DCC04) S65
Fernández-Costa Juan M. (‡D07) S21
Fernández-Garibay Xiomara (‡D07) S21
Fernández-Simón Esther (D03) S21
Fernández-Simón* E. (‡D07) S21
Fernandez Gorka (D04) S19
Fernandez-Eulate Gorka (PN01) S51
Fernandez-Simon Esther (D08) S22
Figueiredo Fernanda Barbosa (PN02) S52
Fitzsimmons Sam (D12) S24
Fitzsimmons Samantha (DC12) S35
Flannery Padraig (MD12) S46
Flett Chloe (DCC07) S67
Foley A. Reghan (DC07) S32
Folland Chiara (D04) S19
Fortunato Fernanda (DCC04) S65
Foster Katie (OD03) S59
Frølich SV (‡DC16) S37
França Marcondes C. (PN02) S52
Franklin Imogen G. (MD06) S42
Fratter Carl (‡MD10) S44, (MD08) S43
Frengen Eirik (MD09) S44, (OD03) S59
Fresno Maria Martinez (DCC04) S65
Freyler Kathrin (DCC04) S65
Fromes Yves (OD06) S61
Frommer J. (D15) S26
Frontzek K. (DCC01) S63
Frontzek Karl (DCC07) S67
Fulea Raul (D12) S24
Futema Marta (DC11) S34
Güleç Ayten (PN02) S52
Güngör Serdal (PN02) S52
Gaeta Alessandra (DC05) S30, (DC06) S31
Galloway Andrew (D03) S19
Galtrey Clare (MND02) S9
Gamaarachchi Hasindu (D04) S19
Gardner Mac (D04) S19
Garone Caterina (MD20) S51
Gaugué Isabelle (PN02) S52
Germain Louise (‡NMJ&C07) S16, (DC15) S36
Geuens Sam (DC09) S33
Ghia Arianna (‡DCC02) S64, (PN08) S56
Gilissen Christian (S03) S4
Giovannini Diane (D04) S19
Girard-Cote Laura (‡DC04) S30
Giunti Paola (PN01) S51
Gobin Stéphanie (OD06) S61
Golder Zoe (MD03) S40
Goméz-Andrés David (‡OD08) S62
Gomes T. Bernardino (MD07) S42
Gorman G. (MD16) S48
Gorman G. S. (MD07) S42
Gorman Gráinne S (MD06) S42
Gorman Grainne (‡DC04) S30
Gorman Professor Grainne (MD17) S49
Gosal David (PN01) S51, (PN04) S54
Graham Robert J. (DC07) S32
Grosz Bianca R (D04) S19
Grover Emma (DC01) S28
Grundmann-Hauser Kathrin (PN02) S52
Guerra Rachel M. (‡MD13) S46
Guglieri Michela (D12) S24, (DC01) S28, (DC05) S30, (DC06) S31, (DC09) S33, (DC14) S36
Haack Tobias B. (PN02) S52
Haagsma Ariele Barreto (D12) S24, (DC01) S28
Hadden Robert DM (PN04) S54
Hadjivassiliou Marios (PN01) S51
Hahn Andreas (‡OD08) S62
Hall Julie (MND01) S8
Hamed Sherifa Ahmed (PN02) S52
Hammadi Dania B. (OD01) S57
Hammans Simon (D04) S19
Hanna M G (OD02) S58
Hanna MG (MD14) S47
Hanna Michael (PN02) S52
Hanna Michael G (‡MD10) S44, (‡MD19) S50, (‡NMJ&C07) S16, (D04) S19, (MD08) S43, (MD11) S45, (MD12) S46, (MD18) S49
Hanna Michael G. (‡MD15) S48
Harms Matt (DC03) S29
Harrer Philip (‡OD08) S62
Harris Elizabeth (DC01) S28
Harrison Emma (MD03) S40, (MD20) S51
Harron Rachel C.M. (D13) S25
Hartley Louise (NMJ&C05) S15
HaselKorn Tmirah (DC07) S32
He Yi (PN02) S52
Heidemann Marcel (DC07) S32
Heidler Juliana (‡MD13) S46
Henderson Robert D (D04) S19
Henehan Leighann (NMJ&C03) S14, (NMJ&C04) S14
Hernández-Lain Aurelio (‡OD07) S61
Herrmann David N (PN03) S53
Heslegrave Amanda (PN01) S51
Heslop Emma (DC05) S30, (DC06) S31, (DC09) S33
Hewamadduma Channa (MND02) S9
Hickson Lucy (DC07) S32, (DC08) S32
Higgs Kiley (DC15) S36
Hildyard John C.W. (D13) S25
Hill Tamara (MD08) S43
Hilsden H (DC13) S35, (DC17) S38
Hilsden Heather (DC03) S29
Hobson Emma (OD03) S59
Holsten S (DC13) S35
Hornby Natasha L. (D13) S25
Horrocks Iain (NMJ&C04) S14
Horvath Rita (‡MD10) S44, (MD02) S39, (MD03) S40, (MD04) S41, (MD05) S41, (MD08) S43, (PN02) S52
Hoshiya Hidetoshi (‡D16) S27
Houlden Henry (‡DCC02) S64, (D04) S19, (PN01) S51, (PN02) S52, (PN08) S56
Hourde C. (D09) S22
Howard R (OD02) S58
Hudon C. (D09) S22
Hudson Judith (DC01) S28
Hunter Heather (DC12) S35
Ibrahim Shahnaz (PN02) S52
Ilyashenko Gennadiy (MND03) S9
Imam Aliza (OD03) S59
Ingell Alexander (MD11) S45
Jacob Maureen (‡OD08) S62
Jacobson Leslie (NMJ&C02) S13
Jalal Salma (‡DC10) S33
James M.K (DC13) S35
James MK (DC17) S38
James Meredith (DC02) S28, (DC12) S35
James Meredith K. (DC03) S29
Jamshidi Yalda (PN02) S52
Jayseelan Dipa (‡NMJ&C07) S16
Jepson James (PN08) S56
Jepson James E. C. (PN02) S52
Joefield Teishel (DC17) S38
Johari Mridul (D04) S19
Johnson Alex (DC05) S30, (DC09) S33
Johnson Alexandra (DC06) S31
Johnson Anna (DC14) S36
Johnson Nicholas (DC02) S28, (DC15) S36
Jones David (‡MND04) S10
Jones P. (D05) S20
Jordanova Albena (PN02) S52
Jungbluth Heinz (DC07) S32, (DC17) S38, (NMJ&C04) S14
Kölbel Heike (‡OD08) S62
Kabiljo R (MD14) S47, (OD02) S58
Kabiljo Renata (‡MD10) S44, (‡MD19) S50, (MD08) S43, (MD11) S45, (MD12) S46, (MD18) S49
Kadhim Kadhim (DC14) S36
Kaliakatsos Marios (MND07) S11
Kallabis Sebastian (MD01) S39
Karimiani Ehsan Ghayoor (PN02) S52
Karkkainen Elena (MND03) S9, (MND05) S10, (MND06) S11
Kaski D. (PN06) S55
Kaski Diego (PN01) S51
Katsikis Panos (‡OD07) S61, (D03) S19, (D08) S22, (D11) S24, (D17) S27, (DCC05) S66
Kaul Ahaan (MND02) S9
Kennerson Marina (D04) S19
Kerr Adam (DC09) S33
Khan A. (MD07) S42
Khan Arif (PN02) S52
Khedr Moustafa (‡D16) S27
Kierdaszuk Biruta (‡OD07) S61
Kinimi Ilin (MND08) S12
Kirschner Janbernd (DCC04) S65
Klingenberg Claus (OD03) S59
Kocak Goknur (DC01) S28
Kok Fernando (PN02) S52
Koohi N. (PN06) S55
Koohi Nehzat (PN01) S51
Kopajtich Robert (‡OD08) S62
Kostera-Pruszczyk Anna (‡OD07) S61
Krüger Marcus (MD01) S39
Kramarz Caroline (PN04) S54
Kronsteiner Barbara (MD06) S42
Kung Jane (NMJ&C04) S14
Kuo Sheng-Han (PN01) S51
Kyrana Eirini (DC07) S32
Labrum R (MD14) S47, (OD02) S58
Labrum Robyn (‡MD10) S44, (MD08) S43, (MD11) S45, (MD12) S46, (MD18) S49
Lagos Daniel (MD05) S41
Laidler Zoe (D03) S19, (D08) S22
Laing Nigel G (D04) S19
Laing Nigel G. (PN02) S52
Lako Majlinda (OD04) S60
Lakshmi K.S (MND08) S12
Lam Amanda (MD12) S46
Lamarche-Vane Nathalie (PN02) S52
Lambton James (OD03) S59, (OD04) S60
Lamont Phillipa J (D04) S19
Lamont Phillipa J. (PN02) S52
Langer Thomas (MD01) S39
Laoudj-Chenivesse D. (D05) S20
Lauffer Marlen (S06) S5
Laurá Matild (‡DCC09) S68
Laurá Matilde (PN03) S53, (PN09) S57
Laurà Matilde (‡DCC02) S64
Laurie Steven (DCC05) S66
Lavin Tim (PN04) S54
Lawless C. (MD07) S42
Lawless Conor (‡DC04) S30, (MD06) S42
Lawlor Michael W. (DC07) S32
Leclaire Leif (PN02) S52
Legouis Renaud (OD03) S59
Leighton Jamie (‡MD10) S44, (MD08) S43
Leighton Jamie K. (MD09) S44
Lemonde Hugh (NMJ&C04) S14
Lench Nick (DCC08) S68
Lennox Anne (DC07) S32
Leo V. Di (MD07) S42
Leo Valeria Di (‡DC04) S30
Leonardis Lea (DC02) S28
Leung Doris G. (DC15) S36
Lewis Leann (DC15) S36
Lightowlers Robert N. (‡MD13) S46
Lignani Gabrielle (PN08) S56
Lillback Victoria (DCC07) S67
Lilleker James (‡OD07) S61, (MND03) S9
Lilleker James B. (MND02) S9
Lilliker James (D04) S19
Lim Y. M. (DCC01) S63
Lin Renee (PN02) S52
Lin S (OD02) S58
Lionello Valentina (‡DC10) S33
Lockhart Paul J (D04) S19
Lofra Robert Muni (DC01) S28, (MND05) S10, (MND06) S11
Lomonosova Yulia (‡D16) S27
Lowe Simon (PN02) S52
Lowes L.P (DC13) S35
Luce Leonela (DC02) S28, (DCC05) S66
Lunn Michael (PN01) S51, (S10) S6
Lupo Vincenzo (PN02) S52
Lyon R (MD16) S48
Müller Juliane S (DCC07) S67
MacDougall J (‡DC16) S37
Machado Pedro (D04) S19
Macken W L (OD02) S58
Macken WL (MD14) S47
Macken William L (‡MD10) S44, (‡MD19) S50, (MD08) S43, (MD11) S45, (MD12) S46, (MD18) S49, (PN04) S54
Madden Matthew (MND03) S9
Madhu Rajesh (OD05) S60
Maganthi Madhuri (MND08) S12
Maguire Alison (‡MD10) S44, (MD08) S43
Male A. (PN06) S55
Man Wai (MD03) S40
Mancini Grazia M. S. (PN02) S52
Mandelenaki Sespoina (NMJ&C04) S14
Manel Véronique (‡OD08) S62
Manera Jordi Diaz (‡D07) S21, (D03) S19, (D11) S24, (D12) S24, (S12) S7
Manini Arianna (‡DCC02) S64
Manzur Adnan (DCC07) S67, (MND07) S11
Margutti Alice (DCC04) S65
Marini Chiara (DC07) S32
Marini-Bettolo Chiara (DC08) S32, (MND03) S9
Mariot V. (D05) S20, (D09) S22
Maroofian Reza (‡OD08) S62, (PN02) S52
Marques Wilson (PN02) S52
Martens William B. (DC15) S36
Marti Ramon (MD20) S51
Martineau O (NMJ&C05) S15
Masingue Marion (D04) S19, (OD06) S61
Mastaglia Frank (D04) S19
Mastellaro S (DC13) S35
Matalonga Leslie (DCC04) S65
Mathew Ann Agnes (MND08) S12
Matias-Valiente Lidia (D10) S23
Matthews Emma (‡NMJ&C07) S16, (DC11) S34, (DCC06) S67, (NMJ&C01) S13
Mayhew A.G (DC13) S35
Mayr Johannes A. (‡OD08) S62
McCallum Michelle (DC01) S28
McCauley Jo (DCC07) S67, (DCC03) S64
McConville John (MND03) S9
McCorvie Thomas J. (OD03) S59
McCullagh Helen (OD03) S59
McDermott Michael (DC15) S36
McDermott Michael P (‡NMJ&C07) S16
McDonald Sam (DC08) S32
McDowell Amy (‡DCC09) S68, (‡MD15) S48
McFarland Professor Robert (MD17) S49
McFarland Robert (‡MD10) S44, (MD08) S43, (OD01) S57, (OD03) S59
McFarlane Adam (DCC05) S66
McLean Catriona A (D04) S19
McNiff Megan (DC06) S31, (DC09) S32
McQueen-Mencias Mark Philipp (DCC06) S67
McWilliams Thomas G. (OD03) S59, (OD04) S60
Mehra Priyanka (‡OD07) S61, (D03) S19, (D08) S22, (D11) S24, (D17) S27
Mein Rachael (DCC03) S64
Mendell Jerry R (DC03) S29
Mengibar Jose M.S. (DC15) S36
Merces George O. T. (‡DC04) S30
Merrison Andria (MND03) S9
Merve Ash (D04) S19
Merve Ashirwad (PN04) S54
Mi Young K (DC13) S35
Miah Mohi-Uddin (D12) S24
Miao Xinyu (PN02) S52
Michell-Sodhi Jassi (DC01) S28, (MND05) S10, (MND06) S11
Mietto Martina (‡D06) S21
Miladi Najoua (DC02) S27
Milev Evelin (‡DCC09) S68
Millner Thomas O (PN04) S54
Milne Paul (MD06) S42
Misceo Doriana (MD09) S44, (OD03) S59
Moat Dionne (DC01) S28, (MND05) S10, (MND06) S11
Moe A. (MD16) S48
Monahan Gavin (D04) S19, (PN02) S51
Monceau Alexandra (‡D07) S21, (‡OD07) S61, (D03) S19, (D08) S22
Montanari Silvia (‡D06) S21
Montgomery Kylie-Ann (DCC08) S68
Montiel Morillo E (DC13) S35
Montse Olivé Eduard Gallardo (‡OD07) S61
Moore Daniel (‡DC10) S5
Morel B. (D09) S22
Morrow Jasper (‡MD15) S48
Morrow Jasper M (‡DCC09) S68
Morsy Heba (PN04) S54
Motazacker M. Mahdi (PN02) S52
Moyle Louise (‡D16) S27
Moylett Áine (MD12) S46
Moylett A (MD14) S47
Moylett Aine (MD11) S45, (MD18) S49
Mozaffar Tahseen (DC03) S29
Mul Karlien (DC15) S36
Muni-Lofra Robert (DC12) S35, (MND03) S9
Munot P (NMJ&C05) S15
Munot Pinki (‡OD08) S62, (DCC07) S67, (MND07) S11, (NMJ&C04) S14
Muntoni F. (D15) S26
Muntoni Francesco (‡D16) S27, (‡DCC09) S68, (D14) S25, (DC06) S31, (DC17) S38, (DCC03) S64, (DCC07) S67, (DCC08) S68, (MND07) S11
Murray L M (NMJ&C06) S15
Musumeci Olimpia (‡OD07) S61
Naik Swati (OD03) S59
Nath Rasya Gokul (D03) S19, (D08) S22, (D12) S24
Nelson Isabelle (‡OD08) S62
Nesbitt Victoria (‡MD10) S44, (MD08) S43
Neumann Katrin (‡D16) S27
Newman J (MD16) S48
Newman Jane (MD17) S49
Ng Joanne (MND08) S12
Ng Yi (MD17) S49
Ng Yi Shiau (MD06) S42
Nicholson Garth (D04) S19
Nitollama P (DC13) S35
Novelli3 Antonio (DCC04) S65
O'Donnell Luke (‡DCC09) S68
O’Donnell Luke (PN03) S52
O’Hanlon Maria E (‡MD10) S44, (MD08) S43
O’Hara Victoria (‡PN05) S55
Ogasawara Y (DC13) S35
Oláhová Monika (‡MD13) S46, (MD09) S44, (OD03) S59, (OD04) S60
Olahova Monika (MD08) S43
Olimpio Catarina (MD02) S39, (MD03) S40
Olive Rivas Montse (DC03) S29
Oprych KB (MD14) S47
Oprych Kathryn (MD11) S45, (MD12) S46, (MD18) S49
Osborn Dan (NMJ&C01) S13
Osborn Daniel P. (PN02) S52
Ottombrino Silvia (DCC04) S65
Pace Filipe Di (DC02) S28
Page Jess (DC07) S32, (MND03) S9, (MND05) S10, (MND06) S11
Pagliarini David J. (‡MD13) S45
Palace Jacqueline (NMJ&C03) S14, (NMJ&C04) S14
Palmowski Pawel (D03) S19
Palvadeau Robin J. (PN02) S52
Papadimas George (‡OD07) S61
Papadopoulos Constantinos (‡OD07) S61
Paradas Carmen (‡OD07) S61, (DC03) S29
Paramonov Ida (MD02) S39
Pardo A. (DC13) S35
Pareyson Davide (PN01) S51
Park Joohyun (PN02) S52
Parman Yesim (PN02) S52
Parmar Jevin M. (PN02) S52
Partlova I (NMJ&C06) S15
Parton Matt (MND03) S9
Patel Y (MD14) S47, (OD02) S58
Patel Yogen (MD11) S45, (MD12) S46, (MD18) S49
Peffers Mandy (D11) S24
Pegoraro Elena (DC03) S29
Peplowska Taisha (‡MND04) S10
Per Huseyin (PN02) S52
Perkins Justin (‡PN05) S55
Perry Chloe (DC05) S30
Perry Luke (DCC07) S67
Pessoa André Luiz (PN02) S52
Pestronk Alan (DC03) S29
Phadke R. (DCC01) S63
Phadke Rahul (‡OD08) S62, (DCC07) S67
Pickett Sarah J. (MD06) S42
Piercy Richard J (‡PN05) S55
Piercy Richard J. (D13) S25
Pinton Luca (‡DC10) S32
Pipis Menelaos (‡DCC09) S68
Pisciotta Chiara (PN01) S51
Pitceathly R D S (OD02) S58
Pitceathly RDS (MD14) S47
Pitceathly Robert (D04) S19
Pitceathly Robert D S (‡MD10) S44, (‡MD19) S50, (MD11) S45, (MD12) S46, (MD18) S49
Pitceathly Robert D.S. (‡MD15) S48
Pitceathly Robert DS (PN04) S54
Pitceathly S (MD08) S43
Pitman Alan (NMJ&C01) S13
Pizzamiglio C (MD14) S47
Pizzamiglio Chiara (‡MD15) S48, (MD11) S45, (MD12) S46
Pogoryelova O (MD16) S48
Pogoryelova Oksana (MD17) S49
Polke J (MD14) S47
Polke James (MD11) S45, (MD12) S46, (MD18) S49, (PN02) S52
Pontoizeau Clément (OD06) S61
Porter Andrew (D03) S19
Prados Ferran (PN01) S51
Prigent Magali (OD03) S59
Privolizzi R. D. (D15) S26
Psifidi Androniki (‡PN05) S55
Pujar Suresh (MND07) S11
Qiu Yichen (PN08) S56
Quartesan Ilaria (‡DCC02) S64, (PN01) S51
Queen Rachel (D08) S22
Quinlivan R (OD02) S58
Quinlivan Ros (D04) S19
Rabinowicz Shira (MND07) S11
Rahman Md Yakeen (D01) S17
Rahman Rezbieara (DC11) S34
Ramdas Sithara (NMJ&C03) S14, (NMJ&C04) S14
Ramdharry G.M. (‡PN07) S56, (PN06) S55
Ramdharry Gita (‡MD15) S48, (PN01) S51, (PN03) S53, (PN09) S57
Ratnaike Thiloka (MD03) S40
Ravenscroft Gianina (D04) S19, (PN02) S52
Read Justin (D04) S19
Receveur NAM (‡DC16) S37
Record Christopher J. (PN02) S52
Reeves Tara (DC01) S28
Reid S. (D09) S22
Reilly M.M. (‡PN07) S56, (PN06) S55
Reilly MM (MD14) S47
Reilly Mary (PN08) S56, (S07) S5
Reilly Mary M (‡DCC02) S64, (‡DCC09) S68, (D04) S19, (MD11) S45, (PN01) S51, (PN03) S53, (PN04) S54, (PN02) S52, (PN09) S57
Renkema H (MD16) S48
Reuben Emily (DC05) S30, (DC06) S31
Reza Mojgan (D08) S22
Ricaurte Camila Armirola (PN02) S52
Richard Isabelle (DC02) S28
Riddell Dominique O. (D13) S25
Riguzzi Pietro (DC01) S28, (DC06) S31
Rinaldi Carlo (DCC08) S68
Rivas Eloy (‡OD07) S61
Robert D (MD08) S43
Roberts Mark E. (‡OD07) S61
Robertson Thomas (D04) S19
Robinson E (DC13) S35
Robinson Emma (DC12) S35
Robinson Emma-Jayne (DC01) S28
Robledo Diego (‡PN05) S55
Rodesch Matt (DCC04) S65
Rojas J (DC13) S35
Romano Adelina (‡MD10) S44, (MD08) S43
Roos Andreas (‡OD08) S62, (S09) S6
Rossi Rachele (D14) S25
Rossor Alex M (‡DCC09) S68
Rossor Alexander (PN01) S51
Rossor Alexander M (PN04) S54
Rossor Alexander M. (PN02) S52, (PN09) S57
Roussel Marie-Pier (‡DC04) S30
Rozanska Agata (OD04) S60
Rudolph K (DC13) S35
Rufibach L (DC13) S35
Rufibach Laura E. (DC03) S29
Russell AJ (‡DC16) S37
Russell Oliver (MD06) S42
Ryan Catherine (DCC08) S68
Ryan Gavin (OD03) S59
Ryan-Phillips Finlay (NMJ&C03) S14
Ryburn Liz (MND03) S9
Ryten Mina (DCC08) S68
Sacconi Sabrina (DC15) S36
Saha Asmita (D12) S24
Salisbury Sarah (‡PN05) S55
Salman Doaa (DC01) S28
Samanta Rajib (OD03) S59
Sandona Dorianna (DC02) S28
Sansen Stefaan (DCC04) S65
Sansone Valeria (DC15) S36
Sarkozy Anna (DC17) S38, (DCC03) S64, (DCC07) S67
Savarese Marco (DCC07) S67
Scardamaglia Annarita (PN02) S52
Schänzer Anne (‡OD08) S62
Schüle Rebecca (S05) S5
Schara-Schmidt Ulrike (‡OD08) S62
Schiava Marianela (DC01) S28, (DC14) S36
Schnekenberg Ricardo (PN08) S56
Schnekenberg Ricardo P (D04) S19
Schnekenberg Ricardo P. (PN02) S52
Schnekenberg Ricardo Parolin (‡DCC02) S64
Schofield Alex (DC17) S38
Schofield Ian (MND01) S8
Schon Katherine (MD03) S40
Schon Katherine R (‡MD19) S50
Schon Kathrine (‡MD10) S44, (MD08) S43
Scodellaro Riccardo (‡D06) S21
Scotchman Elizabeth (MD11) S45, (MD18) S49
Scoto Mariacristina (MND03) S9, (MND07) S11
Scott Emma (NMJ&C05) S15
Scriba Carolin K (D04) S19
Selvatici Rita (DCC04) S65
Sen Anando (DC07) S32
Servais Laurent (S04) S4
Sevilla Teresa (PN02) S52
Sewry C. (DCC01) S62
Sewry Caroline (‡OD08) S62
Shah Sachit (‡DCC09) S68
Sheehan Jennie (DC17) S38
Sheikh Danish (D01) S17
Shi Sinan (‡MD19) S50
Shieh Perry (DC15) S36
Shin Jin-Hong (DC03) S29
Shy Michael E (PN03) S53
Skorupinska Iwona (‡NMJ&C07) S16, (DC15) S36
Skorupinska Mariola (‡DCC09) S68, (PN02) S52, (PN03) S53, (PN09) S57
Slipsager AW (‡DC16) S37
Smeitink J (MD16) S48
Smeland Marie F. (OD03) S59
Sohn S. (D05) S20, (D09) S24
Specterman Mark (MND02) S9
Spillane J (OD02) S58
Stahl Jan-Hendrik (PN02) S52
Statland Jeff (DC15) S36
Steele-Stallard Heather (‡DC10) S33
Stemmerik MPG (‡DC16) S37
Stevanovski Igor (D04) S19
Stojkovic Tanya (D04) S19, (DC03) S29, (PN01) S51, (S11) S7
Storey Elsdon (D04) S19
Straub V (DC13) S35
Straub Volker (D04) S19, (D12) S24, (DC01) S28, (DC03) S29, (DC05) S30, (DC06) S31, (DC08) S32, (DC09) S33, (DC14) S36, (DCC05) S66, (MND01) S8
Sudarsanam Annapurna (OD03) S59
Sudhakar Sniya (DC17) S38
Sukenik-Halevy Rivka (‡OD08) S62
Sultan Tipu (PN02) S52
Suomi Fumi (OD03) S59, (OD04) S60
Szabo Marton (MD05) S41
Töpf Ana (DC01) S28, (DCC05) S66, (DCC07) S67
Talim Beril (DC02) S28
Tankard Rick (D04) S19
Tanner Stephanie (DC01) S28, (MND05) S10, (MND06) S11
Tanzi Rosa (MND02) S9
Tasca Giorgio (‡OD07) S61, (D12) S24, (DC01) S28, (DC02) S28, (DC12) S35, (DC14) S36
Tawil Rabi (DC15) S36
Taylor Lucie S. (MD09) S44
Taylor Robert W (‡MD10) S44, (MD08) S43, (‡MD13) S46, (MD09) S44, (OD03) S59, (OD04) S60
Tedesco Francesco Saverio (‡D16) S27, (‡DC10) S33, (D02) S18
Tejedera-Villafranca Ainoa (‡D07) S21
Tekgul Seyma (PN02) S52
Tetorou Konstantina (D14) S25
Thomas Anisha (MND05) S10, (MND06) S11
Thomas Naomi (MD17) S49
Thompson Kyle (‡MD13) S46
Thorman Portia (MND03) S9
Thornton John S (‡DCC09) S68, (‡MD15) S48
Thornton John S. (S13) S7
Tomaselli Pedro José (PN02) S52
Topaloglu Haluk (PN02) S52
Torres-Masjoan L. (D15) S26
Torron Roberto Fernandez (DC03) S29
Torun Tugce (‡D16) S27
Toscano Antonio (‡OD07) S61
Tropman D. (‡PN07) S56
Tsz Cherry (‡DC10) S33
Tucci Arianna (D04) S19
Turchetti Valentina (PN02) S52
Turnbull D. M. (MD07) S42
Turner Cathy (DC09) S33
Ubiali Anna (DC15) S36
Urquhart Lexie (‡MND04) S10
Valiente Lidia Matias (D03) S19
Van de Vondel Liedewei (PN02) S52
Vanegas Maria (DC17) S38, (NMJ&C04) S14
Vasudevan Pradeep (OD03) S59
Vegezzi Elisa (D04) S19, (PN01) S51
Verdu-Diaz J (DC17) S38
Verdu-Diaz Jose (D08) S22, (MND05) S10, (MND06) S11
Villalobos Elisa (‡D07) S21, (D08) S22, (D11) S24, (D17) S27
Villegas Elisa Villalobos (D03) S19
Vincent A. E. (MD07) S42
Vincent Amy E. (‡DC04) S30
Visser Marianne de (DCC05) S66
Vissing J (‡DC16) S37
Vissing John (DC03) S29
Vivekanandam Vinojini (‡NMJ&C07) S16
Voermans Nicol C. (DC07) S32
Volker S (DC17) S38
Vucic Steve (D04) S19
W.M Roper (DC13) S35
W.Taylor Robert (OD01) S57
Wagner Kathryn (DC15) S36
Wagner Matias (‡OD08) S62
Waldock Pete (DC12) S35
Waldock Peter (DC01) S28
Walker Helen (DC08) S32
Walker Michaela (DC15) S36
Walker Suzie (‡MD10) S44, (MD08) S43
Waller Katie (‡MD10) S44, (MD08) S43
Walsh Cheryl (DCC03) S64
Walsh Julie (DC01) S28
Wang Leo H. (DC15) S36
Ward Erin (DC07) S32
Ward Mark (DC07) S32
Warren C. (MD07) S42
Warren Daniel (OD03) S59
Wastling Stephen (‡DCC09) S68
Webber J (DC13) S35
Webster Richard (NMJ&C02) S13, (NMJ&C08) S16
Weihl Conrad (DC02) S28
Weis Joachim (‡OD08) S62
Weisburd Ben (D04) S19
Wells Dominic J. (D13) S25
Wenninger Stephan (DC02) S28
White Chelsea R. (‡MD13) S46
Whittaker Roger G. (MND01) S8
Whittle Ella F (DCC08) S68
Williams J (MD14) S47
Williams Jessica (MD11) S45, (MD18) S49
Wilson Abigail D. (PN02) S52
Wilson Ian (MND01) S8
Wilson Lindsay (PN02) S52
Wilson Louise C (‡OD08) S62
Winkelmann Juliane (‡OD08) S62
Winter Monika (‡MD10) S44
Wittig Ilka (‡MD13) S46, (MD09) S44
Wolfe Amy (DC17) S38
Wong Karen (DC01) S28
Wong Yan (‡DC10) S33
Wood Marie (DC07) S32
Wood Matthew (‡D16) S27
Woodward C (MD14) S47
Woodward Cathy (MD11) S45, (MD12) S46, (MD18) S49
Woodward Cathy E (PN04) S54
Yépez Vicente (DCC05) S66
Y.S Ng (MD16) S48
Yang Ji-Ming (‡MD19) S50
Yepez Vicente A. (DCC07) S67
Yochai C (DC13) S35
Yoshimura Madoka (DC03) S29
Yousry Tarek (‡DCC09) S68, (PN01) S51
Yu Patrick (MD03) S40
Yue Wyatt W. (OD03) S59
Yung Rhianna (MD05) S41
Züchner Stephan (PN02) S52
Zafeiropoulos Nick (‡DCC09) S68
Zaman Mashaya (PN02) S52
Zammit Peter (‡DC10) S33
Zancolli Marta (DC05) S30
Zanovello Matteo (PN04) S54
Zetterberg Henrik (PN01) S51
Zhelcheska Kristina (PN02) S52
Zhou H. (D15) S26
Zhou Haiyan (DCC08) S68
Zifarelli Giovanni (PN02) S52
Zuccolo Michela (DCC04) S65
Zygmunt Aldona (DCC04) S65
de Antonio Ferrer Marta (DC02) S28
van den Ameele Jelle (MD03) S40, (MD20) S51
van der Kooi Anneke (DCC05) S66


