
Abstract
Background:
Telemedicine, the application of those information technologies to remotely provide health services either for synchronously catching or asynchronous monitoring patient medical data, has shown a growing and widespread application in several chronic diseases, and, especially during and after COVID-19 pandemics, also in neuromuscular diseases.
Objective:
this review aims at providing an updated overview on the application of telemedicine and telemonitoring tools in neuromuscular diseases, in clinical practice, research and trials.
Methods:
a literature search was conducted on PubMed using keywords regarding telemedicine applications and several neuromuscular diseases, including papers up to May 2024.
Conclusions:
several tools have been developed and tested in myopathies, motoneuron diseases, myasthenia gravis and peripheral neuropathies, providing monitoring, assistance, and rehabilitation protocols for such frail population, for which obtaining real life data remotely can represent a concrete advantage in clinical trials and clinical practice. Although several barriers in the implementation of telemedicine in NMD still need to be overcome, there is evidence for both clinicians and patients showing positive acceptance and satisfaction on the use of remote supports, regarding them as confident outcome measures of quality of life in view of a more general concept of e-health solutions in routine medical care.
Introduction
In the last years, the need to provide patients with a more precise, personalized, predictive and preventive medicine has prompted the development and application of novel technological approaches to the medical setting.1,2
In this context, the emerging concept of “decentralized healthcare” to empower data collection and analysis and patients’ engagement for both clinical practice and trials, is currently increasingly considered. 3 In fact, several tools are available – ranging from wearable devices, smartphones, ambient sensors, smartwatches – to collect remotely real-life data, to complement and potentially provide alternative sources to the classical clinic assessments.
However, the theoretical possibility to collect large amounts of digitally acquired data warrants considerations about safety of tools, data protection, interoperability, and clinical significance, among others. Two main frameworks are involved and should be distinguished: while the term “telemedicine” describes the application of electronic technologies to provide health services remotely but synchronously (and has a more common and long-lived application in clinical practice, if we consider that telephonic consultation represents a telemedicine approach), “remote monitoring” entails to gather and analyse patient's data outside the clinical setting, therefore also asynchronously. Combining telemedicine and remote monitoring could integrate in-person interactions, enhance the acquisition of second opinions by experts in the field, support decisional diagnostic and treating algorithms and boost data analysis. 4
The field of neuromuscular diseases (NMDs), which are represented by a broad group of rare disorders, often phenotypically heterogeneous and with incomplete knowledge of their pathophysiological mechanisms, equally poses significant challenges and a potentially fertile ground to a similar approach. The application of tele-health systems could help fill the knowledge voids and provide outcome measures for clinical trials, but their use must undergo a validation process and careful evaluation of the clinical significance of the finely collected data. 5
Certainly, the COVID-19 pandemics has redesigned and implemented provision and use of telemedicine also in NMDs. A survey by the European Network for Rare Diseases on Neuromuscular Diseases (ERN-NMD) 6 reported that among 42 responders on 76 Health Care Providers in Europe, teleconsultations and consultations by phone were the most common type of telemedicine contact, especially in patients with COVID-19 infection who experienced a worsening of symptoms. However telemedicine is still considered a support rather than an alternative to the traditional face-to-face medicine.6,7
In addition, an independent analysis on the state of the art conducted by Healthcare Information and Management System Society (HIMSS) on the use of Electronic Medical Record Adoption Model (EMRAM) across hospitals in Europe, revealed that the achievement of an adequate level of digital maturity, in terms of security, electronic sources, data analytics and clinical decision support, is still far from reached. 8 The main objective of this review is to assess the state of the art on the application and impact of telemedicine and remote assessment in NMDs. We also discuss adequacy, limitations, and feasibility of digital health interventions.
Materials and methods
A literature search on PubMed was performed using the following keywords: “telemedicine” or “telemonitoring” combined with “neuromuscular diseases,” “myopathies”, “Duchenne muscular dystrophy”, “myotonic dystrophy”, “Pompe disease”, “spinal muscle atrophy”, “facioscapulohumeral dystrophy”, “myasthenia gravis”, “amyotrophic lateral sclerosis,” and “peripheral neuropathies.” We included papers up to May 2024. Research and review papers in English language were considered.
Results
Myopathies
The repercussions of telemonitoring the clinical course of patients affected by muscular diseases is intuitive, considering the extreme phenotypic variability which they can express, their progressive course over time and the occurrence of detrimental events, such as respiratory or cardiac complications, which can change the disease's trajectory.
In such clinical conditions, providing objective, frequent and real-life assessments data offer the possibility to guide care in a more precise manner. The usefulness of telecare systems in providing accurate and reliable data and empowering management of NMD patients has been yet exploited in the relatively recent past, bringing out its great potential to intercept slight clinical changes which can imply or predict clinical deterioration or exacerbation.9,10 A telemetric system for the measurement of cardiorespiratory variables (oxygen saturation, heart rate, blood pressure and electrocardiogram) was implemented to monitor, over a period of 5 years, 3 NMD patients with chronic respiratory failure requiring long-term mechanical ventilation. The system was effective in significant reduction of hospital admissions of the patients and consequently high satisfaction by both patients and medical staff, also for the user-friendly interface of the system. 9
Duchenne Muscular Dystrophy (DMD)
A critical determinant of quality and length of life for DMD patients is respiratory function, which has greatly benefited from steroid therapy in the last 20 years 11 but remains one of the core clinical aspects to follow-up. A control-case, open-label study reported the effects of daily monitoring for a period of 3-months performed by home based remote electronic spirometer, networked with a software platform. In addition, the study included 3 in-hospital visits (V1 at enrolment, V2 after 4 weeks and V3 at the end of the study at 12 weeks). 12 Interestingly, 15 boys on 21 included, aged 7–22, performed the home-based measurements (forced vital capacity-FVC, forced expiratory volume in 1 s-FEV1, peak expiratory flow-PEF and maximal inspiratory-MIP and expiratory pressures-MEP for respiratory muscle strength) correctly, confirming previous data. 12 On 1403 traces registered, no differences were found compared with the results obtained with the out-patient clinical setting spirometry done at baseline and after three months of telemonitoring. The aim of the study was also to evaluate patients’ satisfaction and subjective benefits or problems related to the home measurements through a specific survey questionnaire administered at V2 and V3, which reported high general satisfaction levels and, as the most important benefit, subjective feeling of breathing improvement.
Another paramount (but only partially met) need of DMD patients and families is rehabilitation. 13 In the last years, the provision of rehabilitation services has been in many cases adapted to changes imposed by COVID-19 pandemic and new technological equipment has been available. 13 After a survey to map the delivery of rehabilitation services for DMD patients referred to a TREAT-NMD Clinical Center in Poland, 13 an online rehabilitation and motor functional assessment program was designed both for ambulant and not ambulant DMD patients, investigating on their preferences and expectations on different services delivery, in particular online workshops, videos with exercise instructions or individual online consultations.
In another single-blind study 14 19 patients were randomized in two groups comparing, in a rehabilitation program during 8 weeks, three times per week, live telerehabilitation sessions versus pre-recorded video-exercises sessions. One group participated to live-physiotherapist guided sessions, while the other performed the same low-moderate intensity aerobic exercises according to the instructions suggested by streaming videos, without any feedback by physiotherapist. A blind rater performed face-to-face assessment visits recording at inclusion and after the study with functional motor evaluation). Only in the first group patients showed a global improvement in muscle strength both on proximal and distal muscle districts, however not matching with global functional improvements or reduction in caregivers burden measured by Caregiver Burden scale.
Differently from the results reported by Sobierajska-Rek et al. 13 live telerehabilitation program was preferred for a greater engagement of caregivers and patients who received positive reinforcement in training by physiotherapist allowed a systematic scheduling of the appointments. However, the Authors commented that a comparison in terms of outcomes and effectiveness was not conclusive to discern which was the best approach, also pointing out some methodological limits, such as the absence of monitoring of cardiorespiratory variables. 14 Very recently, a remote live stream video evaluation of the NSAA was tested through real time via a web meeting with the patients, caregivers, and physiotherapist, demonstrating high levels of concordance with in-person evaluation. 15 The study was conducted in the framework of COVID-19 driven modified policies for assessment of patients enrolled in delandistrogene moxeparvovec clinical trials.
Facioscapulohumeral Muscular Dystrophy (FSHD)
Despite FSHD representing one of the most common muscular dystrophies, hardly any specific experience is reported in literature for the use of telemedicine supports. Portaro and colleagues 16 tested a 6-month telemonitoring follow-up period in four siblings affected by a severe form of FSHD, living in a rural area far away from the referral centre for NMD. The telemedicine support consisted of multidisciplinary video conferencing and at-distance monitoring of cardiorespiratory variables by pulse oximeters and an aneroid sphygmomanometer. The system architecture consisted of a Control Center, an Application Server, and a Database Manager located at the Hospital Center.
The monitoring timing was tailored on clinical needs. In addition, a protocol of Cardiorespiratory Rehabilitation through commercial Virtual Reality Rehabilitation System applying biofeedback exercises was tested. In general, patients and caregivers appreciated the feasibility of the system, with mild impact on quality of life assessed by SF-36. Also in this case, in line with results reported by Zamarron et al., 9 during the follow-up period no hospital access was necessary and, in case of respiratory symptoms exacerbations due to infectious disease, required pharmacological therapy was managed successfully at distance. 16
In a recent COVID-19 Impact Survey 17 to assess effects of the pandemic on social aspects and medical care in muscle diseases patients, on 1243 responders (including 49% affected by FSHD), residing worldwide and mean age 52.5 years, 61% participated in a telemedicine appointment via telephone calls or video conferencing platforms with great satisfaction; in some cases, technical difficulties were underlined. However, 64.4% of patients who experienced both in-person and telemedicine services preferred in-person visits. This data is globally in line with what previously reported in a similar survey administered to 774 patients affected by muscle diseases (56% FSHD) living in the United States between May 8, 2020, and May 28, 2020. Also in this case the adaptation and satisfaction from the use of telemedicine supports was very high, also considering that the survey ranged in a relatively early pandemic period, nevertheless only 10% of individuals preferred the virtual assessments. 18
Dystrophic and non-dystrophic myotonias
This group of diseases offer a variety of parameters to be periodically assessed and that can be susceptible of clinical benefit from medical therapy. In general, muscular weakness (distal or proximal) can be present, along with cardiological impairment (mainly in terms of arrhythmic disturbances), respiratory involvement, dysarthria and dysphagia, behavioural disorders (in the case of Myotonic Dystrophy type 1) and myotonia, localized at hands, tongue and other variable muscles depending on the specific type of disease. 19 Nonetheless, experience with these disorders is limited. In 2017 Portaro et al. tested 10 patients affected by Non-Dystrophic Myotonias (NDM) and 10 patients with Dystrophic Myotonias (DM), using a sensor-engineered glove (SEG) to assess myotonia. The authors evaluated the time required to perform a complete finger extension (grip myotonia time, GMT) at maximum velocity (MV) after maximum v20oluntary contraction (MVC) in different settings including rest, exercise, and ice effects on handgrip myotonia; the system was found to be sensitive and reliable and is proposed by the authors as a tool to evaluate myotonia also in clinical trials. 20 Hamel et al. 21 studied a more global telemonitoring approach on twenty-three subjects with DM1 using a tablet equipped with a software for videoconferencing and questionnaires, grip dynamometer, and spirometer. Grip strength forced vital capacity, peak cough flow, timed-up-and-go (TUG), and hand opening time (HOT) were determined during remote assessments. In their cohort, the authors report a high level of completion of the study, and moderate to strong correlations between the grip strength and TUG with self-reported inventories.
Pompe disease
In Pompe disease (PD) no significant experience in telemedicine applications was retrieved in our search. In 2018 Ricci et al. 22 developed the mobile app AIG-kit to help adult patients with PD in managing illness-related factors (diet, physical exercise, physiological parameters), also allowing clinicians a continuous tracking of patients in real-time and ambient conditions of everyday life.
Inflammatory myopathies
Paucity of data exists regarding the use of device-based objective measures or other tools for monitoring patients affected by inflammatory myopathies. Naveen et al. validated the use of two novel task-based, patient-centred outcome measures (PCOMs), namely ten times arm lift (AL) test and two-minute walk distance (2MWD) 23 in a cross-sectional observational in-clinic and telemetric study on 22 adult patients (aged 19–65 years, 68% females) with active or inactive idiopathic inflammatory myopathies (IIM). For AL test, patients were asked to abduct their arms parallel overhead ten times as fast as possible, followed by bringing the arms out to the side. The task was repeated three times, and a timer recorded the seconds needed to complete the task. For the 2MWD, the patients were asked to walk as fast as possible for 35 m back and forth on a prescribed line; the total number of rounds was indicative of the total distance covered in 2 min. Both tests showed very high test-retest reliability but while AL time significantly discriminated between active and inactive disease states, 2MWD presented very high variability to be considered a reliable outcome test. More in general, a previous experience of consultation by voice-call during COVID-19 pandemic in follow-up of 250 patients with adult and juvenile IIM confirmed the usefulness of telemedicine to diagnose and manage relapses in IIM. 24
Spinal Muscular Atrophy (SMA)
SMA in its different clinical forms varies in presentation and severity. 25 Across the lifespan of SMA patients, capability in capturing objective and meaningful information regarding motor performances and physiological variables is fundamental to better intercept the grade of their frailty susceptibility. Also considering the new available therapeutic strategies, the development of remote assessments both for clinical care and research purposes may be important to improve clinical outcome assessments by continuous monitoring also during every-day life. In this view, the properties of Pediatric Evaluation of Disability Inventory-Computer Adaptive Test (PEDI-CAT) Daily Activities and Mobility domains tool have been tested in a sample of children and adolescents with SMA. 26 PEDI-CAT includes performance-based tests, already validated for children with developmental disabilities, which provide information about daily activities and motor function in daily environments. 27 Fragala-Pinkham et al. 26 realised a prospective cross-sectional multi centric study instructing parents or caregivers to complete by PEDI-CAT software the reporting measures of the current level of functioning. Overall, 96 patients were included and classified according to their motor skills in non-sitters, sitters, and walkers; in general, a high level of autonomy in administration was revealed, as 85% of tests were completed by parents in a few minutes. Good cross-sectional validity of PEDI-CAT platform in identifying significant differences in daily activities and mobility domains across different SMA types, according to motor subgroup classification done, was noticed. In total, 85 participants had limitations in Mobility and 51 in Daily Activities; these results reflect the natural clinical course of SMA.
In 2016, a Rasch-analysis confirmed the suitability of PEDI-CAT on 58 children and young adults with SMA, although, especially for mobility skills, it was most informative for Type III SMA than Types I and II, and it was not sufficiently sensitive to detect small strength changes over time. 28 In Italy, a national NMD registry was structured as a flexible technological interface which can be updated on demand, being part of the TREAT-NMD Global Registry, interoperable both for patients and clinicians, which allows to share aggregated data for feasibility enquiries by pharmaceutical companies, identify patients suitable to participate in clinical trials and contribute to epidemiological and observational studies. 29 In 2017 in the United States the SMA Clinical Trial Readiness Program to enhance trial readiness development was launched. Cure SMA Clinical Trial Readiness Program included operative phases in which one pillar of its sustainability was represented by implementation of virtual activities both in research and in care networks organization. 30 Recently, Peterson et al. used the Cure SMA registry to assess on a large cohort of US SMA patients their experience with telemedicine; their study was conducted on 463 individuals, of which the majority had already used telemedicine (increasingly in case of male gender, increasing income, having received drug treatment for SMA). 30
Myasthenia Gravis (MG)
Myasthenia gravis (MG) is the most common autoimmune disorder affecting the neuromuscular junction, characterized by skeletal muscle weakness and fatigability. Patients can experience symptoms exacerbation requiring fast access to hospital and needing a close follow-up based on internationally accepted clinical scores or patient-reported outcome measures. 31
Thus, in MG some efforts to digitalize clinical follow-up to better define the disease course has been done, starting from simple tools such as telephonic interviews or video-calls, during which simple semeiotic manoeuvres should be arranged to investigate the signs of fatigability related to the disease. Kukulka et al. 32 conducted a retrospective, single-center review of a pilot study in which the viability of nurse-administered single breath count test (SBCT) peformed during a phone call was proven to predict clinical exacerbation in patients with MG who contacted the referral clinic for worsening of symptoms.
On a total of 45 telephone contacts (median patients age ranged 16–75 years and disease duration was less than 4 years), 25 patients had a breath count of 25 or less and were addressed to the Emergency Department. The telephonic SBCT triage had a positive predictive value of 71%, sensitivity of 80%, and specificity of 60% in diagnosing an MG exacerbation. The study however shows some limitations such as the limited sample size or the possibility of false negatives, i.e., in case of involvement of different skeletal muscles other than respiratory ones. Among bulbar symptoms, swallowing function could be insidious to be evaluated remotely. In 2021 Guidon et al. published an expert guidance including the recommendations for Myasthenia Gravis Core Exam (MG-CE) by televisit. 33 The digital assessment of swallowing in neurological disorders has been approached as early as1996. 34 The Swallowing Monitoring and Assessment System (SMAS), consists of an ultrasound Doppler sensor array, a microphone, and an inertial measurement unit to measure ultrasound signals originating only from swallowing activities. Tested for combinations of two viscosity conditions (water and yogurt) and two volume conditions on 24 healthy participants, it demonstrated to be a non-invasive and quantitative tool which in perspective could be applied in disease conditions. 35
The fluctuating nature of MG with high susceptibility to exacerbations due to exposure to viral or bacterial infections, has imposed during COVID-19 pandemic the implementation of telemedicine services. Avoiding unnecessary in presence consultations and acceptance and guidance for decision-making processes has been shared by Scientific Societies, as American Academy of Neurology (AAN), which provides proper coding elements to dispense these services appropriately. 36
However, in absence of a validated specific tool for telemedicine in MG, Pasqualin and Colleagues developed and validated the Myasthenia Gravis TeleScore (MGTS) which explores ocular, bulbar. respiratory districts and global muscle strength. 37
One hundred thirty-one patients were assessed by means of MGTS and INCB-MG scale selected as reference according to a blind design. First one physician conducted a follow-up visit in presence and collected the INCB-MG evaluation, soon after a MGTS score was completed by another physician in a televisit modality using a commercial app of video-communication service. A very strong correlation between the two scores was found in every subgroup of patients (ocular, generalized early-onset, generalized late-onset, anti-MUSK positive, seronegative and thymoma associated). Intuitively, correlation was lower between items with different evaluation modality (anamnestic vs clinical) and based on muscle fatigability, in consideration of the different posture and physical effort adopted – as the evaluator is not in presence. No data is available regarding the capability of MGTS to detect minimal change over time of clinical course in a single patient. However, even if sample size was limited, validity and reliability of the scale was found to be very high.
Amyotrophic Lateral Sclerosis (ALS)
ALS is a devastating disease with usually rapid progression, leading to complications in multiple domains and to a progressive deterioration and loss of motor functions. For that reason, ALS represents a complex disease model for which the application of telemedicine solutions has been tested. Indeed, telemedicine was usually well accepted,38,39 especially during COVID-19 pandemics, 40 as it does not require patients to travel, and, in comparison with standard in site visit, it is usually cheaper and faster. Although not leaving the house and the lack of personal touch can be seen as a disadvantage for some patients – which are often confined at home and consider the visit as an occasion to move around and meet new people – the trip, the possible overnight stay nearby the centre and the waiting until the visit are felt as a significant burden by patients and caregivers. 40 Selkirk et al. reported that telemedicine was non-inferior regarding quality of care and outcomes in patients affected with ALS. 41 Recently, Garcia-Gancedo et al. 42 reported a pilot observational study regarding remote assessment by means of a commercially available product composed of an accelerometer and a 2-lead ECG and a high-fidelity microphone for the analysis of speech; their pilot results on 25 patients with ALS demonstrated that the system was generally well tolerated and adequate to evaluate worsening in activity of daily living. Telemedicine could also contribute to improving the overall health of patients: Pinto et al. demonstrated that a weekly telemonitoring of non-invasive ventilation (NIV) settings and NIV. compliance significantly reduced hospitalizations compared to the standard of care (i.e., assessment on admission, 2–3 weeks later and after 3 months). 43 In 2023 44 Reginault et al. compared the outcomes of at-home and telemonitored initiation of NIV with in-hospital in a retrospective study on 265 ALS patients; the authors demonstrated better results compared to the in-hospital one in terms of adherence, a good nocturnal hypoxemia correction rate and lower medium delay in NIV prescription. Wills et al., in a randomised study, showed that the decline in ALS Functional Rating Scale Revised (ALSFRS-R) was slower in patients who received tailored nutrition recommendations and recorded their weight and dietary intake twice a week in an ad hoc developed mobile application, compared to those receiving standard of care (i.e., in person nutritional advice once per month). 45 As to evaluation of respiratory function and cough impairment, in 2023 Recasens et al. 46 explored the use of a smartphone app to estimate Cough Peak Flow (CPF) based on cough sounds in a cohort of 50 individuals with neuromuscular disorders, including ALS (kore than half of subjects), MG and myopathies. The tool demonstrated high sensitivity and specificity in identifying CPF impairment also in subjects with oro-facial weakness, which may alter the evaluation. Another study on bulbar function 47 tested a remote deep learning-based system to acquire audio tracks of bulbar-onset ALS patients and healthy control subjects while performing the oral diadochokinesis (DDK) test on 32 healthy control subjects and 11 bulbar-onset ALS via a web app (Homely Care). The study represents a step forward compared to previous experiences in ALS, reporting high accuracy also in the home setting; however, limitation of the study were the limited number of subjects and the low performance in severely impaired patients (which, although, could not be the ideal target population to apply the system on). The same group used Homely Care as a cloud-based storage system for another convolutional neural network (CNN) approach evaluating visual facial landmarks in ALS patients to detect dysarthria. 48 Very recently, Straczkiewicz et al. compared the sensitivity of accelerometers placed on wrists of patients in comparison with the ALSFRS-RSE and reported that the accelerometers’ results changed at a statistically significant rate change over time, and were more rapidly changing compared to survey responses. 49 Another study 50 demonstrated hip accelerometers ability to predict disease progression in a cohort of 97 patients during a prolonged observation. Interestingly, another recent study involving patients with ALS but also other neuromuscular conditions as genetic neuropathies and muscular dystrophies, evaluated the application of the wearable cyborg Hybrid Assistive Limb (HAL), a therapeutic exoskeletal device designed to provide voluntary gait assistance using kinematic/kinetic gait data and bioelectrical signals. 51 The Authors describe it as a powerful tool for data collection, capable of differentiate several clinical conditions and to be used for evaluations during clinical trials.
Peripheral neuropathies
Several forms of peripheral neuropathies (PNs) share quite similar clinical aspects with motor and/or sensory impairment. 52
As in other NMDs, also in PNs the application of telecare is limited by the need of a direct inspection of patients signs not otherwise verifiable, such as reflexes elicitation or testing sensation. 53 Wilson et al. reported the development and pilot testing of the Veterans Affairs Neuropathy Scale (VANS) for remote assessment of PNs. After the selection of several neuropathy exam scales based on literature-reported sensitivity and specificity, a set of tests was included to define VANS which evaluated sensory impairment. Globally, 28 patients affected by varying degrees of PN underwent VANS testing under 5 scenarios which differed by mode of VANS grading (in-person vs. telemedicine) and by the in-person examiner type (neurologist vs. technician under instructions received by a neurologist) in telemedicine scenario. Acceptable concordance and reliability of the VANS in telemedicine with in-person examinations, as well as feasibility in its application, was found. 54
Another randomized trial by Kolb et Colleagues evaluated the possibility of telemonitoring patients with peripheral neuropathies due to chemotherapy treatments and opened interesting speculations on the argument. Authors implemented a telephone-based, automated, symptom-monitoring system that recorded patient-reported neuropathic symptom severity, distress, and activity interference on a 0–10 scale. Patients were instructed to dial the system daily to report numbness and tingling. For patients assigned in the interventional group, an automated system delivered self-care strategies based on the specific symptom and severity while a trained nurse was automatically alerted and the patient were recalled in the next few days to discuss further pain management strategies; for patient in the observational group, the system referred to the oncology teams for any symptoms reported. Authors reported that this telemedicine approach was efficient in reducing days with neuropathic symptoms of any severity and fewer days of any distress. Curiously, although more than 10% of patients in control group reported moderate-to-severe symptoms, no one called the oncology team; while authors do not comment this data, this finding should be further clarified in order to understand this phenomenon. 55
In addition, regular monitoring of PNs patients can improve care outcome, such as lowering the use of opioids for pain control in some cases or falls’ rate reduction 56 As reported by Bohnert et al., 57 however, especially in older cohorts as the diabetic peripheral neuropathy one, technological equipment and education must be addressed before telemedicine becomes a feasible option in clinical care, towards which although patients are favourably disposed.
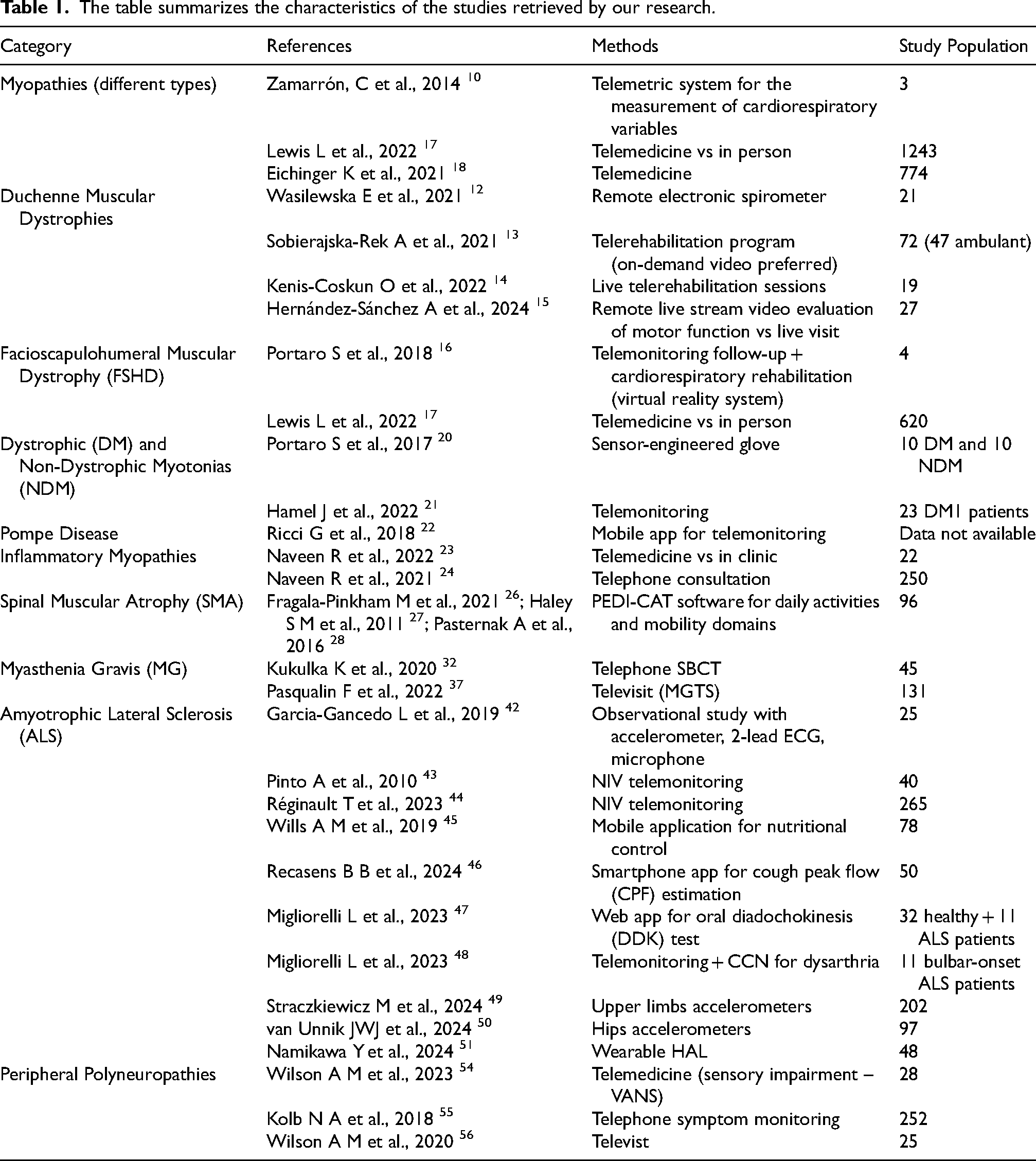
All the studies retrieved by our search are summarized in Table 1.
The table summarizes the characteristics of the studies retrieved by our research.
Discussion
Undoubtably, telemedicine will have a growing application in many clinical settings including NMDs. However, its concrete implications will be determined by several clinical, technical, human, and social issues. First, it may be helpful to understand which patients are optimal candidates for telemedicine consultations. Despite the extreme variability in etiological and pathological terms of the several pathologies, several NMDs share a quite common clinical course with a chronic, progressive evolution in which incidental detrimental events as infections, traumas, and others, at different extent, can change disease trajectory, prompting the need for rapid recognition and timely therapeutic decisions. This consideration requires to expand our knowledge both of strengths and limitations of telemedicine interventions in NMDs. On one side, we have performing technological tools for a continuous objective monitoring of some clinical parameters of interest, useful to better guide care and manage these vulnerable patients and on which healthcare policy is increasingly reliant, for its potential benefit in defining priority settings of action and reducing in-hospital procedures (and related costs). On the other side, the experience acquired in NMDs is still quite poor, and some clinical issues require necessarily in-person clinician-patient interaction, to capture clinical signs not fully explorable by televisit. A critical point is the lack of “standard procedures” or well-known practices for these methods.
From a technical point of view, many types of sensors (e.g., near-body or far-body sensors for noninvasive measurement of heart rate, SpO2, blood pressure, body temperature, digestive gastric activity, etc.) that have been already developed and validated in-lab, are potentially very useful in NMDs. Nonetheless, they never progress from the lowest Technology Readiness Levels (TRL) (e.g., TRL 4: Laboratory-validated technology) to the highest ones (e.g., TRL 8: Comprehensive and qualified system), with serious detriment to the health and quality of life of many NMD patients. The factors driving this situation are many and complex, but researchers and policy makers should seriously discuss about more effective technology transfer strategies by integrating medical expertise, technological skills, unmet patient needs, and marketing opportunities.
In addition, more in general, the terms “telemedicine” and “telemonitoring” were used before COVID-19 almost only in a technical sense (i.e., usage of telecommunication devices for performing remote monitoring or medical activities). After the three waves of COVID-19, however, in many European countries, the terms telemedicine and telemonitoring often refer to regulated services admitted as reimbursable benefits. These two meanings are very different, and the differences must be considered when planning their implementation in clinical practice.
Further methodologically rigorous studies, searching for suitable short and long-term outcome measures taking advantage of telemedicine approaches are needed to strengthen the use of these tools both in clinical trials and practice.
Conclusions
While in recent years evidence supporting the importance of telemedicine in several neurological diseases has been produced, its role in managing NMDs patients has not been extensively explored. In general, both clinicians and patients have shown acceptance, confidence, and satisfaction on the use of telemedicine support. This last aspect has been further emphasized by Covid pandemics during which, inevitably, the old conception of healthcare has been disrupted and radical shifts in delivery digitalized models have been created, also in NMDs field. Quality and reliability of outcomes reported in several studies push towards the development of evidence-based insights for the integration of e-health solutions in routine medical care, whereas several barriers need to be overcome. Last, but not least, social determinants in challenges related to weak policy for the implementation of an equitably digital health should be considered. Although generally taking advantage of simple and largely available tools, limiting factors for its widespread use can be found in digital poverty in terms of financial conditions, privacy policies and digital education, which can restrict the access to the digital services, slowing the progress in this direction.
In conclusion, policies of digital inclusion in routinary clinical practice and research could enhance the services outcome indexes in terms of acceptability, accessibility, usability, both for patients, caregivers, and clinical staff in NMDs, but wider standardized studies are needed.
Footnotes
Acknowledgments
G.S., G.R., E.S. and F.T. are members of the European Reference Network for Neuromuscular Diseases – Project ID No 870177.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.