
Abstract
Objective:
Wheelchair users with neuromuscular disorders have symptoms related to the disease and complications to the sedentary lifestyle, such as constipation and lower back pain. Physical training might be beneficial. This systematic review investigates the potential benefits and harms of physical training for wheelchair users with neuromuscular disorders.
Methods:
We systematically searched PubMed including studies published until July 2024. Inclusion criteria: 1) participants with a neuromuscular disorder, 2) at least 60% of participants in a study were wheelchair users, 3) physical training and its effects were investigated, 4) studies were prospective, and 5) English language was used. Non-peer-reviewed articles were excluded. Search results were screened by title, abstract, and full text. Two independent authors assessed the quality with the Downs and Black Quality Index.
Results:
We included 14 studies of 140 patients from 5 types of neuromuscular disorders (Duchenne muscular atrophy, spinal muscular atrophy, limb-girdle muscular atrophy, facioscapulohumeral muscular dystrophy, and amyotrophic lateral sclerosis). The mean quality was low (16/32) due to flaws in study design, selection bias, and power. Even though many were of low quality and lacked descriptions of adverse events, they all showed positive effects. Most studies investigated physical training of mastication or respiration with improvements in both. Other findings were improvements in endurance, extremity strength, and range of motion.
Conclusions:
Physical training of wheelchair users with neuromuscular disorders is not well investigated. Physical training seems safe and beneficial, but training of respiratory and masticatory muscles is the only well-documented exercise modality that can be advised in patients with Duchenne Muscular Dystrophy or Duchenne Muscular Dystrophy/Spinal Muscular Atrophy, respectively. Larger, high-quality trials, including other neuromuscular disorders, are needed to assess the effects and adverse events of physical training.
This is a visual representation of the abstract.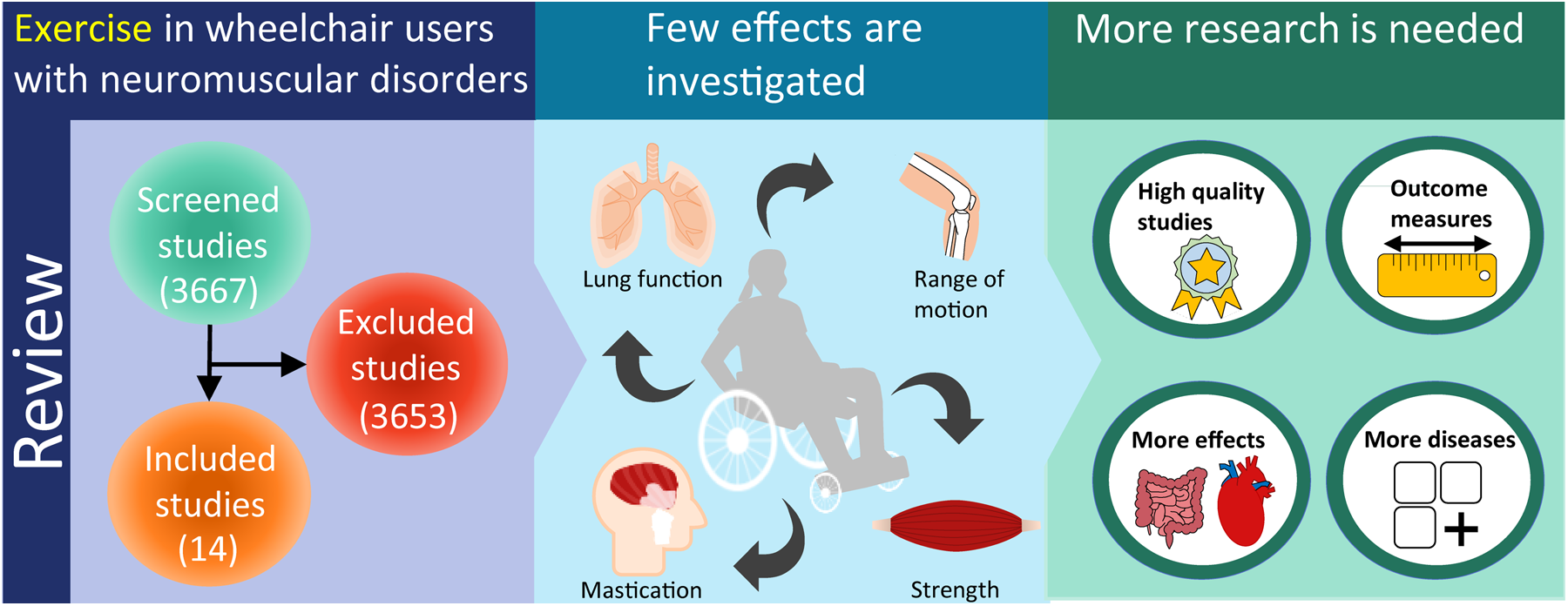
Introduction
Physical training of wheelchair users with neuromuscular disorders (NMD) is a relatively ignored field in medical research. Symptoms, progression, and severity differ among disorders, but most disorders can lead to wheelchair dependence. Wheelchair users with NMD can have pain, fatigue, or weakness of cardiac, respiratory, axial, bulbar, or masticatory muscles.1–4 Wheelchair use leads to immobilisation and, thus, an increased risk of musculoskeletal pain, constipation, reduced quality of life (QoL), weight gain, osteoporosis, and lifestyle disorders.5–10 They are limited in activities of daily living and often need personal assistants to facilitate clothing and personal hygiene. Since none of the disorders are curable, patients rely on treatments that ease their symptoms or increase their independence.
Physical training positively influences physical and mental health in healthy individuals.11,12 Benefits include lowering blood pressure, improving insulin sensitivity, favourable plasma lipoprotein profile, positive effects on the heart, and reduced constipation and fatigue.13–15 Even small amounts of physical training decrease mortality. 16
Physical training in wheelchair users affected by other diseases than NMD, such as spinal cord injury, cerebral palsy, and multiple sclerosis, has also shown positive effects. The main effects have been reduction in pain, correction of lipid levels, and improvement in cardiorespiratory status, endurance, muscle strength, and activities of daily living.17–20 Only within the last two decades have the benefits and safety of physical training of ambulatory patients with NMD become better understood.21–23 For many years, it was believed that the muscles of neuromuscular patients would be damaged during physical training. This belief arose from studies of eccentric training and electrical stimulation of dystrophin-deficient mice models.24,25 More recent studies have shown that patients with NMD, including dystrophinopathies, benefit from most types of physical training.21,26 Benefits include improved VO2max, strength, functional tests, and QoL, and reduced fatigue. 27 There are a few exceptions: a few types of NMDs should avoid specific types of training – dystrophinopathies should for example avoid eccentric exercise. There is now evidence to suggest that physical training should be advised for most patients with NMDs. 21
Since physical training benefits healthy individuals, wheelchair users with non-NMD and ambulatory patients with NMD, it might also benefit wheelchair users with NMD. However, it can be speculated whether the muscle mass of wheelchair users with NMD is too low to gain the potential benefits from training seen in ambulatory patients and to impact the cardiovascular system during aerobic training. 28 This review, therefore, investigates if patients with NMD benefit from training after becoming wheelchair users, which effects and harms are seen, and which form of physical training is beneficial.
Method
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Eligibility criteria
Inclusion criteria were: 1) investigated patients should have a diagnosis of a progressive NMD, 2) at least 60% of patients in a study should be wheelchair users to ensure that the majority of patients were wheelchair users without excluding relevant studies, 3) studies should investigate physical training, defined as purposeful, planned, structured, and repetitive physical activity, 4) studies should investigate the effects of an exercise program, 5) studies should be prospective, and 6) studies should be written in English. Studies were excluded if they were non-peer-reviewed, studies on animals, or systematic reviews.
Data sources and search strategy
We performed a MeSH and Text Word search using PubMed (Supplementary Table 1). Studies published until the beginning of November 2020 were included in the initial search. We updated the search prior to submission in July 2024 using the same in- and exclusion criteria as the initial search. Reference lists of systematic reviews were checked. Case reports were included not to miss any relevant information.
Study selection
Two independent reviewers (LRK and NSP) screened the articles from the initial search in the following three steps: 1) screening by title, 2) by abstract, and 3) by full text. Any disagreements between reviewers were solved by consensus. The updated search (786 studies) was only screened by NSP.
Data extraction
All included studies were evaluated by LRK and re-evaluated by NSP with the following questions: 1) Which NMDs were investigated? 2) Which training method was used? 3) How many patients were included? 4) Which frequency, intensity, time, and type of training was investigated (the FITT factors)? 5) Which effects and harms were found? 6) Which limitations and solutions to physical training were seen?
Quality assessment
Two independent reviewers (LRK and NSP) assessed the quality of all included studies through the Downs and Black Quality Index 29 (see Table 1). For each study, 27 quality markers in 5 areas (reporting, external validity, internal validity bias, confounding/selection bias, and power) were evaluated, and a total score of 0–32 was acquired. Any disagreements between reviewers were solved by consensus.
Quality index score.
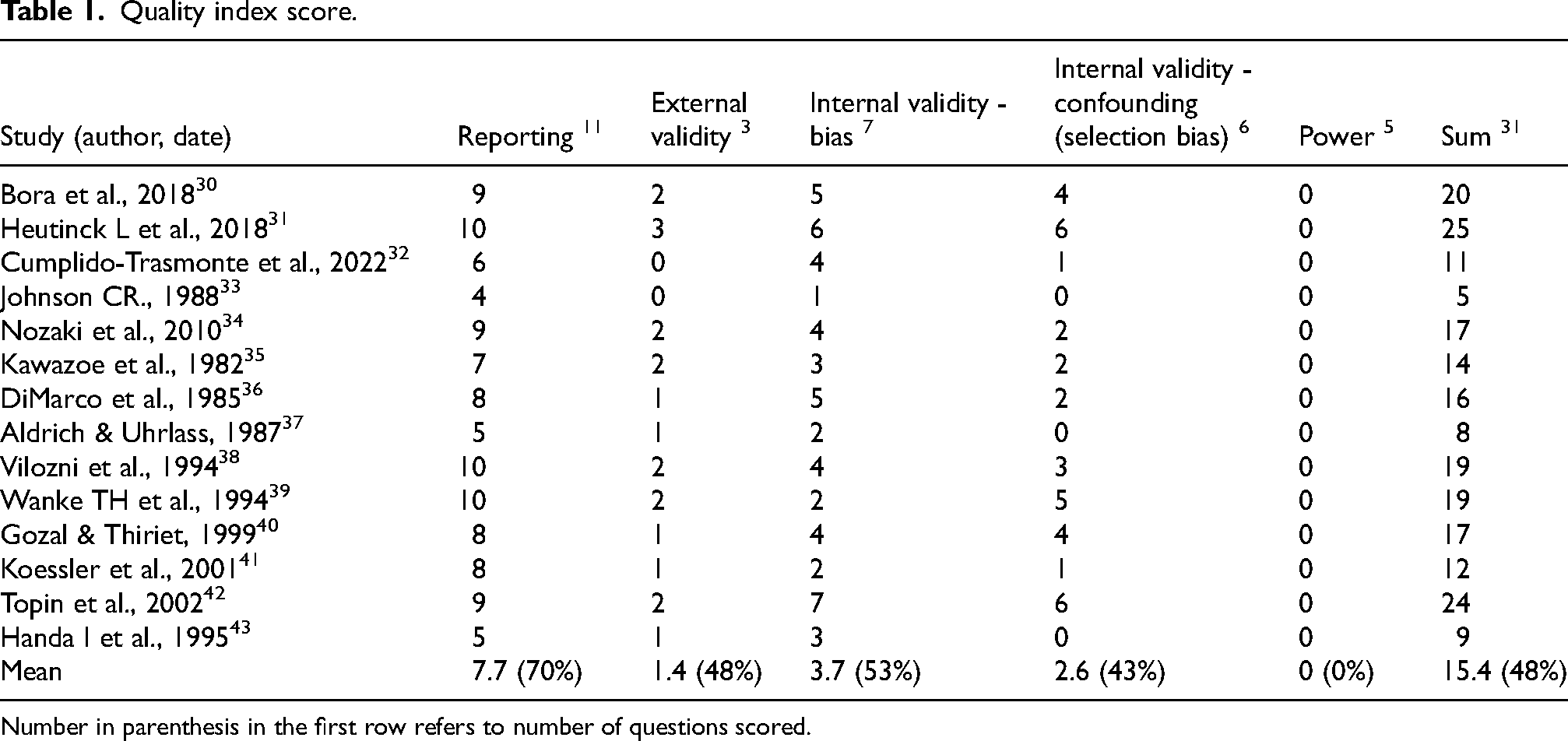
Number in parenthesis in the first row refers to number of questions scored.
The Downs and Black Quality Index excels by including randomised controlled trials (RCTs), case-control studies, and cohort studies. Unfortunately, it is not intended for use in case reports, but rather than using many different quality indexes that cannot be compared, we chose to score case reports on this scale as well. Questions not suited for case reports were scored 0, which was found acceptable since these questions handled items that should lower study quality when not met (for example, power, random variability, and population representation).
The interpretation of question 27 was unclear, so we scored 0 when no power calculation was performed, 3 when a power calculation was performed but was unclear, and 5 when a power calculation was performed, and precise calculations were provided.
Pooled effects were not assessed due to significant heterogeneity regarding intervention, type of NMD, and outcome measures. Only descriptive findings are provided.
Results
Study selection
A total of 3667 articles were identified. Only 14 studies met all criteria (Figure 1). The main reasons for exclusion at abstract/full article level were that no or only a few participants had a neuromuscular disease and that either no or not enough participants were wheelchair users. Other main reasons were the lack of either an exercise program or measurements of exercise effects.
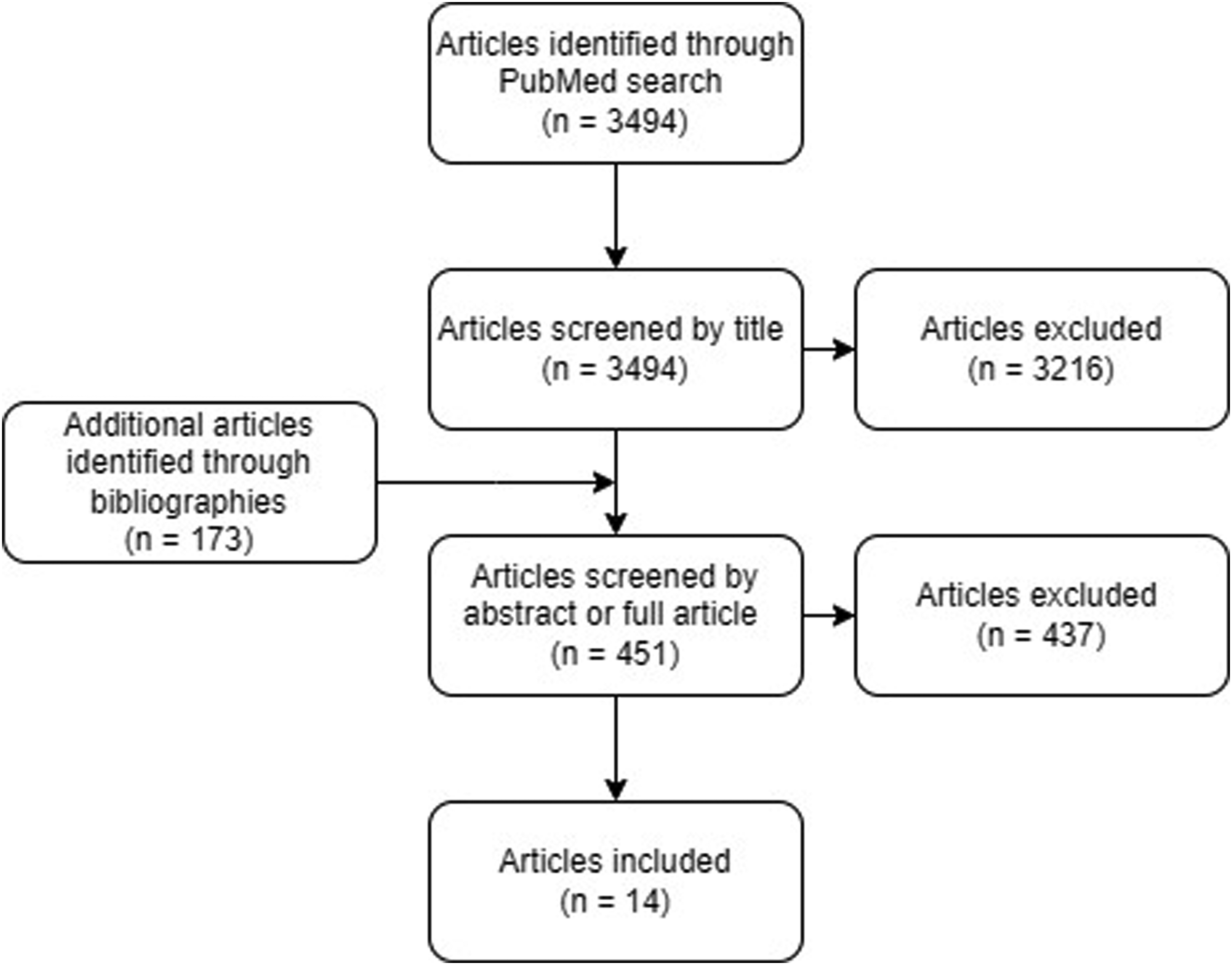
Flow diagram. Flowchart of number of articles screened by each level.
Only one study that seemed relevant was excluded: The study investigated arm and leg cycle exercise in children with DMD and was excluded since only 40% of patients were wheelchair users. 44 Subgroup analyses were not made. It is, however, worth mentioning their challenges in investigating this patient group since these might apply to other wheelchair users with NMD as well (or at least to the child population). Challenges included a limited attention span and exhaustion after only 6 min of exercise.
Quality assessment scores
Scores ranged from 5 to 25 out of 32, with a mean score of 15 (Table 1). Three studies were case reports, and only four studies were RCTs. When removing case reports from calculations, the mean quality score increased to 18. The domains “Power” and “Selection bias” scored the lowest. Very few studies used blinding or randomisation or described periods of inclusion, number of participants invited, compliance/adherence, or loss to follow-up.
Effects of physical training
The 14 included studies showed local and systemic effects after physical training (Table 2 and Figure 2).
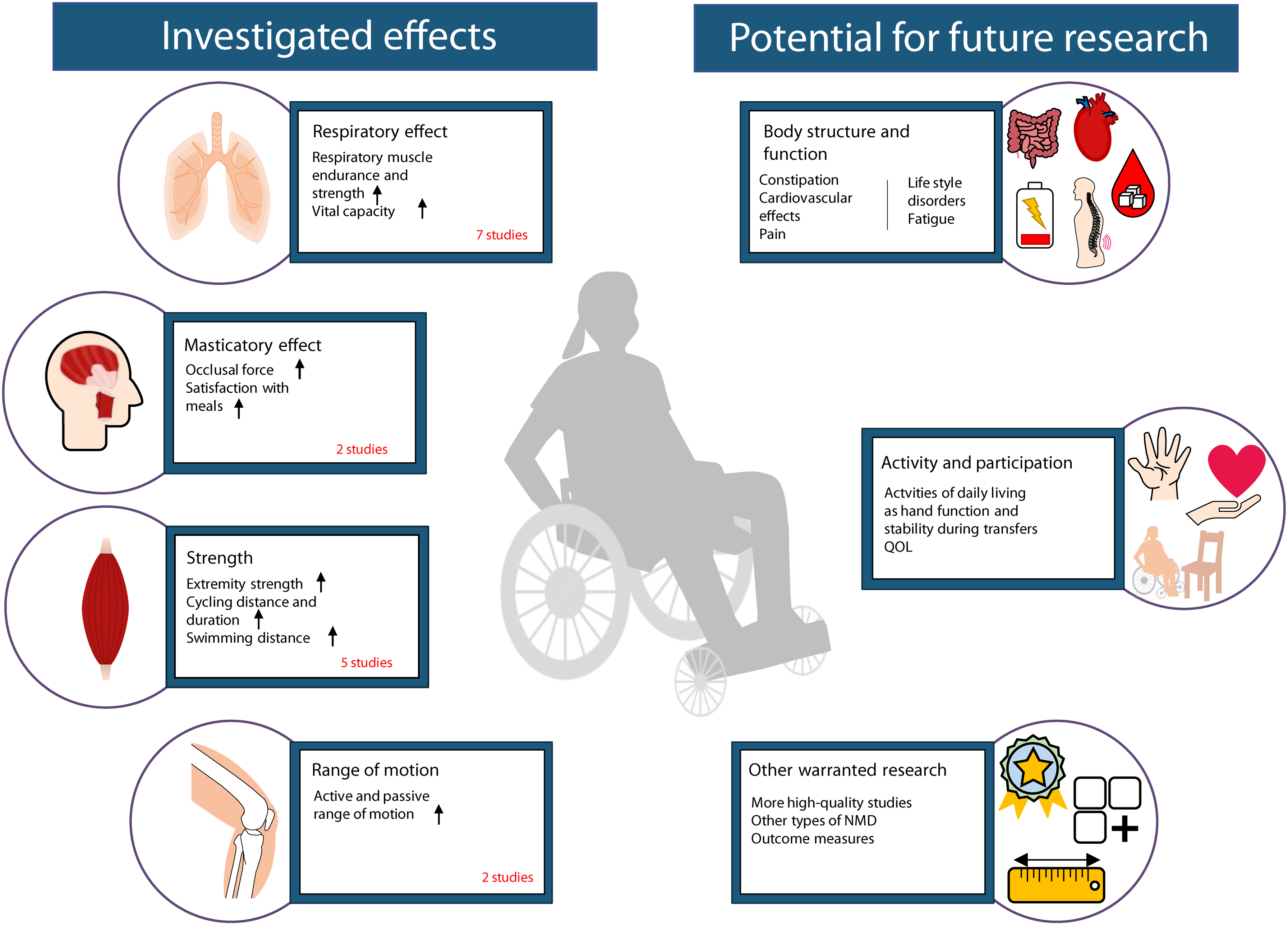
Investigated effects and potential for future research of exercise in wheelchair users with neuromuscular diseases. To the left is shown investigated effects. To the right is shown potential for future research.
Included studies.
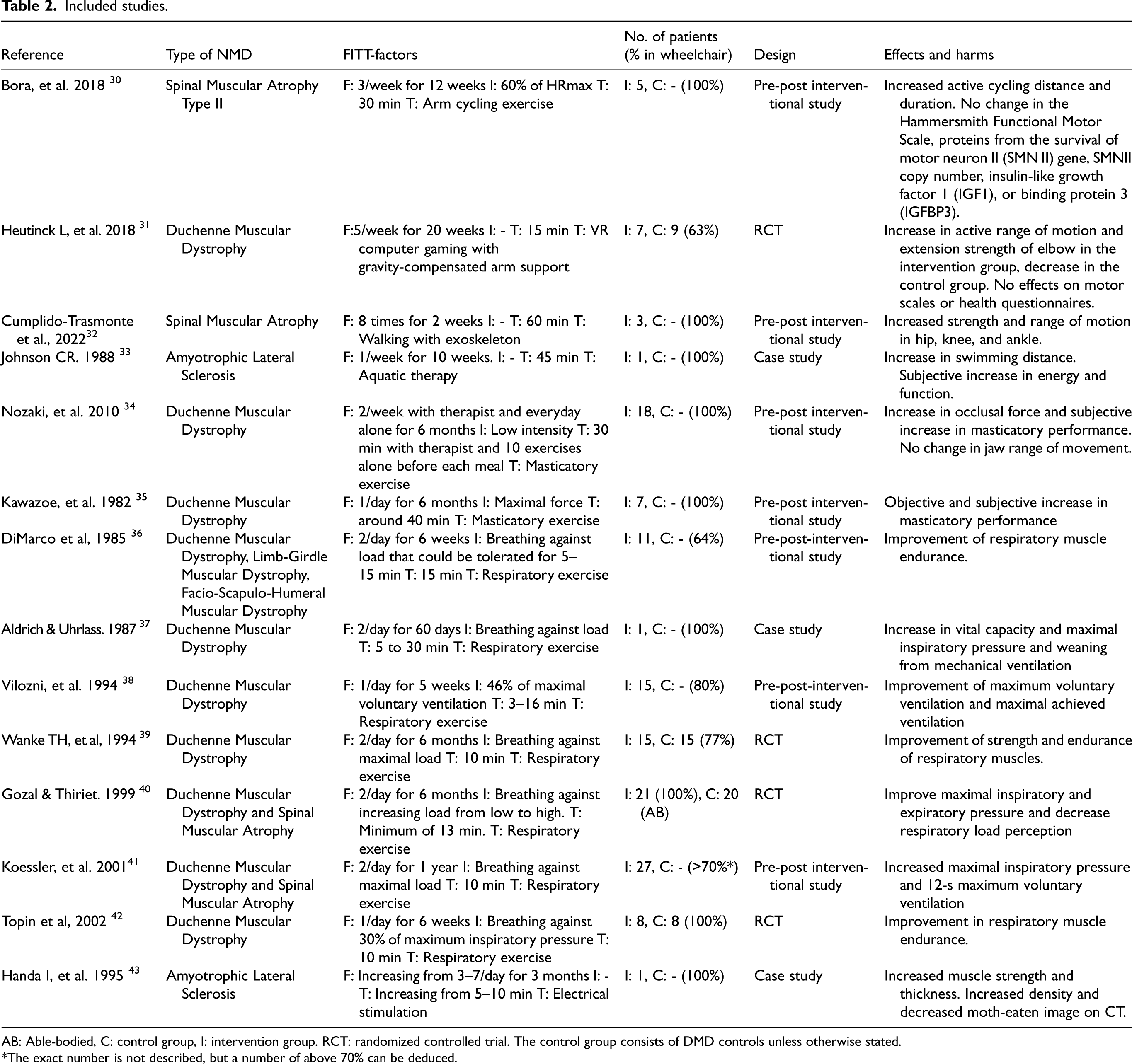
AB: Able-bodied, C: control group, I: intervention group. RCT: randomized controlled trial. The control group consists of DMD controls unless otherwise stated.
*The exact number is not described, but a number of above 70% can be deduced.
Arm cycle exercise
One study investigated twelve weeks of supervised arm cycle exercise in five children with SMA type II (all wheelchair users). 30 They trained at 60% of their maximal heart rate three times weekly for 30 min per session for 12 weeks on a cycle ergometer, recording the children's active, passive, and total cycling duration and distance. The active cycling distance and time increased significantly during the training period by around 50%. The Hammersmith Functional Motor Scale (HFMS), the levels of the survival motor neuron protein encoded by the survival motor neuron gene 2 gene (SMN2), SMN2 copy number, insulin-like growth factor 1 (IGF1), and binding protein 3 (IGFBP3) were not significantly affected by the training. None of the patients experienced muscle pain or cramps, but three had fatigue initially, decreasing during the training period.
Virtual reality computer gaming
One study investigated the effect of using virtual reality (VR) computer gaming for exercising children with DMD. 31 Seven patients trained for 15 min in five sessions per week for 20 weeks playing virtual reality (VR) games using gravity-compensating dynamic arm support. Nine DMD patients were controls. 63% were wheelchair users. The active ROM and elbow extension strength (measured with handheld dynamometry (HHD)) increased in the intervention group with an average of 15.7 degrees and 1.5 lbs, respectively, whereas they decreased in the control group. Performance of upper limb (PUL) score, assisted 6-min cycle test, motor function measure 32 (MFM32), Abilhand-measure, Kidscreen-52, and Global Health Question did not differ between the two groups. One patient experienced shoulder and thumb pain, which disappeared after equipment adjustment. No other adverse events were recorded. The Gainboy can encourage training in ROM and elbow extension strength in patients with DMD.
Walking with exoskeleton
In one study, three children with SMA type II (all wheelchair users) walked with an exoskeleton for 60 min eight times over two weeks. 32 Improvements in hip-, knee-, and ankle- strength and ROM were measured using an HHD and a goniometer, respectively. Hip ROM increased by 12.6% and ankle ROM by 34.1%. Knee ROM was stable. Strength increased across hip by maximal 112%, across knee by maximal 119%, and across ankle by maximal 93% (from baseline to 10-week follow-up). The authors did not describe adverse events.
Aquatic therapy
One case study involving a patient with amyotrophic lateral sclerosis (ALS) used aquatic therapy. 33 By the beginning of the training, the patient needed a lift and the assistance of three people to be transported from his wheelchair to the pool. He could not stand alone and could only propel himself 10 feet. After a training program of 45 min once per week for ten weeks, he could swim 4290 feet aided by a flotation vest, with only occasional need for assistance for direction. He reported no fatigue, and his wife said he could assist more during transfers following a swimming lesson than during other times in the week.
Masticatory exercise
Two studies investigated the training of masticatory function in patients with DMD. The first 34 used a heat pack, massage, and then ROM exercises on the jaw of 18 patients (all wheelchair users) for 30 min two times a week and self-training with ROM exercises before every meal. The occlusal force and patients’ satisfaction with meals increased after six months (the mean change of occlusal force was 23.5 N). The maximum degree of mouth opening did not change. The authors did not describe adverse events.
In the second study, 35 occlusal force and tongue pressure were trained by daily supervised repetitions of jaw clenching and pressing the tongue against the palate combined with head movement in seven patients with DMD (all wheelchair users). Improvement in masticatory performance was seen after one month of training (relative mean change of around 25%), with further improvement in the sixth month (relative mean change of around 40% from baseline). Six of the seven patients reported an improvement in chewing function. The authors did not describe adverse events.
Thus, masticatory exercise can be beneficial for DMD patients having problems eating.
Respiratory exercise
Seven studies investigated the effects of respiratory exercise. All included patients with DMD,36–42 two also patients with SMA,40,41 and one also patients with LGMD and FSHD. 36
Five studies36,37,39,41,42 used inspiratory muscle resistance training (IRT), one resistive inspiratory and expiratory training, 40 and one a video game-based training device. 38
The first study 36 included 11 patients (of whom 7 where wheelchair users) with DMD, LGMD, and FSHD with two sessions of 15 min of IRT daily for six weeks. They found increased respiratory muscle endurance measured by increased maximum resistance that could be tolerated for 5 min (mean change 104 cmH2O/litre/sec), and by the maximum duration, the ventilation could be sustained at four given percentages of the maximal voluntary ventilation (MVV) (mean change ranging from 75–128 s). Six patients trained for another six weeks with further improvements. However, there was no effect on spirometry data. There were no adverse events of training.
The second study 37 used gradually increasing inspiratory resistance training in one wheelchair user with DMD on mechanical ventilation twice daily for 60 days. After the first 45 days, the patient's vital capacity had risen from 380 mL to 850 mL, and he could tolerate T-piece breathing for 16 h. The patient was weaned off mechanical ventilation after two additional weeks. There was no evidence of malnutrition, electrolyte disorder, or thyroid dysfunction, and his haematocrit and serum CK were stable.
In the third study, 38 15 children (of whom 12 where wheelchair users) with DMD used a video game-based training device at home for 3–16 min daily for five weeks. MVV and maximal achieved ventilation (VEmax) improved (mean change 10% and 55% respectively), and the progressive isocapnic hyperventilation manoeuvre (PIHV) duration increased (mean change 46%), but only in the patients with moderately reduced lung function. The group of patients with severely reduced lung function did not improve by training. The authors did not describe adverse events.
The fourth study 39 used IRT and maximal static inspiration for ten minutes twice daily for six months, followed by a 6-month discontinuation in 15 patients with DMD and 15 DMD controls (77% wheelchair users). They found increased inspiratory and diaphragmatic muscle strength (mean change 2.36 kPa and 2.67 kPa, respectively) and increased inspiratory muscle endurance (mean change 3.3 min) in patients with moderately reduced lung function but not in patients with severely affected lung function. The five patients with severely reduced lung function stopped training after 1 month due to lack of improvements. They found no CK elevations.
The fifth study 40 included 21 children with DMD or SMA (all wheelchair users) and 20 healthy controls. Patients and controls trained with either a device to provide inspiratory and expiratory pressure or similar training with no load twice daily for six months. Only the group of patients with NMD who trained with load experienced improvements in respiratory muscle strength measures such as maximal inspiratory and expiratory pressure and a decrease in respiratory load perception (mean change +19.8 cmH2O, + 27.1 cmH2O, and −1.9 Borg visual analogue scale points, respectively). The authors did not describe adverse events.
The sixth study 41 included 27 patients (>70% wheelchair users, the exact number is not given) with DMD or SMA divided into three groups depending on their initial lung function. The study used specific inspiratory muscle training with ten 1-min loaded breathing cycles twice daily for 24 months. They found an increase in respiratory muscle strength and endurance measured by maximal inspiratory pressure (relative mean change 56%) and 12sMVV (relative mean change 12%), respectively, across all three groups until ten months of training, where they reached a plateau. The authors did not describe adverse events.
The seventh study 42 used IRT for 10 min daily for six weeks in 8 children with DMD and 8 DMD controls (all wheelchair users). The training group breathed against higher pressure than the control group. They found an increase in endurance by 46% in the training group but no change in maximal inspiratory pressure (strength). The authors did not describe adverse events.
Respiratory training benefits patients of all disorders, but different disease severity levels might require different approaches.
Electric stimulation
Electric stimulation was investigated in one study in a wheelchair user with ALS with weakness and atrophy of facial and extremity muscles, more severely affected on the right side. 43 Electric stimulation was applied to the upper and lower extremities of the right side of the body every day with an increase in duration and frequency, ending at 10 min 7 times per day in week 7. After 3.5 months, the difference in strength between the right and left sides of the body was reduced (−0.8 points with manual muscle testing) due to reduced strength in the left side. The authors interpret this as preserved strength of the muscles on the right side of the body. They also found an increased thickness and density and reduced moth-eaten image on CT on the right side of the body (quantification not reported). The authors did not describe adverse events.
Summary of results
The total number of exercising patients was 140 across five different NMDs (94 DMD, 17 SMA, 5 LGMD, 2 ALS, 1 FSHD, and 21 patients with either DMD or SMA (not specified in the study 40 ). Of these, more than 112 were wheelchair users (one study 41 did not describe the exact number of wheelchair users).
Respiratory and masticatory exercises were the most investigated types of physical training (98 exercising patients in 7/14 studies and 25 exercising patients in 2/14 studies, respectively). The five remaining studies (17 exercising patients) investigated endurance and strength training of extremities with different interventions: one investigated arm cycle exercise, one computer gaming, one walking with an exoskeleton, one aquatic therapy, and one electric stimulation.
Frequency, intensity, and time of exercise differed among the studies, primarily due to the different types of exercise investigated. Physical training was prescribed for two weeks to one year, with masticatory and respiratory exercises being prescribed for the most prolonged period (typically 6 months). The time of each training session differed from 5–60 min, with the respiratory training often being shorter than other types of training (typically 5–15 min). The effects of physical training are summarised in Figure 2; effects include facilitated breathing and chewing and increased strength, ROM, and endurance. Adverse events to exercise were registered in 6/14 studies, of which four did not find any. Three patients experienced fatigue at the beginning of the exercise period and one joint pain; all were known adverse events to exercise and either passed spontaneously or with adjusted equipment.
Discussion
We found that physical training is not well investigated in wheelchair users with NMD. This limits this review's ability to give insight into the benefits and harms of physical training, to make specific exercise recommendations, and to give advice regarding FITT factors. High-quality studies are needed on more types of NMD, different types of exercise, additional outcomes (such as cardiovascular benefits, hand function, and constipation), and a systematic screening for adverse events. Nevertheless, all studies point towards physical training as beneficial, and no studies have reported severe or unexpected adverse events.
Respiratory and masticatory exercises are the only well-documented exercise interventions and can improve function and satisfaction with meals in patients with DMD or DMD/SMA, respectively. Other not well-documented findings are that 1) physical training might improve active ROM, cycling distance, and strength in extremity muscles, 2) the decrease in motor function with disease progression might be slowed down by bicycle training, and 3) some patients might experience fatigue after exercising, but this decreases during the training program.
Fatigue and joint pain were the only described adverse events of exercise. Cramps and muscle pain were not reported in any of the six studies describing adverse events, and no serious adverse events were described. CK is a safety marker for muscle damage frequently used in exercise studies with ambulant patients, but it was only investigated in two of the included studies and only with respiratory training. It can be questioned whether CK is a useful safety marker in exercise studies in wheelchair users. The muscle mass is small and training intensity low, so potential muscle damage might not significantly increase CK.
Study limitations
There is a risk that relevant studies were missed in the screening process by only reviewing papers from PubMed. With a broad search including all types of NMDs and all types of exercise, relevant studies might have been missed in the search strategy if not all diseases and types of training with all their synonyms were included. The Downs and Black quality index score is not intended for use in case reports but was used in this review to make the quality comparable among studies. This increases the risk of overestimating the mean quality of studies. The mean quality of studies did not change substantially by removing case reports from the analysis, and the mean quality is thus not underestimated.
Guidance for physical training
Even though not many studies have focused on physical training of wheelchair users with NMD, and the quality of the studies was generally low, many effects, exercise modalities, and challenges are described that can inspire rehabilitation programmes.
Endurance is low partly due to the low muscle mass; in one study, a patient could exercise for only 6 min. 31 Signs of fatigue should, therefore, be monitored. Intensity, resistance, and exercise duration can be reduced, the exercise can be divided into more but shorter exercise bouts, or another training method might be more suitable if the exercise is too strenuous. Aquatic therapy involves, for example, many muscles and reduced gravity, and therefore, less strain is put on each muscle.
Guidance for choosing outcome measures
Choosing a relevant outcome measure to plan and monitor the effects of physical training can be challenging due to the severely reduced motor function and, thus, changed response to exercise. Below are suggestions on how to measure and monitor outcomes, distributed on the two International Classification of Functioning, Disability and Health (ICF) domains of Functioning and Disability:
Body function and structure: The cardiovascular effect of training is often measured using the maximal heart rate or VO2peak in ambulant patients. In more advanced stages of NMDs, the limited peripheral capacity and low muscle mass make it difficult to reach the true maximum heart rate/cardiac output with exercise. 48 The maximal heart rate and VO2peak are thus not valid for many patients. A solution could be to measure the active cycling duration and -distance from an assisted cycle test, which was used to detect changes during an exercise program in one of the included studies. 30
Improvements in muscle strength were detected with HHD in one of the included studies. 31 However, HHD cannot measure strength when manual muscle testing scores go below 3, which is often the case in more advanced stages of NMD. MRI can measure increases in muscle size with exercise in healthy individuals 49 but is often complicated and even impossible to use for wheelchair users due to severe contractures, low respiratory capacity, or a cardiac or respiratory device. Muscle ultrasound is less sensitive than MRI and might not detect changes in slowly progressive muscles with short exercise periods. One of the included studies 43 detected increased muscle size by CT and decreased moth-eaten image in one patient with ALS after electric stimulation. However, with this low evidence and the radiation risk that CT brings, it is questionable whether CT can and should be used. There is thus a need to find other ways to measure improvements in muscle strength and/or size. The maximal watt and how active the patient is during a cycle test (measured in percent of total work), is used somewhat in other diseases,50,51 and could have a potential in wheelchair users with NMD as well.
The respiratory effects of exercise are highly relevant, given the high risk of respiratory failure in many types of NMD. In many studies, improvements in respiration could be measured with outcome measures of inspiratory and expiratory pressure. Even though two studies on respiratory training found that the most affected patients did not improve, this might be due to too short an exercise period, poor technique, low power, or low sensitivity of outcome measures.38,39
Activity and participation: Improvements in masticatory function with exercise have been measured in wheelchair users with NMD using active ROM of the jaw and occlusal force/bite pressure. Motor function scales (such as the MFM32 or HFMS) for measuring improvements in muscle function are not helpful in wheelchair users since most tasks cannot be performed; likewise, the studies using HFMS could not detect changes after exercise. A motor scale for more advanced stages of NMD is thus warranted.
Even though questionnaires on QoL are now developed for patients with a progressive NMD, 52 these are not targeted wheelchair users and include unimportant areas and lack essential areas.
Unexplored, potential effects
Due to the few studies with generally low quality, more research of high quality is needed.
Areas still needing investigation are (see Figure 2): 1) If wheelchair users benefit from endurance and strength training of extremities. 2) If so, the establishment of FITT factors and the feasibility of the various training modalities are needed. 3) If wheelchair users with other NMDs than DMD and SMA have an effect on physical training and which training method is the most desirable for each disease. 4) If wheelchair users with NMD can experience the cardioprotective effects of exercise. 5) If physical training can reduce consequences of wheelchair use such as constipation, lower back pain, and risk of lifestyle disorders. 6) If physical training can improve QoL as it can in wheelchair users with other diseases than NMD. 53 7) If physical training can reduce fatigue. Many patients with NMDs suffer from fatigue, which often increases with the severity of the disease. 54 Fatigue can be very disabling, significantly impacting the QoL, independence, and daily living,55,56 but can be reduced with exercise in ambulatory patients. 27 8) If functions essential for daily living, such as hand function, stability, and transfers, can be improved. 9) If there is a limit on how affected a muscle can be and still benefit from exercise.
Conclusion
We have found that physical training in wheelchair users with NMDs is not well documented. Conclusions are limited by only studies on a few genetic disorders, limitations in the number of included patients, design, strength, and quality of most studies, and only four studies made in the last 10 years.
All studies have found that physical training seems safe and beneficial. With the low overall quality of the studies, the only conclusion that can be made is that physical training of respiratory and masticatory muscles is well documented and should be advised in patients with DMD or DMD/SMA, respectively. There is thus a need for larger studies of higher quality, with more types of NMD, describing the effects and adverse events of physical training.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602241313114 - Supplemental material for Physical training of wheelchair users with neuromuscular disorders: A systematic review
Supplemental material, sj-docx-1-jnd-10.1177_22143602241313114 for Physical training of wheelchair users with neuromuscular disorders: A systematic review by Nanna Scharff Poulsen, Lærke Rykær Kraglund and John Vissing in Journal of Neuromuscular Diseases
Footnotes
Abbreviations
Acknowledgements
The authors have no acknowledgements to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available within the article and its supplementary material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.