
Abstract
Background
With advancements in cardiorespiratory care, the lifespan of patients with Duchenne Muscular Dystrophy (DMD) has significantly increased, shifting the focus from merely extending life to enhancing quality of life and managing complications effectively. However, there is a lack of interest in the management of adult DMD, highlighting a gap in holistic care approaches for this aging population.
Objective
This study aims to assess the current state of care for adult DMD patients in South Korea, focusing on multidisciplinary management and identifying key areas for improvement.
Methods
We retrospectively reviewed the medical records of 168 adult DMD patients who visited the Pulmonary Rehabilitation Center at [blinded for review] from 2022 to 2023. Demographic data, ventilatory support status, cardiac function, gastrointestinal, renal, and skeletal health were analyzed.
Results
Of the patients, 93.8% required non-invasive ventilatory support, while 6.2% used invasive ventilation. Cardiac medications were prescribed to 82.1% of patients, with beta-blockers being the most common. Renal dysfunction was found in 10.1% of patients, with one patient requiring dialysis. A significant portion (54.8%) were on anti-constipation medications due to gastrointestinal issues, and 41.7% of patients had undergone scoliosis correction surgery. Bone mineral density was significantly reduced in most patients, with an average Z-score of −3.3.
Conclusions
This study emphasizes the need for improved care protocols that enhance lifespan and quality of life and manage complications for patients with DMD. This study advocates a shift in healthcare strategies toward a more integrated and holistic care model for adult patients with DMD.
Introduction
Duchenne Muscular Dystrophy (DMD) is a genetic disorder caused by mutations in the dystrophin gene, resulting leading to progressive muscle degeneration affecting skeletal, cardiac, and respiratory muscles.1,2 With a prevalence of 21.2 per 100,000 school-aged boys, 3 DMD typically presents between the ages of 2 and 3 when affected children begin experiencing difficulties climbing stairs or running. By ages 10 to 12, most patients are wheelchair-dependent, and respiratory and cardiac complications begin to emerge. 4 Cardiomyopathy, which often develops after age 10, is present in all adult patients and can be accompanied by life-threatening arrhythmias. Additionally, spinal deformities, especially in patients not receiving corticosteroids, can further compromise respiratory function and mobility. 5
Global guidelines for the care of DMD were initially introduced in 20106,7 and have undergone several updates, with the most recent revision in 2018.2,8,9 These guidelines emphasize a multidisciplinary approach across different stages of the disease, from early diagnosis to the late non-ambulatory phase. With the development of diverse multidisciplinary treatments, patients’ lifespans have been greatly extended. 6 In the 1960s and 1970s, few patients survived beyond their teenage years, but since the 1980s, advances in care—particularly in respiratory, cardiac, and nutritional management—have dramatically increased life expectancy, with many now living into their 30 s and beyond. 10
This shift in longevity has brought new challenges, emphasizing the need for comprehensive care that addresses not only life-threatening complications but also quality of life in adulthood. Although extensive research has been conducted on DMD, most studies focus on pediatric care, leaving gaps in the recommendations for adult patients who face an increasing burden of complications. 6 Addressing these gaps through a multidisciplinary approach is critical to enhancing both life expectancy and the quality of life in adult patients with DMD.
Therefore, this study aims to investigate the multidisciplinary management of adult patients with DMD in South Korea based on data from patients who visited the specialized Pulmonary Rehabilitation Center of [blinded for review], assessing the current state of care and identifying key areas for improvement based on clinical data.
Materials and method
Study cohort
Data were retrospectively collected from the medical records of adult DMD patients who were admitted to the Pulmonary Rehabilitation Center at [blinded for review], a tertiary referral hospital for neuromuscular disorders, focusing on their clinical assessments and outcomes documented within this period.
At our center, we primarily manage DMD patients who require ventilatory support, providing comprehensive care. Patients typically follow up every 3–12 months in the outpatient clinic. However, when signs of respiratory insufficiency appear, we admit them for overnight ventilatory monitoring. If ventilatory support becomes necessary, we admit the patients annually to ensure proper ventilator use. Considering the challenges of patient mobility, we also conduct a general assessment during admission and refer them for consultations as needed. 11
For this study, we included patients admitted to our center between 2022 and 2023. The exclusion criteria were as follows: 1) patients under the age of 20, and 2) patients who lost ambulation after their 18th birthday. A cutoff age of 18 was used to exclude individuals with the Becker phenotype, while allowing the inclusion of patients with prolonged ambulation due to steroid use.
Variables analyzed
As mentioned previously, all patients with DMD using ventilators are admitted annually. During their admission, pulmonary function tests are conducted, along with laboratory tests to screen for various conditions, including complete blood count (CBC), routine chemistry, cardiac markers, urine analysis, cystatin C, and arterial blood gas analysis (ABGA). If any abnormalities are found, we consult the relevant specialists for further examinations and treatments as needed. In particular, consultations with a cardiologist are mandatory, and we conduct annual electrocardiograms (EKG), transthoracic echocardiography (TTE), and, if necessary, 24-h Holter monitoring. Chest and abdominal X-rays are also taken to check for any abnormalities. For patients over 20 years of age, dual-energy X-ray absorptiometry (DXA) scans are performed to assess bone mineral density and determine the need for osteoporosis management.
By reviewing the charts, we gathered the following demographic and clinical data: (1) Basic information, including age, date of diagnosis, and age at which wheelchair use began; (2) respiratory management status: use of mechanical ventilator, type of ventilator support (non-invasive or invasive), and initiation date of ventilatory support; (3) information related to cardiac conditions: ejection fraction by echocardiogram, use of implantable cardioverter-defibrillators (ICDs), and administration of cardiac medications; (4) use of medications related to constipation, leus, and other bowel disorders; (5) use of hepatology-related medications; (6) lumbar spine bone mineral density results from DXA scans and the use of medications for osteoporosis; (7) the presence of kidney-related conditions, such as renal failure or urolithiasis; (8) history of scoliosis surgery; and (9) presence of other central nervous system-related symptoms.
For bone mineral density, it is standard practice to use adjusted Z-scores that account for factors such as age, height, bone age, and overall bone size. Previous studies have shown that spinal deformities or anatomical changes can cause inaccuracies in the measurement of bone mineral density through DXA scans.12,13 In this study, both bone density and Z-scores were measured concurrently.
Statistical analysis
All statistical analyses were performed using R version 3.5.3 software (R Foundation for Statistical Computing). We calculated both numbers and percentages for the categorical variables. For continuous variables, we used the mean ± standard deviation. When comparing by age group, we divided the groups into 5-year increments starting from 20 years of age, with those aged 40 years and over grouped together. We conducted a one-way analysis of variance to analyze the differences between the groups. A linear regression analysis was performed to assess the relationship between age and eGFR by cystatin C. Scatter plots with a fitted trend line were generated to visualize the data distribution. The significance of the trend was evaluated using the p-value from the regression model, with statistical significance defined as p < 0.05.
Ethical approval
This study was approved by the Institutional Review Board of the [blinded for review], Seoul, Korea (Identifier: 3-2023-0311). The requirement for informed consent was waived. The study protocol was conducted in accordance with the tenets of the Declaration of Helsinki.
Results
Basic characteristics of included patients
A total of 168 patients were included in this study, excluding 33 patients under the age of 20 years with confirmed records of DMD, 32 of whom were not genetically diagnosed, and four suspected to be of the Becker type based on genetic analysis and clinical considerations, such as age of loss of ambulation and timing of ventilator use (Figure 1). As for the dystrophin gene mutation profile, of the 167 patients analyzed, 109 had exon deletions and 18 had exon duplications (Figure 2). Additionally, 41 patients were identified as having point mutations through gene sequencing, which were not detectable through exon-level analysis such as MLPA.
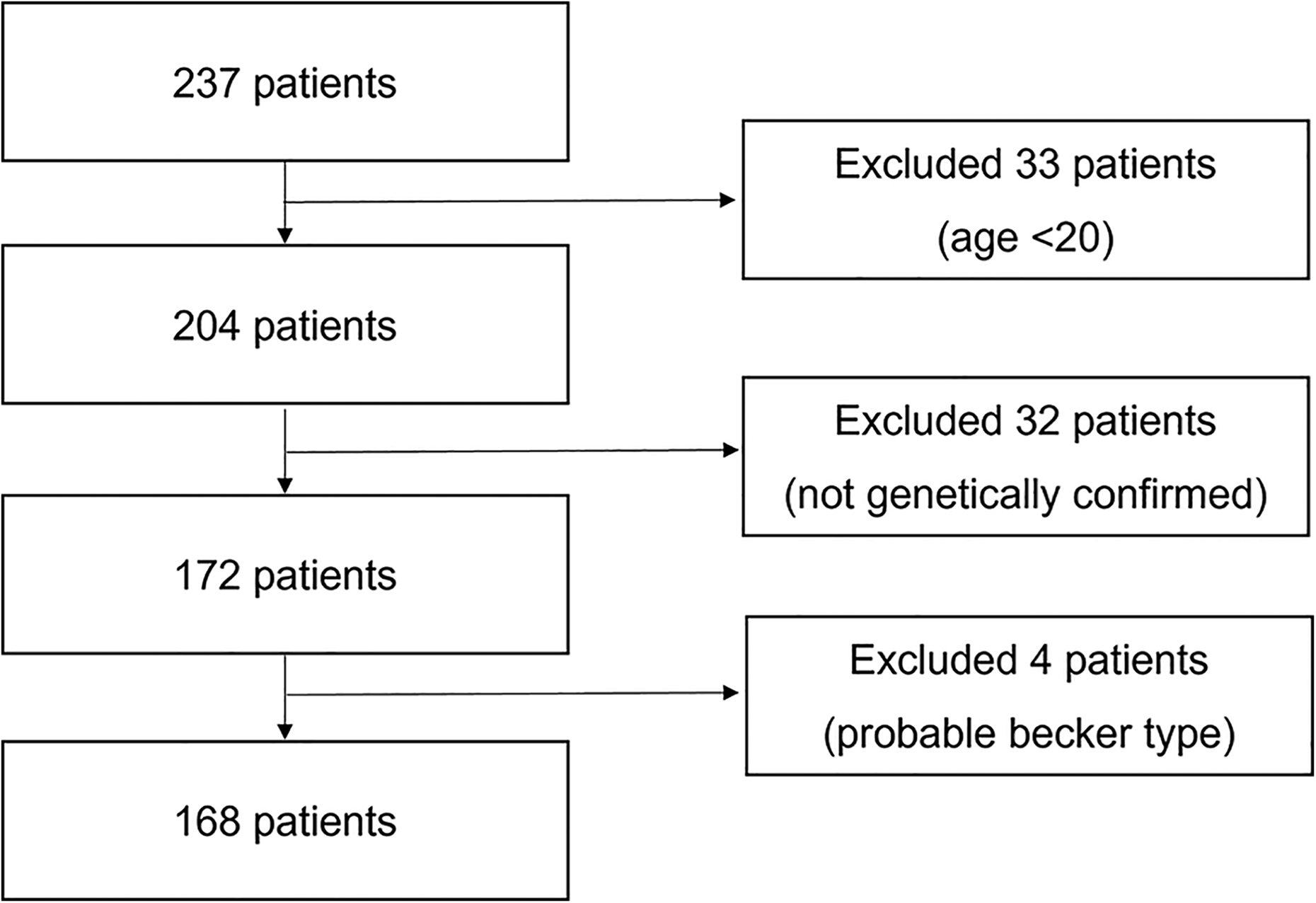
Flow chart diagram.
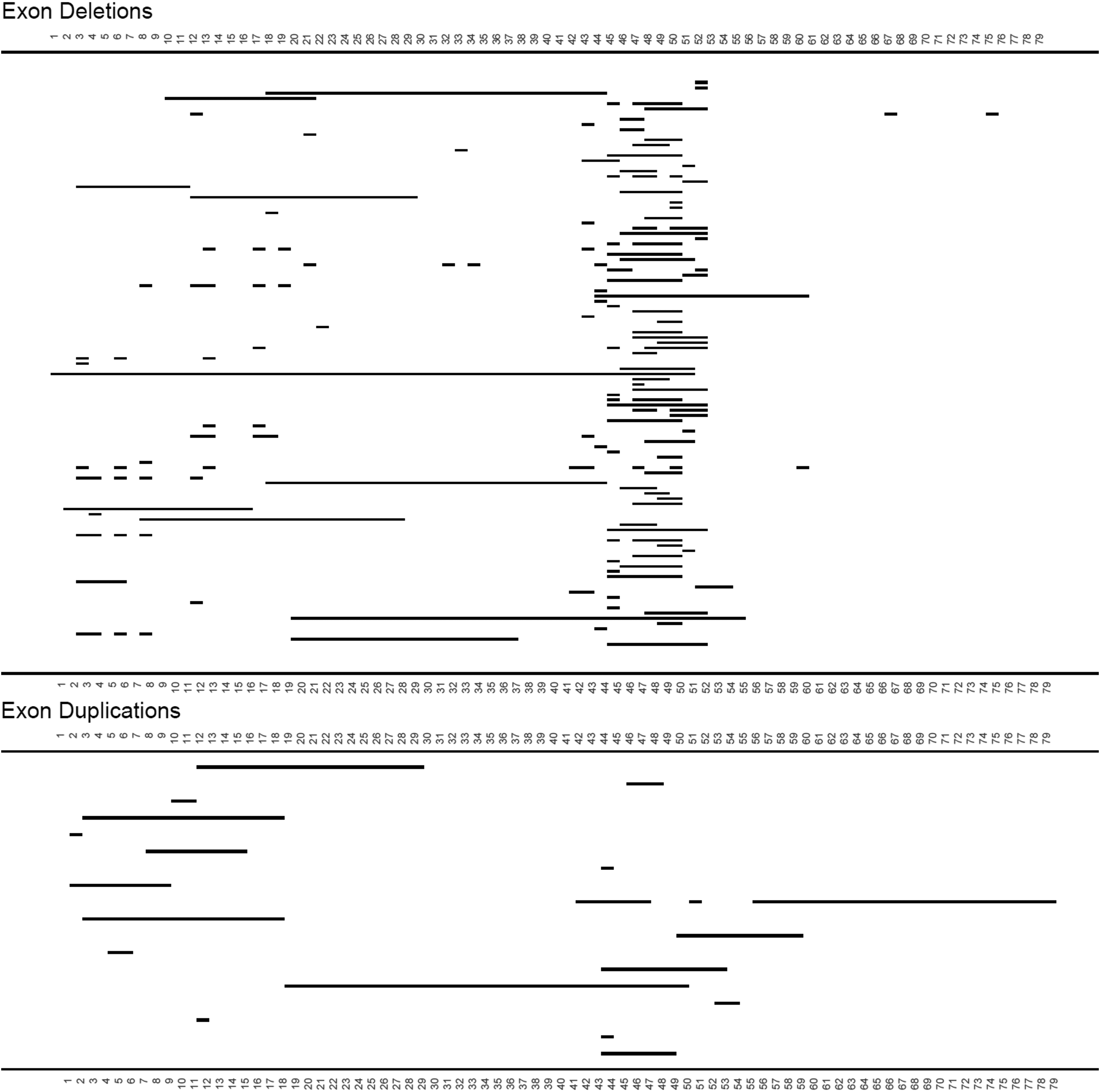
Frequency of deleted and duplicated exons in dystrophin gene in DMD patients.
As of the end of the year 2023, the mean age of the 202 patients was 29.5 ± 6.1 years. Among the patients, 41 (24.4%) were aged 20–24, 61 (36.3%) were aged 25–29, 38 (22.6%) were aged 30–34, 16 (9.5%) were aged 35–39, and 12 (7.1%) were 40 or older.
The patient's wheelchair-bound age was 11.0 ± 2.1 years. Among the wheelchair-bound age groups, the age that accounted for the most frequency was 10 years, accounting for approximately 26.2% (44 patients; Figure 3).
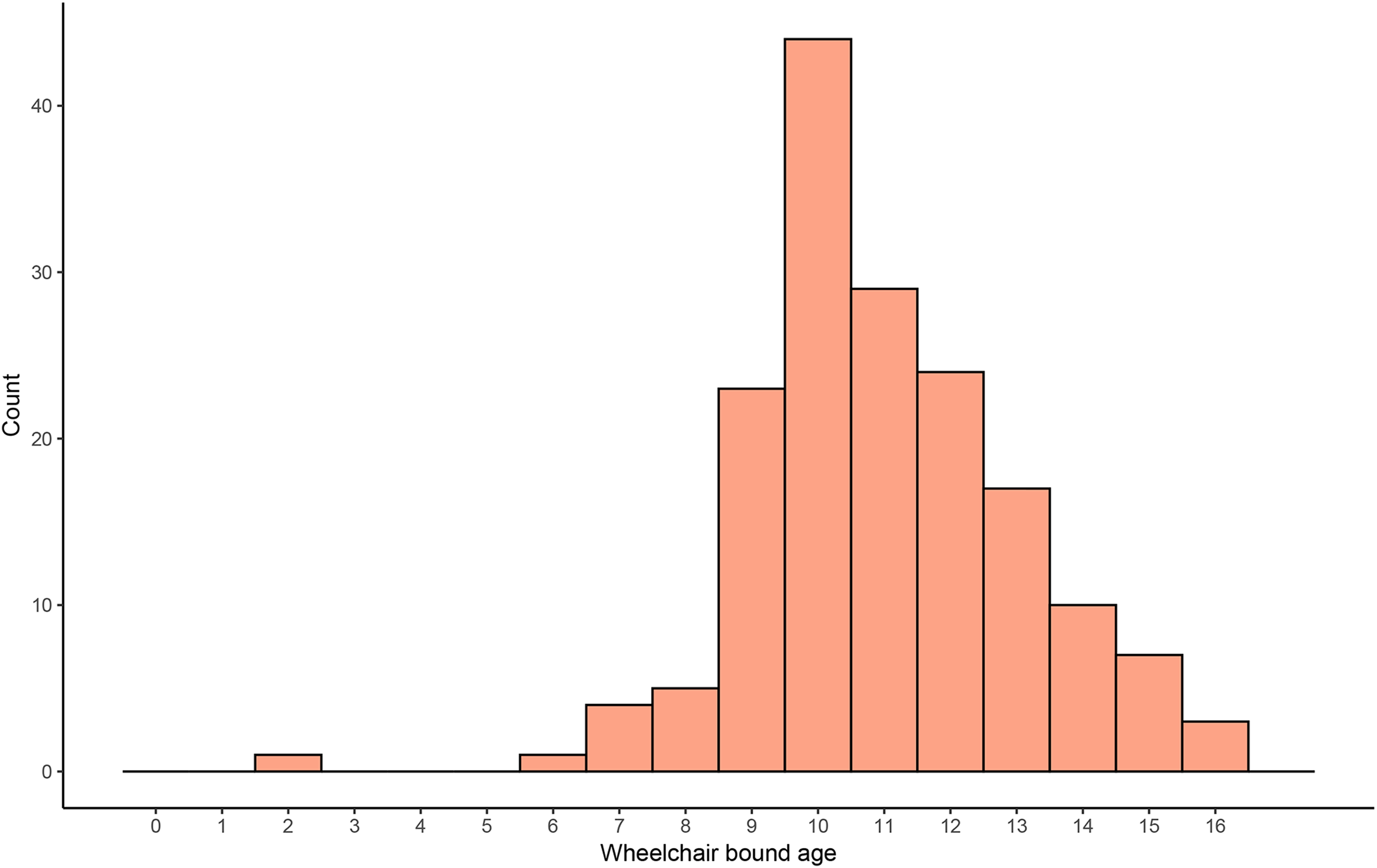
Age distribution of patients with DMD bounding to wheelchair.
Respiratory management
Of the 168 patients, 161 required mechanical ventilation support. Most patients (151 (93.8%)) required mechanical ventilation using non-invasive ventilation (NIV), while the remaining 10 (6.2%) required invasive ventilation through tracheostomy. The reasons for using invasive ventilation were as follows: out of the 10 cases, five received tracheostomy due to respiratory failure caused by aspiration pneumonia, two reported breathing difficulties with uncontrolled hypercapnia despite the use of NIV, one failed extubation following severe pneumothorax, 1 decided to maintain tracheostomy due to recurrent seizures, and 1 failed extubation after respiratory failure following peritonitis.
Among the 161 patients requiring ventilatory support, the age at initial ventilatory support was 19.8 ± 4.3 years. For patients with NIV, the average age was 29.6 ± 5.8 years, and the average hours of use per day was 15.4 ± 7.0. Patients with invasive ventilation had an average age of 32.7 ± 8.1 years, and 24-h ventilatory support was necessary (Figure 4).
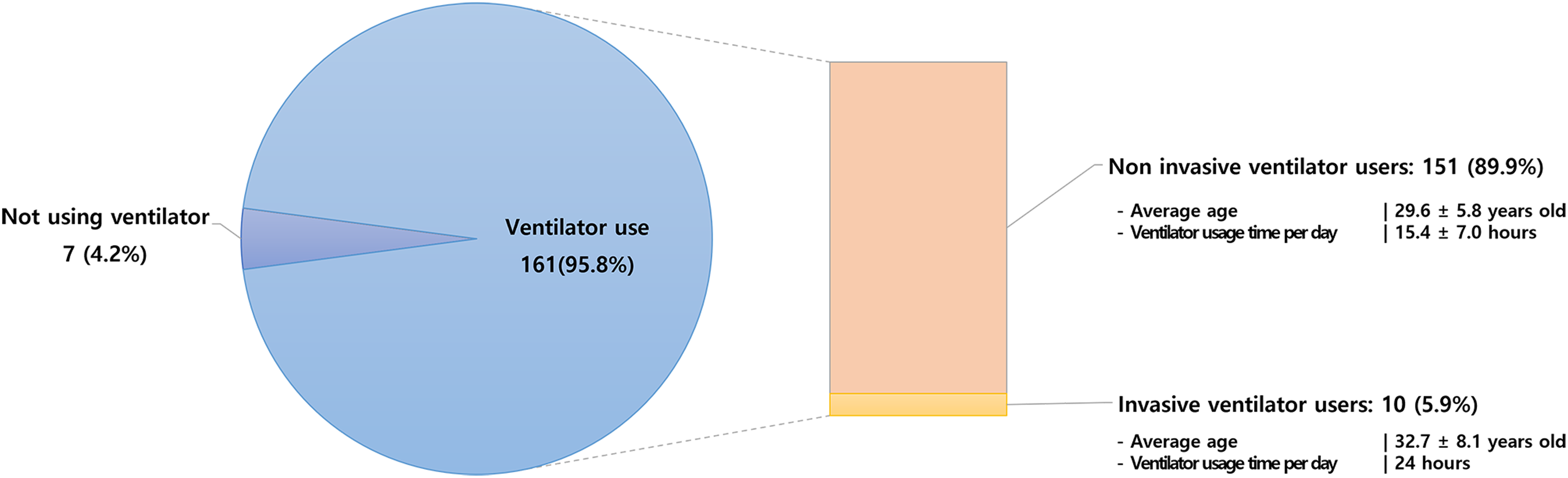
Usage status of mechanical ventilator.
Cardiac management
Except for 12 patients for whom echocardiographic results were unavailable because of follow-up at another hospital, we assessed the left ventricular ejection fraction (LVEF) of 156 patients. The LVEF results for different age groups were as follows: for those aged 20 or older but less than 25, LVEF was 47.4 ± 13.5%; for those aged 25 or older but less than 30, LVEF was 45.4 ± 14.4%; for those aged 30 or older but less than 35, LVEF was 40.0 ± 14.2%; for those aged 35 or older but less than 40, LVEF was 40.7 ± 13.0%; and for those aged 40 or older, LVEF was 39.6 ± 15.8%. There were no statistically significant differences between the groups (Figure 5).
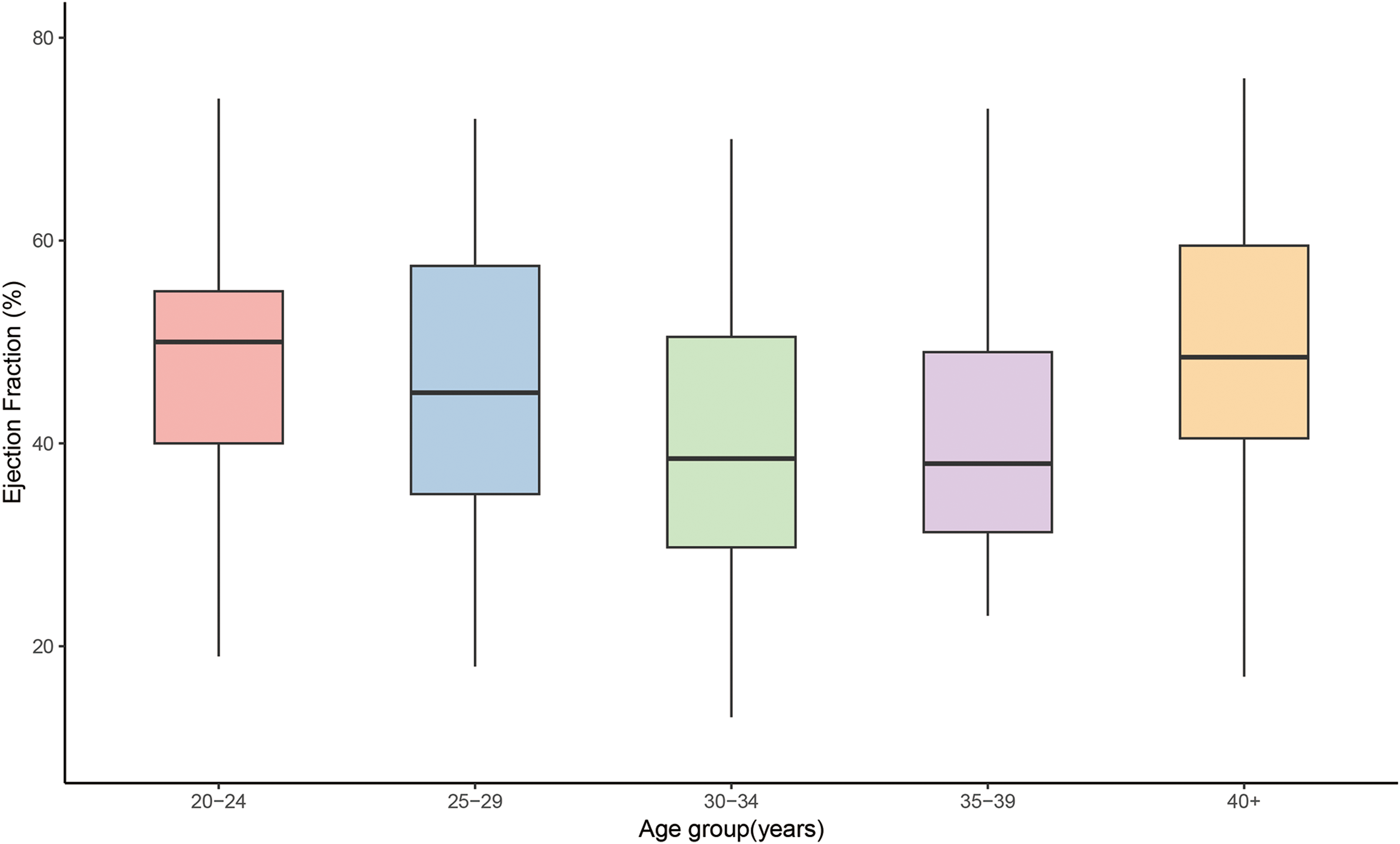
Mean ejection fraction of patients with DMD according to age.
Of the 168 patients, 28 (17.9%) were not receiving medications for cardiomyopathy. Among these, one patient had voluntarily discontinued their medication. The remaining 27 patients had preserved heart function with a LVEF above 50%. All patients were under the annual care of cardiologists specialized in DMD-related cardiomyopathy. 14
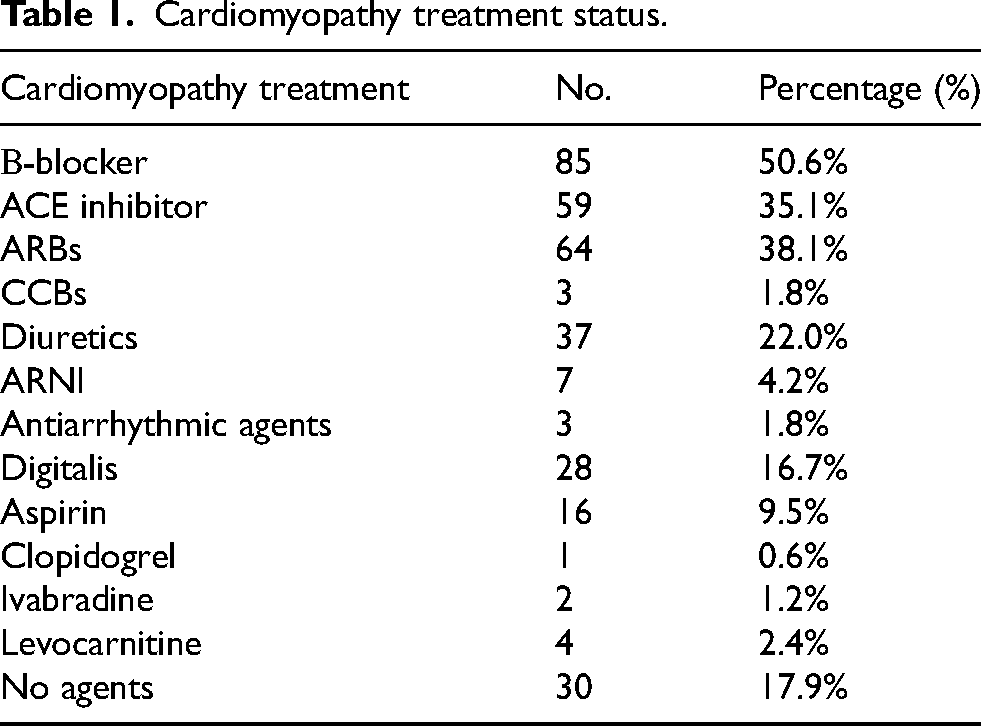
When cardiac medications were prescribed, multiple types were often used concurrently. Beta-blockers were most commonly used, with 85 (50.6%) patients using them. Additionally, angiotensin-converting-enzyme (ACE) inhibitors were used by 61 (35.1%), angiotensin receptor blockers (ARBs) by 64 (38.1%), calcium channel blockers (CCBs) by 3 (1.8%), diuretics by 37 (22.0%), angiotensin receptor neprilysin inhibitor (ARNI) by 7 (4.2%), antiarrhythmic agents by 3 (1.8%), digitalis by 28 (16.7%), aspirin by 16 (9.5%), clopidogrel by 1 (0.6%), ivabradine by 2 (1.2%), and levocarnitine by 4 (2.4%) patients (Table 1). Three patients (1.8%) had an ICD.
Cardiomyopathy treatment status.
Osteoporosis management of patients with DMD
Excluding seven individuals who could not undergo bone mineral density measurement due to severe lumbar spine deformities or the insertion of instruments during scoliosis surgery, the average bone mineral density of 161 individuals was 0.60 ± 0.22 (g/cm2), Z-score −3.3 ± 1.9.
Bone mineral density and Z-scores varied by age group as follows (Figure 6): ages 20–24 had bone mineral density of 0.56 ± 0.24 g/cm^2 (Z-score: −4.1 ± 2.3), ages 25–29 showed 0.61 ± 0.22 g/cm^2 (Z-score: −3.3 ± 1.9), ages 30–34 reported 0.55 ± 0.18 g/cm^2 (Z-score: −3.3 ± 1.4), ages 35–39 had 0.64 ± 0.16 g/cm^2 (Z-score: −2.4 ± 1.4), and those 40 and older presented with 0.77 ± 0.23 g/cm^2 (Z-score: −1.4 ± 1.6) (Figure 6).
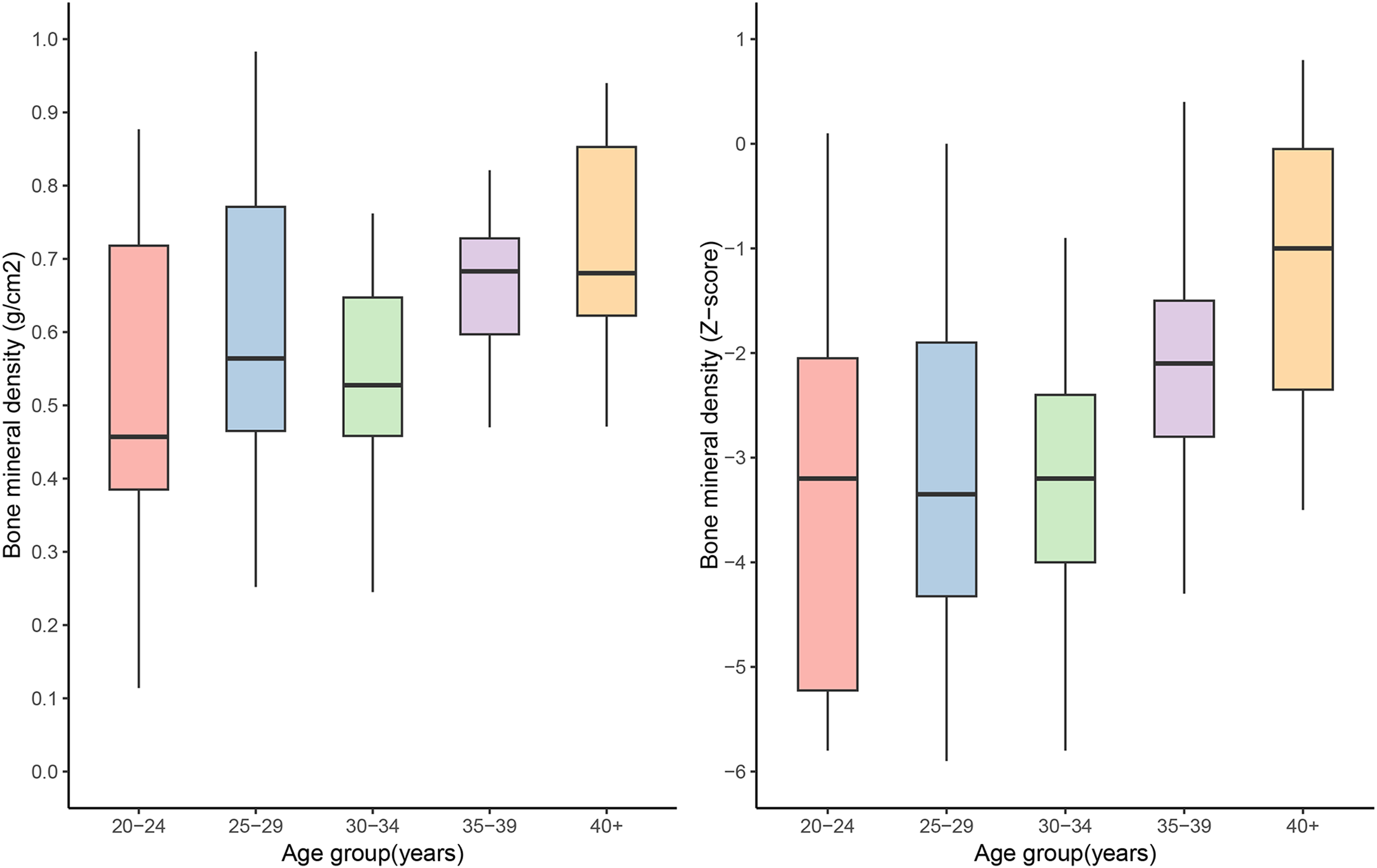
Bone mineral density and Z-score of patients with DMD according to age.
Osteoporosis medications were as follows: calcium supplements by 73 individuals (43.5%), vitamin D by 147 individuals (87.5%), and bone resorption inhibitors by 118 individuals (70.2%).
Steroid use, and gastrointestinal, hepatic, renal, and neurological management in patients with DMD
Twenty-seven patients were receiving corticosteroids, while the remaining 141 were not using steroids at the time of the study. The mean age of patients on steroids was 23.8 ± 3.7 years, whereas the mean age of those not using steroids was 30.5 ± 5.8 years. Ninety-two patients (54.8%) were using anti-constipation medications due to constipation, such as probiotics, magnesium oxide, or Dulackhan syrup. According to the radiology specialist's interpretation, nearly all the patients exhibited signs of bowel distension or ileus on the abdominal X-ray.
Twenty-eight patients (16.7%) were taking medication such as ursodeoxycholic acid or carnitine complex (GODEX®) due to elevated AST/ALT and gamma-glutamyl transferase.
For nephrological management, 17 individuals (10.1%) had a history of urinary or kidney stones, three had chronic kidney disease, and one of them was undergoing dialysis (Table 2). We tried to assess the estimated glomerular filtration rate (eGFR) using cystatin C. Excluding the six patients who did not undergo eGFR testing by cystatin C, the distribution of patients based on their eGFR was as follows: one patient had an eGFR less than 15 mL/min/1.73 m², three patients had an eGFR between 15 and less than 30 mL/min/1.73 m², two patients had an eGFR between 45 and less than 60 mL/min/1.73 m², and 21 patients had an eGFR between 60 and less than 90 mL/min/1.73 m². Additionally, there were 135 patients with an eGFR of 90 mL/min/1.73 m² or above.
Status of other treatment of patients with DMD.
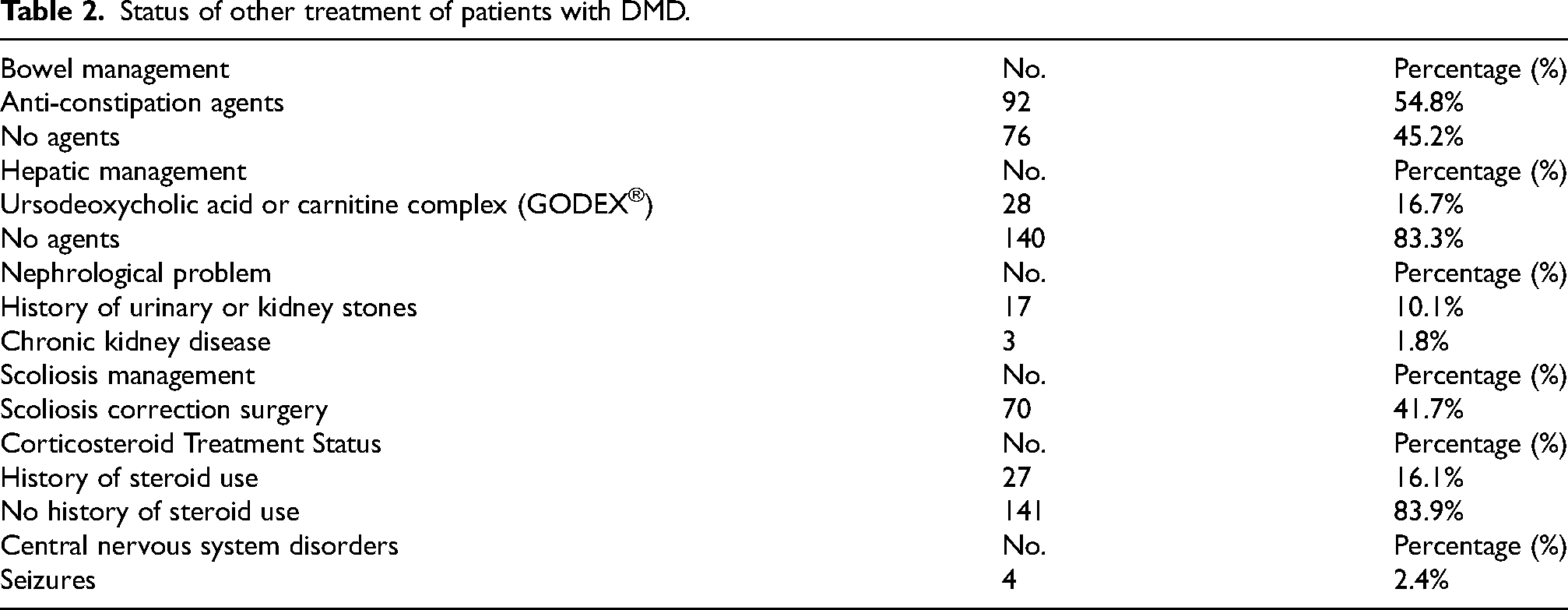
Figure 7 shows the scatter plot and trend line of eGFR values in relation to age for individuals. The negative slope of the trend line indicates a gradual decline in eGFR with increasing age, with the linear regression analysis yielding a statistically significant relationship (
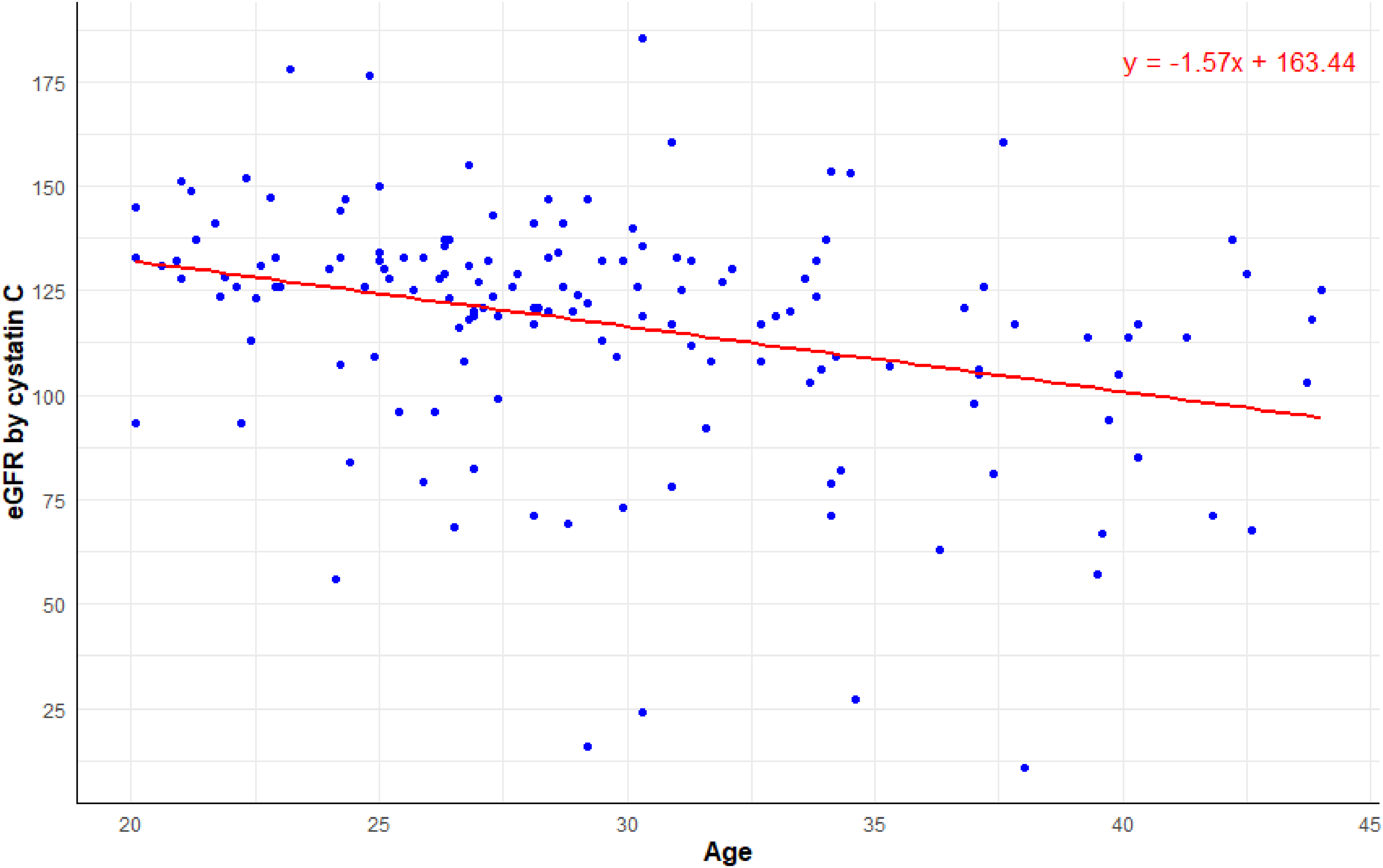
Relationship between age and eGFR by cystatin C.
Seventy patients (41.7%) underwent scoliosis correction surgery. Four patients (3.0%) had a history of seizures (Table 2).
Discussion
This study investigated the current multidisciplinary management of Korean adult patients with DMD, aiming to examine the current status of management for this patient group. Due to advancements in cardiopulmonary interventions,15,16 lifespan of patients with DMD continues to increase.17–19 One study reported that the average lifespan of patients with DMD not using respiratory support was 19.0–19.4 years, while those using respiratory support had an average lifespan of 29.9–31.8 years, demonstrating an extension in lifespan due to respiratory support. 20 The increased lifespan of patients with DMD underscores the importance of managing their overall health and quality of life. With the significant increase in life expectancy, the management of adult patients with DMD has become a crucial issue, and complications that may arise and the corresponding treatment are increasingly prominent for adult patients with DMD. In Korea, government funding for the provision of mechanical ventilators to patients with DMD 21 has significantly contributed to an increase in their lifespan. Our research indicates that 39.2% of adult patients with DMD were aged 30 years or above, and 7.1% were aged 40 years or above, emphasizing the importance of effective management for aging patients with DMD.
Cardiopulmonary intervention is particularly crucial for patients with DMD. Respiratory muscle weakness was the primary cause of death in DMD in the past; however, the use of mechanical ventilation and assisted cough techniques has reduced hospitalization rates and dramatically improved survival rates in patients with DMD. 22 Recently, guidelines for respiratory management based on disease stage have been introduced, with most patients with DMD being adequately managed with NIV. 8 Our study yielded similar results. Almost all patients (approximately 95%) were found to be using ventilatory support, and other patients, mostly in their early twenties, also have a high likelihood of soon requiring respiratory support. The average age of initiation of ventilatory support was reported as 19.8 ± 4.3 years, consistent with previous research. 23 Most patients used NIV, even in cases requiring 24-h respiratory support. However, certain patients are advised to consider invasive mechanical ventilation in instances of failed extubation, non-invasive mechanical ventilation failure, or when managing secretions becomes challenging because of weakened bulbar muscles. 24 As individuals age, those risks are expected to increase. In our study, a total of 10/161 (6.21%) patients required invasive ventilation. Although not a high percentage, it provides insight into the probability of using invasive ventilation among older individuals diagnosed with DMD.
Management of cardiomyopathy in patients with DMD has become increasingly crucial with advancing age. In this study, beta-blockers were the most commonly used medications for heart disease management, followed by RAS inhibitors and diuretics. These proportions closely resembled the findings of other studies. 1 Previous research has reported that the EF decreases by approximately 3% every two years. 23 Our study showed a trend of decreasing EF with age; however, this trend was not observed in patients aged over 35 years. Such findings may reflect a bias toward only relatively healthy individuals with DMD who can survive.
In our study, 28 patients were not receiving heart failure management. Previous studies suggest that initiating ACE inhibitors in asymptomatic boys with normal left ventricular systolic function as they approach 10 years of age can improve long-term cardiac outcomes. The 2014 NHLBI working group recommended use of ACE inhibitors or ARBs by the age of 10 years in boys with DMD. 25 However, the decision to start medication must be carefully weighed by cardiac specialists. In our institution, DMD patients are managed by a cardiologist who specializes in DMD-related cardiomyopathy. Annual TTE, 24-h Holter monitoring, and regular checks of cardiac markers, including Troponin T or I, BNP or NT-proBNP, guide the timely initiation of treatment. In the case of the 28 patients not receiving heart failure medication, all had LVEF above 50% and showed no significant BNP elevation, which led to the decision to forgo cardiac medications.
As individuals with Duchenne muscular dystrophy age, congestive heart failure often worsens, potentially resulting in complications, such as severe left ventricular dysfunction and associated arrhythmias. In such cases, ICD can be a viable solution. In our study, ICD insertion was performed in three patients: two underwent insertion due to complete AV block and one due to recurrent ventricular tachycardia. All these individuals exhibited severe left ventricle dysfunction. Research based on these recommendations has shown that the use of ICD in patients with DMD with severe left ventricular dysfunction and cardiomyopathy increases survival rates and reduces complications. 26
Corticosteroid therapy is recommended not only for ambulatory DMD patients but also for those in the non-ambulatory stage. 2 However, a considerable number of present patients had not received oral corticosteroid treatment. Several factors contribute to this. In Korea, the use of NIV for DMD patients began approximately 20 years ago with our center, but it took a long time for its widespread adoption, supported by government initiatives. 27 Prior to that, and for some time afterward, many medical professionals viewed DMD patients as “hopeless,” leading to a lack of proactive treatments, including corticosteroid use. Moreover, while the importance of corticosteroid therapy has been increasingly supported by evidence, it has taken time for widespread adoption. Another reason for the relatively low usage rate in our cohort is that many patients began visiting neuromuscular special hospital at an older age, after already transitioning to NIV. At this stage, there are concerns that the risks of corticosteroid use, particularly its impact on bone health, may outweigh its benefits. Another reason for the relatively low usage rate in our cohort is that many patients began visiting neuromuscular specialty centers at a relatively older age, due to issues such as hospital accessibility. As previous research has shown, concerns arise that the risks of corticosteroid use may outweigh the benefits as patients age, 28 particularly due to its impact on bone health. However, as the body of evidence supporting the long-term benefits of corticosteroids continues to grow, it is likely that more adult patients with DMD in Korea will begin to receive corticosteroids. This is further supported by the observation that younger patients are more likely to have a history of steroid use, as reflected by the age difference between those with a history of steroid use and those without.
Generally, individuals with DMD tend to have a lower bone mineral density and an increased risk of osteoporosis. Reduced physical activity owing to muscle weakness can negatively affect bone health. Some individuals with DMD may take medications, such as steroids, which can also affect bone health. Our findings confirmed the presence of osteoporosis and osteopenia in a significant number of patients. As osteoporosis can lead to bone fractures, it is essential to manage this condition. 29 In patients with DMD, the first-line therapy for osteoporosis is IV bisphosphonates, 8 and other treatments include calcium, vitamin D, and testosterone. Adequate calcium intake is recommended as it can slow bone resorption and improve bone health, with a daily intake of 750 mg of calcium recommended for patients with DMD. Vitamin D is also considered essential as it plays a crucial role in calcium absorption in the gastrointestinal tract. 29 Calcium, vitamin D, and anti-resorptive inhibitors such as bisphosphonate and denosumab are often used to treat these individuals. Further research is essential to determine the appropriate use and dosage of bone medications in adult patients with DMD. 30
Another interesting finding regarding bone mineral density was that, when categorized by age group, there was no decrease in bone mineral density with advancing age, contrary to previous studies that have shown a gradual decrease in lumbar bone mineral density as age increases.31,32 The tendency of bone mineral density to remain constant or increase with age could be attributed to the cross-sectional nature of this study. Furthermore, in Korea, the use of IV bisphosphonates is permitted for individuals over 20 years of age due to healthcare insurance policies, which could also contribute to this effect. Another consideration is that patients with better lumbar bone mineral density live longer. To further explore this, a linear longitudinal study involving individual patients is necessary.
In our study, the majority of patients presented with varying degrees of ileus on abdominal X-rays. Notably, 92 patients (54.8%) were on anti-constipation medications. Constipation is a common clinical observation in DMD patients, 33 primarily due to the disease's impact on intestinal smooth muscle, reduced physical activity, and decreased dietary intake.2,33 Our center has developed a tailored approach to manage these symptoms based on clinical experience. Interventions include promoting bowel movement through abdominal massage, administering probiotics, and using magnesium oxide and other anti-constipation medications. Suppositories or enemas are also employed when necessary. In severe cases of gas distention, gastric or rectal tubes are inserted to relieve intestinal gas. Constipation is a common issue for most patients, and symptomatic treatment remains the only option, making it crucial to provide careful, individualized management and care.
Diagnosing hepatobiliary diseases in DMD patients is particularly challenging. Commonly used liver function tests, such as AST and ALT, may not provide accurate screening results in DMD patients, as these enzymes are often elevated due to the underlying muscle degeneration. Additionally, decreased physical activity of DMD likely contributes to biliary stasis, 34 which further complicates the clinical picture. We collaborate with hepatobiliary specialists and use GGT as a screening tool to monitor liver function. However, we recognize the limitations of relying solely on GGT. 35 To overcome this, we are considering additional diagnostic tests, such as ultrasound and fibroscan, to improve accuracy. As this aspect of care has been relatively neglected, we are planning further research to explore these issues in greater depth.
In adult patients with DMD, muscle mass is significantly reduced, making traditional kidney function markers like BUN and creatinine less reliable. At our center, we rely on cystatin C, which is less influenced by muscle mass, to assess kidney function. 36 A substantial portion of our patients exhibited signs of renal dysfunction, with one patient requiring dialysis. Renal dysfunction was found to be correlated with age, and further research is needed to identify other contributing factors to declining renal function in these patients.
One patient who eventually required dialysis was first diagnosed with CKD stage 2 at around the age of 28. A CT scan at that time revealed a right UVJ stone with mild proximal ureter dilation, as well as multiple small Randall's plaques or calyceal stones in both kidneys. Additionally, polycystic kidney disease was observed. This patient was closely monitored by the nephrology team, and by the age of 37, their cystatin C level had risen to 4.74 mg/L, with an eGFR of 11 mL/min/1.73 m², indicating impending ESRD and necessitating the initiation of dialysis. It was suspected that cardiac dysfunction also played a role in the patient's renal decline, as they had severe dilated cardiomyopathy with an EF of 12%. Although there were initial concerns about starting dialysis by the nephrology team, the patient expressed a strong will to live. Now, two years after starting dialysis, the patient continues to live well.
Even in specialized hospitals that manage a large number of DMD patients, there is still a tendency among some healthcare professionals to view DMD patients as ‘hopeless’ cases, avoiding proactive treatment approaches. However, as the life expectancy of DMD patients continues to increase, there is an urgent need to shift the focus from merely extending lifespan to improving the quality of life and managing complications effectively. This requires a comprehensive interdisciplinary approach that goes beyond the scope of muscular dystrophy specialists and involves collaboration with various medical fields.
This study has some limitations. First, it focused on patients with DMD who visited a single institution. However, the Pulmonary Rehabilitation Center of [blinded for review] is a specialized referral center for patients with neuromuscular diseases. Considering the prevalence of DMD in Korea, it is estimated that approximately 2000 individuals have DMD. Excluding pediatric patients, the 168 adult patients with DMD in this study can be considered reasonably representative. Nevertheless, a comprehensive worldwide analysis is necessary for holistic management in the future. Another limitation of this study is the inclusion of only surviving patients with DMD at a specific point in time, which may introduce bias in data interpretation. However, as the primary objective was to assess the current care status of patients with DMD, this limitation was not considered a significant concern.
Conclusion
This study emphasizes the critical importance of a multidisciplinary approach to managing adult patients with DMD, highlighting the need for personalized care strategies for this aging group. While advances in respiratory and cardiac care have notably improved life expectancy, an increase in lifespan has made the management of other conditions increasingly vital. Our findings suggest the need for ongoing research and the development of comprehensive care protocols aimed at optimizing health outcomes and improving the quality of life of adult patients with DMD.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mokhoon Foundation under Fursys. The funder had no role in the design of the study, data collection, analysis, interpretation of data, or in writing the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Datasets/data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data is not publicly available due to privacy or ethical restrictions.