
Abstract
Background:
Myotonic Dystrophy type 1 (DM1) is a slowly progressive hereditary neuromuscular disorder affecting several organ systems including the musculoskeletal system.
Objective:
To examine the effects of rehabilitation technology on arm and hand function in the assessment and treatment of adults with DM1 with moderate to severe muscle impairment.
Methods:
A single subject experimental design study (SSED) with 6 participants. The assessments were done weekly through remote study assessments using the video-conference system Whereby®. Participants performed the nine-hole peg test (NHPT), active range of motion (AROM) of the shoulder and patient reported outcome measures (PROMS). Three participants also measured grip and pinch strength and performed the Nut and Bolt task. The intervention was a three-week in-patient rehabilitation stay with the use of rehabilitation technology for exercising arm and hand function. Exercises were performed in AMADEO and the ArmeoSenso. The participants exercised the upper extremities for 30 min 5 times a week.
Results:
Improvement on the NHPT test on the dominant hand were found for five of the six participants. Three of six improved on the non-dominant hand and in AROM. Two of the three participants that measured pinch and grip strength improved, and all three improved on the Nut and Bolt task. Self- reported function, myotonia and fatigue remained stable. All participants were able to participate in video assessments.
Conclusions:
Impairment in arm- and hand function affects independence in people with DM1.Our findings suggest that exercising arm- and hand using rehabilitation technology may have a positive effect on function measured by dexterity, strength, and movement in DM1. There is a need to study the effect of exercise on arm- and hand function in DM1 in larger studies. The use of video-consultations can be a supplement in assessment of people with neuromuscular conditions in research and clinical practise.
Introduction
Myotonic Dystrophy type 1 (DM1) is the most common hereditary neuromuscular disorder (NMD) in adults. 1 This slowly progressive autosomal dominant disorder is heterogeneous with a high degree of phenotypic variability. 2 Symptoms of DM1 can manifest at all life stages, from birth to late adult life. 1 In addition to motor symptoms, such as myopathy and myotonia, DM1 affects a multitude of organs and functions. 1 Fatigue and excessive daytime sleepiness are common symptoms that may impact the possibility of participation in exercise and rehabilitation programs. 3 Hand myotonia and weakness in fingers and elbow extensors are often initial motor signs. 2 Contractures in the upper extremities are not common but might occur late in the disease especially in the shoulder and elbow. 4 Reduced arm- and hand function is an important but sometimes neglected motor affection of DM1. Impairment in the musculoskeletal system can be measured using the muscular impairment rating scale (MIRS). 5 The MIRS was developed to assess disease progression in DM1 and has been shown to be a valid and reliable measurement. 5 MIRS is graded from one (no muscle impairment) to five (severe proximal muscle impairment). 5 Neck and trunk flexors are often affected early in DM1, 6 and an impaired trunk stability may influence the ability to move the arms in a functional manner. A significant decline in both dexterity and grip and pinch strength over a nine- year period has been found in people with DM1. 7 Reduced arm- and hand strength will affect the ability to perform personal hygiene and daily activities. 8 To support self-reliance and independence, there is a need to explore treatments and exercises that improve or maintain muscle function.
Exercise
Exercise in muscular dystrophies, including DM1, were previously considered to be potentially harmful but is now recommended when performed in a moderate and safe way. 9 Strength training and aerobic exercise may be beneficial, but more research is needed.9,10 One study found that physically active people with DM1 have better hand- and elbow strength compared to those that are inactive. 11 Previous research on DM1 suggests that moderate intensity strength exercises and endurance training is safe and might improve body functions and activity levels. 12 Increased muscle strength and endurance have been reported in several studies 12 and might increase activity and participation for people with DM1. 13 Two studies have examined the effect of hand training with moderately positive results.14,15 One scoping review concludes that there is a research gap on the effects of exercise of arm- and hand function in DM1. 12
Rehabilitation technology
Rehabilitation technology refers to technology used in treatment and rehabilitation, and includes gaming technology and computer games, equipment for training motor skills and for measuring movements. 16 Applying technology in rehabilitation have influenced treatment effects such as improvement of activities of daily living, arm function and muscle strength in various neurological conditions.17,18 However, the number of studies is limited, and the quality of evidence is low. Research on the effects of rehabilitation technology in upper limb function is increasing. 19 Most of the studies have been on people with stroke, 18 spinal cord injury, 20 and multiple sclerosis.21,22 A systematic review on the use of rehabilitation technology in upper limb motor recovery, concludes that few studies have been performed on NMDs. 17 However, a few pilot studies and case reports exist.23–25 The overall advantage of using rehabilitation technology is the potential to increase the dose of exercise for the individual. 18 However, it is not considered superior to human provided therapy. 18 Telehealth is using digital information and video consultations to provide health care regardless of time or distance. 26 The COVID-19 pandemic increased the use of video consultations. 27 There is some evidence supporting telehealth for assessment in the management of neurological conditions, 26 and a few studies have explored the use of telehealth in NMDs.28,29 One study on remote assessment of DM1 found that video consultations were feasible for data collection when evaluating muscle function and patient reported outcome measures (PROMS). 30 The use of video consultations for assessments increases the possibility for people to participate in research not limited by proximity to the research facility. The primary aim of this study was to examine the effects of technology assisted rehabilitation on arm and hand function in adults with DM1. Our hypothesis was that daily exercise with rehabilitation technology could improve arm and hand function in DM1.
Materials and methods
Design
This is a single subject experimental design study (SSED). SSED is well-suited for studies of small and heterogeneous populations in which it may be challenging to recruit enough participants for a randomized controlled trial. 31 A SSED study is a prospectively conducted study including controlled manipulation through an experimental design. 32 In SSEDs, participants are their own controls, thus controlling for confounding factors. 31 DM1 is a rare and heterogeneous disorder, and there is little knowledge of the effect of rehabilitation technology on arm- and hand function. We found SSED to be an appropriate design in the present study. SSED is characterized by measuring the outcome repeatedly in individual participants through the different phases of the study. 31 The participants go through a series of baseline measures before the experiment starts, followed by a series of measurements during the intervention phase. 32 We used a study period of 7 weeks for each participant and assessed them once a week using video consultations at eight timepoints (Figure 1). The study period had three phases: the baseline period (A1), the intervention period (B), and the follow-up period (A2). The baseline period (A1) and follow up period (A2) both lasted for two weeks, with three and two video assessments respectively. The participants were instructed to carry on with their normal life in these phases of the study.
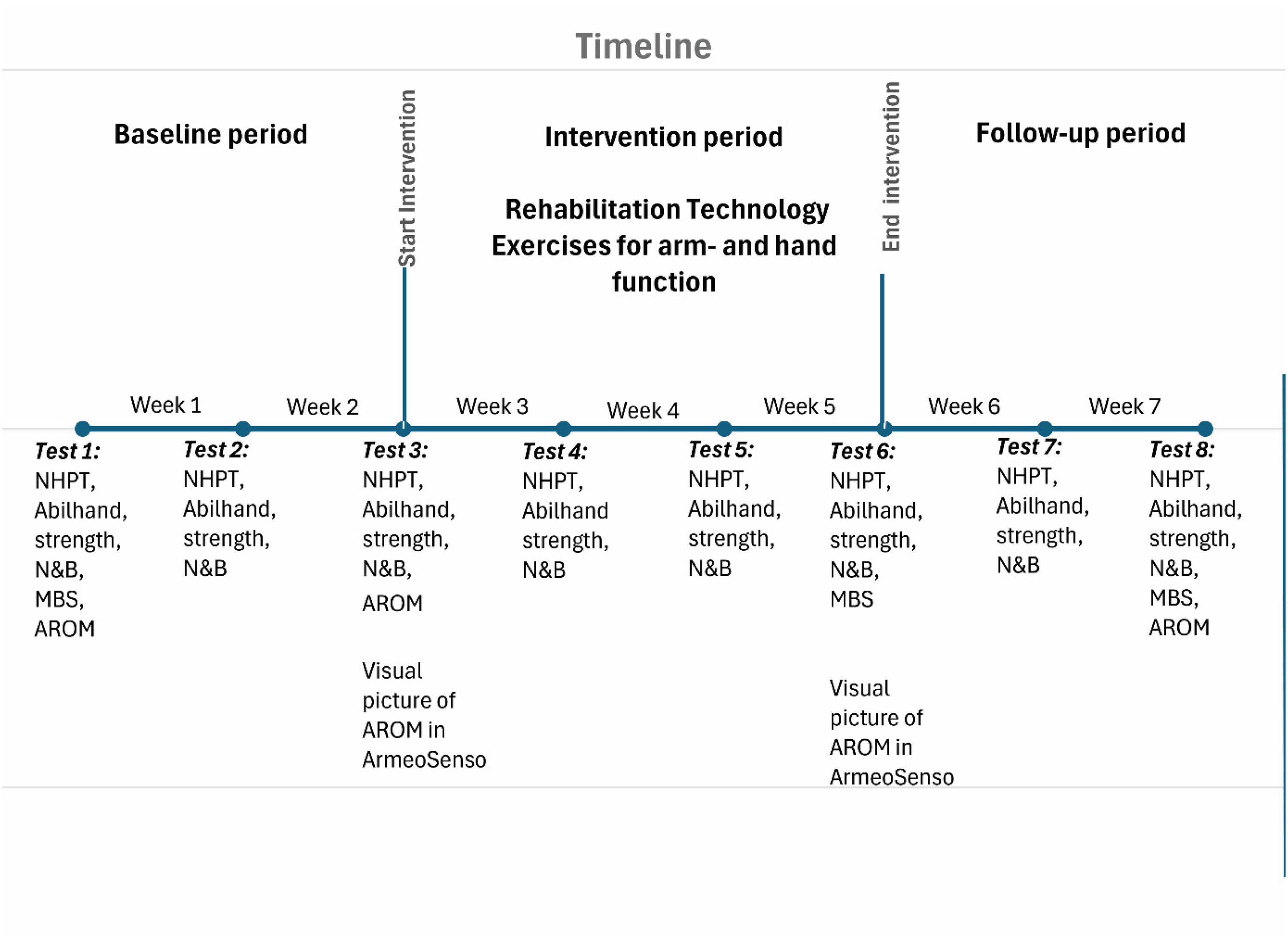
Study timeline for the individual participant.
The intervention period (B) lasted for three weeks during an in-patient rehabilitation stay at Vikersund Rehabilitation Centre, Norway. The participants underwent three video assessments during this period. The intervention was exercising the arm- and hand function in two rehabilitation technology devices, the AMADEO and the ArmeoSenso. Both devices use computer games, developed to motivate participants and to make the training more fun, thereby possibly increasing the exercise amount. The participants exercised five times per week. They trained both arms and hands in each session, or alternated between arm and hand exercises every other day. Each session lasted for max 30 min, although some of the more affected participants would end their sessions after 20 min. Assistance during the training sessions was given by a physiotherapist or an occupational therapist experienced in treatment of rare NMDs. Hand exercises were performed in AMADEO, a hand robot connected to a computer, where the participant actively moved the fingers to control the motions in the video games. 33 The exercises focused on active finger flexion and extension with resistance. 19 The AMADEO can assist in part of, or the whole range of motion if the participant lacks full active movement. In research the AMADEO has primarily been used in stroke rehabilitation,34,35 but as it trains finger strength and various aspects of grasping in general it might be beneficial for other patient populations in need of upper limb rehabilitation. 19 Arm function was exercised in the ArmeoSenso. Movement sensors, attached to the arm and the chest of the participant, communicate with the computer. 36 The computer games are designed to exercise different movements of the arm at different difficulty levels. Initial examination of range of motion in the ArmeoSenso was used to guide the selection of games and exercises for each participant.
Participation criteria
Inclusion criteria for participation in the study was a genetically confirmed diagnosis of DM1, age above 18 years and being approved a rehabilitation stay at Vikersund Rehabilitation Centre. Exclusion criteria were no muscle impairments (a MIRS score of 1), reduced cognitive function or being unable to participate in the technological rehabilitation and the digital evaluation.
Assessments and measurements
All participants were assessed in weekly consultations using the video conference system Whereby®. The participant received a link to the video consultation and logged on with their smartphone, tablet or laptop to a live evaluation with an assessor. The participants had received the testing equipment, sent by mail to their home, and they used this to perform the assessments. The participants were assessed on functional tests and PROMS. The assessor asked the questions and noted the answers to the PROMS, watched and timed the participant performing the dexterity test. On the strength measurements the participant were instructed on how to perform the test and show the digital measurement to the camera for the assessor to document.
The following instruments were used: The Nine Hole Peg Test (NHPT) as a measure of fine motor dexterity. 37 The NHPT has been validated for DM1 38 and is recommended as a standardized measure to assess dexterity in DM1. 39 In the NHPT the participants insert nine pegs, one at the time, into the pegboard. Thereafter the pegs are removed, one at the time. The insertion and removal of the pegs are done as quickly as possible, and the test is timed in seconds by the assessor. 37 Both hands were measured once at each assessment, with one trial before the first assessment. The Abilhand-NMD is a PROM designed to measure the ability to use the hands in manual activities in people with neuromuscular disorders. 40 It consists of 22 items, 18 of which to be answered by adults. The Abilhand-NMD has been translated to Norwegian and reliability tested for DM1. 41 The assessor asked the participants to score the difficulty of performing each of the tasks and registered the answers. We used Abilhand-NMD to assess the participants’ perceived difficulty in performing activities that require the use of the hands. The participants answered the PROMIS29 questionnaire at baseline before start of the intervention and after the intervention was finished. The PROMIS29 is a questionnaire translated and validated in Norwegian asking about seven health domains. 42 In this study, we report the results from the fatigue and sleep disturbance sections.
To measure shoulder movement, we used the Active Range of Motion (AROM) of shoulder flexion and abduction. AROM was measured twice in the baseline period and once at the end of the study, using the app Angulus in the video assessments. The participants displayed their active shoulder abduction with their front to the camera, and their shoulder flexion with their side to the camera in a standing or sitting position. The assessor took a picture at their maximum range and used this picture to calculate the AROM in the Angulus app. The fulcrum of the digital goniometer in the Angulus app was placed in the centre of the glenohumeral joint, the proximal arm parallel to the midaxillary line of the thorax and the distal arm aligned with the midline of the humerus. This was used to calculate the participants AROM in degrees. In addition, AROM was measured on arrival to and departure from the rehabilitation centre by the therapist using the ArmeoSenso giving a visual picture of the range of motion. The AROM measured by ArmeoSenso became decisive in selecting the various exercise games. Active and passive range of motion in the fingers were assessed clinically by the therapist and in the AMADEO. In the AMADEO active ROM is measured as percentage of the passive ROM (0–100%). To assess myotonia, we used The Myotonia Behaviour scale. The participants answered this at the baseline assessment, at the end of the intervention and at the end of the study. This is a scale from zero which is no muscle stiffness to six which is incapacitating stiffness. 43 A score of one or two indicate some myotonia, not limiting daily activities. A score of three indicate that myotonia impacts some activities, and a score of four indicate that myotonia impacts all activities of the participant.
After the first three participants had completed the study, we decided to add some additional outcome measures: grip strength, finger strength and the Nut and Bolt task. Feedback from these participants and their physiotherapist/occupational therapist made us realize we were missing measurements on some important functions. We therefore decided to add measurements of muscle strength and an additional hand dexterity test to the study. Hence, we tested grip strength, pinch gauge and the Nut and Bolt task for the last three participants. Grip Strength was measured by the Jamar digital dynamometer. 44 The participants were instructed to sit with their elbows in 90 degrees of flexion and the underarm in a neutral position. Strength was measured twice on each hand and the average value in kilogram was reported. We also measured Finger strength by the Jamar digital pinch gauge. 8 Strength was measured twice on each hand and the average value in kilogram was reported. We also included The Nut and Bolt Task, a measure of fine motor dexterity originally designed as a simple test of hand and finger dexterity in Huntington's disease. 45 During the video assessments the participants were asked to hold the bolt with one hand and screw the nut onto the bolt with the other. The nut was placed at the bottom of the bolt before starting and we measured the time (in seconds) the participant used from starting to screw until the nut reached the top of the bolt. The task was performed with both hands and with two different sized nuts and bolts (small and large). The participants were allowed to support their elbows if needed. They were instructed not to flick the bolt but use a turning motion to screw the bolt onto the nut and were allowed to change the grip during the task if wanted.
Data analysis
Methods for analysing data in SSED studies include visual analysis to determine the change in the individual participants’ score throughout the study period. 46 Visual analysis of the NHPT, Nut and bolt test, and muscle strength were conducted by plotting the scored values for each test at each time point into Microsoft Excel. Mean values were calculated for the baseline period, the intervention period, and the follow-up period. Based on this, the mean shift, the trend, and the overlap were calculated. The mean shift is the difference between the means of the measurements in the baseline and the intervention period respectively. 47 A change in the mean between the two periods can indicate an improvement or deterioration of the function measured. 32 Trend is the direction of the curve, where two or more of the measures goes in the same direction. A positive trend will be if the measurements in the intervention phase (two or more) are better than the mean value for the baseline phase. Overlap is improved (or deteriorated) where two or more of the measures (more than 50%) in the intervention period differs from the baseline period. 47 Visual analysis of the change of AROM from the beginning to the end of the intervention period was conducted by the ArmeoSenso. This shows the difference in active range in shoulder abduction (frontal plane), flexion (sagittal plane) and horizontal adduction (transversal plane).
Ethical considerations
When studying small samples of individuals with rare diseases, it is a risk that participants might be identified. To reduce this risk, we present general information about the participants as a group, and we have avoided linking the personal information to the results of the individual participants. The study has been approved by the Regional Committees for Medical and Health Research Ethics and the Norwegian Agency for Shared Services in Education and Research (#256361). The study is registered in clinical trials (no. NCT05560438).
Results
Participants
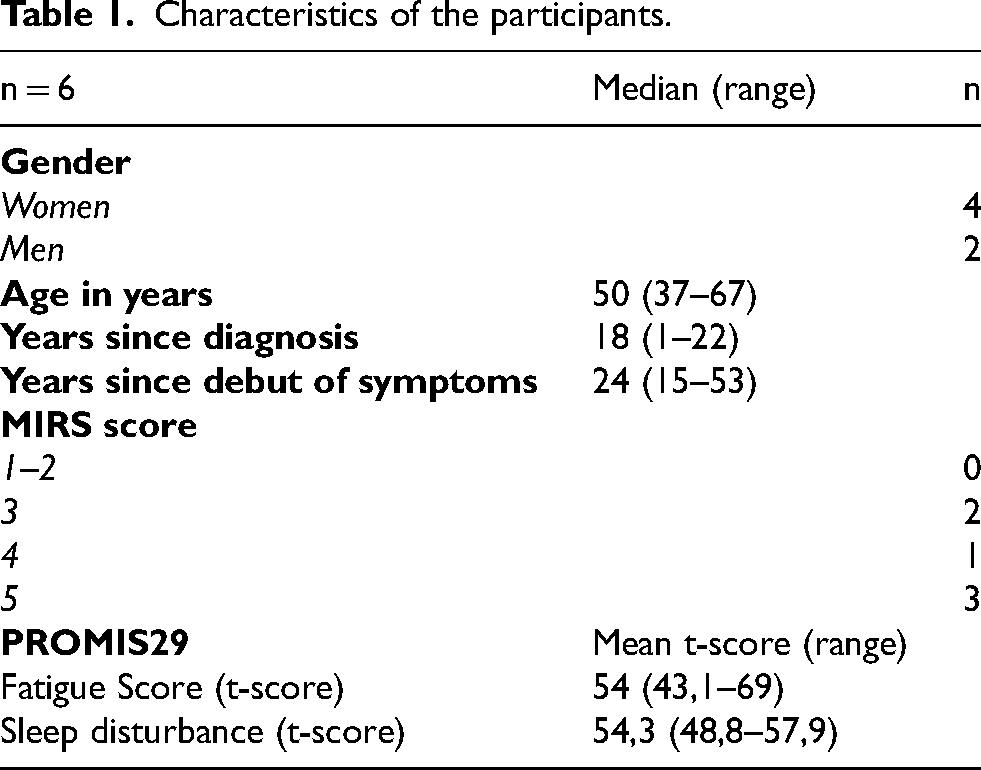
Eight adults with a confirmed DM1 diagnosis were included in the study. Two participants withdrew from the study before the intervention period started due to other health conditions. Among the six completing the study there were four women and two men, median (range) age 50 (37–67) years (Table 1). Two of the participants had only distal weakness, with a MIRS score of three, one had mild to moderate proximal weakness with a MIRS score of four and three participants had severe proximal impairment with a MIRS score of five. The participants had a slightly higher fatigue and sleep disturbance t- score at baseline compared to the normative data in PROMIS29 where a t-score of 50 is the mean (Table 1). Two of the participants did weekly physiotherapy sessions outside the intervention period, two performed structured exercise on their own and two had no regular exercise routine in the baseline and follow-up period. The two participants receiving regular physiotherapy outside the study had severe muscle impairment in their lower extremities and the physiotherapy was primarily focused on their balance and lower limb function. None of the participants were on anti- myotonic drugs or any other drugs influencing the exercise treatment or treatment effects.
Characteristics of the participants.
Nine hole peg test (NHPT)
All the participants were able to perform the NHPT during the video assessments. The calculated mean shift, trend and overlap indicated a positive change on the NHPT in the dominant hand in five of the six participants (Table 2). The size of the mean shift varied and, although positive, were in some instances small. We also found a positive change on the non- dominant hand in three of the six participants. In the visual analyses, we found large variability between and within the participants. Some were stable in the baseline phase assessments while others showed highly variable results within the baseline assessments. We found an improvement in participants 3, 4 and 5 on both hands on the NHPT, and especially participant 4 and 5 showed gradual improvement during the intervention (Figure 2).
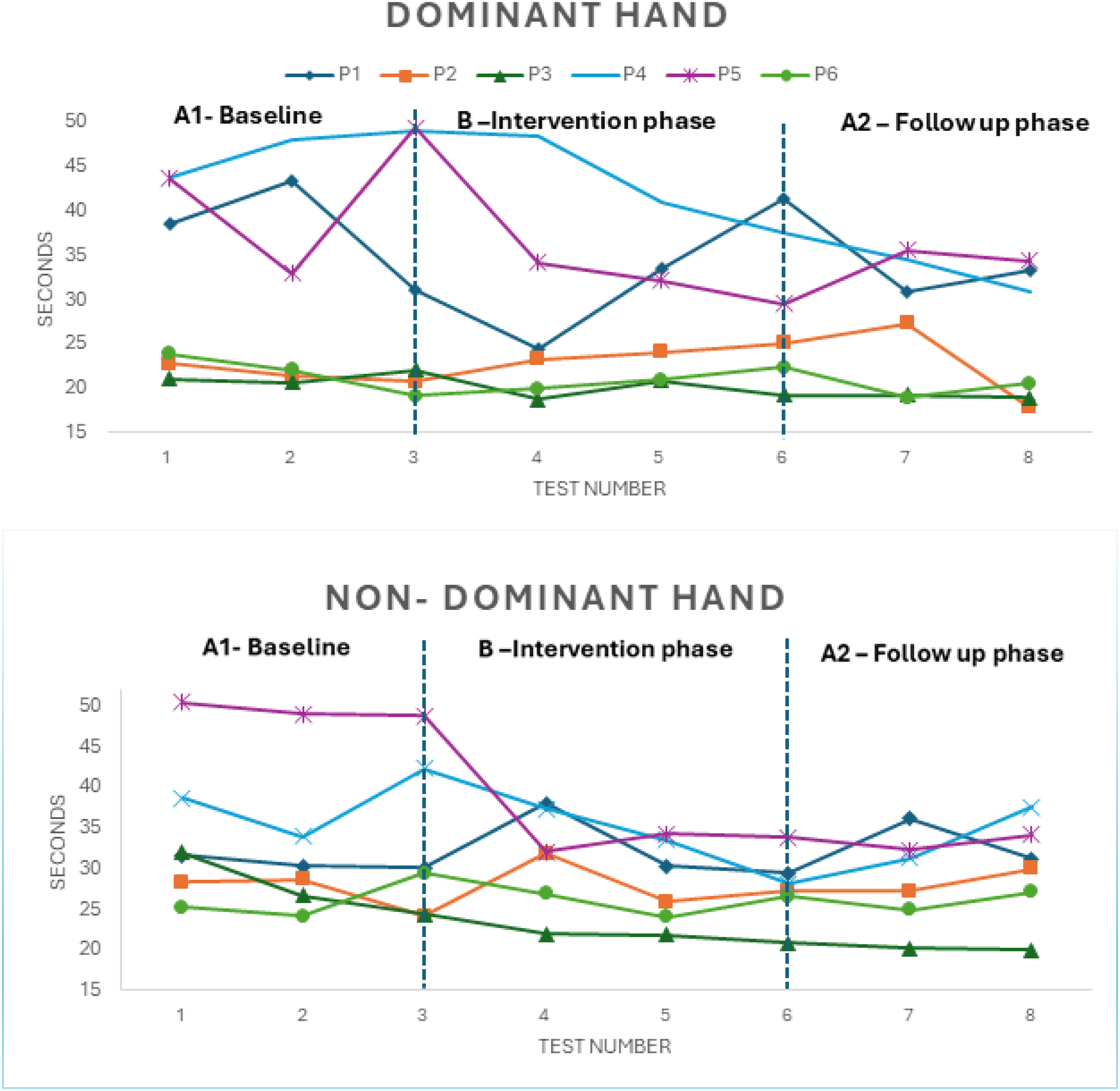
Nine-hole peg test (NHPT) on dominant and non- dominant hand, for the 6 participants, at each measure point.
Change from baseline to intervention in Nine Hole Peg Test (NHPT) for the six participants.
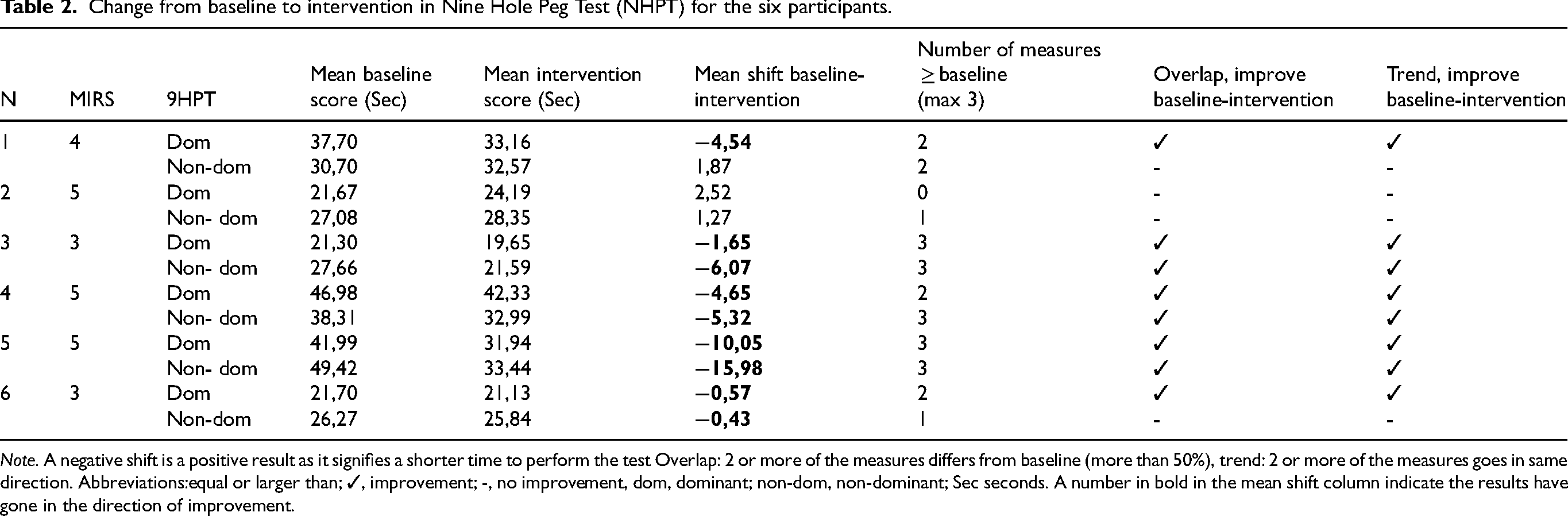
Note. A negative shift is a positive result as it signifies a shorter time to perform the test Overlap: 2 or more of the measures differs from baseline (more than 50%), trend: 2 or more of the measures goes in same direction. Abbreviations:equal or larger than; ✓, improvement; -, no improvement, dom, dominant; non-dom, non-dominant; Sec seconds. A number in bold in the mean shift column indicate the results have gone in the direction of improvement.
Active range of motion (AROM)
AROM in shoulder abduction and flexion of the dominant arm improved in three participants (2, 4 and 5), while the other three remained stable (Figure S1 and S2 in supplementary file). AROM measured with the ArmeoSenso showed a positive change from the beginning to the end of the intervention in abduction (frontal plane), flexion (sagittal plane) and adduction (transversal plane) for participant 1, 3 and 5. Figure 3 shows the changes in participant 5 from the beginning of the intervention (in red) to the end of the intervention (in black) showing an increase in AROM in all directions (Figures of the other participants are in the Supplementary File Figures S3–S7). The participants had full active and passive range of motion in the fingers measured by the therapist and in the AMADEO.
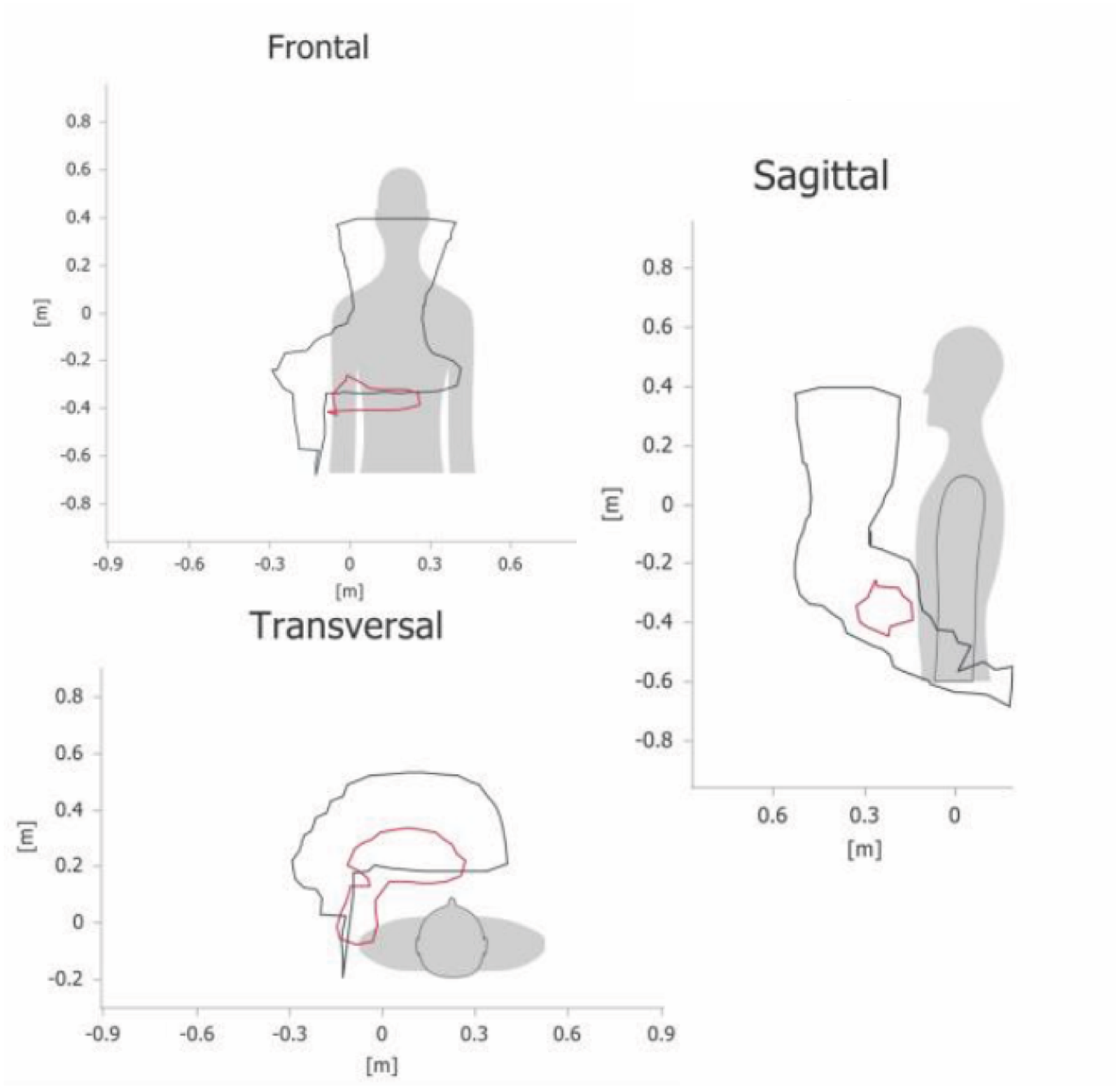
Active range of motion in participant five done in the ArmeoSenso. The smallest (in red) drawing is at the beginning of the intervention and the largest (in black) drawing is at the end of the intervention. A bigger drawing indacates a larger range of motion.
Patient reported outcome measures (PROMS)
All participants remained stable in self-reported hand function (Abilhand-NMD) throughout the study. Most participants had low levels of myotonia to begin with, and they remained stable during follow-up. One participant self-reported high level of myotonia at baseline (score four), and reduced levels of myotonia after the intervention (score three) on the myotonia behaviour scale. The level of fatigue remained stable, while four out of six reported better sleep at the end of the intervention. This suggests that the exercise intervention did not have a negative effect on myonia, fatigue or sleep.
Muscle strength & nut and bolt task
The three participants tested with the Jamar digital dynamometer, increased their muscle strength in the dominant hand, and 2 of 3 in the non-dominant hand as calculated by the mean shift, trend and overlap (Table 3). Two of three participants also increased their pinch strength. All the three participants, tested with the nut and bolt task, reduced their performance time on both dominant and non- dominant side with the small bolt as measured by the calculated mean shift, trend and overlap (Table 3). Two of three participants reduced the performance time on the big bolt.
Change from baseline to treatment in strength and Nut & Bolt task for the three participants tested.
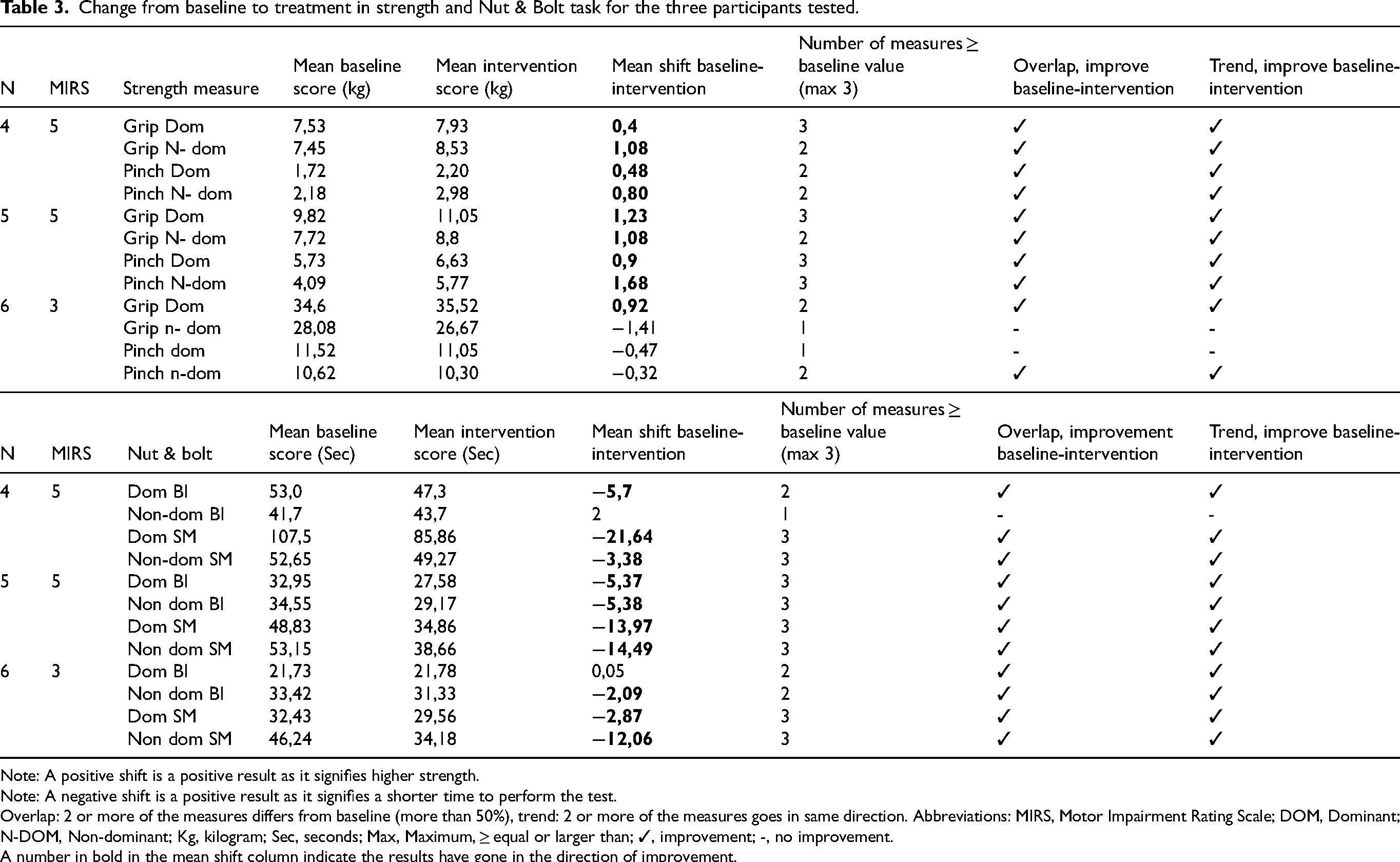
Note: A positive shift is a positive result as it signifies higher strength.
Note: A negative shift is a positive result as it signifies a shorter time to perform the test.
Overlap: 2 or more of the measures differs from baseline (more than 50%), trend: 2 or more of the measures goes in same direction. Abbreviations: MIRS, Motor Impairment Rating Scale; DOM, Dominant; N-DOM, Non-dominant; Kg, kilogram; Sec, seconds; Max, Maximum, ≥ equal or larger than; ✓, improvement; -, no improvement.
A number in bold in the mean shift column indicate the results have gone in the direction of improvement.
Discussion
We found an improvement on the primary outcome, the NHPT, in five of the six participants on the dominant side, and three of six on the non-dominant side based on the calculated mean shift, trend and overlap. The NHPT is a validated and recommended outcome measure in studies of DM1,38,39 used in natural history studies and intervention studies. The majority of our participants used longer time to perform the NHPT compared with the participants in the validation study 38 but more in line with results from another study that used NHPT in DM1. 48 Our participants had more severe motor impairments compared to the participants in the validation study, 38 which may explain why they used more time when performing the test. Our participants performed the NHPT once on each hand at every assessment. It has been recommended to do two tests, as a learning effect from the first to the second trial has been demonstrated. 49 This means that most participants will score better on their second try, as they have learned how to perform the test. Before the first assessment the participants did one practise trial to become familiarized the test. On the other assessments each participant did one trial unless they lost one of the pins on the floor that would severely affect the score. They were then allowed to redo the test. Although we saw a positive change in five of the six participants, the changes were in some of the participants small. Some of our participants demonstrated an unstable baseline period in the NHPT, indicating variability not only between the participants but also within each participant. The observed variability in the baseline period is important to be aware of. It shows that the participants had large variations even though the baseline measures were performed at approximately the same time of the day to eliminate factors related to daily rhythm that could influence the results. As only one baseline measure is common in several study designs, acknowledging that DM1 participants can have a fluctuating performance might be important when designing future studies.
Three of the participants improved their AROM with more than ten degrees in abduction and flexion, and none of the participants deteriorated. We found an improvement on the AROM measured by the Angulus in participant 2 and 4 but not on the visual ROM measured by the ArmeoSenso. One explanation for this could be that the measurements were performed at different time. Hence, it could be influenced by daily physical form, muscle soreness or fatigue. 3 Another explanation could be that it is two different ways to measure the AROM.
We had some difficulties in measuring the AROM in a reliable manner in the video consultations. Small changes in the participants position or where the marker is set can change the angle and thereby range of motion. This could question whether small changes measured in the AROM were real changes or due to measurement errors. Small changes could also be due to variation in daily function. However, we do consider that a change of more than 10 degrees from baseline to the end of the study is a clinically significant change. 50
The scores on the PROMS remained stable throughout the study period. It is unlikely that the perceived hand function would be significantly altered during this short intervention period. We are, however, satisfied that neither the scores on function nor myotonia or fatigue was negatively affected by the increased amount of exercise. All our participants, except for one, had moderate to low levels of myotonia at baseline. This is in line with the scores from the validation study on the NHPT, showing that myotonia was not a severe problem for our participants. 38 The participant reporting high levels of myotonia at baseline in our study reported improvement in the myotonia behaviour scale after the intervention. Altogether, this suggests that the exercises did not worsen myotonia and might in some cases have a positive effect. Fatigue is an important aspect in DM1 and other neuromuscular conditions.3,51 Our participants had moderate to high levels of fatigue at baseline that did not significantly change after the intervention. This is in line with most studies on the effect of exercise on fatigue in muscular dystrophies,52,53 although some interventions in DM1 have been able to impact fatigue positively.13,54 The studies that have successfully reduced fatigue in DM1 used a longer intervention period than in our study, indicating that time is needed to be able to positively impact fatigue.
We found improvement in the muscle strength measures on both sides and in both grip and pinch in two of the three participants tested. Those two participants had quite severe muscle impairment, and weak hand and pinch strength at baseline. We find it promising that the rehabilitation technology seemed to be able to find exercises and movements performable even for those with weak muscle strength. We know from clinical practise and research that it is usually much easier to exercise those with moderate to good muscle strength.55,56 However, finding exercise options for those with severe muscle impairment are highly needed within the NMD field. To our knowledge, this is the first time the Nut and Bolt task has been used in a study of motor function in people with DM1. In our previous study on translation and validation of the Abilhand, we found that a twisting motion as when opening a screwcap is difficult for many with DM1. 41 The results from the Nut and Bolt task in the present study are promising but needs to be studied further in a larger sample. Although the NHPT is a validated function test for DM1, additional outcome measures that may detect other impairments in dexterity are needed.
To our knowledge it is the first time the AMADEO and ArmeoSenso have been used in a study on DM1. Both rehabilitation technologies have primarily been used in research on stroke rehabilitation.34–36 The clinics in Norway having the equipment uses it on a wide range of neurological conditions, with both central and peripheral paresis. In theory, all patients in need of upper limb exercises can benefit from the technology for moving and exercising the arm and hand with or without resistance and in different directions. As there is emerging evidence of the effect of exercise in neuromuscular conditions, 56 the use of rehabilitation technologies is a promising addition to exercise interventions in these disorders. A clear disadvantage of the use of rehabilitation technology is the lack of accessibility for patients not granted access in the specialized clinics. We utilized video consultations, which significantly minimizes the barrier of distance. This means that participants living far away from the research facilities could be included in the SSED study. A disadvantage is that it places some limitations as to which assessments are available.
There are some limitations to our study. First, a SSED study has by design a limited generalizability. 32 However, the DM1 population is so heterogeneous that generalizability is difficult even with other study designs. A SSED study does not increase in strength by adding the number of participants, but we do consider it a strength to have included participants with different impairments and functional levels. Some of the assessments are done on only half of our participants as they were included after the initiation of the study. The results of these additional tests showed improvement in most assessments. It would have been interesting to see if this was the case in all the participants, not only the last three. To have several baseline measures is generally a strength to a SSED study, 32 but the relative unstable measurements in at least some of our participants can be seen as a limitation. It does, however, highlight what we know from clinical experience that daily function varies in this patient population. This should be taken into consideration when designing future clinical trials with DM1 participants, as a single baseline measure is the norm in many study designs- and it may in fact not necessarily represent the DM1 participants’ general functional level.
Conclusion
To our knowledge, this is the first study to use technology-assisted rehabilitation in exercising arm- and hand function in DM1. Our results showed that five of the six participants had a positive although small change in dexterity. Three of the six improved in AROM and two of three participants increased their hand and pinch strength. Self-reported function and myotonia remained stable. None of the participants worsened due to the intervention. Our findings suggest that exercising arm- and hand using rehabilitation technology may have a positive effect on function in people with DM1.This was a single subject experimental design study where the participants acted as their own control, but the promising results encourage designing larger studies on exercise of arm- and hand function in DM1.
Supplemental Material
sj-tif-1-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-1-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-2-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-2-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-3-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-3-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-4-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-4-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-5-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-5-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-6-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-6-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Supplemental Material
sj-tif-7-jnd-10.1177_22143602241301675 - Supplemental material for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study
Supplemental material, sj-tif-7-jnd-10.1177_22143602241301675 for Rehabilitation technology in assessment and treatment of arm and hand function in myotonic dystrophy type 1: A single subject experimental design study by Hanne Ludt Fossmo, Kristin Ørstavik, Aagot Gurandsrud, Jan C Frich and Hilde Stendal Robinson in Journal of Neuromuscular Diseases
Footnotes
Acknowledgements
We would like to thank the patients that participated in the study and Vikersund Rehabilitation Centre, Norway, for letting us use their facilities, rehabilitation technology and employees to execute the study. Authors Fossmo and Ørstavik are affiliated with European Reference Network for Rare Neuromuscular disorders (ERN Euro-NMD).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Norwegian Association for Muscle Disease research fund and Sophie and Leif Torps fund for research on myotonic dystrophy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.