
Abstract
Background
Diabetes Mellitus (DM) cause a high burden to health systems. Information pertaining to health-related quality of life could be useful towards a better understanding between DM and functioning.
Objective
To investigate the association between muscle strength and quality of life according to the severity of neuropathy in people with DM using different classification methods.
Methods
A total of 67 participants were recruited in a rehabilitation centre and stratified into groups. Isometric ankle dorsiflexor muscle strength was assessed using a portable dynamometer and quality of life (utility) was assessed by the EQ-5D-3L questionnaire. Neuropathy was assessed using The Michigan Neuropathy Screening Instrument (MNSI) and the Neuropathy Disability Score (NDS). A multinomial logistic regression was performed to estimate the association between a set of variables, and the neuropathy classification methods.
Results
Most participants were women aged >60 years, with a mean diagnosis of DM of 16.1 years. The mean utility was 0.66, with those with neuropathy having the worst utility. Female gender was associated with a lower chance of developing neuropathy when compared with individuals with mild (OR: 0.15) and moderate (OR: 0.11) neuropathy. Increased ankle dorsiflexor strength was associated with a lower chance of developing neuropathy compared to those without loss of sensation (OR:0.62).
Conclusion
Women with diabetes were less likely to be classified as having loss of sensitivity and had a lower utility compared with men. Individuals with neuropathy reported the worst utility scores. Moreover, increased ankle dorsiflexion strength was associated with lower chance of having neuropathy.
Introduction
Diabetes Mellitus (DM) is a major burden for individuals and healthcare systems. In 2021, data from the 10th edition of the International Diabetes Federation estimated that the number of cases would rise from 643 million in 2030 to 783 million in 2045. 1 Accordingly, peripheral neuropathy is one the most incapacitating aspects of DM, as it may cause pain, cramps, and absence of deep tendon reflexes and/or absence of vibratory and/or sensitivity in the lower limbs.2,3
Approximately 50% of DM neuropathies are asymptomatic, and the later the diagnosis, the greater the risk of injury and plantar ulcers.3,4 In addition, one of the major consequences is loss of muscle strength and mobility, especially in the lower limbs. 5 Furthermore, information on health-related quality of life could be useful to determine the health status of this population to better understand the relationship between DM and clinical and functional aspects. 6 Quality of life is widely recognised as a relevant outcome to consider in addition to the traditional morbidity and mortality outcomes used in DM, including quality-adjusted life years. 6
However, we raise a question whether changes in muscle strength and quality of life are associated with sensory classification in relation to the presence of neuropathy. Although previous studies have shown an association between reduced muscle strength and the occurrence of neuropathy,7,8 the diagnosis of neuropathy is made when subjects have already lost the protective sensitivity of the foot. Conversely, in more subtle cases of decreased sensitivity, it is not known whether there is a relevant loss of muscle strength.
Currently, different classification methods are used to classify individuals with DM according to sensory loss. These methods are widely adopted, however, to the best of our knowledge there is a lack of information on the association of relevant outcomes, such as strength and quality of life, with sensory loss, and whether they might be useful in helping clinicians to anticipate treatment goals based on an expected level of sensory loss. Therefore, the overall aim of this study was to investigate the association between muscle strength and quality of life according to the severity of neuropathy in people with DM using different classification methods.
Method
Study design
Cross-sectional study in which data was collected from March to November 2022 at a Rehabilitation Centre for Diabetes, Specialised Centre for Diabetes, Obesity and Hypertension (Centro Especializado em Diabetes, Obesidade e Hipertensão arterial – CEDOH, in Brazilian Portuguese) in the city of Brasília, Brazil. The study was reported in accordance with the STROBE guideline.
Participants
Participants were users attending the Rehabilitation Centre and recruited at random during their routine appointments. Participants were included if they were: (1) diagnosed with type 2 diabetes mellitus for 5 years or more; (2) male or female; (3) 18 years of age or older; and (4) not pregnant for at least 12 months prior to the study.
The exclusion criteria were: (a) changes in muscle strength, such as neurological, orthopaedic, or rheumatological diseases; (b) active foot ulcers; (c) amputation of any level in the lower limbs; and (d) non-attendance to assessments.
The study was granted approval by the Institutional Ethics Committee under protocol 4.974.078 and 5.217.470, and participants gave their signed informed consent.
Assessments
Participants attended the rehabilitation centre for a single 50-minute face-to-face assessment of sociodemographic information and body mass index (BMI) measurements. Clinical data (most recent glycated haemoglobin - HbA1c values, associated comorbidities, previous screening tests for diabetic neuropathy and retinopathy) were extracted from each participant’s medical record.
Neuropathy screening
This study used two neuropathy screening tools, that is, the Michigan Neuropathy Screening Instrument (MNSI) and the Neuropathy Disability Score (NDS) questionnaires.
The MNSI 9 is a valid and reliable self-administered instrument consisting of two parts. Part 1 contains 15 questions that add 1 point to each answer ‘Yes’ for questions 1–3, 5–6, 8–9, 11–12, and 14–15, or ‘No’ for questions 7 and 13. Questions 4 and 10 do not score as they deal with the measure of circulatory insufficiency, and measure of general asthenia. A score ≥7 was considered abnormal. Part 2 comprised a physical examination bilaterally, each positive finding on inspection and presence of an ulcer received 1 point bilaterally and on physical examination each finding was scored 0.5 when decreased (vibration, reflex, monofilament sensitivity) and 1 point when absent. Neuropathy was defined by a score >2.0 on the MNSI.
The second screening instrument was the short version of the NDS questionnaire, validated and adapted to the Brazilian Portuguese. 10 The scores for painful, thermal, and vibratory sensations in the tests were (0) if present, and (1) if reduced/absent. For the reflex, the scores were (0) if normal, (1) if present with reinforcement, or (2) if absent, bilaterally. The NDS physical examination score is classified as normal (0–2), mild (3–5), moderate (6–8), or severe (9–10).
Tactile sensitivity assessment
The sensitivity assessment was performed with the Semmes-Weinstein SORRI-Bauru® nylon monofilament aesthesiometer set, 11 which is the gold standard, and a valid and reliable instrument. The instrument was applied with the participant in the supine position and eyes closed, on the plantar region in four recommended areas, namely, point 1 (hallux and distal phalanx) and points 4, 5, and 6 (1st, 3rd, and 5th metatarsals), bilaterally and perpendicular to the skin at 1–2 cm.
The participants were instructed to verbally respond with ‘Yes’ in case of sensitivity in the tested area. The monofilaments in the kit range from 0.07 g to 300 g, with the 10.0 g monofilament being able to detect gross fibre alteration and assess plantar protective sensitivity.
Based on the results, participants were stratified into the following groups of sensitivity: Group 1 – Normal or altered sensitivity for the hand and foot with difficulty with shape and temperature discrimination (0.07 g, 0.2 g, and 2.0 g); Group 2 – Loss of protective sensitivity and hot/cold discrimination (4.0 g and 10g); and Group 3 – Neuropathy, presenting loss of sensitivity to deep pressure, but feel pain (300g).
Strength assessment
Lower limb muscle strength was assessed in kilogram-force (kgf) with a portable Hoggan microFET2® dynamometer (Hoggan Scientific, LLC, Salt Lake City, UT, USA), 12 based on previous studies.13–15 The final value used for analysis was the average of three consecutive attempts. The portable dynamometer has inter- and intra-assessor reliability and was considered valid for muscle strength assessments.13,16
The participant was positioned in supine position with the ankle relaxed and hips and knees extended. After positioning, they were instructed to perform a maximum voluntary ankle dorsiflexion isometric contraction lasting 5 seconds, with a 30-second interval between three attempts.
Quality of life assessment
The Brazilian Portuguese validated version of the Euroqol EQ-5D-3L was used. 17 The questionnaire is self-administered, and measures five health dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression. These are classified into 3 levels of severity with the response options: (1) no problems, (2) some problems, and (3) extreme problems. The result represents the dimensions evaluated by this system that allows describing a total of 243 possible health states, translated into codes representing utility values ranging from 1 (perfect health) to −0.176.
Data analysis
Assumptions of data normality were confirmed using the Shapiro-Wilk test. Data were analysed descriptively using mean and standard deviation, absolute and relative frequencies.
We adopted a multinomial logistic regression with a backward stepwise method to estimate the association between the predictive variables age, gender, dorsiflexion strength, utility, glycated haemoglobin, and time since the diagnosis, and different diagnosis methods (categorical dependent variable). For regression model 1, we adopted the filament method as the independent variable, and for regression model 2, we adopted the NDS method as the independent variable to investigate whether the set of predictive variables corrected classified the participants. We used the monofilaments and the NDS as independent variables, because of two main reasons: (a) the monofilaments are the gold standard measure of neuropathy, and (b) the NDS is widely used in the healthcare system, especially in the rehabilitation centre where we recruited the participants.
Collinearity assumptions between the independent variables were confirmed in an exploratory analysis, using a correlation matrix. Data were checked for outliers through a scatter plot and residual analysis. In the data analysis, Nagelkerke’s pseudo R2 was calculated. In the backward stepwise method selection, each variable was automatically removed based on the significance, and the model considered only those variables presenting significant contributions (p<0.05). We also checked the Akaike information criterion (AIC), for which lower values indicated a more adequate fit of the data.
The statistical significance was set at 5% (p<0.05), with a confidence interval of 95%. The SPSS software version 29.0 was used for all analyses.
Results
A total of 80 people with type 2 diabetes mellitus (T2DM) were assessed for eligibility. Thirteen participants were excluded (four due to the presence of an ulcer, five due to amputation of any part of the lower limb, and four participants did not wish to participate). The final sample consisted of 67 participants.
Characteristics of the study’s participants.
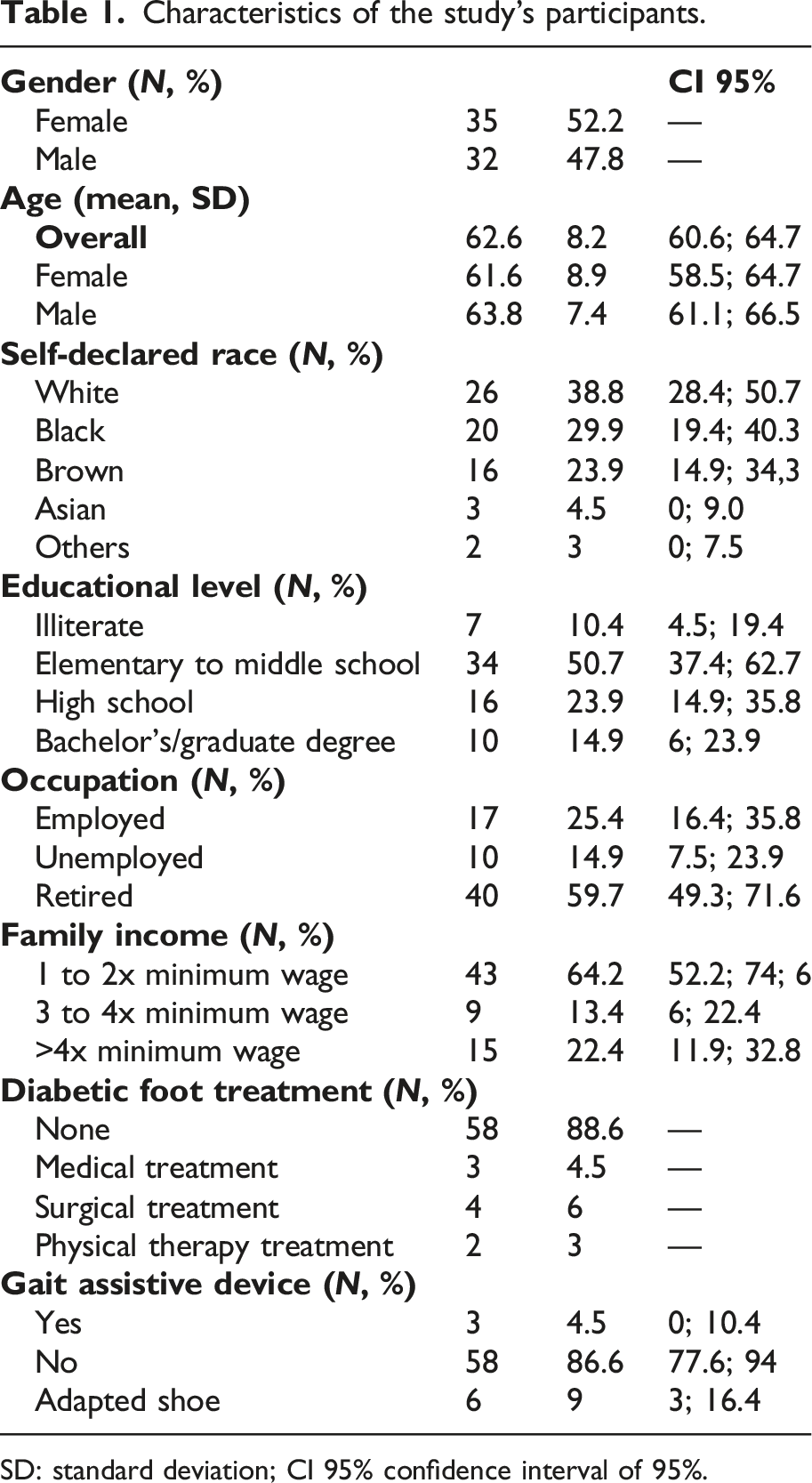
SD: standard deviation; CI 95% confidence interval of 95%.
The frequency of twice-daily blood glucose monitoring was somewhat higher in 21 participants (30%), and 63 participants (94%) were taking insulin. Retinopathy was reported by 26 participants (16 with mild and 4 with severe non-proliferative retinopathy, and 6 with proliferative retinopathy). The most common comorbidities found were hypertension (78.1%), followed by dyslipidemia (48.7%), and obesity (n = 10; 15.6%).
Classification of participants’ neuropathy according to the instruments used in the study.
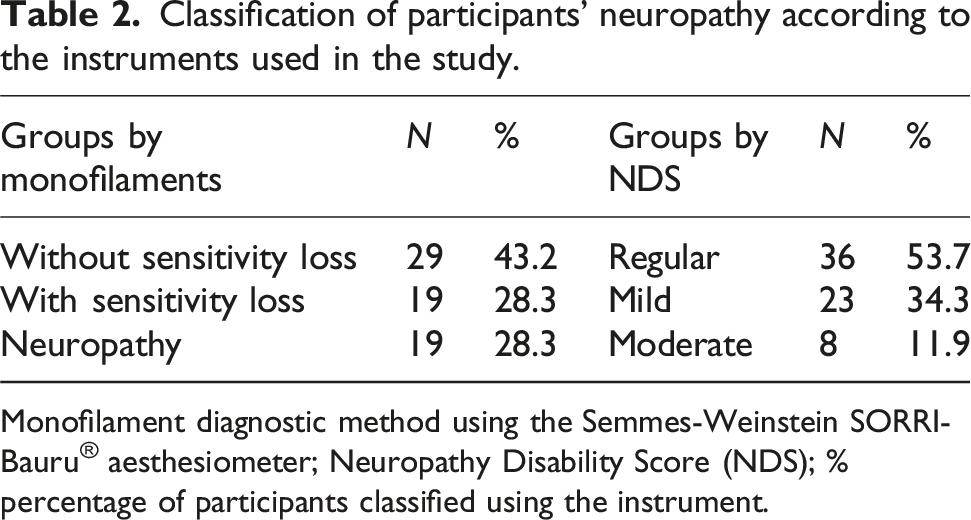
Monofilament diagnostic method using the Semmes-Weinstein SORRI-Bauru® aesthesiometer; Neuropathy Disability Score (NDS); % percentage of participants classified using the instrument.
Data on the utility scores and EQ-5D-3L dimensions of the participants, stratified by sensitivity loss and gender.
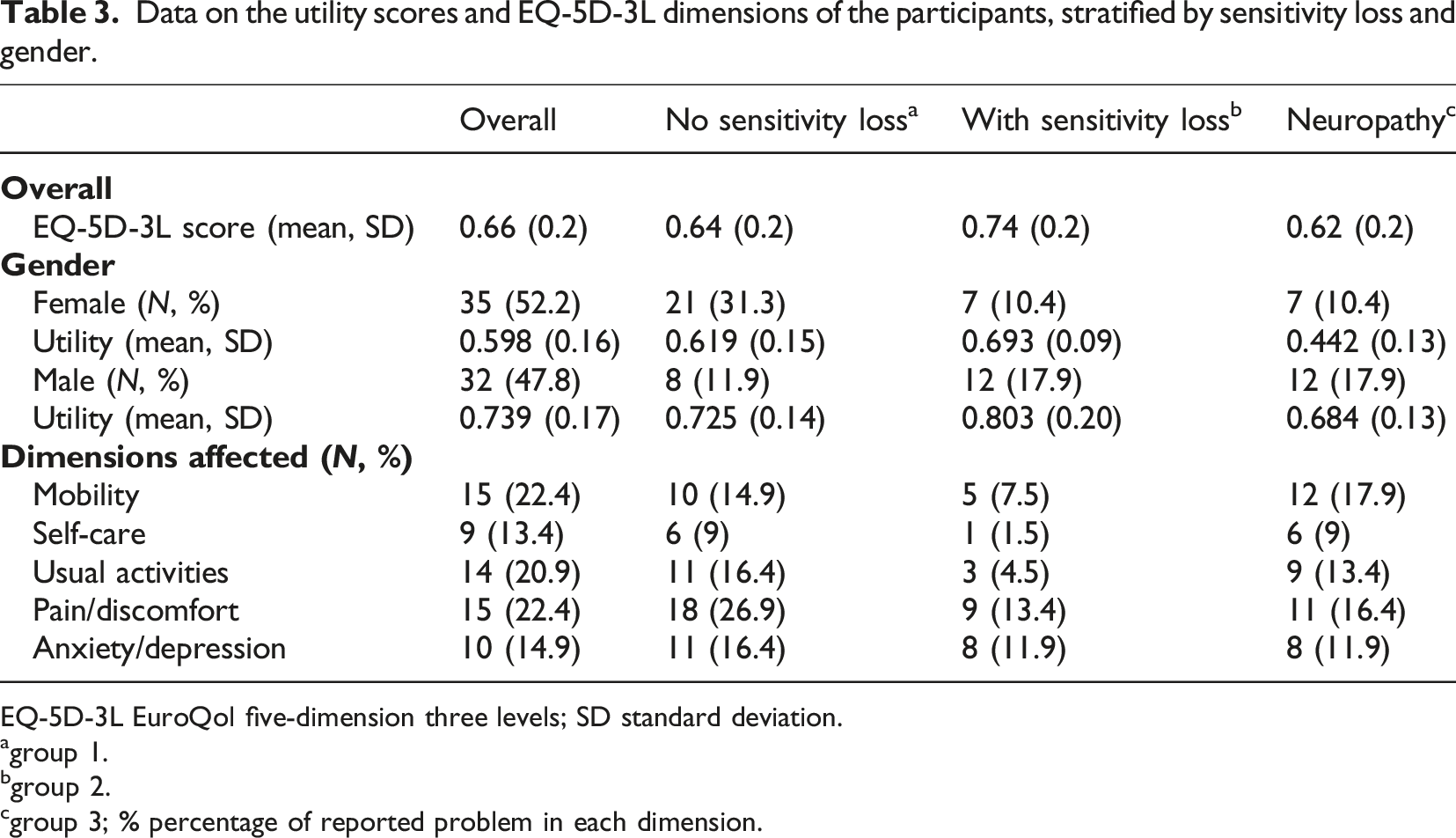
EQ-5D-3L EuroQol five-dimension three levels; SD standard deviation.
agroup 1.
bgroup 2.
cgroup 3;
Regression model 1 with monofilament diagnosis method.
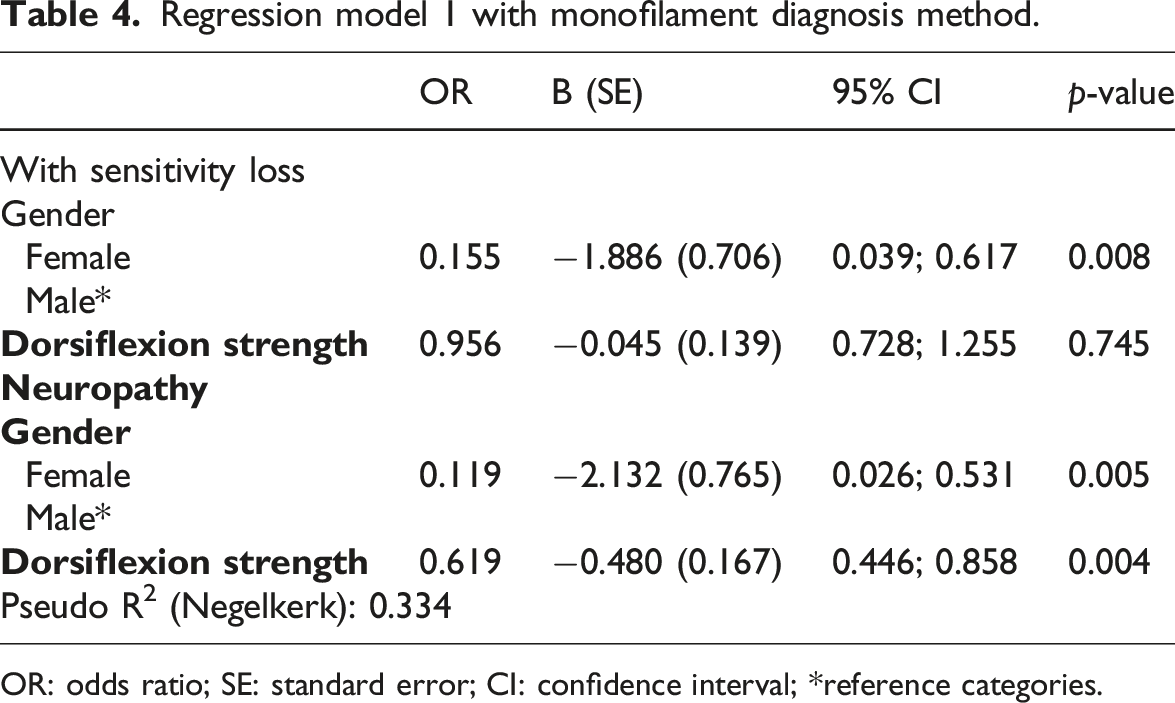
OR: odds ratio; SE: standard error; CI: confidence interval; *reference categories.
Regression model 2 with neuropathy disability score diagnostic method.
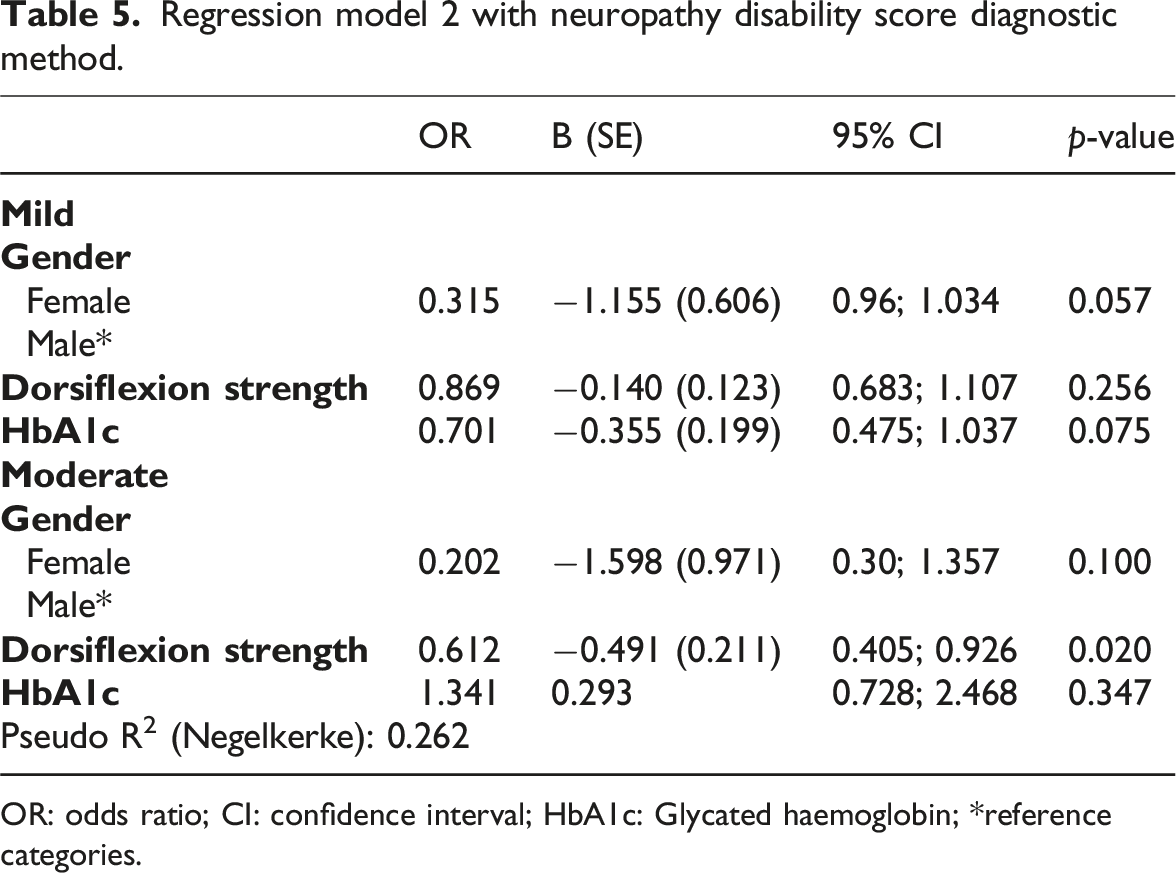
OR: odds ratio; CI: confidence interval; HbA1c: Glycated haemoglobin; *reference categories.
Discussion
We investigated the association between a set of clinical and functioning variables in individuals with type 2 diabetes in accordance with different sensory classification methods. Participants with neuropathy, especially women, had lower utility scores compared to those with and without sensory loss. We found associations between reduced muscle strength, gender, and impaired sensitivity. Females were less likely to be classified with loss of sensitivity, compared to males. In addition, increased ankle dorsiflexion strength was associated with a lower chance of having neuropathy.
We found a higher frequency of female individuals, who underwent insulin treatment, with a mean age of 61.6 years. Those findings are corroborated by previous studies, in which people without neuropathy were older and presented higher levels of HbA1c. 18 This is relevant, as a risk factor for neuropathy is age >60 years.19–21 Furthermore, a proportion of the participants (22%) in the present study reported mobility limitations. This is important because with increasing age there is an increase in comorbidities related to muscle mass and mobility loss. For instance, more than 70% of adults with DM have limited mobility, in addition to functional decline and risk of falling.22,23 In the present study, the most common comorbidities were hypertension, obesity, and dyslipidemia, corroborating a previous study. 24 Moreover, the HbA1c profile was higher than 7%, which is recommended for the prevention of long-term vascular complications. 25 Glycaemic control, as well as the treatment of modifiable risk factors such as blood pressure and lipid control, may modestly slow the progression of neuropathy. 26
We found a lower mean utility score compared with previously reported data in individuals with DM. 27 Individuals with neuropathy, especially women, had worse utility values. Currie, Poole 28 reported that quality of life in hospitalised individuals with DM presented no significant differences between gender or type of DM. However, the authors reported a deterioration of quality of life as the severity of neuropathy increased. These data show a relevant association between severe symptoms of neuropathy and worsening quality of life in individuals with DM, which corroborates our findings. It is possible to assume that the severity of neuropathy is strongly associated with frailty and mobility limitations linked to muscle mass loss and decreased gait speed.5,29 The presence of impaired mobility was also reported by IJzerman, Schaper (5) (e.g. impairments in the timed up and go test; six-minute walk test) and was associated with loss in muscle strength and lower quality of life in this population.
We found that women had a lower chance of being classified with loss of sensitivity, compared to men. This finding might be explained by different health seeking behaviours and improved self-care of women compared with men. This is corroborated by a previous study 30 investigating the type of health service sought (prevention vs treatment/diagnosis), in which out of 205,529 individuals, 17.54% reported seeking health services mostly for treatment and diagnosis. Another recurring aspect is that health services characteristics are predominantly aimed at the female public, such as structure, organisation, decoration, and communication, which may explain why women are more susceptible to seek preventive services and health promotion. 31
Our findings showed that for each unit increase in muscle strength, women presented a lower chance of being classified as neuropathic. Hyperglycemia, an early manifestation for the development of DM, is associated with the development of frailty and limited mobility linked to loss of muscle mass. 23 Higher levels of HbA1c, and longer duration of diabetes is also associated with worsening muscle quality and lower quadriceps strength in adults >50 years. 32 This is interesting because lower limb muscle weakness related to DM has shown greater impairment in ankle and knee muscles regardless of the presence of neuropathy.14,29,33–35 Thus, data on the severity of neuropathy and its influences on dorsiflexors muscles strength are relevant for recommending self-care and prevention strategies by physiotherapists in the population with DM. 36
Scarton, Jonkers 37 investigated lower limb muscle strength, as well as joint kinetics and kinematics in people with neuropathy. The authors reported a decrease in hip joint mobility with a greater angle of pelvic rotation at the end of the gait cycle, as well as reduced strength in the hip flexor muscles. Individuals with neuropathy also showed reduced ankle flexion/extension range of motion in the support phase, and reduced muscle strength of the muscles involved in ankle plantar flexion, compared to controls. The authors highlighted the function of the posterior tibial muscle in the stabilisation of the ankle and in the support of the medial foot arch. Thus, the decrease in muscle strength could affect gait and balance, contributing to the risk of falling. 22 This confirms the clinical relevance of our findings, particularly the relevance of measuring the ankle dorsiflexor strength in this population. This is interesting because people with DM are more likely to have accelerated loss of muscle mass and strength in the lower extremities compared to people without DM.23,32
One strength of this study was the adoption of a real-world approach by recruiting participants in a clinical rehabilitation setting. Nevertheless, due to restrictions within this setting we were not able to perform a sample size calculation, which might present some limitations regarding statistical power and generalisation to other populations. In addition, because we used a cross-sectional design, we were limited to draw conclusions regarding predictive analysis.
Conclusion
Our results showed that women with diabetes were less likely than men to be classified as having tactile sensitivity loss. Additionally, increased ankle dorsiflexion muscle strength was associated with a lower chance of having neuropathy. The results also showed that participants with neuropathy, especially women, had lower utility scores compared to those with and without sensitivity loss.
Footnotes
Acknowledgements
The authors would like to thank Alexandra Rubim Camara Sete and Eliziane Brandão Leite for allowing the research to be carried out during service hours in the CEDOH (Centro Especializado em Diabetes, Obesidade e Hipertensão). We also would like to thank Silvio César Parente, Luz Marina Alfonso Dutra, and Danyelle Lorrane Carneiro Veloso for their support during the participants’ recruiting.
Ethical approval
The study was granted approval by the Institutional Ethics Committee under protocol 4.974.078 and 5.217.470, and participants gave their signed informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code (001); UnB/DPI/DPG; and Fundação de Apoio à Pesquisa do Distrito Federal (FAPDF). The funding source was not involved in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.