
Abstract
INTRODUCTION
Over the past years, some legislative decrees considerably modified the Public Health Care System in Italy focusing on cost containment. Improving the financial situation calls for more attention to expenses.
Now we are living in a transitory phase that outlines a fundamental fact: an irreversible process has started to convert the local sanitary units into company-orientated facilities which boundaries are not yet defined.
The first impact of the financial laws in the laboratory forced suppliers to reduce product prices. Generally, supply and service contracts are regulated through public tenders, in which up to 70% of the total score is assigned to the price and the rest to instrument technical features and reagent quality.
The lab, as a supplier of services, is required to increase efficiency and productivity. Being organized like a private company means acquiring goods and services according to rational rules of economy and cost-efficiency, in order to guarantee quality disease management. This clashes with the cost reduction of products imposed by the Italian law.
We faced global cost reduction, by examining the lab processes through a workflow analysis. Workflow analysis is essential to find weaknesses in the organization and to achieve high productivity.
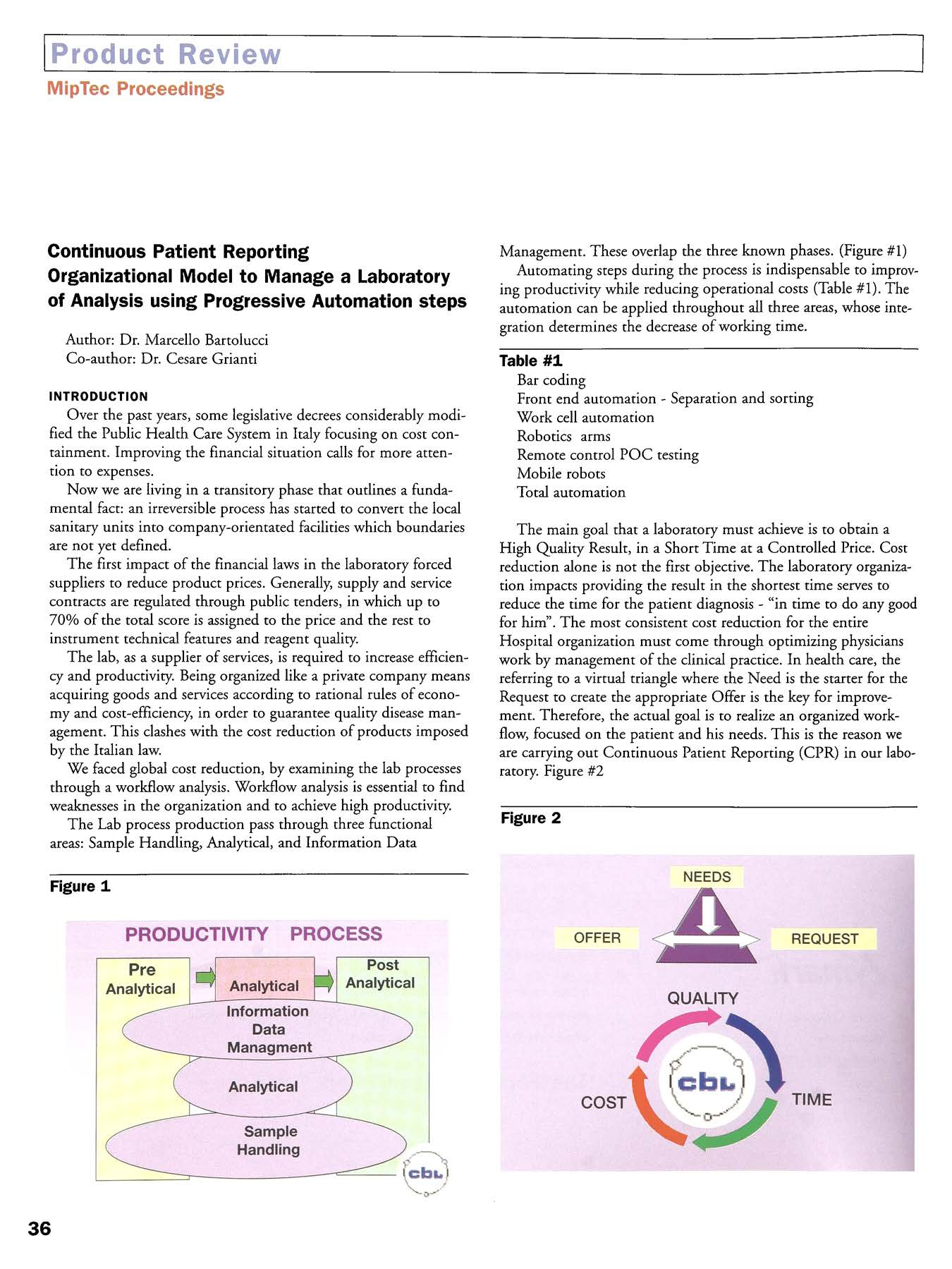
The Lab process production pass through three functional areas: Sample Handling, Analytical, and Information Data Management. These overlap the three known phases. (Figure #1)

Automating steps during the process is indispensable to improving productivity while reducing operational costs (Table #1). The automation can be applied throughout all three areas, whose integration determines the decrease of working time.

The main goal that a laboratory must achieve is to obtain a High Quality Result, in a Short Time at a Controlled Price. Cost reduction alone is not the first objective. The laboratory organization impacts providing the result in the shortest time serves to reduce the time for the patient diagnosis — “in time to do any good for him”. The most consistent cost reduction for the entire Hospital organization must come through optimizing physicians work by management of the clinical practice. In health care, the referring to a virtual triangle where the Need is the starter for the Request to create the appropriate Offer is the key for improvement. Therefore, the actual goal is to realize an organized workflow, focused on the patient and his needs. This is the reason we are carrying out Continuous Patient Reporting (CPR) in our laboratory. Figure #2

HOW THE LAB HAS EVOLVED
In the early 90's, the Italian Laboratories were organized into different laboratory areas depending on instrument location and tests ordered. The full time employees were assigned to the different sections and worked as independent laboratories.
Before the organizational changes in our lab, samples arrived along with a written request stating patient data and tests required. The requests formed departmental worklists that were sent to the different sections where they were entered into the instrument's PC. Then the tubes were sorted by test/panel type and if required they were separated to centrifuge and aliquot cups. The analytical phase lasted from 10 a.m. until 2 p.m. After this, there was the validation and printing of reports (one report for each section) that reached the department in the late afternoon.
It is obvious that such an organization with many manual procedures and multiple instruments implied a lot of trained people and very high costs.
At the same time, urgent sample handling required a STAT section. Since the TAT (Turn Around Time) was lower for these analyses than for the routine tests, the departments increased the number of urgent requests. Our lab has received up to 500,000 Stat tests on 2,500,000 total tests per year. This phenomenon brought very high incremental costs.
The laboratory was reorganized and the LIS (centralized patients management) was developed. A unique area receives all sample tubes and bar-coded labels are printed. Then tubes are sorted and sent to workstations. This situation led to using fewer instruments, favoring those that allow multiple tests, primary tubes with a barcode reader on board and connection on-line with the LIS.
In 1997, with further LIS enhancements, we began using optical cards for inputting requests, to speed up sample patient acceptance. The departments started to place the tubes sorted by patient ID and test panels in special baskets and to transfer to the lab barcoding area.
With these enhancements, we created the conditions to realize the CPR (Continuous Patient Reporting)
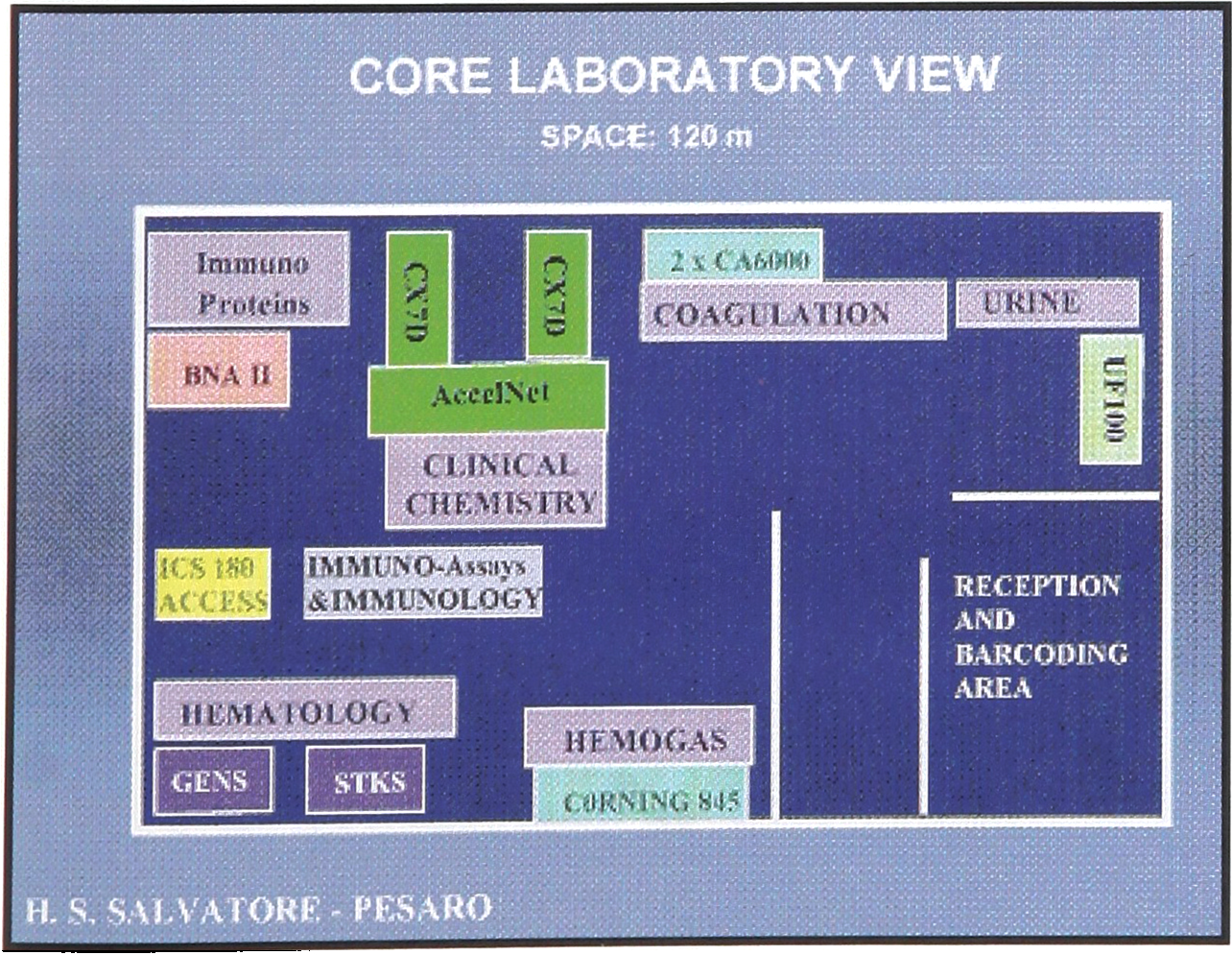
We are approaching the creation of a core lab, putting together the most automated instruments which perform 80% of the tests requested in Clinical Chemistry, Proteins, Immunoassay, Hematology, Coagulation and Urine, executed within 2hrs. Fig.#3
Priority #1 is started from the sample patient processing. There is no distinction between routine and urgent analysis request. The two laboratories have merged in a unique area thanks to the application of CPR. The real emergency tests can be handled between 20–30 minutes. Samples are accepted, tested, approved and sent to departments continuously 24-hours a day.
Working with the head of the other departments and the offsite points of drawing, tubes have been planned to arrive consistently throughout the day.
People were fully involved in the reorganization. Personnel reallocation has allowed the development of new diagnostic sections (to execute high profitability tests) such as molecular biology or cytometry. Revenues have increased while cutting costs.
Personnel costs do not exceed 35% of the total operational costs.

In September 1997, the first evaluation of the AccelNet' System supplied by Beckman Coulter, Inc. started in our Lab. After the appropriate fine tuning, the system has been processing up to 250 clinical chemistry tubes per day for about 3 months. Since June 1998, the AccelNet is reporting results.

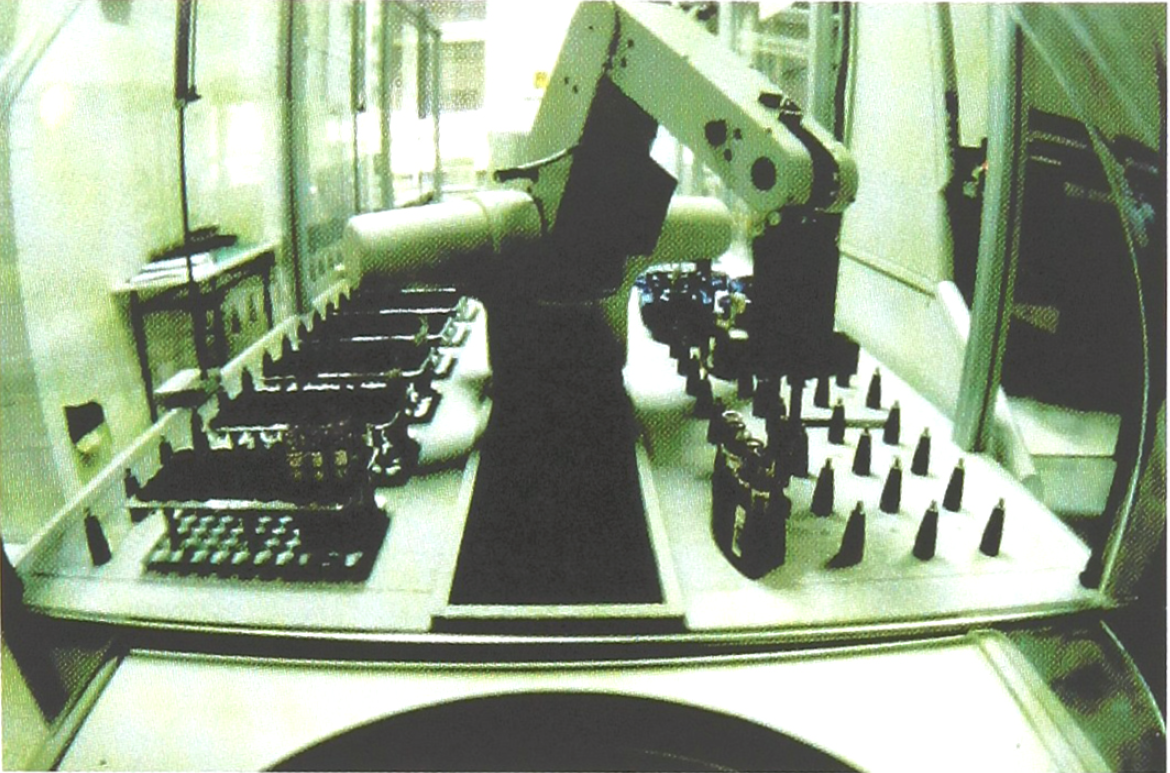
The AccelNet system is composed of an AccelX ‘;automated central processor linked to 2 CX'7 Delta (or CX9 ALX) analyzers and to the AccelSpin’ robotic centrifuge, managed by the DataLink data manager software connected with one on-line to the main host.
The front-end of Accelnet system automates- many operations:
Receiving ID# and tests requested from LIS “Sorting samples to be centrifuged
Loading, running and unloading centrifuge
Decapping tubes
Loading tubes in CX racks
Loading and unloading CX instruments
Automatic Ordac, rerun, reflex test, delta check
Reporting test results directly to the LIS
Sorting samples to appropriate storage racks, for routing to other locations
Prioritizing STAT samples
In clinical chemistry phased approaches of automation and sample processing have been planned to start fall of 1998 using AccelNet 24 hours a day.
We are looking for this automation to pay back within 5 years.
The Future — Integration and Improvement
Using the CPR concept, through the progressive workstation automation and a specimen matrix tube consolidation, we will increase the percentage of tests done in the core lab to reduce the TAT.
A core lab with 24 hours readiness will be formed in the near future by using:
BE A PROCESS CONTROLLER NOT ONLY DATA CONTROLLER
The analysis of the production workflow has showed that among the health care facilities the laboratory can be compared with an industrial company.
It is quite logical that the automation process started first in the laboratory rather than in other departments.
The availability on the market of sophisticated automated technological systems allows achieving a high level of efficiency and efficacy.
We experienced a positive impact on lab staff upon implementing this new way of working. The human resources are fundamental to arrive to a final objective. Their total involvment into the process control is the key to optimize their job and to be more effective, reliable and flexible.
The implementation of this lab workflow organization is expected to be the catalyst to better management of other hospital departments.
The final goal is the patient care with attention to give to the clinicians the results in real time.
The Azienda Ospedaliera needs to answer to patient needs with quality, short time and cost controlled answers.
A special thanks for their contribution in writing this article to Ezio Fabrizi and Bruno Bastianeiii of Beckman Coulter.