
Abstract
Introduction
Total hip arthroplasty (THA) is a widely performed orthopaedic procedure that significantly alleviates pain and enhances the quality of life for patients with hip osteoarthritis who have not responded to conservative management. 1 The demand for THA continues to rise, with over 262,000 primary THA performed in the United States in 2020. 2 It is projected that annual volume of THA will increase by 176% by 2040 and up to 659% by 2060. 2 Given the high clinical demand, optimizing surgical outcomes in THA becomes crucial.
Numerous strategies have been developed to improve the outcomes of THA, for example evaluating spinopelvic relationship in preoperative planning and templating, 3 and using larger femoral head sizes to minimize risk of dislocation. 4 However, precise implant positioning remains the cornerstone of successful surgery. 5 Lewinnek et al. 6 defined the ‘safe zone’ of the acetabular cup as an inclination of 40° ± 10° and an anteversion of 15° ± 10°. This was later modified by Callanan et al. 7 to an inclination of 30°–45° and anteversion of 5°–25°. Inappropriate positioning of components can result into detrimental complications, including asymmetrical polyethylene wear, pelvis osteolysis, migration of components, and recurrent dislocation. 8 These complications may necessitate revision surgeries, resulting in an unnecessary burden for patients and the healthcare system. 9
Robotic-assisted THA has been developed to improve surgical accuracy and predictability of implant positioning, potentially enhancing patient safety, and reducing surgical complications. It does not only provides surgeons with three-dimensional computed tomography (CT) scan-based planning but also offers haptic guidance during key steps of surgery such as reaming and cup impaction. While some evidence suggests advantages over conventional THA, 10 there is limited evidence of such advantage in this locality. Moreover, the benefit on the femoral side is still unclear.
This retrospective cohort study aims to compare (i) the accuracy of implant positioning between robotic-assisted and conventional THA, and (ii) other intra-operative and post-operative outcomes, including blood loss, operative time, length of stay, and associated surgical complications. It is hypothesized that robotic-assisted THA enhances the surgical accuracy and consistency of implant positioning in various radiological parameters when compared with conventional THA.
Materials and methods
Patient recruitment and study design
This study was a single-centre, retrospective cohort study involving patients who underwent primary cementless THA in one of the local major joint replacement centres between November 2017 and October 2023. MAKO SmartRobotics (Stryker Corporation, Kalamazoo, MI, USA) was introduced at our centre in June 2022. During this captioned period, 134 patients had received THA at our centre. Of this cohort, 97 patients were eligible for inclusion: 50 patients underwent robotic-assisted THA and 47 patients received conventional THA. Ethical approval was granted by the local Institutional Review Board.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (i) patients aged between 18 and 90 years old; (ii) patients who underwent primary cementless THA; (iii) patients with a minimum follow-up of 1 year post-operatively.
The exclusion criteria were: (i) pre-existing neuromuscular disorders resulting in musculoskeletal dysfunction; (ii) patients with incomplete clinical data; (iii) patients with non-standardized radiographs, including prone view, hemipelvis asymmetry, deviation of pubic symphysis from coccyx of more than 2 mm, 11 femoral rotational asymmetry, difficulty in identification of lesser trochanter, and insufficient visualization ; (iv) patients with proximal femur fractures; (v) patients with a prior history of hip surgery performed on the operated hip.
Pre-operative preparation
For conventional THA, pre-operative planning and templating were performed using standard pelvis and hip radiographs with the use of OrthoView (Materialise NV, Leuven, Belgium). Surgeons templated component size and position and planned the desired level of neck cut. Implant selection was based on the pre-operative templating.
For robotic-assisted THA, standardized CT scan of the bilateral hips and knees were performed and imported into the MAKO software for patient-specific three-dimensional templating. Surgeons adjusted the desired implant position referencing the reconstructed three-dimensional images.
In both groups, pre-operative templating planned all acetabular cups for implantation at 40° inclination. The anteversion was adjusted based on surgical approach: 20° for the Southern approach and 15° for the Hardinge approach. The goal was to achieve balanced limb length.
Surgical procedure
All surgeries were performed by the same team of fellowship-trained orthopaedic surgeons experienced in joint reconstruction. Procedures were conducted under general, spinal, or combined spinal-epidural anaesthesia. The surgical approach adopted was based on the surgeon's preference and expertise.
In conventional THA group, implant components were chosen at the surgeon's discretion with reference to pre-operative templating. The options were the Zimmer Continuum acetabular system and ML taper femoral hip stem (Zimmer Biomet Inc, Warsaw, USA) or the Smith & Nephew R3 acetabular system and Polarstem femoral hip stem (Smith & Nephew, Watford, England). Femoral neck osteotomy was performed after dislocation of the hip. The acetabular procedure utilized the transverse acetabular ligament to guide cup orientation.12–13 After acetabular cup and polyethylene liner placement, femoral preparation and broaching were performed, followed by femoral stem insertion.
In the robotic-assisted THA group, all patients received the Stryker Trident II acetabular system and Accolade II femoral hip stem (Stryker Corporation, Kalamazoo, MI, USA). A pelvic array was fixed to the iliac crest using three bone pins. Checkpoints were placed to the proximal femur and outside the acetabular cavity. Apart from the placement of pelvic array and checkpoints, the sequence of the operation remained unchanged. The express workflow of Makoplasty was adopted for robotic-assisted procedures.
After surgery, all patients received prophylactic antibiotics, analgesics and a standardized rehabilitation programme. All patients were followed up in clinic approximately four months after the surgery.
Radiological analysis
Radiographic study included pre-operative and first post-operative clinic follow-up X-ray radiographs. Radiographic measurements were performed by two independent investigators: an orthopaedic resident and an orthopaedic specialist experienced in hip arthroplasty.
The radiographic parameters of interest included: acetabular inclination, acetabular anteversion, leg length discrepancy, acetabular offset, femoral offset, global offset, femoral stem alignment angle, and intramedullary prosthetic canal fill ratio.
For acetabular inclination, a trans-ischial line was drawn across the ischial tuberosities as reference. A concentric ellipse was used to fit the opening of the cup. Acetabular anteversion was defined as the angle between the line bisecting the ellipse and the trans-ischial line.
Acetabular anteversion was calculated using the method described by Liaw et al., 14 which has been shown to be the most accurate method among its counterparts. 15 With the ellipse drawn, a line (AB line) was plotted across the maximal diameter, a perpendicular line (CD line) was drawn at the midpoint, and a line (AC line) was drawn connecting point A to C. The Angle (β) formed between lines AB and AC was used for calculation with following formula: Anteversion = sin−1 tan β (Figure1). In all cases, correct placement of acetabular cup in anteversion was confirmed using X-ray radiograph of the hip in lateral oblique view.
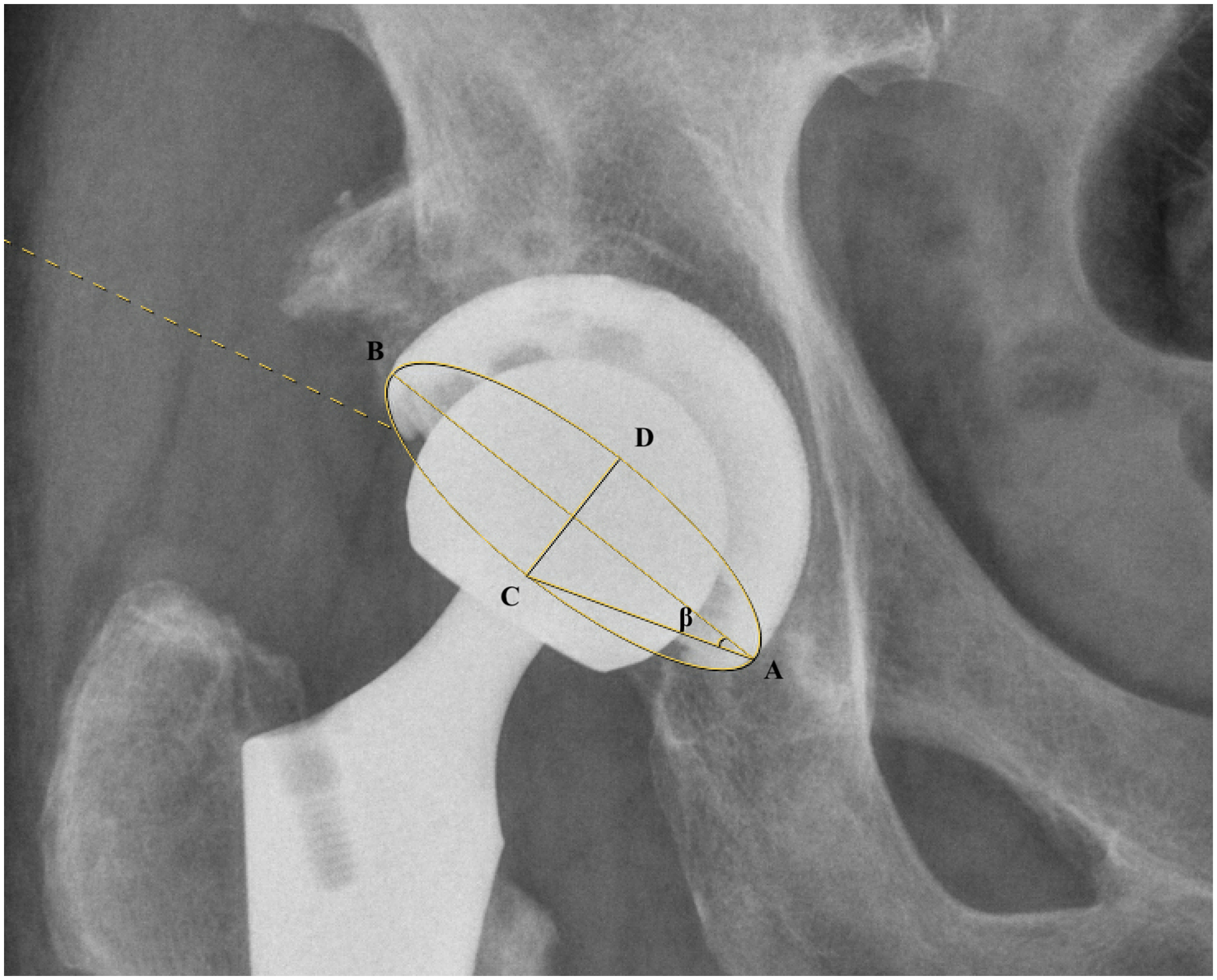
Depiction of the method described by Liaw et al. β angle was used for calculation of the anteversion.
The inclination and anteversion angles of the acetabular cups were evaluated against the safe zones defined by Lewinnek et al. and Callanan et al. Lewinnek et al. 6 described the safe zone as an inclination of 40° ± 10° and an anteversion of 15° ± 10°, whereas Callanan et al. 7 defined the safe zone as an inclination between 30° and 45° and an anteversion between 5° and 25°.
Leg length discrepancy was defined as the vertical distance from lesser trochanter to trans-ischial line. 16
The centre of rotation was defined on X-rays by drawing concentric circles encompassing the preserved acetabulum and femoral head in preoperative scans, 17 and the prosthetic head in postoperative radiographs. Femoral offset was defined as the distance from the centre of rotation to a line bisecting the long axis of femur. 18 Acetabular offset was defined as the distance from the centre of rotation and a line bisecting pubic symphysis. 19 Global offset was calculated as the sum of femoral and acetabular offsets.
The femoral stem alignment angle was measured by comparing the alignment of the implant to the femoral shaft axis. For the intramedullary prosthetic canal fill ratio, the stem width was measured at three levels: at the level of lesser trochanter, 2 cm below and 7 cm below. The canal fill ratio was defined as the ratio between the width of the prosthesis and the intramedullary width at each respective level. 20
Random cases were selected to evaluate inter-observer and intra-observer reliabilities for various radiographic parameters. The inter-observer correlation coefficient was the agreement between the measurements conducted by the resident and the specialist (Table 1); and the intra-observer correlation coefficient was the agreement between the first and second measurements by the resident three months apart (Table 2). These results indicated excellent inter-observer and intra-observer reliability of the measurements.
Inter-rater Reliability of Measurements.
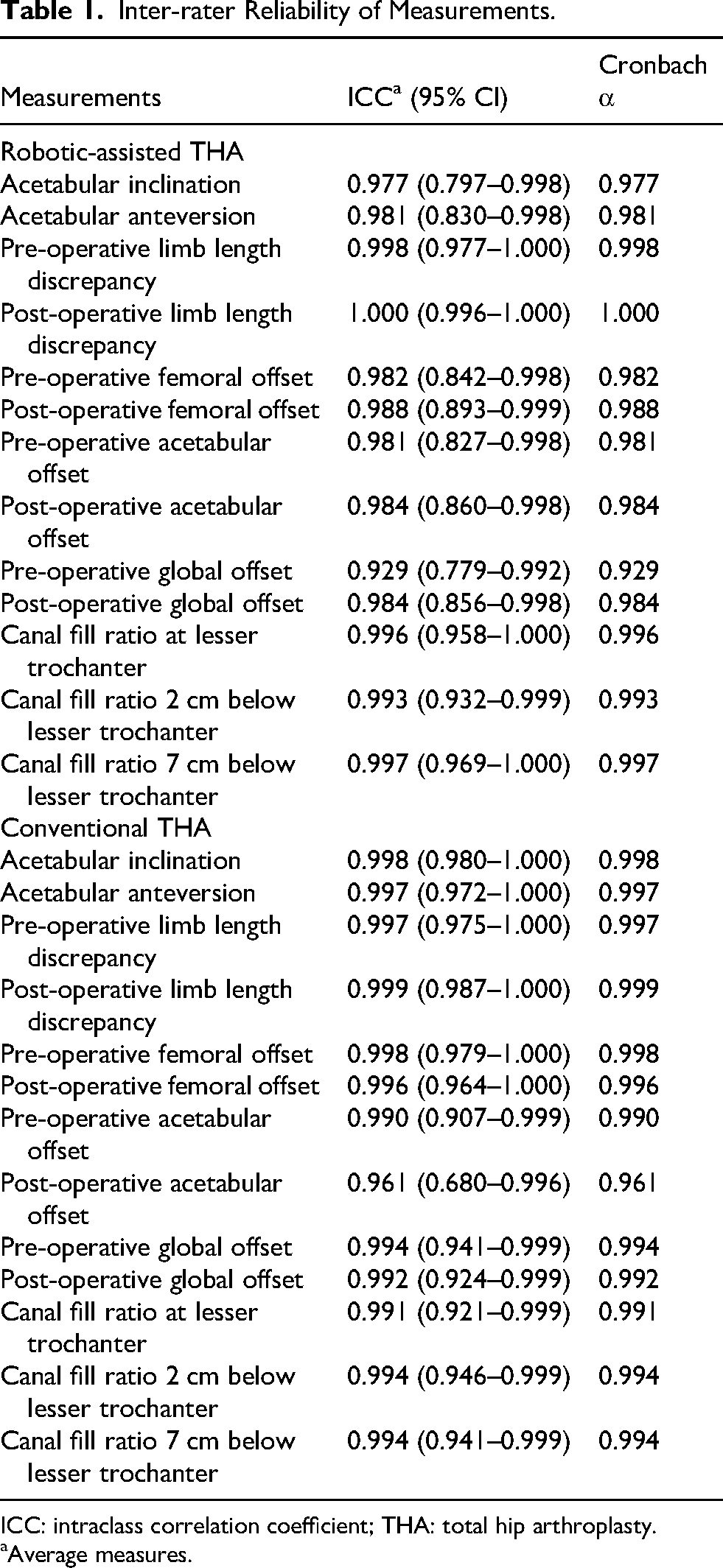
ICC: intraclass correlation coefficient; THA: total hip arthroplasty.
Average measures.
Intra-rater Reliability of Measurements.
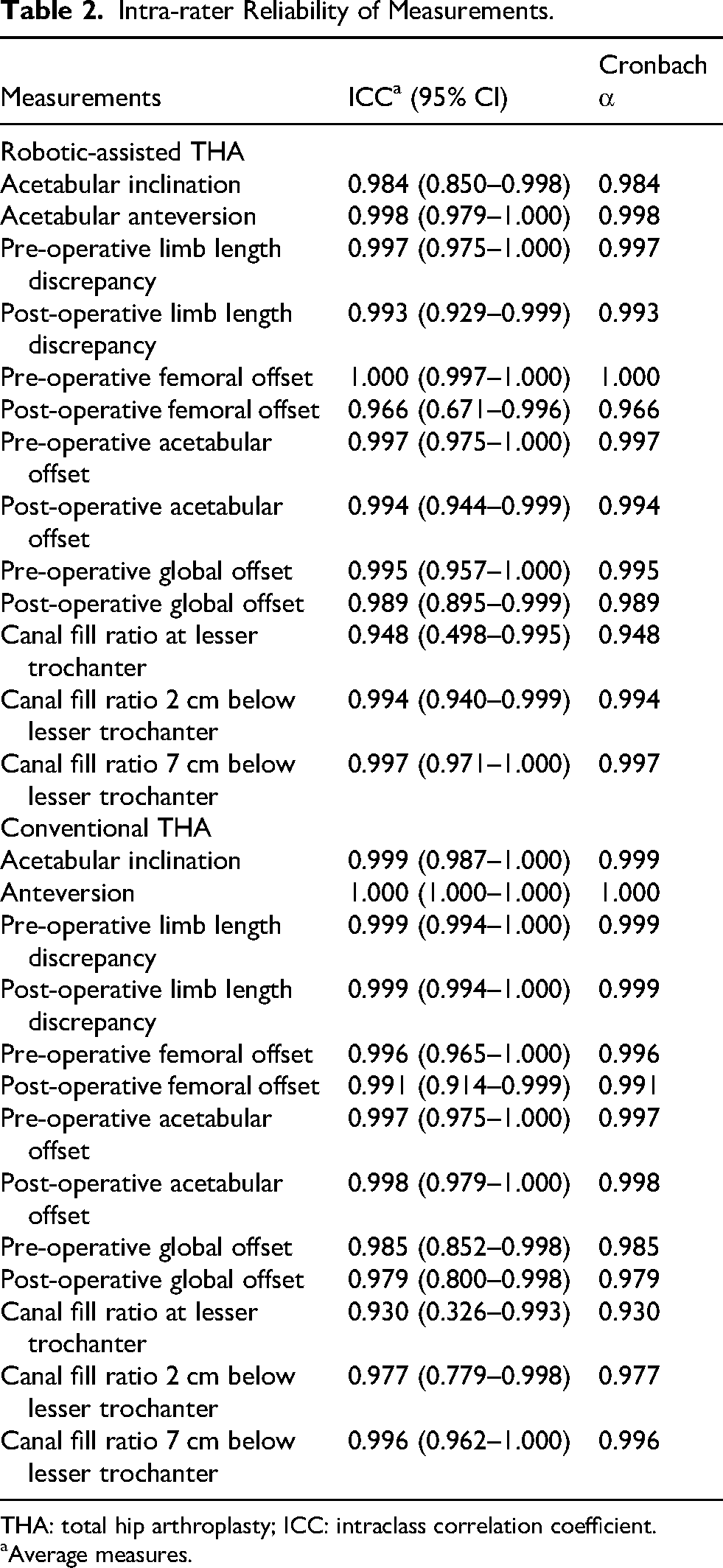
THA: total hip arthroplasty; ICC: intraclass correlation coefficient.
Average measures.
Data collection
Medical records were reviewed for all patients. Operation time was recorded as the duration from skin incision to wound closure. Blood loss was recorded intra-operatively.
Data analysis
Demographic and operative characteristics between the robotic and conventional groups were compared using the Student's t-test for continuous variables and the Chi-square test for categorical variables where appropriate. Similar analyses were conducted for radiographic parameters. Focusing specifically on acetabular cup anteversion, the dataset was further stratified based on surgical approach, namely the Southern and the Hardinge approaches. Consequently, comparisons between the robotic and conventional groups were performed separately for each surgical approach. Consistency and accuracy for acetabular inclination and anteversion at specific target angles were evaluated using descriptive statistics, root mean square error (RMSE), and the proportions of measurements within ±3°, ±5°, ±1 standard deviation (SD), and ±2 SD. Data normality was assessed with the Shapiro-Wilk test, confirming normal distribution across all groups. Distributions of acetabular inclination and anteversion were visualized using stacked histograms. All statistical analyses were conducted with IBM SPSS version 29 (IBM Corp, Armonk, NY, USA), with a significance threshold set at p < 0.05.
Results
Demographics of the patients
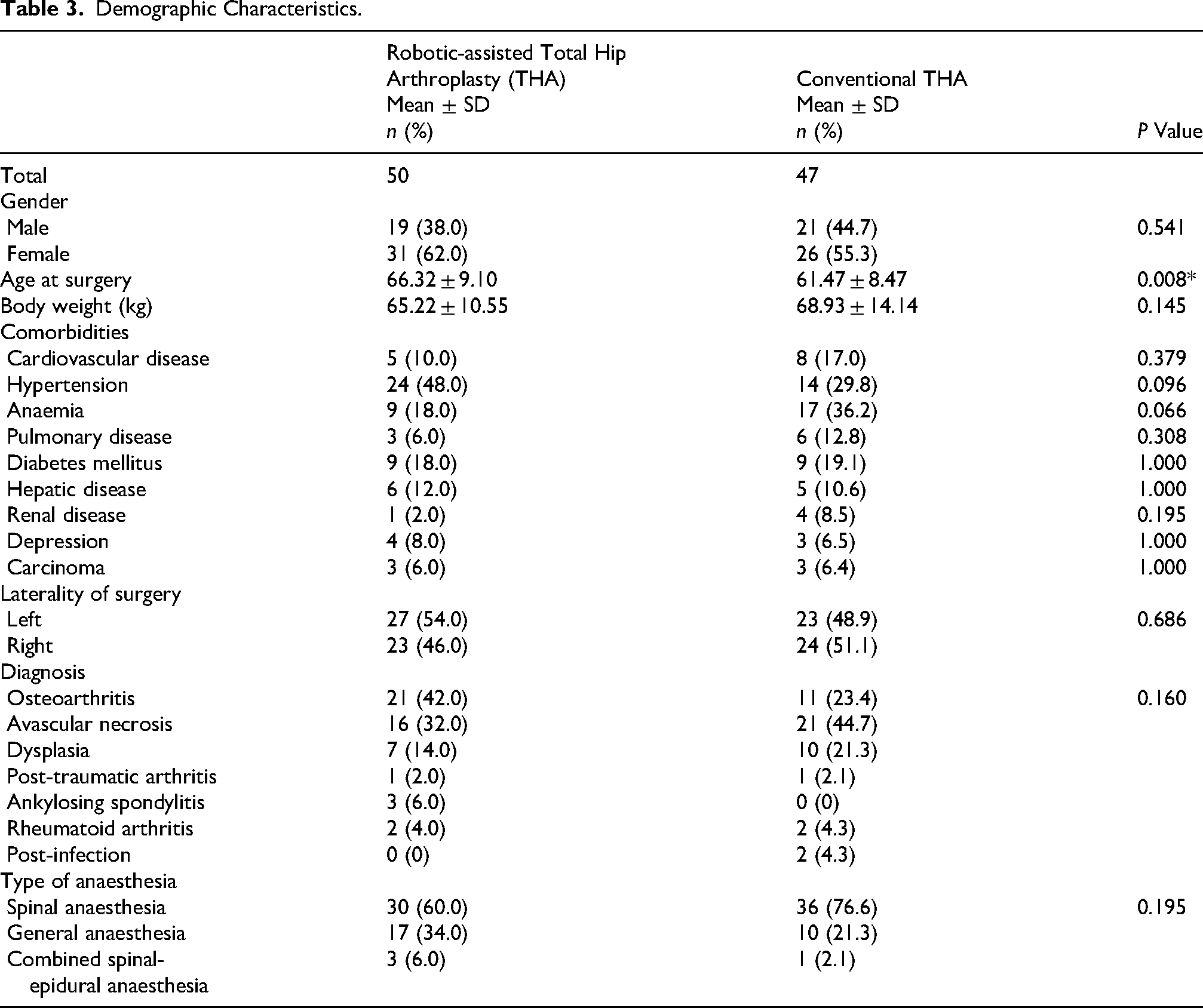
A total of 97 patients were recruited to this study: 50 patients in robotic-assisted THA cohort and 47 patients in conventional THA cohort. Table 3 provided the demographic characteristics of the subjects involved. The mean age at surgery in robotic group was 66.32 ± 9.10 compared to 61.47 ± 8.47 in conventional cohort (p = 0.008). Otherwise, there were no significant differences in terms of their gender, body weight, comorbidities, indication of surgery, laterality and anaesthesia of surgery as indicated.
Demographic Characteristics.
Radiographic parameters
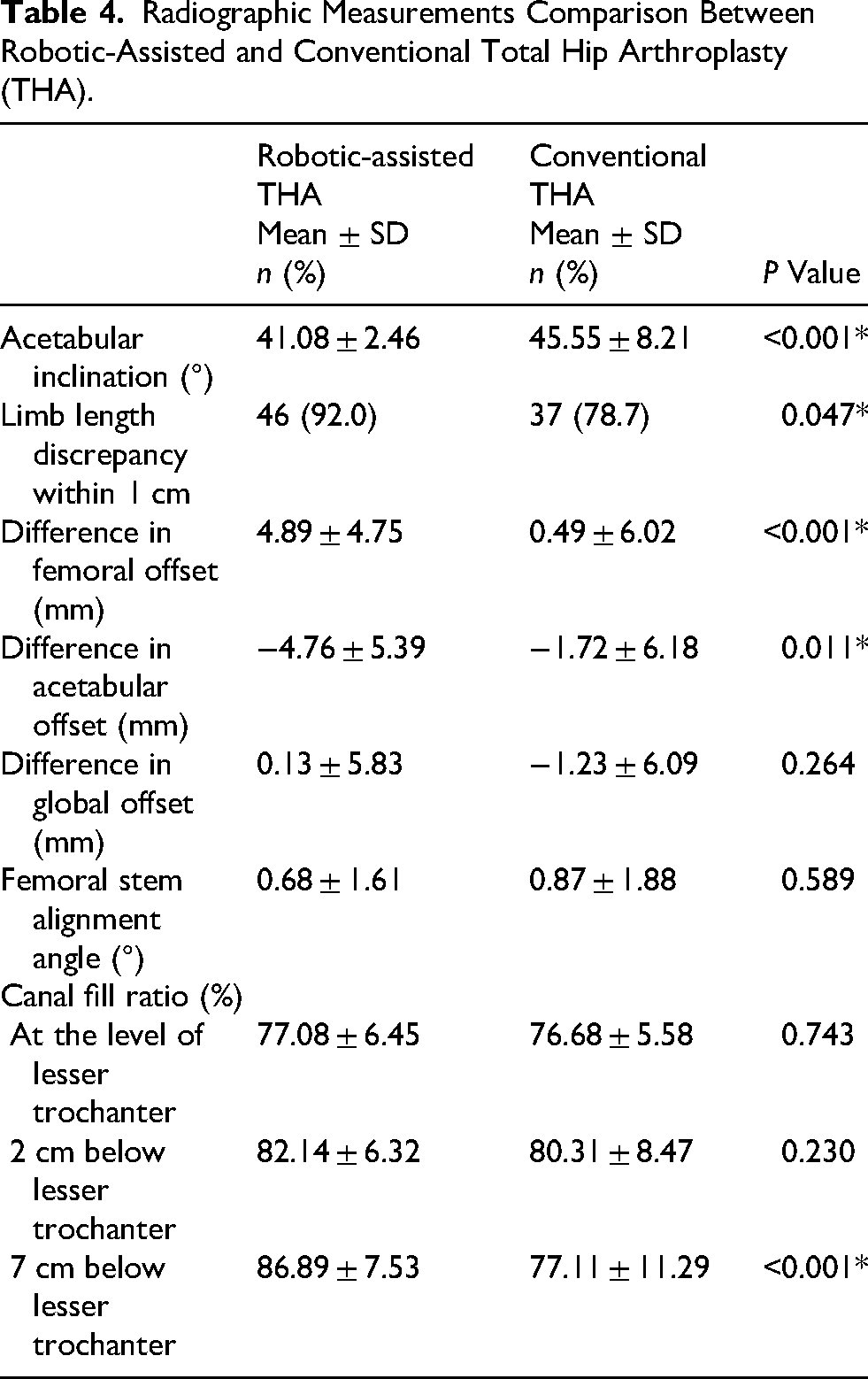
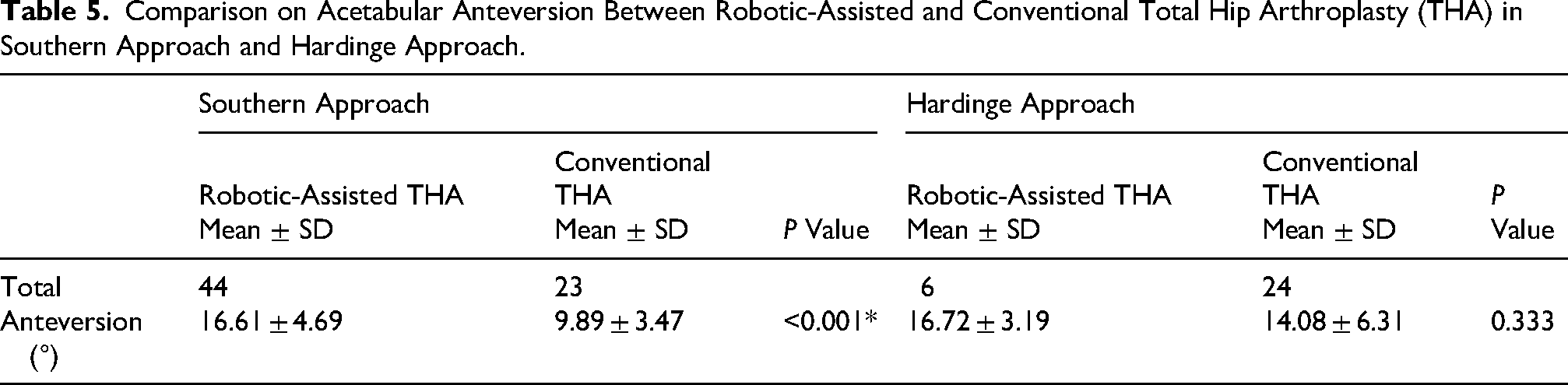
Patients in robotic group reached significantly closer to the target degree in acetabular inclination (41.08 ± 2.46° vs. 45.55 ± 8.21°, p < 0.001), more balanced post-operative limb length discrepancy (92% within 1 cm vs. 78.7%, p = 0.047), more increase in femoral offset (4.89 ± 4.75 mm vs. 0.49 ± 6.02 mm, p < 0.001), more decrease in acetabular offset (−4.76 ± 5.39 mm vs. −1.72 ± 6.18 mm, p = 0.011), and a higher canal fill ratio 7 cm below lesser trochanter (86.89 ± 7.53% vs. 77.11 ± 11.29%, p < 0.001) (Table 4). Patients in robotic group achieved significantly closer to the target anteversion (16.61 ± 4.68° vs. 9.89 ± 3.47°, p < 0.001) in Southern approach. However, this was not evident in patients underwent surgeries in Hardinge approach (Table 5). No statistically significant difference was identified in global offset, femoral stem alignment, canal fill ratio at lesser trochanter and 2 cm below lesser trochanter.
Radiographic Measurements Comparison Between Robotic-Assisted and Conventional Total Hip Arthroplasty (THA).
Comparison on Acetabular Anteversion Between Robotic-Assisted and Conventional Total Hip Arthroplasty (THA) in Southern Approach and Hardinge Approach.
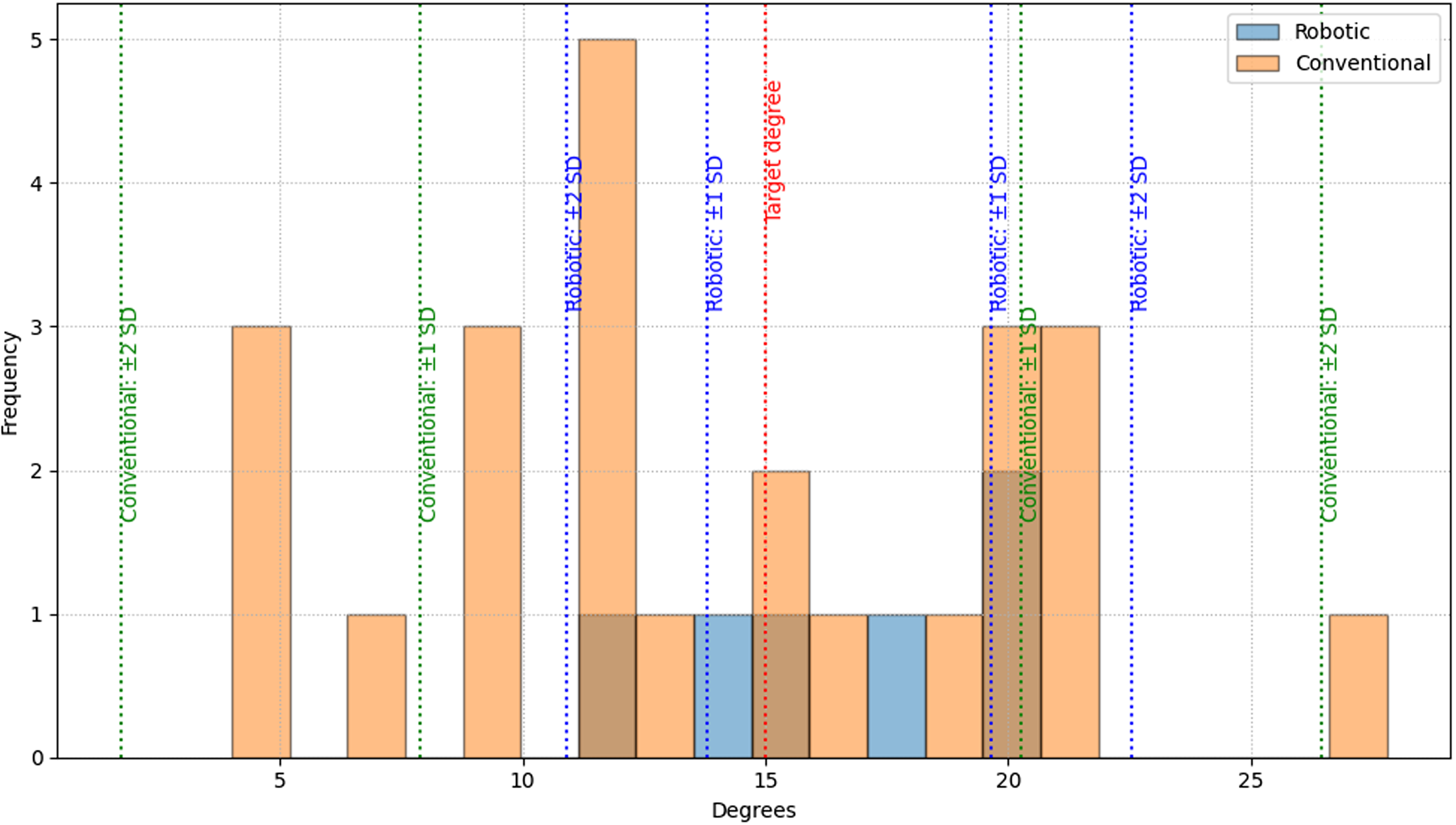
Moreover, robotic-assisted THA achieved a higher proportion of patients with acetabular inclination within 3° (88%) and within 5° (94%) of the target value (Table 6). A similar pattern was observed for acetabular anteversion: in the Southern approach, 43.2% of patients were within 3° and 63.6% within 5° of the target, while in the Hardinge approach, 50% were within 3° and 66.7% within 5° of the target (Table 7). These outcomes were statistically significantly superior to those observed with conventional THA. Similar percentages within ± 1 SD and ± 2 SD were found in all the data. Stacked histograms of the findings were presented in Figures 2–4.
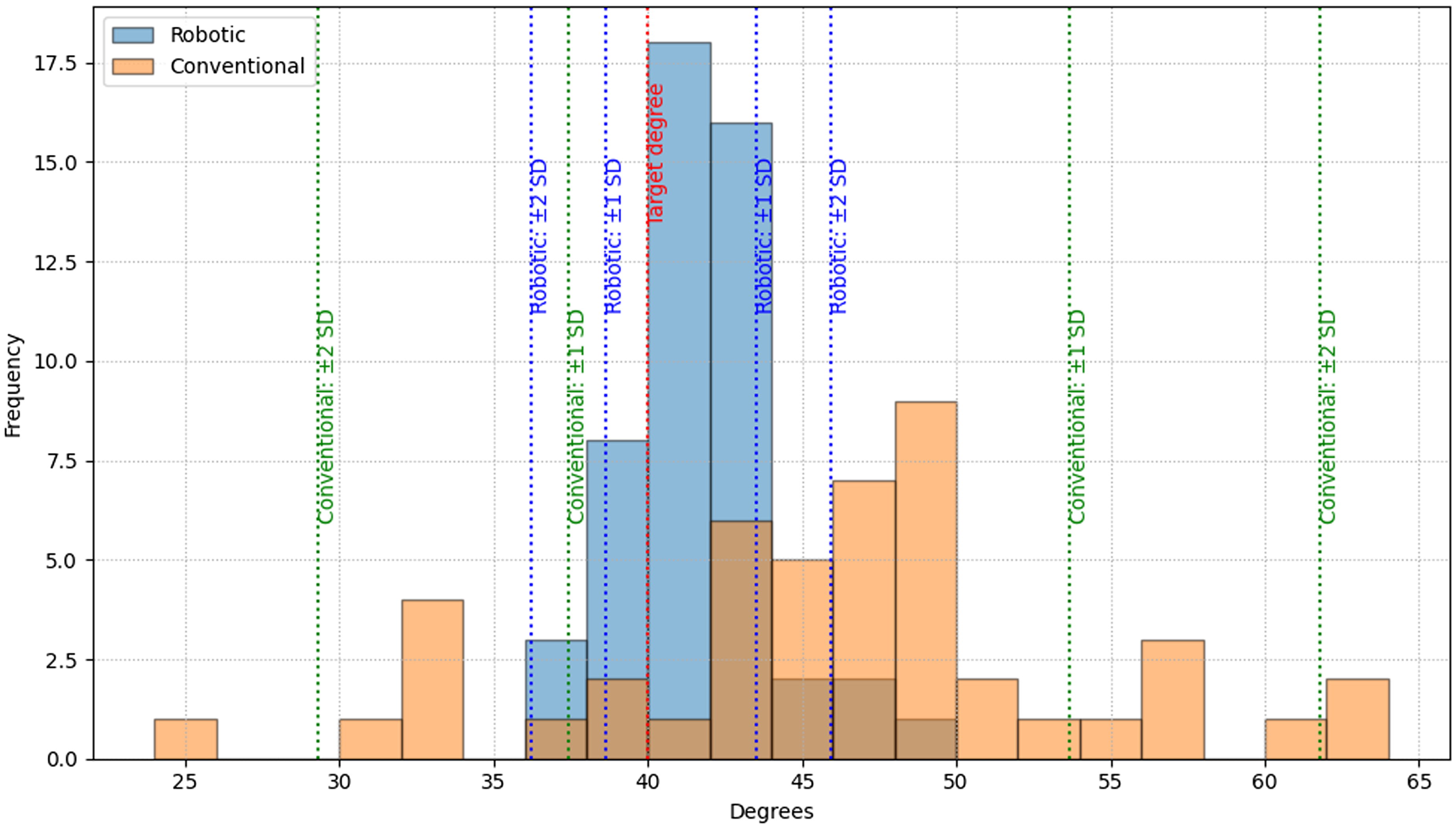
Stacked histogram showing the distribution of acetabular inclination in robotic-assisted total hip arthroplasty (THA) and conventional THA.

Stacked histogram showing the distribution of acetabular anteversion in robotic-assisted total hip arthroplasty (THA) and conventional THA in Southern approach.
Stacked histogram showing the distribution of acetabular anteversion in robotic-assisted total hip arthroplasty (THA) and conventional THA in Hardinge approach.
Consistency and Accuracy on Acetabular Inclination Comparison Between Robotic-Assisted and Conventional THA.
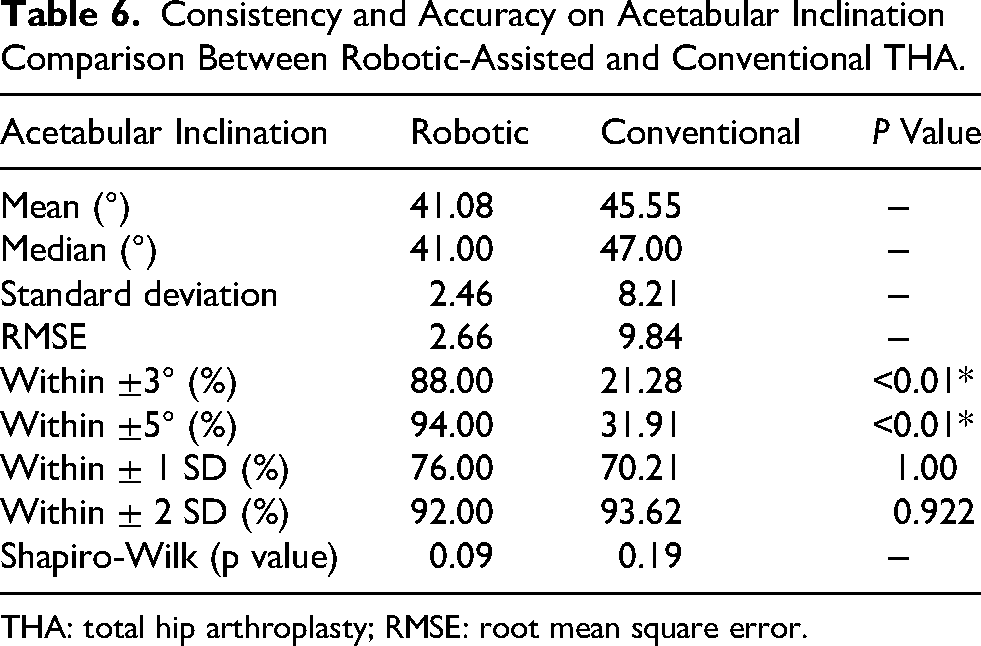
THA: total hip arthroplasty; RMSE: root mean square error.
Consistency and Accuracy on Acetabular Anteversion Comparison Between Robotic-Assisted and Conventional THA.
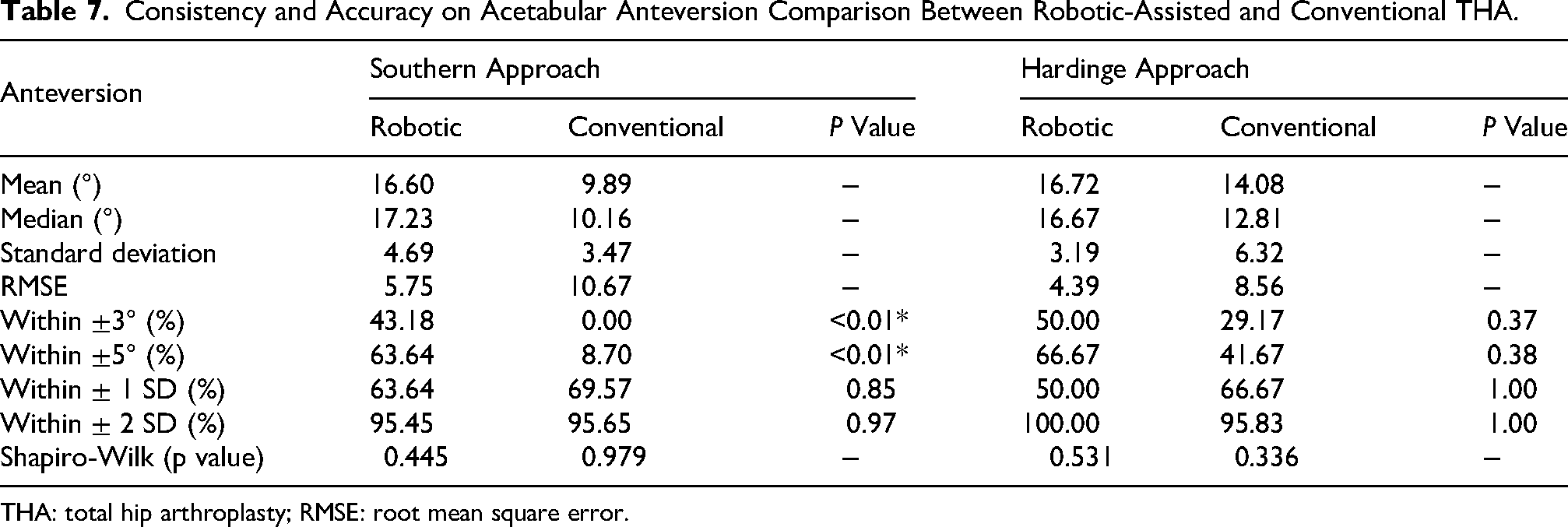
THA: total hip arthroplasty; RMSE: root mean square error.
Location of acetabular cup with reference to safe zones
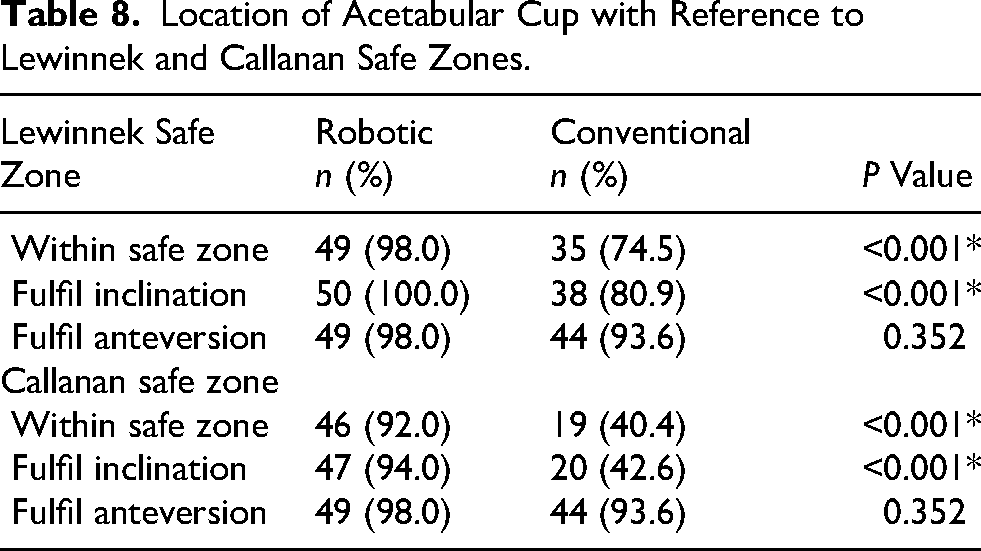
Table 8 presented the acetabular cup positions for both groups according to the safe zones defined by Lewinnek et al. 6 and Callanan et al. 7 The robotic group achieved 98% placement within the Lewinnek safe zone, compared to only 74.5% in the conventional group. A similar trend was observed for the Callanan safe zone, with 92% of the robotic group and 40.4% of the conventional group achieving the target position. When inclination and anteversion were analyzed separately, the robotic group demonstrated excellent results for both parameters within the Lewinnek safe zone, whereas most conventional cases (9 out of 47) did not meet the inclination criterion. In the Callanan safe zone, three cases in the robotic group did not reach the desired inclination, and a comparable pattern was seen in the conventional group, with only 20 of 47 patients achieving the inclination recommended by Callanan.
Location of Acetabular Cup with Reference to Lewinnek and Callanan Safe Zones.
Intra-operative and post-operative outcomes
The duration of surgery and intra-operative blood loss were slightly higher in the robotic group, but these differences were not statistically significant (Table 9). Initially, post-operative length of stay appeared comparable between the two groups. Upon further review, a case with an unusually prolonged hospital stay of 43 days was identified in the robotic group, attributed to the extended rehabilitation and placement issue related to the patient's preexisting total blindness. This case was excluded as an outlier from the length of stay analysis. After exclusion, the mean postoperative length of stay in the robotic group was 8.12 ± 4.41 days, approximately one day shorter than the conventional group's 9.21 ± 4.54 days, although this difference remained statistically non-significant.
Intra-operative Outcomes Comparison Between Robotic-Assisted and Conventional THA.
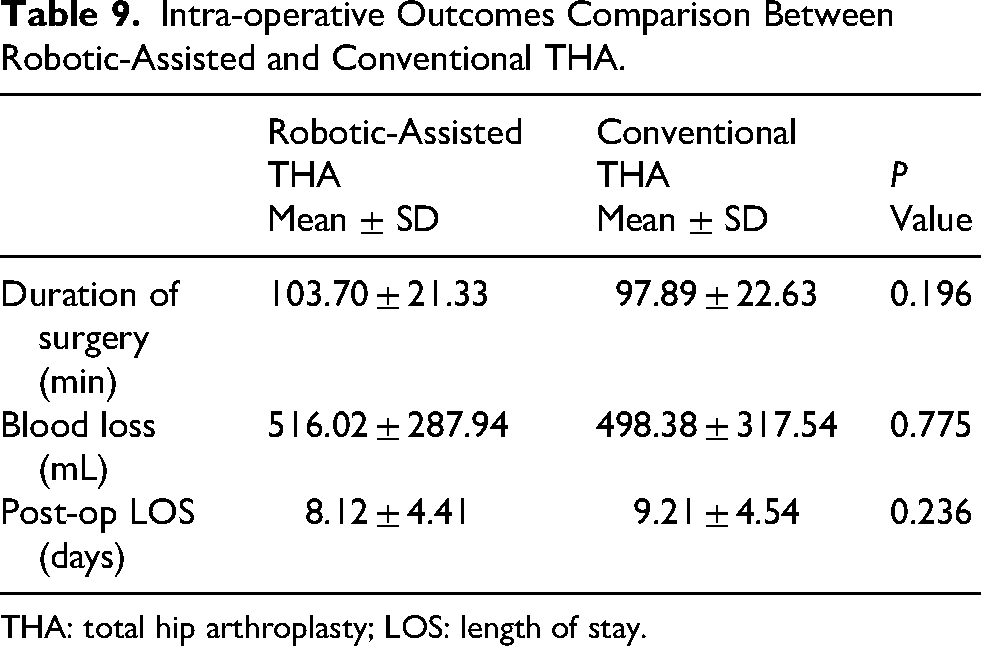
THA: total hip arthroplasty; LOS: length of stay.
With respect to surgical complications within the first year of follow-up, two patients (4%) in the robotic group experienced early complications: one periprosthetic fracture and one case of peroneal nerve palsy. In the conventional group, three patients (6.4%) developed early complications, comprising two periprosthetic fractures and one case of sciatic nerve palsy. No cases of dislocation, prosthetic loosening, prosthetic joint infection, or revision surgery were observed in either group.
Discussion
The MAKO robotic-assisted THA enabled surgeons to implant components with greater precision and consistency, reducing the incidence of significant post-operative leg length discrepancy.21–22 Notably, this advantage was observed across various surgical approaches. 23 Not only did it allow consistently accurate placement of the acetabular cup, but the MAKO system also enhanced pre-operative planning and templating compared with the conventional technique. For instance, Shaw et al. 24 reported that robotic-assisted surgery can significantly lower the risk of instability and dislocation. Domb et al. 25 also reported favourable 5-year outcomes with robotic-assisted THA, including higher clinical scores, a significant reduction in acetabular cup misplacement beyond Lewinnek and Callanan safe zone by 89% and 79%, respectively. Moreover, Loke et al. 21 similarly observed that robotic assistance enhanced over 40% more successful component placements within the Lewinnek safe zone and nearly 60% more within the Callanan safe zone.
In our cohort, the robotic group demonstrated more precise and consistent inclination of acetabular cup (41.08° ± 2.46° vs. 45.55° ± 8.21°). Stratifying by surgical approaches, patients undergoing the Southern approach achieved significantly more accurate acetabular anteversion (16.61° ± 4.69°) with robotic-assisted surgery; however, this difference was not seen with the patients who underwent surgery in the Hardinge approach. A higher proportion of patients in the robotic group achieved cup placement within the Lewinnek safe zone (98% vs. 74.5%), with an even more remarkable trend for Callanan safe zone (92% vs. 40.4%). The robotic-assisted technique not only increased the rate of accurate placement of acetabular cup, but also enhanced the consistency: over 95% of robotic cases achieved acetabular inclination within 5° of the target, in contrast to less than 35% only in the conventional group. Furthermore, approximately two-thirds of the patients in robotic group had acetabular cup placed within 5° of the target anteversion, compared to only 8.7% and 41.7% for Southern approach and Hardinge approaches, respectively, in the conventional group. Collectively, these findings strongly supported the superior accuracy and consistency of robotic-assisted THA in acetabular component positioning.
Spinopelvic relationship and the concept of the lumbopelvic complex 26 carried important implications for acetabular component planning and positioning. The MAKO system could help surgeons place the acetabular cup more precisely by accounting for the dynamic behaviour of the spinopelvic junction. It allowed pre-operative three-dimensional templating that incorporated sacral slope measurements from standing and sitting radiographs, enabling surgeons to visualize the relationship between acetabular cup and femoral head in various angles of hip motion. This approach may enhance surgical outcomes and minimize the risk of prosthetic impingement, instability and dislocation.
Ankylosing spondylitis may alter the spinopelvic relationship, and thereby increase the risk of complications. In cases of pathological spine-hip relations, individualized acetabular cup positioning may be required to optimize surgical outcomes. Within this cohort, three patients in the robotic group suffered from ankylosing spondylitis, whereas no patients in the conventional group were affected. These three cases were therefore evaluated independently before inclusion in the cohort, with reference to the Bordeaux Classification of Spine-Hip Relations. 26 After assessing pelvic incidence and the difference in sacral slope between standing and sitting radiographs, one case was classified type 1A (pelvic incidence <40° and sacral slope difference in sacral slope >10°), and other two cases were classified as type 2A (pelvic incidence 40°–60° and sacral slope difference >10°). None of the three cases required additional individualization of the acetabular cup planning. Therefore, all three cases were included in the study without introducing additional bias into the analysis.
Conversely, the benefit of robotic-assisted THA in reducing postoperative limb length discrepancy was less pronounced. Shimizu et al. 27 found out that there was no difference in limb length discrepancy beyond 5 or 10 mm between robotic-assisted and conventional THA, despite minor differences in the absolute values. This finding was in accordance a meta-analysis published in 2024. 10
Difference in limb length below 10 mm would be asymptomatic after THA.28–29 Thus, this supported our use of this as a threshold for evaluation. We found that significantly more patients (46 in 50) achieved balanced limb length with robotic-assisted THA. Potential contributing factors included: (i) more accurate placement of acetabular cup; (ii) more accurate intra-operative limb length measurements facilitated by the navigation function in MAKO robotic system. However, in conventional THA, there were also methods in prevention of limb length discrepancy. Supine patient positioning, for example, in direct anterior approach, could allow direct measurement of limb length and use of intra-operative fluoroscopy to facilitate balanced limb length after surgery. 30
Both groups in our study showed excellent restoration of global offset, which is crucial in improvement of the gait pattern, pain and health-related quality of life after surgery. 31 However, the robotic group further benefited from better medialization of the acetabular cup and increased femoral offset. The biomechanical advantage of such placement had been proposed long ago by Charnley. 32 A decrease in acetabular offset could effectively reduce the stress applied to prosthetic joint. 33 It was believed that increase in femoral offset up to 5 mm could improve clinical outcomes following THA, 18 including enhancing functions of hip abductors and external rotators, 34 and improving post-operative Oxford hip score. 35 These biomechanical improvements may endow the robotic group with functional advantages.
Our findings revealed similar precision in femoral stem alignment and proximal canal fill ratio between groups. Inadequate proximal femoral filling could impair osteointegration. 36 Though some difference in canal fill ratio was observed in distal part of femoral stem, this might reflect variations in femoral morphology, implant design, but not the difference in surgical technique adopted. Our results proved that both methods were equally effective for successful femoral stem sizing and placement in THA.
Robotic-assisted THA was associated with slightly longer surgery duration and increased intra-operative blood loss, although neither was significant. These results aligned with the expected learning curve, as reported in the literature – approximately 12–13 cases per surgeons for mastery.37–38 Additional time for placement of array and checkpoints, setup and registration with the robotic system might account for the difference in time required for surgery. A longer operative time would also be associated with a larger blood loss experienced during the procedure. Notably, with increased surgical experience, operative times decreased, reducing from a mean of 113.7 min in the first ten cases to 86.7 min in the last ten cases of our early robotic-assisted THA series, ultimately surpassing the efficiency of conventional surgery.
Some studies suggested that robotic-assisted THA might reduce hospital length of stay. A study in 2021 by Remily et al. 39 reported a shorter duration of stay (3.4 days) in patients receiving robotic-assisted THA in comparison with conventional THA (3.7 days). Another recent Spanish study in 2023, 22 which included their early series of MAKO robotic-assisted THA cases, reported a mean length of stay of 4.4 days – significantly shorter than the 5.7 days documented in a prior nationwide study involving 141 hospitals. 40 In our cohort, this advantage was also observed; however, the difference was not statistically significant, and overall hospital stays exceeded those reported in previous literatures.22,40–41 Factors, such as age, gender, 42 comorbidity burden, score on the American Society of Anaesthesiologists assessment, 43 might contribute to this outcome. This warranted further investigation within our population.
Both procedures demonstrated low rates of early post-operative complications. Within first year follow-up, only 3 in 47 (6.4%) patients in conventional group experienced complications, whereas in the robotic group, only 2 patients (4%) among 50 suffered from early complications. One patient from each group suffered from Vancouver type A2 fracture intra-operatively over the medial femoral neck during femoral broaching. Both cases were treated with cerclage wiring around the proximal femur. It was postulated that it could be resulted from technical error during the procedure, for instance varus placement of the broach during insertion or removal. As both groups shared similar incidence of this complication in a similar fracture pattern, it does not suggest being related to additional procedures required in robotic-assisted surgeries, which included the placement of femoral checkpoint. Another patient in the conventional group experienced an anterior acetabular wall osteophyte fracture during the reduction of the prosthesis. This was treated with the use of three acetabular screws for fixation of the acetabular cup without requirement of additional osteosynthesis. One patient in the conventional group suffered from sciatic nerve palsy after the surgery. One patient in robotic group experienced peroneal nerve palsy after the operation. None of our patients suffered from dislocation, prosthetic loosening, prosthetic joint infection, or revision surgery within the first year follow-up. This was supported by previous literature, which reported that complications were low in both MAKO robotic-assisted (mean: 3.0%) and conventional THA (mean: 3.5%), and no difference was identified between the two procedures. 21
There were several limitations in this study. First, the reliance on X-ray radiographs, instead of CT scans, might have reduced measurement accuracy, particularly regarding acetabular anteversion and centre of rotation. Second, limb length discrepancy was assessed only at the hip joint level, without accounting for the entire lower limb using full-length radiographs. Third, although patient demographics were generally comparable, the robotic group consisted of significantly older individuals, which might have introduced confounding effects to the outcomes. Fourth, the involvement of multiple surgeons introduced variability in surgical experience, representing an additional potential confounding factor. Fifth, this study involved the use of three different choices of implants. Variations between the implant designs could potentially influence the radiological analysis, for instance the canal fill ratio of the femoral stem. Finally, the sample size and follow-up duration were limited, highlighting the need for larger-sample-size, longer-term studies to validate these findings and reduce confounding influences. Additionally, future research should incorporate clinical outcome assessments to explore the relationship between radiological parameters and patient satisfaction following surgery.
Conclusion
Robotic-assisted THA significantly improved the precision and consistency of implant placement and effectively reduced postoperative limb length discrepancy compared to conventional techniques. Importantly, these advantages were achieved while maintaining similar levels of safety and surgical efficiency. Although our findings were promising, further research involving larger patient cohorts and extended follow-up periods is essential to fully understand the long-term clinical benefits and potential impact of robotic-assisted THA on patient outcomes.
Footnotes
Ethical considerations
This study has been approved by the Central Institutional Review Board of the Hospital Authority of Hong Kong S.A.R. under the reference CIRB-2025-243-5. Consents for participation and publication are not applicable in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article. Raw data that support the findings of this study are available from the corresponding author, upon reasonable request.