
Abstract
Hallux valgus is a common disorder of the foot that is often coupled with metatarsus varus, which may cause pain, discomfort and affect shoe wear. Studies have shown that the first intermetatarsal angle (IMA) can be significantly reduced after first metatarsophalangeal joint arthrodesis alone; however, the presence of long-term interval change in the first IMA after first MTPJ arthrodesis is still controversial. This retrospective observational study aims to evaluate the radiographic outcomes of first metatarsophalangeal joint arthrodesis for hallux valgus deformities. Patients who received first MTPJ arthrodesis for management of hallux valgus deformity between January 2011 and December 2018 were reviewed. Angular measurements of the HVA and first IMA were performed on X-Rays of these patients taken at pre-operation, early post-operative (4–6 weeks) and at final follow up. Patients who received X-rays at 1 year, 2 years, and 4 years post-operation, were also evaluated for first IMA and HVA on these X-rays. About 88 patients were evaluated, with final follow up ranging between 9 and 565 weeks. The pre-operative mean HVA of 42.6 (95% CI [40.3, 44.9]) degrees was significantly reduced (p < 0.001) to a mean HVA of 10.4 (95% CI [8.9, 11.7]) degrees at 4–6 weeks after first MTPJ arthrodesis. The pre-operative mean first IMA of 16.9 (95% CI [16.2, 17.7]) degrees was significantly reduced (p < 0.001) to a mean IMA of 11.8 (95% CI [11.2, 12.5]) degrees at 4–6 weeks after first MTPJ arthrodesis. There was a small statistically significant reduction in the first IMA between early post-operation and at 1 year post-operation (0.96 degrees – 1.87 degrees, depending on subgroup). First metatarsophalangeal joint arthrodesis is effective in reducing the widened first IMA associated with hallux valgus deformity, and is able to maintain the correction upon long-term follow-up.
Introduction
Hallux valgus is a common disorder of the foot, which may cause pain, discomfort and affect shoe wear and walking. First metatarsophalangeal joint (MTPJ) arthrodesis is a well-established treatment option for symptomatic hallux valgus, especially in cases with severe deformity, associated with first MTPJ degenerative changes, secondary to rheumatoid arthritis or secondary to neurological conditions. First MTPJ arthrodesis was reported to be an effective treatment option for hallux valgus by Clutton in 1894. 1 Subsequently there have been multiple further studies reporting satisfactory and reproducible long-term results when used for treatment of hallux valgus with severe deformity or with degenerative changes, including significant deformity correction, reduced pain and improved functional outcomes.2–5
Hallux valgus deformities are known to be coupled with metatarsus primus varus leading to a widening of the forefoot, 6 this is particularly apparent in severe cases of hallux valgus. Multiple studies have shown that the first intermetatarsal angle (IMA) can be significantly reduced after first MTPJ arthrodesis alone.7–16 A systematic review by Dayton et al. 17 has demonstrated that the single procedure of first MTPJ arthrodesis can significantly reduce the first IMA in patients with all ranges of severity of hallux valgus deformity, hence additional metatarsal osteotomy procedures are not necessary to correct the metatarsus primus varus component of the hallux valgus deformity.
However, the presence of long-term interval change in the first IMA after first MTPJ fusion is still controversial. Results reported by Costa and colleagues 16 showed a loss of correction of 0.2 degrees at mean follow up of 58 months. In comparison, a study by Cronin and colleagues 7 in 2006 detected an additional 4 degrees or more of correction achieved between 6 weeks and the final follow up visit in 20% of the patients reviewed.
In addition, most previous studies have evaluated Caucasian patients, and there is limited data on the outcome of first MTPJ arthrodesis in Asian patients. At baseline, Asian feet tend to be shorter and wider than their Caucasian counterparts. 18 Hallux valgus and metatarsus primus varus lead to further pathological widening of the forefoot, which may cause more difficulties in tolerating with shoe wear. Hence adequate correction of the metatarsus primus varus in Asian patients with symptomatic hallux valgus is important.
The purpose of this retrospective study is to evaluate the radiographic outcomes of first metatarsophalangeal joint arthrodesis for hallux valgus deformities in a group of ethnically Chinese patients from a single centre in Hong Kong, and to evaluate whether there are further interval changes in the first intermetatarsal angle after initial correction.
Methodology
This is a single-centre retrospective single-arm observational study. Operation records of patients with hallux valgus deformities treated with first metatarsophalangeal joint arthrodesis between January 2011 and December 2018, performed by the Department of Orthopaedics and Traumatology at a single regional hospital in Hong Kong were reviewed. Patients were included in the study if they were 18 years of age or above at the time of operation, ethnically Chinese, and had first metatarsophalangeal joint arthrodesis performed with any fixation technique. Patients were excluded from the study if they had prior surgery undergone on the first ray.
Angular measurements of the hallux valgus angle (HVA) and intermetatarsal angle (IMA) were performed on dorsoplantar radiographs of the foot of these patients at 3 time points: pre-operative, early post-operative (4–6 weeks), and final follow up. If available, radiographs taken at 1 year, 2 years and 4 years post-operation were also evaluated.
HVA and IMA were measured according to recommendations by the American Orthopaedic Foot and Ankle Society as described by Coughlin, 19 where the reference points for angular measurements were placed equidistant from the outer border of the medial and lateral cortices of the respective bone, at 1 to 2 cm from the proximal and distal joint surfaces for the first and second metatarsals, and at 0.5 to 1 cm from the proximal and distal joint surfaces for the first proximal phalanx.
The mean scores for the HVA and IMA for each time point were calculated, and data analysis was conducted using repeated measures ANOVA to identify significant differences between the time points. The level of significance is set at a p value of below 0.05.
Results
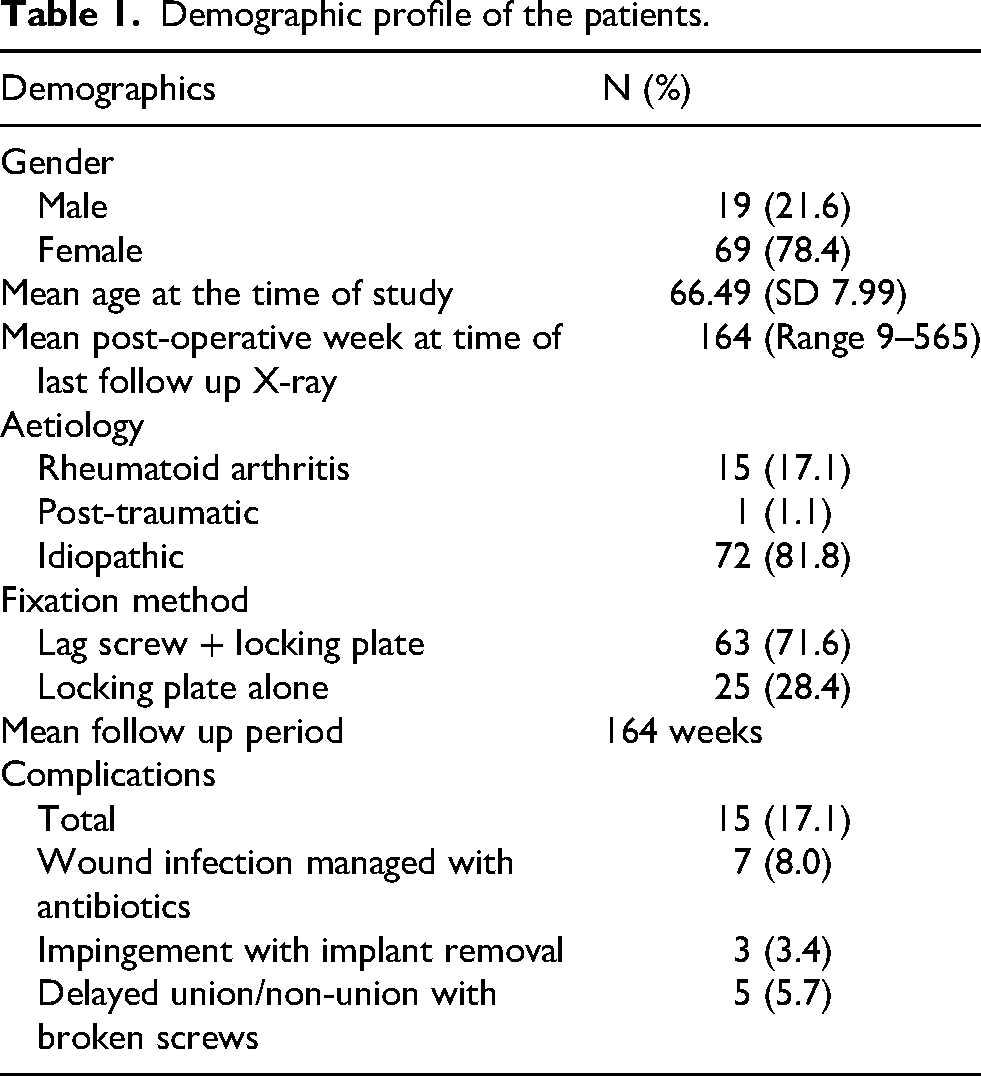
About 88 patients were included in our study, with a mean follow-up period of 164 weeks. The study group consisted of 19 male patients and 69 female patients, with a mean age of 66.49 years at the time of operation. About 15 patients had underlying rheumatoid arthritis, one patient had history of prior trauma and 72 were idiopathic. All operations were performed with a dorsal longitudinal skin incision, and the first MTPJ prepared with a spherical cup and cone articular preparation technique. About 63 patients had the first MTPJ fixed with a lag screw and a locking plate whilst 25 patients had fixation with a locking plate only.
About 15 patients developed post-operative complications, including seven patients with wound infection managed by antibiotics, three patients had implant impingement requiring operation for implant removal, delayed union with broken screws was noted in five patients, four of these patients were asymptomatic, but one patient required re-operation for revision fixation (Table 1).
Demographic profile of the patients.
The pre-operative mean HVA of 42.6 (95% CI [40.3, 44.9]) degrees was significantly reduced (p < 0.001) to a mean HVA of 10.4 (95% CI [8.9, 11.7]) degrees at 4–6 weeks after first MTPJ arthrodesis. The mean HVA at final follow up was 1.045 degrees greater than the mean HVA at 4–6 weeks, which was a significant increase (p = 0.009) (Figure 1).

Pre-operative vs. post-operative HVA.
The pre-operative mean first intermetatarsal angle (IMA) of 16.9 (95% CI [16.2, 17.7]) degrees was significantly reduced (p < 0.001) to a mean IMA of 11.8 (95% CI [11.2, 12.5]) degrees at 4–6 weeks after first MTPJ arthrodesis. At final follow up, the mean IMA was maintained at 11.4 (95% CI [10.7, 12.2]), which was not significantly different (p = 0.479) from the early post-operative first IMA (Figure 2).
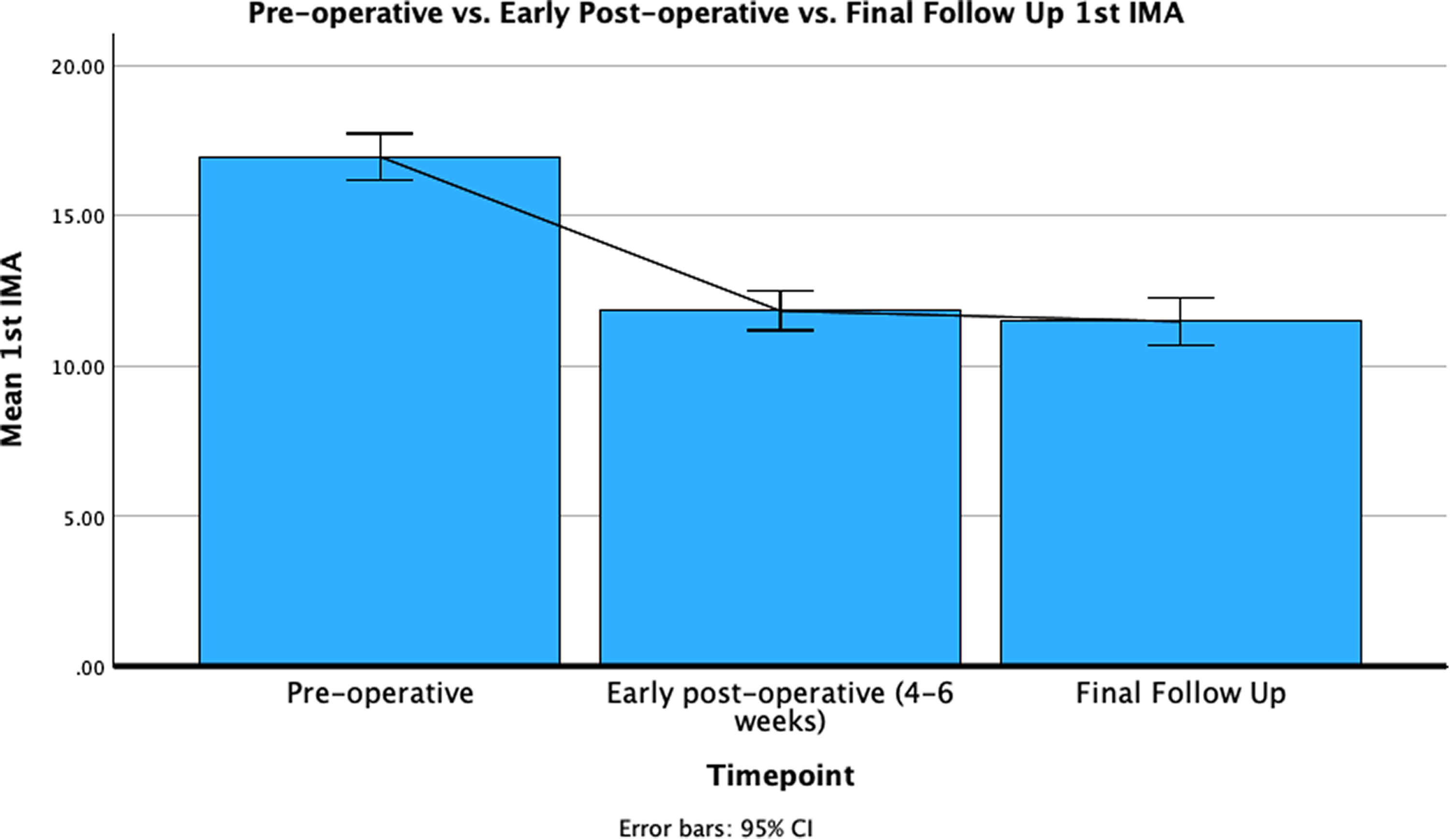
Pre-operative vs. early post-operative vs. final follow up first IMA.
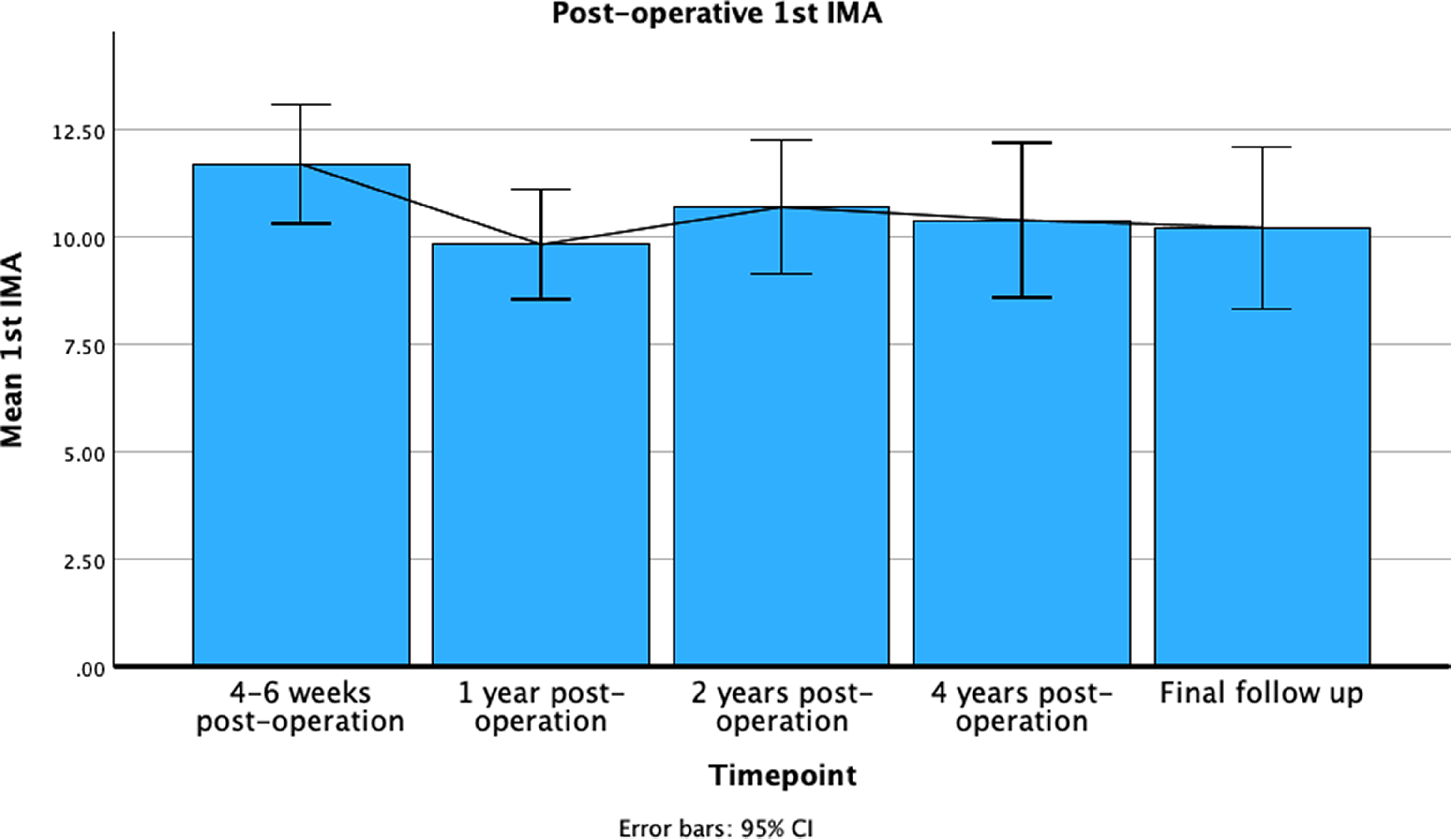
When analysing a subgroup of 68 patients who had radiographs performed at post-operative 1 year, the mean first IMA at 4–6 weeks was further significantly reduced (p = 0.001) by 0.96 degrees at 1 year post-operation to 10.6 (95% CI [9.9, 11.3]) degrees. In this subgroup, the first IMA at final follow up was not significantly different (p = 1.000) from the first IMA at 1 year (Figure 3).
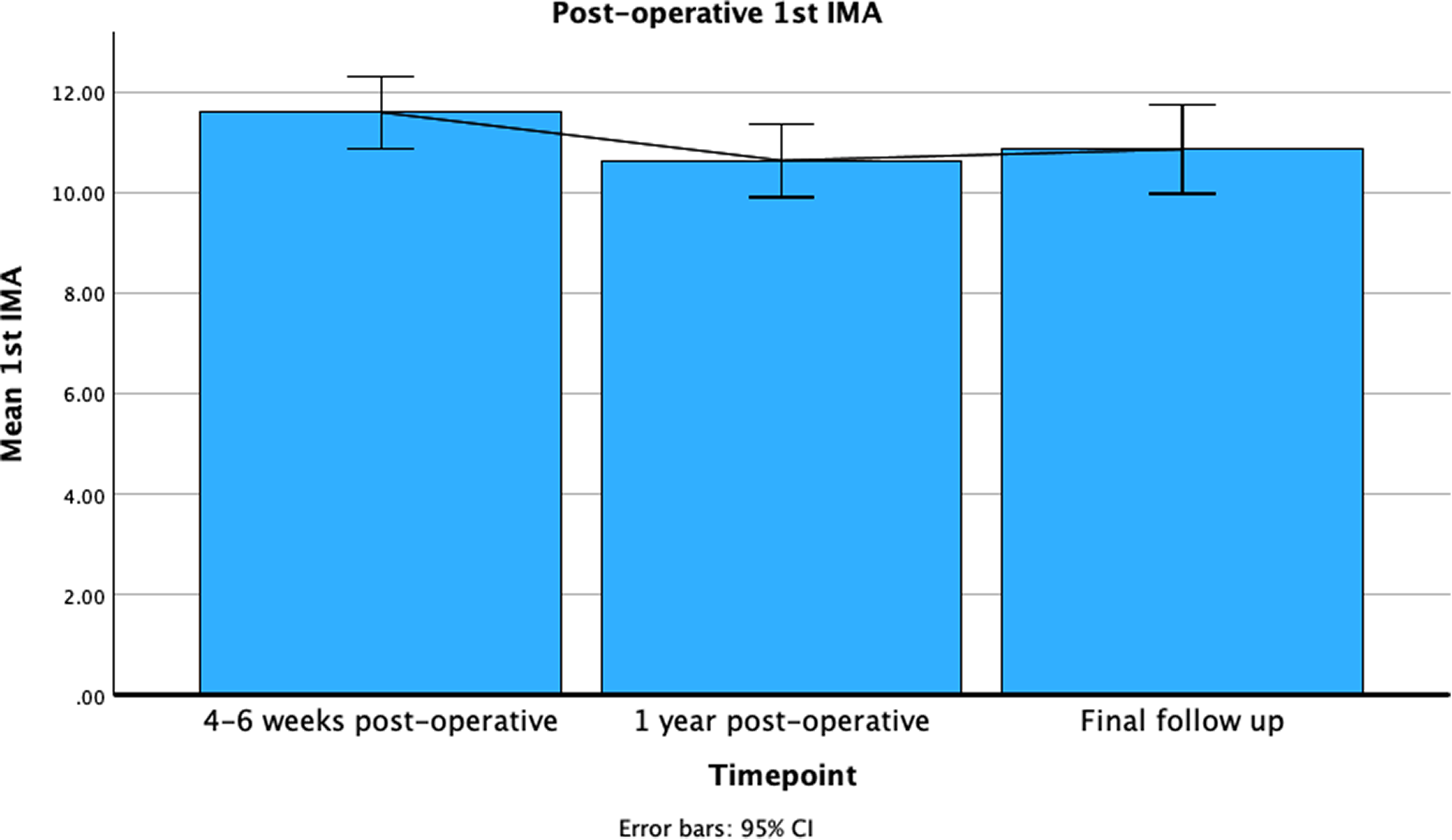
Longitudinal first IMA changes in subgroup with radiographs performed at 1 year post-operation.
Similarly, in a subgroup of 51 patients who had radiographs performed at post-operative 1 year and at post-operative 2 years, the mean first IMA at 4–6 weeks was also significantly reduced (p < 0.001) by 1.3 degrees at 1 year post-operation to 10.5 (95% CI [9.6, 11.3]) degrees. In this subgroup, there was no further significant change of the mean first IMA at 2 years (p = 0.465) and at final follow up (p = 1.000) (Figure 4).
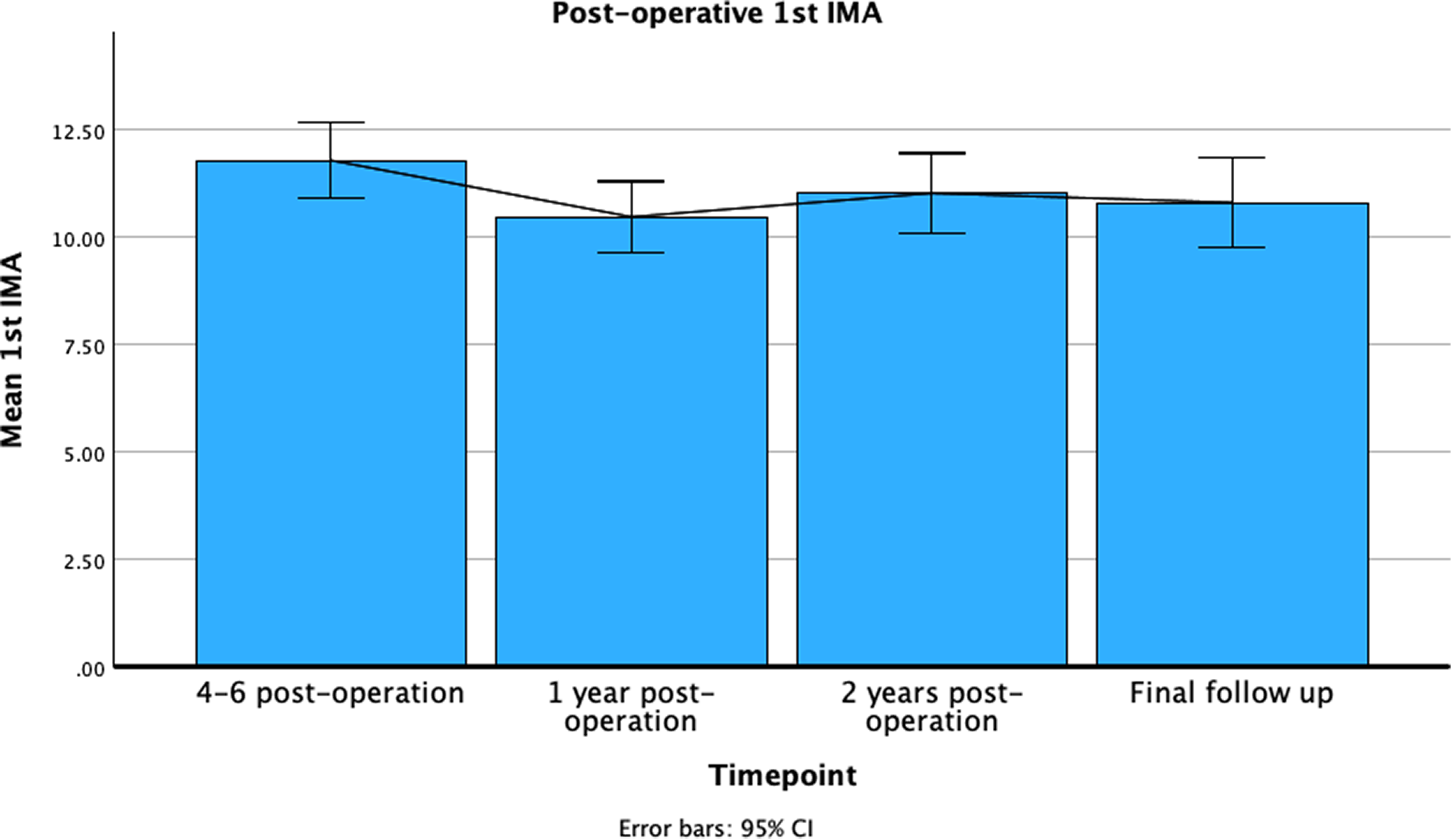
Longitudinal first IMA changes in subgroup with radiographs performed at 1 year and 2 years post-operation.
In a subgroup of 23 patients who had radiographs performed at post-operative 1 year, 2 years and 4 years, the mean first IMA at 4–6 weeks was significantly reduced (p = 0.007) by 1.87 degrees at 1 year post-operation to 9.8 (95% CI [8.5, 11.1]) degrees. In this subgroup, there were no further significant changes of the mean first IMA at 2 years (p = 1.000), 4 years (p = 1.000) or at final follow up (p = 1.000). (Figure 5)
Longitudinal first IMA changes in subgroup with radiographs performed at 1 year, 2 years and 4 years post-operation.
Discussion
In our retrospective single-center series of ethnically Chinese patients, first metatarsophalangeal joint arthrodesis has provided reliable correction of both the hallux valgus angle and the first intermetatarsal angle, and this correction was maintained at medium to long term follow up. The mean first IMA was reduced from 16.9 degrees to 11.8 degrees at 4 to 6 weeks post operation and maintained at 11.4 degrees at final follow up (mean: 164 weeks), with no significant loss of correction over time. The subgroup analyses with radiographs obtained at 1, 2, and 4 years post-operatively demonstrated small additional reductions in the first IMA at 1 year (0.96–1.87 degrees), which were not followed by further significant changes at subsequent time points. These findings support the use of first metatarsophalangeal arthrodesis as a definitive procedure for correction of hallux valgus associated with metatarsus primus varus and suggests that the achieved reduction in the first IMA is radiographically stable.
Our results are consistent with previous reports that isolated first MTPJ arthrodesis can reliably reduce the first IMA without the need for additional proximal first metatarsal osteotomy procedures. Mann and Katcherian 15 reported that the intermetatarsal angle correction was proportional to the pre-operative intermetatarsal angle, and therefore first MTPJ arthrodesis alone is able to achieve adequate correction of the first IMA even in feet with a large pre-operative intermetatarsal angle. Subsequent series have also consistently supported these findings. Dayton et al. 11 reported a mean reduction of 6.41 degrees in patients with pre-operative first IMAs greater than 15 degrees. Feilmeier et al. 20 reported a mean reduction of the first IMA by 5.44 degrees, with a larger mean reduction in patients with more severe deformities. Sung et al. 10 reported a reduction of the mean first IMA from 14.0 degrees to 9.7 degrees, and also noted that as the severity of the deformity increased, the amount of first IMA correction also significantly increased. A systematic review by Dayton et al., 17 pooling 15 studies and a total of 701 first MTPJ arthrodesis procedures reported a mean pre-operative first IMA of 13.74 degrees and a post-operative first IMA of 9.38 degrees, with a mean reduction of 4.36 degrees. And in the subgroup analysis, their results also concurred that patients with a greater initial deformity had a greater degree of first IMA correction after first MTPJ arthrodesis.
The mechanism by which first MTPJ arthrodesis corrects the first IMA has not been definitively established, but several biomechanical explanations have been proposed. Humbert 14 suggested that in hallux valgus, the valgus deviation of the hallux causes lateral bowstringing of the extensor hallucis longus and flexor hallucis longus tendons, which reinforces the action of the adductor hallucis muscle and pushes the first metatarsophalangeal head proximally and medially to further increase the metatarsus primus varus; fusion of the joint eliminates these deforming influences. Cronin 7 proposed that the mechanism for correction of the first IMA is due to the action of the adductor hallucis, which prior to first MTPJ arthrodesis works as a deforming force by inserting through the lateral sesamophalangeal ligament at the base of the first proximal phalanx to exacerbate the valgus deformity at the first MTPJ; however once the first MTPJ is fused, these adduction forces have an increased lever arm, and acts on the first metatarsal as well, instead of the proximal phalanx only, and hence works to correct the varus malalignment. Pydah et al. 9 also similarly hypothesised that the lateral pull of the adductor hallucis may assist in reducing the first IMA but emphasized the importance of a concomitant mobile metatarsocuneiform joint. Feilmeier et al. 20 postulated that the reduction in the medially directed retrograde force from the hallux on the metatarsal after correction of the first MTPJ alignment is the main reason for the IMA decreases post first MTPJ arthrodesis. Though these mechanisms remain theoretical and have not been experimentally confirmed, the immediate post-operative reduction and maintenance of the first IMA over time observed in our cohort are consistent with the notion that first MTPJ arthrodesis neutralizes the deforming soft tissue forces and permits passive or dynamic rebalancing of the first ray.
Longitudinal changes in the first IMA after the early post-operative period remain controversial. Costa et al. 16 reported a statistically insignificant finding of a small loss of correction (0.2 degrees) at a mean follow up period of 58 months, suggesting that, in their series, the initial correction of the first IMA was largely maintained. In contrast, Cronin et al. 7 observed that in 20% of their patients, there was an additional 4 degrees or more of improvement between 6 weeks and final follow up, raising the possibility of progressive, active correction over time.
Our study is one of the few to evaluate serial radiographs at sequential time points after arthrodesis. We found a small statistically significant reduction in the first IMA between early post-operation and at 1 year post-operation (0.96 degrees–1.87 degrees, depending on subgroup). However, we believe that these relatively small longitudinal changes detected should be interpreted with caution because the magnitude of these changes are substantially smaller than the measurement error previously reported for the first IMA by Condon et al. 21 and by Resch et al. 22 which were 3.60 degrees and 5.4 degrees respectively. It was also noted that in our results, the hallux valgus angle showed a significant increase of 1.045 degrees when comparing the early-post-operation and final follow up radiographs. This increase again is less than the degree of measurement error for HVA reported by Resch et al. 22 which was 6.4 degrees. Furthermore, our early post-operative radiographs were mostly performed without weightbearing so as to protect the arthrodesis construct, whereas the latter radiographs were more likely to be performed whilst weightbearing, which may have affected the angle measurement as per previously reported by Boszcyzyk et al. 23 More importantly, we did not detect further significant changes in the intermetatarsal angle beyond 1 year up to final follow up (mean: 164 weeks). This supports the conclusion that, in our cohort, most of the deformity correction is established by the early post-operative period, and any subsequent longitudinal change appears to be minimal and of doubtful clinical significance.
Most prior studies on first MTPJ arthrodesis for hallux valgus have involved a predominantly Caucasian population. It is known that Asian foot shapes tend to be relatively shorter and wider than foot shapes of populations from Caucasian descent. 18 Given that hallux valgus and metatarsus primus varus further increase forefoot width, it is possible that correction of the first IMA may be particularly important for shoe wear and comfort in Asian patients. Our study adds to the data on Asian patients receiving first MTPJ arthrodesis, as it consists of an exclusively ethnically Chinese cohort. The results show that the degree of radiographic correction of the first IMA in this Chinese cohort was comparable to that reported in the literature. This suggests that first MTPJ arthrodesis is similarly effective in reducing the varus component of the first ray irrespective of underlying ethnic differences in foot morphology. Future work incorporating measurements of forefoot width, functional footwear outcomes or three-dimensional imaging may help to clarify the effects of first MTPJ arthrodesis on improving shoe wear concerns in hallux valgus patients.
In our cohort, 17.1% of patients experienced post-operative complications, most of which were minor and manageable (seven superficial wound infections treated with antibiotics; three symptomatic implant impingements managed with implant removal). Delayed union or nonunion with broken screws occurred in five patients (5.7%), but only one patient required revision surgery. These rates are comparable to those described previously in the literature where nonunion rates typically range from approximately 0% to 8%.2–5,7,10–13,24–28
Several limitations of this study should be acknowledged. Firstly, its retrospective design and reliance on available radiographic records introduces inherent selection bias. And also, because of its retrospective design, the follow up period was not uniform, and only a subset of patients had radiographs at 1, 2 and 4 years resulting in smaller sample sizes for the longitudinal subgroup analyses. Secondly, the angular measurements were performed by a single observer, and the absence of repeated measurements may have hindered the angular measurement accuracy. Thirdly, we did not systematically collect clinical outcome scores and functional measures, which would have allowed for correlation between radiograph correction and patient centered outcomes.
In conclusion, our study supports current evidence that first metatarsophalangeal joint arthrodesis alone can reduce the first intermetatarsal angle in patients with hallux valgus. The correction of the first intermetatarsal angle can be achieved at early post-operation and maintained at subsequent longer-term follow-up.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.