
Abstract
Introduction
Fragility fracture is strongly associated with significant morbidity and mortality. Multiple studies have shown that a critical gap exists between osteoporosis burden and the implementation of relevant investigation and treatment following primary fragility fracture. The purpose of this study was to examine whether adequate osteoporosis investigation or treatment has been offered to surgically treated fragility fracture patients. Another purpose was to investigate whether osteoporosis treatment is associated with a lower readmission rate of repeated fragility fracture.
Methods
A retrospective study of the patients admitted with hip fracture and distal radius fracture from 1 July 2016 to 30 June 2021 was conducted. The patients were followed up for 2 years and are divided into three groups, including the control group, the Calcichew only group and the group with both calcichew and bisphosphonate. We tried to find out the readmission rate of repeated fragility fracture and the prevalence of new symptomatic osteoporotic vertebral collapse in different patient groups.
Results
From 2016 to 2021, a total of 515 patients were included in this study. All of them underwent surgery after suffering from either a hip fracture or a distal radius fracture. Approximately 69.3% of the patients were female (n = 357) while 30.7% of them were male (n = 158). Approximately 63.5% of them suffered from hip fracture (n = 327), while 36.5% of them suffered from distal radius fracture (n = 188). Overall, a dual-energy X-ray absorptiometry scan was arranged in only 8.2% (n = 42) of the patients. Only 14% (n = 72) of the patients were given both calcichew and bisphosphonate, while 25.6% of them (n = 132) had only calcichew prescribed after surgery. Approximately 5.2% (27 out of 515) of the patients were readmitted due to repeated fragility fracture. Approximately 70.4% (19 out of 27) and 29.6% (8 out of 27) of the patients belong to the control group and the calcichew only group, respectively. None of the patients in the group with both calcichew and bisphosphonate was readmitted for recurrent fragility fracture. Approximately 3.7% (19 out of 515) of the patients suffered from new symptomatic osteoporotic vertebral collapse. Approximately 47.4% (9 out of 19), 21.1% (4 out of 19), and 31.6% (6 out of 19) of the patients belong to the control group, the calcichew only group and the group with both calcichew and bisphosphonate, respectively. A significant reduction in the readmission rate of repeated fragility fracture was observed in the active treatment group treated with both calcichew and bisphosphonate (vs. control group: P-value = 0.035; vs. calcichew group: P-value = 0.041).
Conclusion
Our study showed suboptimal osteoporosis management after primary fragility fracture. Patients subsequently were prone to suffering from repeated fragility fracture. The patients receiving both calcichew and bisphosphonate were associated with a significant reduction in the readmission rate of repeated fragility fracture. The results implied that osteoporosis management should be started earlier after the first fragility fracture.
Introduction
The prevalence of osteoporosis in Hong Kong is gradually increasing due to an ageing population, with life expectancy for males and females reaching 82.5 years and 87.9 years, respectively, in 2023.1,2 The prevalence of osteoporosis in people aged ≥50 years in Hong Kong is reported to be as high as 37% in one of the epidemiology studies. 3
Fragility fracture is defined to result from low-energy trauma by a fall from standing height or less, signifying underlying osteoporosis. 4 According to the study consisting of 4000 community-dwelling older adults in Hong Kong, there were 7% of men and 11% of women suffering from ≥1 incident of major fragility fracture over 9.9 and 8.8 years of follow-up, respectively. 5
The mortality rate of hip fragility fracture was reported to be up to 24% in the first year. 4 Loss of independence is prevalent, with 60% of the survivors requiring walking aid, and 33% being totally dependent or in a nursing home in the first year after hip fragility fracture. 6 The direct cost was estimated to be HK$81,120 to treat each hip fracture in Hong Kong public hospital. This is equivalent to an annual estimated cost of HK$511 million in the Hong Kong public healthcare system. 7
Treatment of osteoporosis by anti-osteoporosis drugs, including bisphosphonates, has been demonstrated to improve bone mineral density and reduce future fracture risk. 8 Despite the high prevalence and significant consequences of osteoporosis, a critical gap exists between the disease burden and the implementation of appropriate investigation and treatment. According to territory-wide retrospective studies, only 6% to 15% of patients received osteoporosis medication after hip fracture, while only 8.4% of patients received medication after distal radius fracture.9,10 The patients suffering from one fragility fracture are predisposed to a higher risk of sustaining a second fragility fracture, especially in the first two years after the initial fragility fracture. 4 However, little local data have been published to investigate the relationship between the osteoporosis medication following fragility fracture and the readmission rate of repeated fragility fracture.
The objective of this retrospective cohort study was to examine whether adequate osteoporosis investigation or treatment has been offered to surgically treated fragility fracture patients. Another objective was to investigate whether osteoporosis treatment is associated with a lower readmission rate due to repeated fragility fracture.
Methods
Study design
This longitudinal study investigated the clinical outcome of surgically treated patients suffering from hip or distal radius fractures from 1 July 2016 to 30 June 2021. Ethical approval was obtained from the Joint CUHK-NTEC Clinical Research Ethics Committee. All patients were extracted from the Clinical Data Analysis Reporting System (CDARS), the central patient database in public healthcare system.
Study participants
Eligible patients (1) sustained an index fragility fracture of the hip or distal radius during the study period; (2) at the time of their index fracture were ≥65 years old and admitted to North District Hospital; and (3) underwent surgery to manage their index fracture.
Exclusion criteria were (1) pathological fracture, (2) high-energy trauma, (3) previous exposure to anti-osteoporosis medication, or (4) patients undergoing conservative treatment.
Outcome measures
Demographic data (age and sex) and clinical details, including the type of fragility fracture and surgical procedure, were collected from the Hospital Authority Clinical Management System.
The patients with a history of surgically treated hip or distal radius fracture were divided into three groups, including the control group, calcium and vitamin D (calcichew) only and both bisphosphonates and calcichew. Only alendronate was used in this study because it is the first-line bisphosphonate medication in the public healthcare sector. Drug compliance of every patient was assessed in each follow-up to determine whether all medication had been completed. This is documented in the progress note in the Hospital Authority Clinical Management System.
The clinical information of these three patient groups were reviewed in the subsequent two years after their index fracture, including (1) the total number of patients undergoing a dual-energy X-ray absorptiometry (DEXA) scan within six months of the index injury, (2) the total number of patients starting anti-osteoporosis medication after surgery and the type of treatment patients received, (3) the readmission rate of repeated fragility fracture, and (4) the prevalence of symptomatic osteoporotic vertebral collapse. The clinical outcome was examined by comparing these three patient groups in terms of the readmission rate of repeated fragility fracture and the prevalence of new symptomatic vertebral collapse. The patients with symptomatic vertebral fracture were included in this study when they presented with new episodes of back pain with radiological evidence of new vertebral collapse. They were identified when they were re-admitted to public hospitals or presented to outpatient clinics.
Data analysis
All clinical data were stored anonymously in an encrypted file to protect personal data privacy.
Statistical analysis was performed by using IBM SPSS Statistics Version 29. Categorical data were illustrated as frequencies and percentages, while continuous data were presented as mean.
Independent t test or analysis of variance was performed to compare the baseline parameter (mean age, gender, and type of index operation) among different surgically treated fragility fracture and treatment groups, respectively.
Chi-squared test was used to estimate any significant association between anti-osteoporosis medication and (1) readmission rate of repeated fragility fracture, and (2) the prevalence of symptomatic vertebral collapse. A P-value of <0.05 was considered statistically significant.
Results
Baseline statistics
From 1 July 2016 to 30 June 2021, 638 patients were filtered from CDARS. Approximately 123 patients were excluded because of the following reasons: (1) <65 years old (n = 101), (2) previous exposure to anti-osteoporosis medication (n = 6), (3) high-energy trauma (n = 11), and (4) pathological fracture (n = 5) (Figure 1).
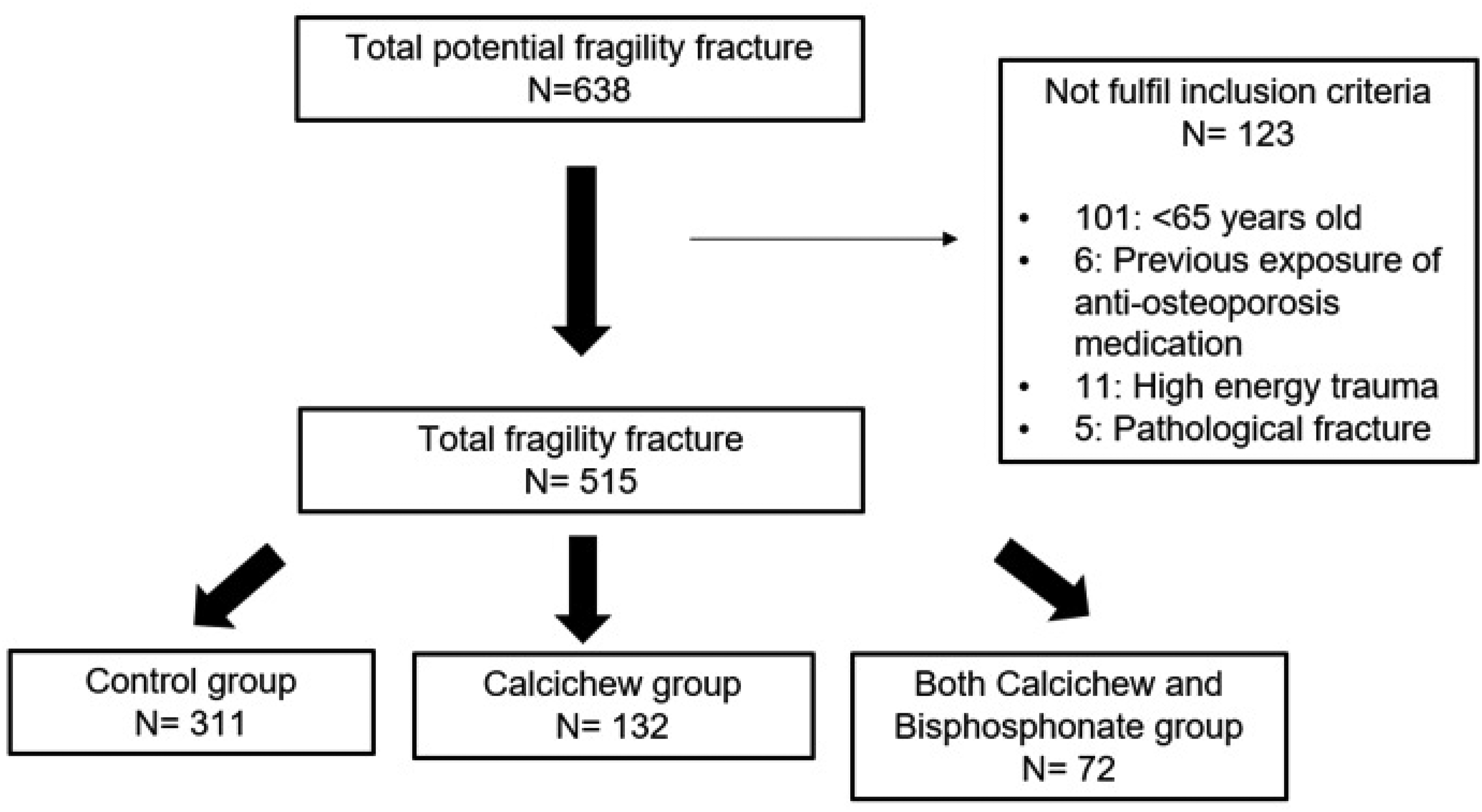
Flowchart showing how many patients were excluded and allocated into different patient groups.
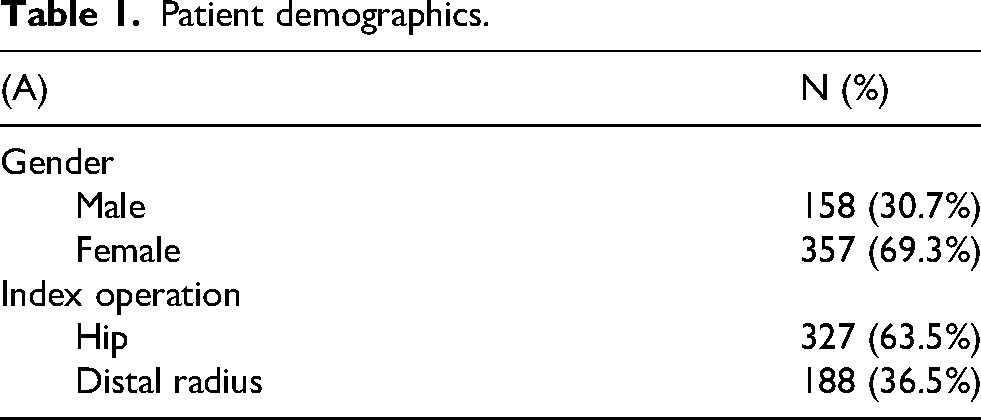
In total, 515 patients were included and underwent surgery following primary fragility fracture. Approximately 63.5% (327 out of 515) and 36.5% (188 out of 515) of the patients suffered from hip or distal radius fracture, respectively. The mean age of these patients was 75.8 (range 65–100 years old). Approximately 30.7% of the patients were male (n = 158), while 69.3% of the patients were female (n = 357) (Table 1(A) and (B)).
Patient demographics.
F: female; M: male.
Data in bold are statistically significant.
The patients suffering from fragility hip fracture (mean age: 80.5) are statistically older than those with distal radius fracture (mean age: 73.9; P-value = 0.001). On the other hand, there is no statistically difference in sex ratio between the groups of hip and distal radius fracture (P-value = 0.739; Table 1(B)).
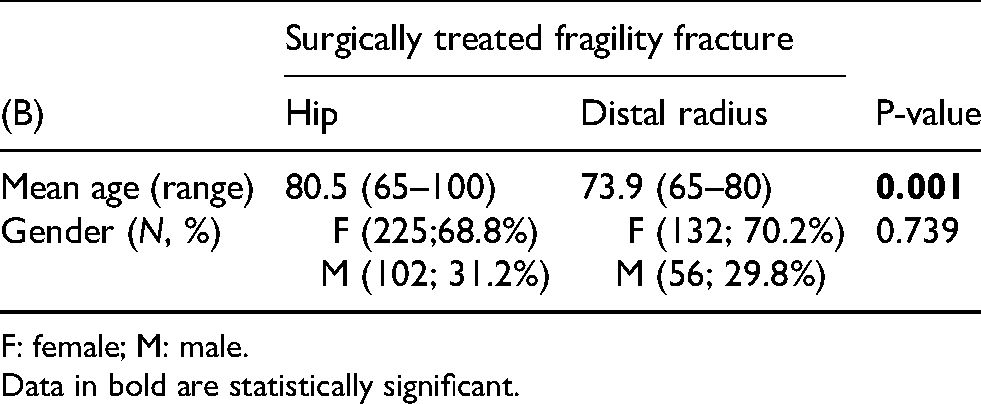
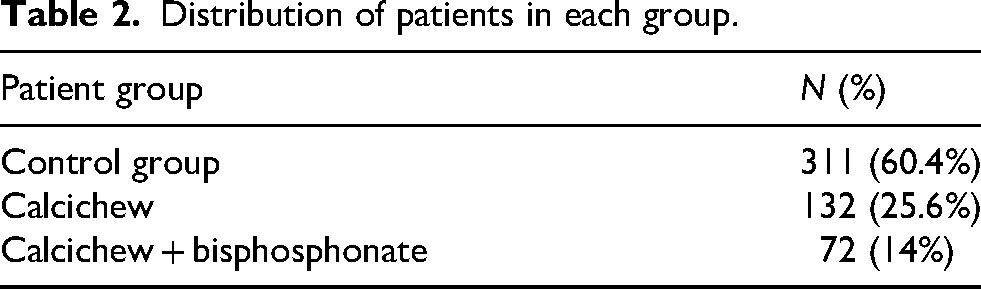
Approximately 60.4% of the patients did not have any osteoporosis medication after fragility fracture (n = 311), while 25.6% of the patients took only calcichew (n = 132). The remaining patients (14.0%, n = 72) were prescribed both bisphosphonates and calcichew (Table 2).
Distribution of patients in each group.
The patient demographics of these three groups do not show any statistically significant difference in terms of mean age, sex ratio and types of index surgeries (Table 3).
Patient demographics in each patient group.
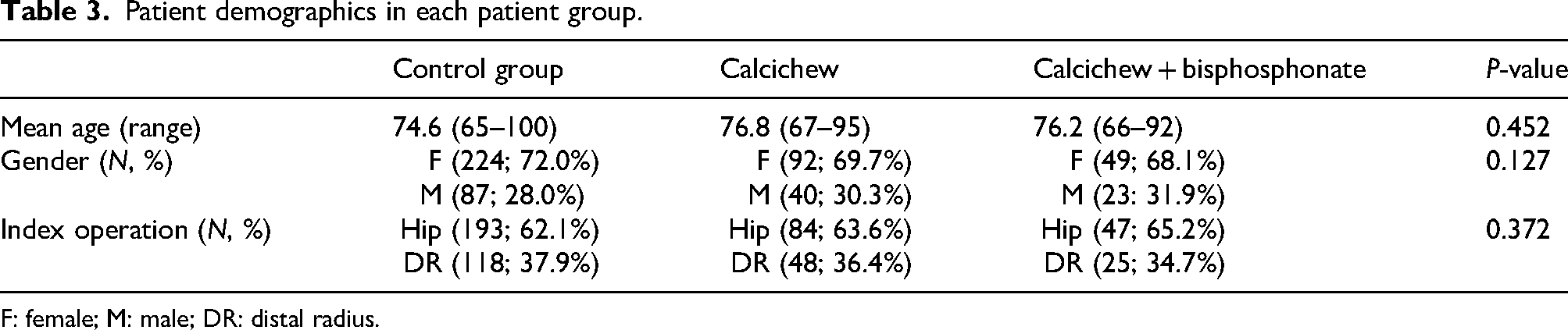
F: female; M: male; DR: distal radius.
Outcome
Osteoporosis investigation
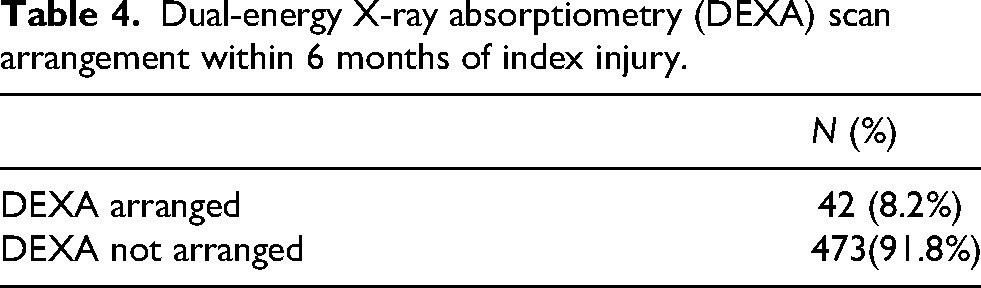
The DEXA scan was arranged in only 8.2% (n = 42) of the patients (Table 4).
Dual-energy X-ray absorptiometry (DEXA) scan arrangement within 6 months of index injury.
Readmission rate of repeated fragility fracture
Approximately 6.1% of the patients were readmitted due to repeated fragility fracture in the control group and calcichew group. Only the patients taking both calcichew and bisphosphonates are statistically significantly associated with a lower readmission rate of repeated fragility fracture in comparison with the other two groups (n = 0; vs. control group: P-value = 0.035; vs. calcichew group: P-value = 0.041) (Table 5).
Readmission rate of repeated fragility fracture in each patient group.

Data in bold are statistically significant.
Symptomatic osteoporotic vertebral collapse
There are 2.9% and 3.0% of the patients in the control group and calcichew group, respectively, presenting with new symptomatic osteoporotic vertebral collapse.
On the other hand, 8.3% of the patients taking both calcichew and bisphosphonates show new symptomatic osteoporotic vertebral collapse. Higher prevalence of new symptomatic osteoporotic vertebral collapse is observed in the group with both calcichew and bisphosphonate in comparison with the control group and the calcichew group, respectively (P-value = 0.026 and 0.033; Table 6).
Prevalence of new symptomatic osteoporotic vertebral collapse.
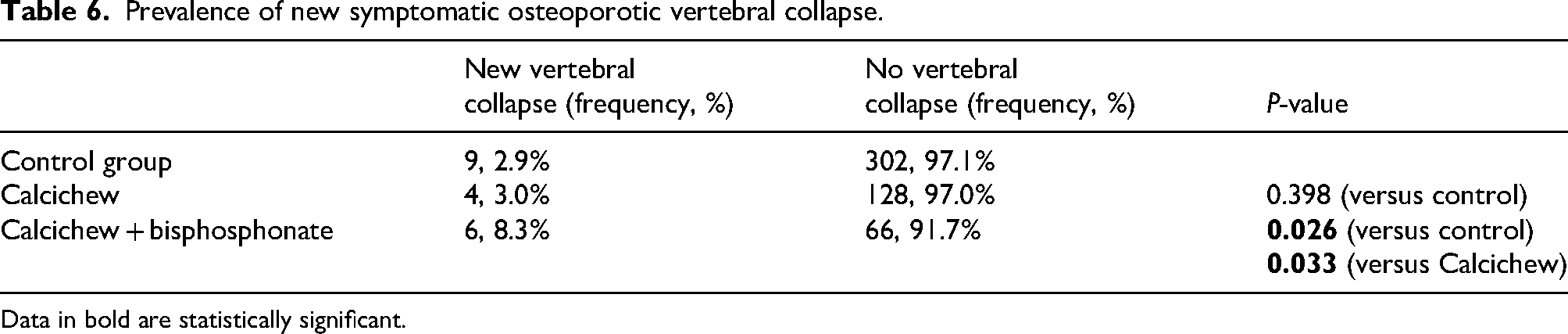
Data in bold are statistically significant.
Discussion
This retrospective study shows that a low proportion of patients underwent the DEXA scan within 6 months after index fragility fracture. Only 8.2% of patients underwent an osteoporosis screening test. This is comparable to the study conducted in the United States, with 11.4% of patients taking the DEXA scan following primary fragility fracture. 11
This could reflect poor awareness of orthopaedic surgeons in starting osteoporosis screening tests. The study conducted in 2019 revealed that orthopaedic surgeons believe that osteoporosis investigation and management are mainly responsible of primary healthcare practitioners. 12 They mainly focus on the surgical management of fragility fracture without adequate osteoporosis follow-up. Another reason is that there are limited DEXA scanning facilities in the public healthcare system in Hong Kong. 13 The average waiting time for an osteoporosis screening exam ranges from 1 to 6 years, depending on location.
Approximately 5.2% of patients (27 out of 515 patients) were readmitted due to repeated fragility fracture within 2 years following index fragility fracture. No readmission was noted in the group of calcichew and bisphosphonate. All patients received alendronate because this is the first-line anti-osteoporosis medication following the first episode of fragility fracture, according to the guideline in Hospital Authority. This group of patients was strongly associated with a lower readmission rate of fragility fracture in comparison to the other two patient groups, respectively (P-value = 0.035 and 0.041). On the other hand, there was no significant association between the patients receiving calcichew only and a lower readmission rate of repeated fragility fracture (P-value = 0.421). This result signified that optimal anti-osteoporosis treatment should be initiated as early as possible following primary fragility fracture so as to minimise recurrent fragility fracture. On the other hand, the result showed that calcichew only could not provide any protective effect to avoid recurrent fragility fracture.
Multiple clinical studies have justified the efficacy and safety of antiresorptive therapies.14,15 A meta-analysis of eight studies revealed that antiresorptive therapy of osteoporosis is significantly associated with a 11% reduction in mortality rate (risk ratio (RR) 0.89, 95% CI 0.80 to 0.99, P = 0.036). Furthermore, this is a cost-effective method in managing fracture prevention. The literature review predicted that a combination of alendronate with calcium and vitamin D supplementation could save Hong Kong healthcare system HK$425 million in 10 years, in addition to a reduction in costs of outpatient follow-up and institutional care. This estimation is based on the fact that antiresorptive therapy costs approximately HK$2500 while the direct cost of each hip fracture is estimated to be HK$81,120 in 2017. 16
Fracture liaison services (FLS) have been carried out in numerous countries to avoid undertreatment of secondary prevention of fragility fracture. 13 FLS model has been shown to be cost-effective in addressing the osteoporosis treatment gap. FLS aims to recognise patients with primary fragility fracture and give long-term education, monitoring and treatment in a multidisciplinary approach, involving orthopaedic surgeons, geriatricians, fracture liaison coordinators and allied health professionals. The patients with new fragility fracture are recruited and referred to an osteoporosis screening exam, in addition to investigating secondary causes of osteoporosis. All patients diagnosed with osteoporosis are prescribed anti-osteoporosis medication, and their drug compliance is regularly monitored during follow-up. Lifestyle risk factors and fall prevention are also assessed accordingly. A systematic review of 13 studies showed the risk of secondary fragility fracture was significantly lower in the FLS intervention at ≥2 years (RR 0.68, 95% CI 0.55 to 0.83). Patients benefit from FLS with standardised screening and management of fragility fracture secondary prevention, avoiding heavily relying on orthopaedic surgeons to recognise unmanaged osteoporosis. 17
On the other hand, there is a significant association between the patient group of both calcichew and bisphosphonates and a higher prevalence of new symptomatic osteoporotic vertebral collapse in comparison with the control group and the calcichew group, respectively (P-value = 0.026 and 0.033). This can be explained by the retrospective cohort study design. Some patients with symptomatic vertebral collapse might be missed because they could be admitted to Department of Accident and Emergency or private healthcare sector, resulting in incomplete data collection and selection bias. The total number of patients suffering from the new onset of osteoporotic vertebral collapse without any anti-osteoporotic therapy may be underestimated.
Also, there was no standardised protocol for addressing secondary prevention of fragility fracture before conducting this study. Multiple confounding factors are involved. The patients following primary fragility fracture were not closely monitored for their compliance with anti-osteoporosis management. They could also undergo different types of rehabilitation given by allied health professionals. Quality of care could vary among these patients, including the type of destination they were discharged to and the extent of social and financial support from their family. Further analysis can be carried out to further divide each patient group into either distal radius or hip fracture. Different types of fragility fracture in each patient group can be analysed to evaluate any significant association with repeated admission due to recurrent fragility fracture.
Conclusion
In conclusion, it was noted that osteoporosis diagnosis and intervention rates were suboptimal among the patients after their first fragility fracture. Our retrospective cohort study has shown both calcichew and bisphosphonate were statistically significantly associated with a lower readmission rate of repeated fragility fracture, signifying the importance of starting anti-osteoporosis medication after the first fragility fracture. Orthopaedic surgeons should focus not only on the acute management of fragility fracture, but also on secondary prevention of fragility fracture.
This was the first local study to stress the impact of starting osteoporotic therapy after fragility fracture on reducing the readmission rate of recurrent fragility fracture, and subsequently alleviating the financial burden on the public healthcare system. Standardised anti-osteoporosis management protocol should be implemented. This can not only facilitate orthopaedic surgeons to manage secondary prevention of fragility fracture, but also minimise the morbidity and mortality of patients due to repeated fragility fracture.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.