
Abstract
Keywords
Introduction
Patella fractures, comprising about 1% of skeletal injuries, typically arise from direct knee trauma or excessive eccentric contraction of the knee extensor mechanism.1,2 These fractures impair knee function and increase risk of early post-traumatic osteoarthritis. Operative management is often required to restore joint congruency and extensor function, which facilitates fracture healing and early mobilisation. According to the AO Foundation, type 34-C3 patella fractures are characterised by intra-articular and multifragmentary patterns. These fractures are among the most common yet challenging to fix. 3 This fracture pattern, marked by severe comminution with multiple small bony fragments, significantly complicates achieving and maintaining anatomical reduction with adequate fixation.
Tension band wiring has been the standard fixation method for patella fractures. However, recent biomechanical studies revealed its inadequate conversion of tension force to compression force in tension band constructs in a few indications.4–6 This prompted the AO Foundation to update its guidelines and adopt the term ‘cerclage compression wiring’ (CCW) in December 2023. 7 Despite its established use, this fixation method has been reported in multiple clinical studies with significant implant-related complications, high reoperation rates, and inconsistent functional outcomes.8–10 In contrast, locking plate (LP) fixation has emerged as a promising alternative. Its superior biomechanical properties offer enhanced stability and improved clinical outcomes in a series of clinical studies.11–15
Given the limited literature directly comparing LP and CCW in terms of clinical and functional outcomes, this study was conducted to compare these two fixation methods and provide evidence to guide optimal treatment strategies for these complex fractures.
Methods
This retrospective cohort study was conducted at Caritas Medical Centre, a district hospital in Hong Kong. Inclusion criteria were defined as: adult patients aged 18 or older who underwent primary surgical fixation for isolated AO Foundation type 34-C3 patella fractures with either LP or CCW between 31st January 2023 and 31st January 2025 (Figures 1 and 2). Eligible patients were required to have at least 6 months follow-up and complete medical records to be recruited. Patients who refused surgery, received conservative treatment, or alternative surgical fixation methods (e.g. screws, sutures, or salvage techniques) were excluded. Having incomplete medical records, or being unable to follow the rehabilitation program were also excluded from this study.
Clinical data were retrieved from the hospital clinical management system and identified through manual screening of operative records. All patients admitted with isolated patella fractures during the study period were assessed for eligibility and grouped based on fixation method. The LP group was treated with the DePuy Synthes 2.7 mm Variable Angle Locking Patella Plating System, while the CCW group received fixation with wire loops in cerclage wiring and figure-of-eight configuration. Supplemental fixation with screws or sutures was applied at surgeon discretion in both groups. Prophylactic antibiotics were given according to local antibiotic guidelines. All patients followed a standardised postoperative rehabilitation protocol as full weight-bearing with a hinged knee brace and stepwise increase in knee flexion (30°, 60°, 90°) at 2-week intervals.
Primary outcomes were complication and re-operation rates. Complications included wound complications (persistent dehiscence or gapping at 6 weeks 16 ), nonunion (no radiographic evidence of fracture healing after 3 months 17 ) and malunion (fracture healed in nonanatomical alignment). Implant-related complications comprised impingement (prominent implants causing patient discomfort) and failure (implant breakage). Radiographs were reviewed by a senior surgeon for diagnosis of complications. Reoperation rates included surgeries for osteosynthesis revision or implant removal.
Secondary outcomes, including hospital length of stay, functional outcomes (Tegner Activity Scale scores pre-injury and 6 months postoperation, Lysholm functional score at 6 months postoperation), and range of motion were assessed through follow-up clinic and physiotherapy records at 6 months.
Demographics such as age, gender, diabetes history and American Society of Anesthesiologists (ASA) health status score were evaluated. Procedural data including time from admission to surgery, operative time, and use of supplemental fixation methods were reviewed. For analysis, means and standard deviations were used for parametric data. Medians and interquartile ranges were used for non-parametric data. Student's t-tests compared parametric data, Mann–Whitney U tests compared non-parametric data and Fisher's exact tests were used for binary categorical data. Statistical significance was set at p < 0.05.
This study was approved by the Hong Kong Hospital Authority (HA) Central Institutional Review Board (Central IRB). Informed consent was waived by the HA Central IRB because the study used retrospective data. All personal data were anonymised and handled according to HA patient data privacy policies.
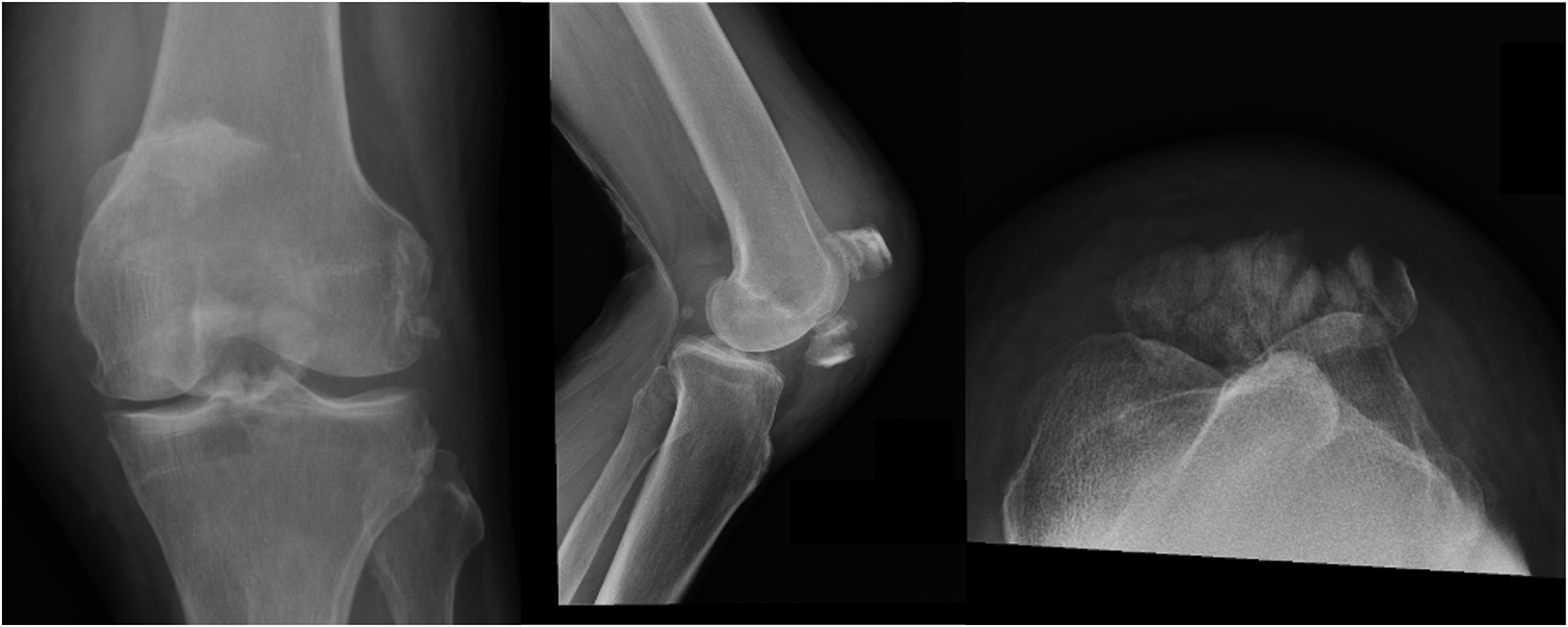
Radiograph of an AO foundation type 34-C3 patella fracture.
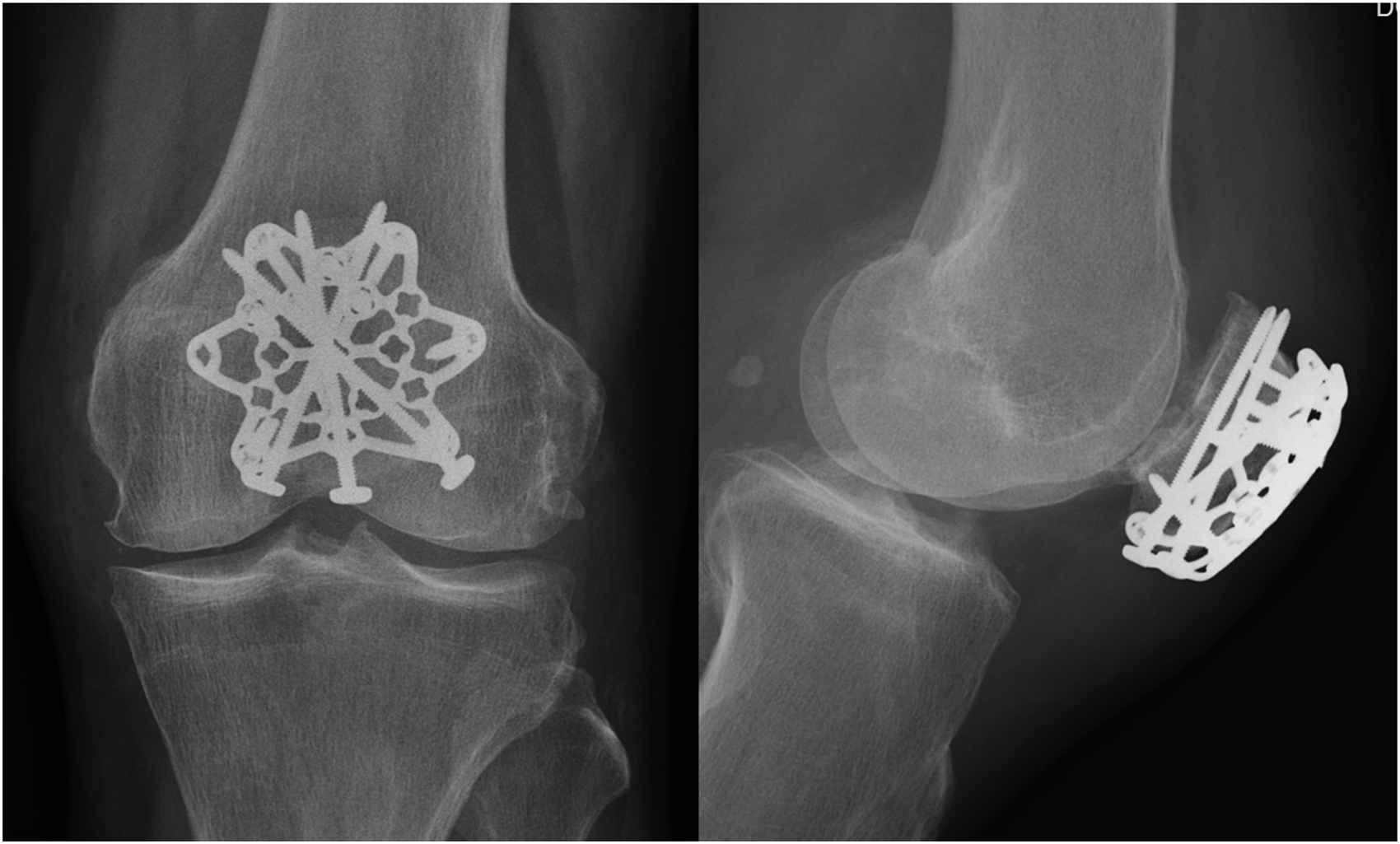
Patella fracture fixed with locking plate.
Results
Patient recruitment
Of the 95 patients admitted with patella fractures during the study period, 65 were excluded (27 received conservative management, 32 had fracture patterns other than AO Foundation type 34-C3, 3 underwent alternative fixation methods, and 3 had incomplete medical records). The remaining 30 patients were stratified into the LP group (n = 14) and CCW group (n = 16) (Figure 3).
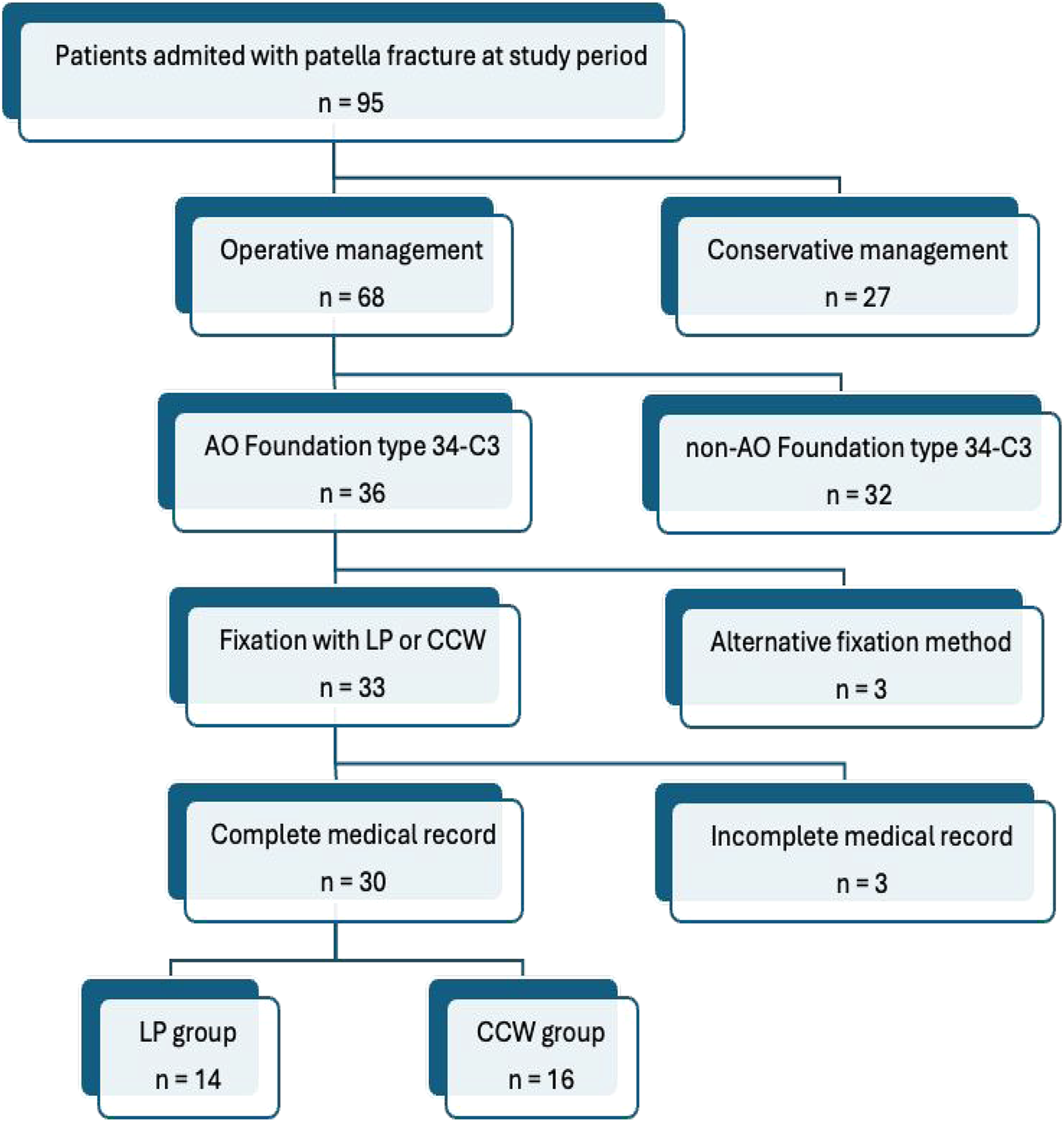
Flow chart for patient selection process.
Demographics
Among the 30 patients recruited, the overall male-to-female ratio (M:F) was 13:17. No statistically significant differences were observed between the CCW and LP groups in mean age (CCW: 68.75, SD 16.5 vs. LP: 68.4, SD 17.3; p = 0.956), gender distribution (M:F; CCW 9:7, 56.2%:43.8% vs. LP 4:10, 28.6%:71.4%; p = 0.151), ASA score (CCW: median 2, IQR 1–3 vs. LP: median 2, IQR 2–3; p = 0.614), or diabetes prevalence (CCW: 6, 37.5% vs. LP: 3, 21.4%; p = 0.439). These findings indicate comparable baseline characteristics between groups (Table 1).
Demographics.

Procedural outcomes
The LP group had a significantly longer mean operative time compared to the CCW group (CCW: 102.9 min, SD 30.7 vs. LP: 140.9 min, SD 30.7; p = 0.002). No significant differences were found in mean time to surgery (CCW: 3 days, SD 2.45 vs. LP: 4.14 days, SD 2.67; p = 0.235) or use of supplemental fixation methods (CCW: 8, 50% vs. LP: 5, 35.7%; p = 0.494), including screws (CCW: 6, 37.5% vs. LP: 3, 21.4%; p = 0.439) or Kirschner (K-) wires (CCW: 4, 25% vs. LP: 2, 14.3%; p = 0.657). (Table 2)
Procedural data.

Primary outcomes
The CCW group had a significantly higher complication rate than the LP group (CCW: 9, 56.3% vs. LP: 2, 14.3%; OR 7.71, 95% CI 1.28–46.37; p = 0.017). Implant-related issues were the most common complication (CCW: 8, 50% vs. LP: 2, 14.3%; OR 6, 95% CI 1–35.87; p = 0.057). The CCW group had one case each of malunion and nonunion (12.5%; OR 5, 95% CI 0.22–113.38; p = 0.485), with the malunion case also having implant issues, specifically K-wire displacement. No wound complications were reported in either group. Reoperation rates were comparable in both groups (CCW: 4, 25% vs. LP: 1, 7.1%; OR 4.33, 95% CI 0.42–44.45; p = 0.337). (Table 3)
Primary outcomes.

Secondary outcomes
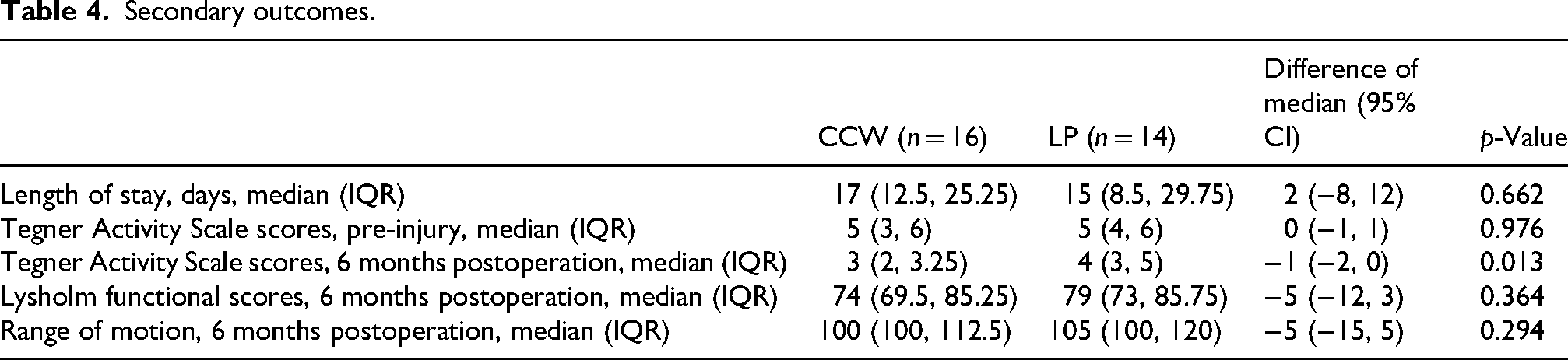
The median length of hospital stay was similar between groups (CCW: 17 days, IQR 12.5–25.25 vs. LP: 15 days, IQR 8.5–29.75; p = 0.662). Pre-injury Tegner Activity Scale scores were the same in both groups. (median 5; CCW: IQR 3–6 vs. LP: IQR 4–6; p = 0.976). Postoperative Tegner Activity Scale scores were significantly higher in the LP group (CCW: median 3, IQR 2–3.25 vs. LP: median 4, IQR 3–5; p = 0.013). No significant differences were observed in postoperative Lysholm functional scores (CCW: median 74, IQR 69.5–85.25 vs. LP: median 79, IQR 73–85.75; p = 0.364) or range of motion (CCW: median 100, IQR 100–112.5 vs. LP: median 105, IQR 100–120; p = 0.294) (Table 4).
Secondary outcomes.
Discussion
Comminuted patella fractures have historically been managed with CCW as the standard fixation method.8,18 However, with the advent of patella-specific LP, it has become popular due to its superior biomechanical properties.11–15 This retrospective cohort study compared the outcomes of fixation with LP and CCW for AO Foundation type 34-C3 patella fractures in a district Hong Kong hospital. The LP group had a significantly lower complication rate and a better postoperative Tegner Activity Scale scores. However, their operative time was longer compared to the CCW group. These findings showed LP may offer advantages in reducing complications and improving functional outcomes in complex comminuted patella fractures.
For primary outcomes, the CCW group exhibited a significantly higher complication rate (56.3% vs. 14.3%, p = 0.017), primarily due to implant complications such as impingement or failure. This could be explained by the biomechanical limitations of CCW. A series of clinical studies highlight the lack of conversion of tension forces into compression forces in tension band principle constructs with K-wires and cerclage wiring.4–6 These findings led the AO Foundation to review and update its fracture fixation guidance, and now adopt the term ‘cerclage compression wiring’. 7 Consequently, early pressure loading on fracture gap, as previously recommended, may lead to implant failure. 19
LP provides rigid and stable fracture fixation with multiple fixation points, whereas CCW relies mainly on tension forces to aid fracture healing. This high complication rates in CCW group aligns with biomechanical studies in the literature. Thelen et al. compared fixed-angle plate and tension wiring with screw fixation for patella fracture, evaluating fracture gap widening after 100 simulated cyclic loadings in cadaver knees. It showed significant displacement of 3.7 ± 2.7 mm with lag screws plus wiring and 7.1 ± 2.2 mm with tension band wiring alone, both considered clinical failures. Conversely, fixation with fixed-angle plates showed minimal gap widening of 0.7 ± 0.5 mm. 6 Similarly, Kim et al. demonstrated enhanced stability with LP constructs, showing significantly less deformation after cyclic testing compared to tension band wiring. The results also favoured LPs with higher failure resistance under tensile testing (1359 ± 21.53 N) than tension band wire fixation (780.1 ± 22.62 N). 20 These studies support that LPs have better biomechanical properties than CCW, leading to fewer fracture or implant complications, especially under strain testing. This is consistent with the lower complication rate observed in the LP group in our study.
Absence of wound complications in both groups highlights the efficacy of perioperative infection control with sterile technique and prophylactic antibiotics, along with effective surgical wound closure. A single case of nonunion and malunion each occurred in the CCW group, though they were not statistically significant (p = 0.485). Larger studies are needed to further evaluate these findings.
Reoperation rate was higher in the CCW group (25% vs. 7.1%), primarily due to implant removal for impingement, with one case requiring additional revision osteosynthesis for non-union. However, the difference between groups was not statistically significant (p = 0.337). Despite a higher complication rate in the CCW group, the comparable reoperation rates may reflect patients’ preference on conservative management for complications, when functional outcomes remain satisfactory. Klassen and Trousdale reported that minimally symptomatic nonunion of patella fractures can be treated conservatively with satisfactory functional outcome. Their study showed the mean Knee Society knee score of 72/100, a function score of 78/100, and an average knee range of motion of 127°. 21 Although the high complication rates in our study were primarily due to implant impingement, the findings from Klassen and Trousdale provide useful insight into the potential efficacy of conservative management for such complications.
For secondary outcomes, pre-injury functional status, assessed with Tegner Activity Scale scores, showed no significant difference between groups (median: LP = CCW = 5, p = 0.976). Postoperatively, the LP group demonstrated significantly higher Tegner Activity Scale scores (median: 4 vs. 3, p = 0.013) at 6 months, suggesting LP fixation is superior in restoring postoperative functional status to pre-injury activity level. This aligns with Ellwein et al., who reported significant functional improvement in displaced patella fractures fixed with LPs. The Tegner Activity Scale scores increased from 2.6 at 6 weeks to 3.6 at 6 months, ultimately reaching 4.1 as baseline pre-injury level at 24 months postoperatively. 22 Although length of stay, postoperative Lysholm functional scores, and range of motion showed no significant differences, the LP group displayed a trend toward better post-operative knee function and activity levels. This is consistent with recent studies on functional outcome favouring LP over CCW in patella fracture fixation.23,24
Operative time was noted significantly longer in the LP group (140.9 vs. 102.9 min, p = 0.002), likely due to the technical complexity and learning curve associated with LP fixation as a relatively new fixation technique. However, the median operative times of the LP group decreased from 151 mins to 121 mins between the first and second halves of the study, suggesting marked improvement with experience that is expected to continue. Although the initial operative time was longer, the lower complication rate and better functional outcomes seen in the LP group outweigh this drawback. To our knowledge, this is the first study to evaluate operative time in patella fracture fixation comparing LP and CCW.
Baseline demographics (age, gender, ASA status, diabetes) and procedural factors (time to operation, supplemental fixation) showed no significant differences, suggesting that outcomes are primarily driven by the fixation method rather than confounding patient factors.
This study has several limitations. The small sample size (n = 30) reduces statistical power, particularly for rare outcomes like nonunion or malunion, leading to wide confidence intervals. The retrospective design introduces potential selection bias, as fixation method choice was surgeon-dependent, though comparable baseline demographics alleviate this concern. The single-centre setting may limit generalisability to other populations. Finally, a minimum follow-up of 6 months may be insufficient to capture long-term complications or functional recovery.
Conclusion
This retrospective cohort study was conducted at a district hospital in Hong Kong. It provides consistent evidence that LP fixation is superior to CCW for AO Foundation type 34-C3 comminuted patella fractures, particularly in Asian populations. The LP group exhibited significantly lower complication rates and superior postoperative functional outcomes. Despite the limitations of a small sample size and single-centre design, these findings support adopting LP fixation for complex patella fractures. Larger, multi-centre prospective studies are needed to validate these results and provide guidance on future fracture management strategies.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.