
Abstract
Introduction
Smokers are known to have inferior outcomes after anterior cruciate ligament reconstruction (ACLR) than non-smokers. Currently, there is no published data on the prevalence of smoking among athletes who receive ACLR in Hong Kong.
Methods
A retrospective study was conducted in patients who received ACLR between 2007 and 2021 at a regional hospital in Hong Kong. The prevalence of smoking in ACLR patients was compared with the published data of the general population in Hong Kong.
Results
The prevalence of current daily cigarette smoking in patients who received ACLR between 2007 and 2021 was 16.4%, compared to 11.8%, 10.7%, 10.1%, and 9.5% in 2007, 2012, 2017, and 2021, respectively, for the general population. The daily smoking prevalence for male ACLR patients aged 20–29 years was 21.1%. For male adolescents younger than 20 years old who received ACLR, the prevalence was 5.7%, compared to 1.6% in the general population. Despite a steady decline in the smoking rate in the general population, a progressive drop in the prevalence of daily smoking in patients who received ACLR was only observed in men aged 30–39 years, not in the other age and sex groups.
Conclusion
The prevalence of current daily cigarette smoking in patients aged under 30 years old who received ACLR in Hong Kong is alarmingly high. There is a pressing need for the government to implement more focused anti-smoking campaigns and cessation support programmes tailored specifically for these young athletes, as there is a common misconception that they do not smoke.
Keywords
Introduction
Smoking is a significant risk factor affecting health. 1 Although smoking is widely recognised as a health hazard, the reported prevalence of smoking in athletes who underwent anterior cruciate ligament reconstruction (ACLR) varied from 13.5% to 37%, with rates ranging from 18.7% to 39.7% in men and 8.7% to 23.8% in women.2–4 These figures are alarming, considering that smoking is particularly discouraged among young athletes.
While the global age-standardised prevalence of current tobacco smoking is 32.7% among men and 6.6% among women, 1 the corresponding figures in the general population of Hong Kong (HK) are lower, at 16.7% for men and 3% for women. 5 In addition, the prevalence of smoking in HK has steadily dropped over the past 20 years. Currently, there is no published data on the prevalence of smoking among HK athletes who receive ACLR. It is not known whether there is any difference in the prevalence of smoking in athletes who receive ACLR between HK and other parts of the world, given that the prevalence of smoking in the general population in HK is low compared to the global average.1,5 It is also unknown whether there has been a progressive drop in the prevalence of smoking in HK patients who received ACLR over the past 15 years, as seen in the general population in HK.
The purposes of this research were (1) to report the prevalence of smoking in patients who received ACLR at a regional hospital in HK, (2) to study the trend of smoking in this subgroup between 2007 and 2021, and (3) to compare the prevalence and trends with those of the general population in HK.
Methods
The current study received approval from the local ethics committee at the author's institute (Document number: UW 24-412). The ethics committee waived the need for obtaining informed consent from the patients.
A retrospective study was conducted. Patients were included in the current study if they (i) underwent primary ACLR at the author's institute between July 2007 and December 2021, and (ii) were skeletally mature. Patients were excluded if the smoking status was not known.
Collection of demographic data
Patients were assessed in a pre-operative assessment clinic one week before the scheduled surgery. Demographic data, including smoking status, and medical information such as the Tegner activity scale (TAS) and body mass index, were obtained. The information was prospectively documented using a standard research documentation form. Patients were considered to have participated in pivoting sports before the injury if the pre-morbid TAS was 6 or above.
Definition of smoking
Smoking was defined as the use of conventional cigarettes and did not include the consumption of e-cigarettes or heated tobacco products. The data were captured at the time of ACLR. Ever-smokers were defined as patients who had smoked before the time of ACLR. Ever-smokers included daily smokers, non-daily smokers, and ex-smokers. The definition of cigarette smoking in this study aligns closely with that of the HK census report. 5
Prevalence of smoking in the general population
The prevalence of smoking in HK was obtained from the reports published by the Census and Statistics Department. Data were retrieved from the censuses conducted in 2007, 2012, 2017, and 2021.5–8
Statistics
To study the trend of smoking prevalence among patients who received ACLR between 2007 and 2021, data were analysed in three 5-year intervals: 2007–2011, 2012–2016, and 2017–2021. The selected time intervals facilitated comparison with the census data, which were collected in 2007, 2011, 2017, and 2021. A narrative description and comparison of smoking prevalence between the patients who received ACLR and the general population in HK were performed. Statistical analysis was carried out using SPSS version 28 only for patients who received ACLR, not for the census data. Descriptive statistics were reported. Independent t-tests and analysis of variance were used to compare continuous data, while chi-square tests were used to compare categorical data. Statistical significance was assumed if p was <0.05.
Results
Between July 2007 and December 2021, 765 primary ACLRs were performed at the author's institute. Among these, 59 patients with unknown smoking status were excluded. A total of 706 primary ACLRs met all inclusion and exclusion criteria, including 583 men and 123 women. The average age of the included patients was 27.3 ± 8.2 years (range = 14 to 58 years). Among the included ACLRs, 644 (91.2%) were performed in patients aged <40 years old.
Prevalence of smoking in patients who received ACLR
There were 166 ever-smokers, including 116 current daily smokers, 27 current non-daily smokers, and 23 ex-smokers. The prevalence of ever-smoking and current daily smoking was 23.5% and 16.4%, respectively. In total, 107 out of 116 current daily smokers (92.2%) were found in patients aged younger than 40 years old.
The prevalence of ever-smoking in men and women who received ACLR was 27% and 7.3%, respectively. There were more ever-smokers among men than women (p < 0.001). The distribution of current daily smokers, current non-daily smokers, ex-smokers, and non-smokers between sexes is reported in Figure 1.
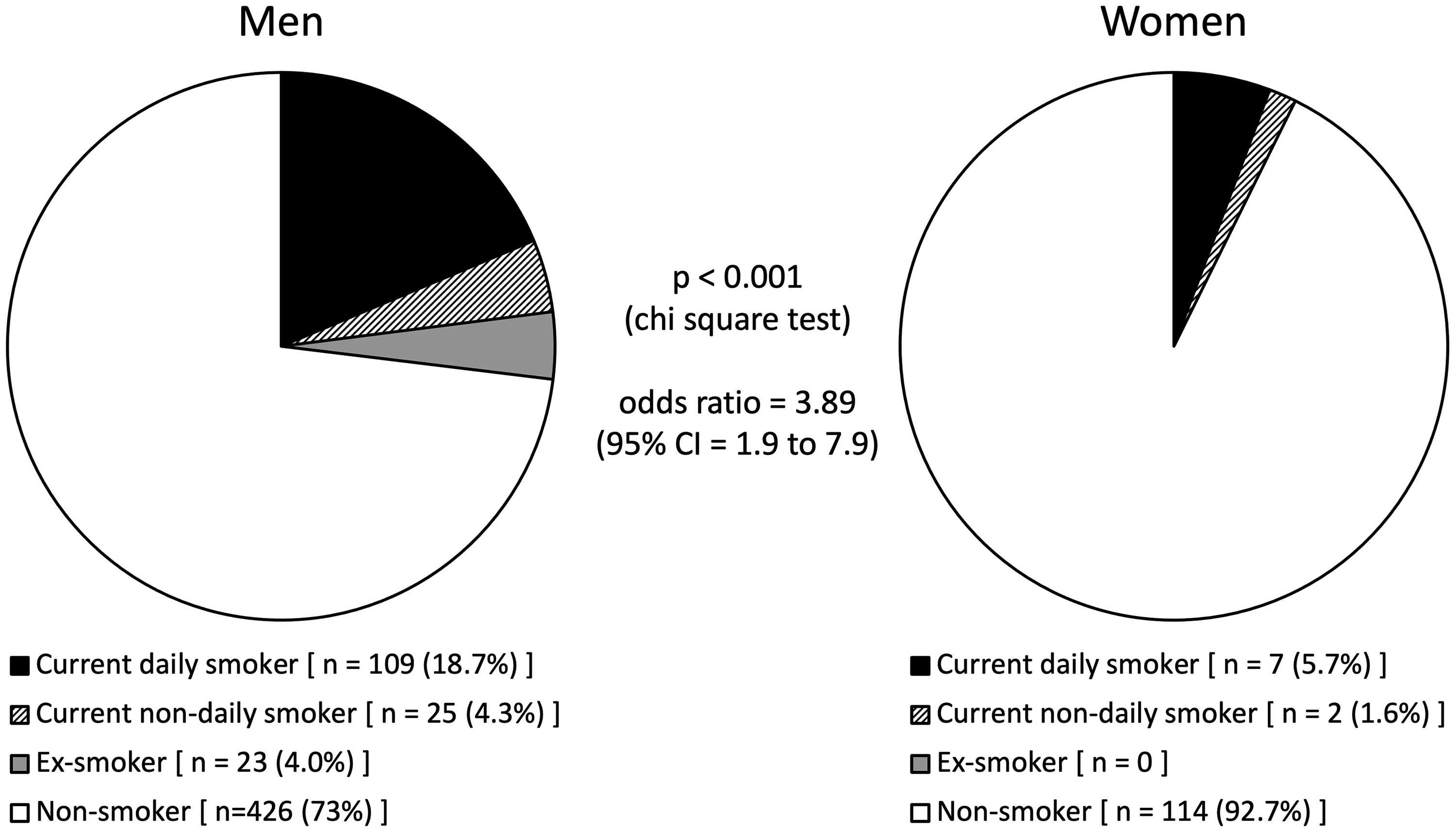
Distribution of smoking among men and women who received ACLR.
The patients who received ACLR were found to be younger than 60 years old. The distribution of ever-smokers (i.e. current daily smokers, current non-daily smokers, and ex-smokers) according to age and sex is shown in Figure 2. The prevalence of ever-smoking was highest in the age groups of 20–29 years old and 30–39 years old for both sexes, with rates of 29.5% and 31.6%, respectively, for men, and 9.1% and 13%, respectively, for women. The prevalence of ever-smoking in men was lowest in the age group of <20 years old, which was 10.3% (Figure 2).
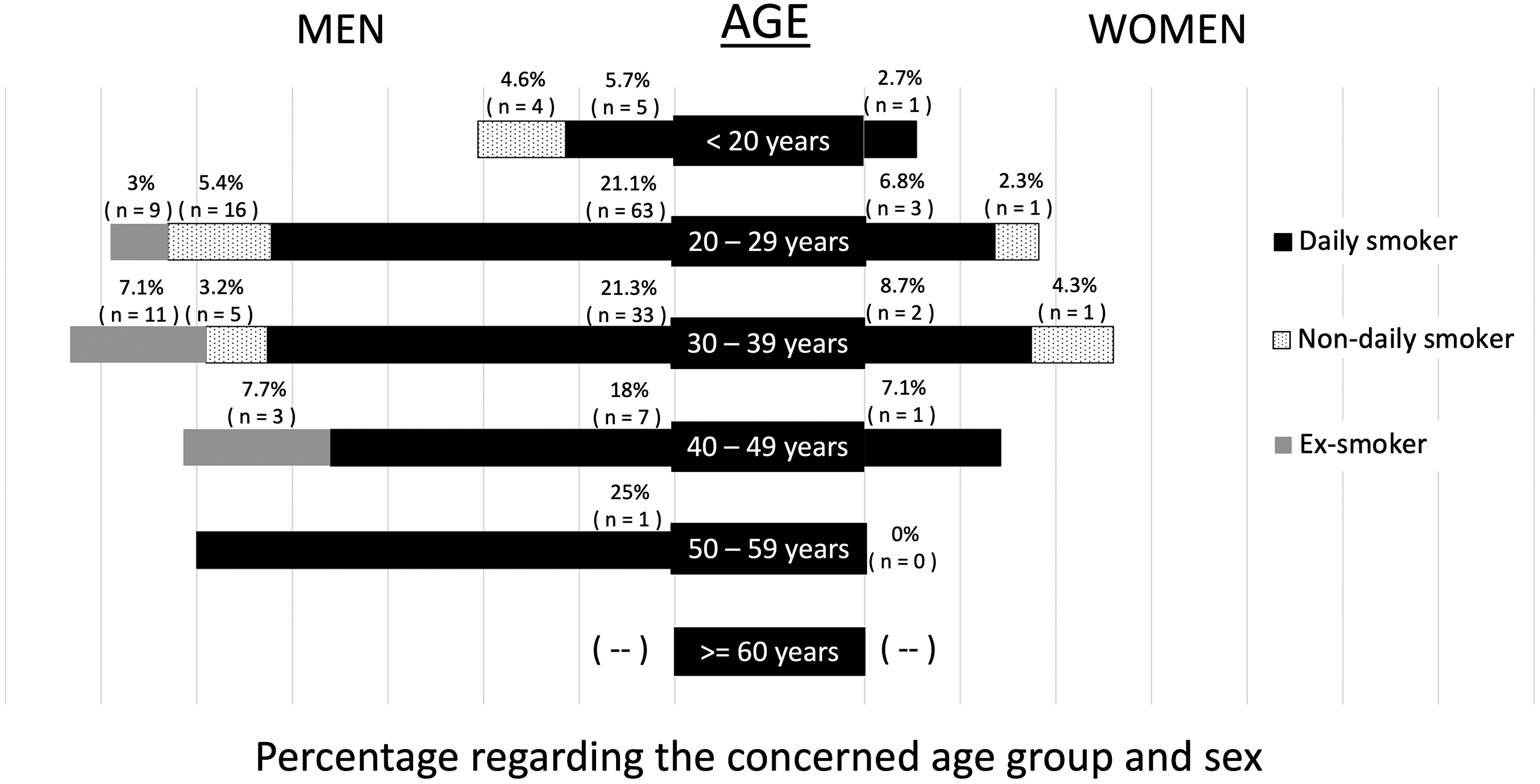
Prevalence of ever-smoking by age and sex in patients who received ACLR between 2007 and 2021.
The prevalence of ever-smoking among patients who received ACLR for the periods 2007–2011, 2011–2016, and 2017–2021 was 27%, 23% and 19%, respectively (p = 0.129).
The prevalence of current daily smoking by age, sex, and time of surgery in patients who received ACLR is presented in Figure 3. Regarding men aged <40 years old, the prevalence was higher in the time period 2007–2011, compared to the time periods 2012–2016 and 2017–2021.
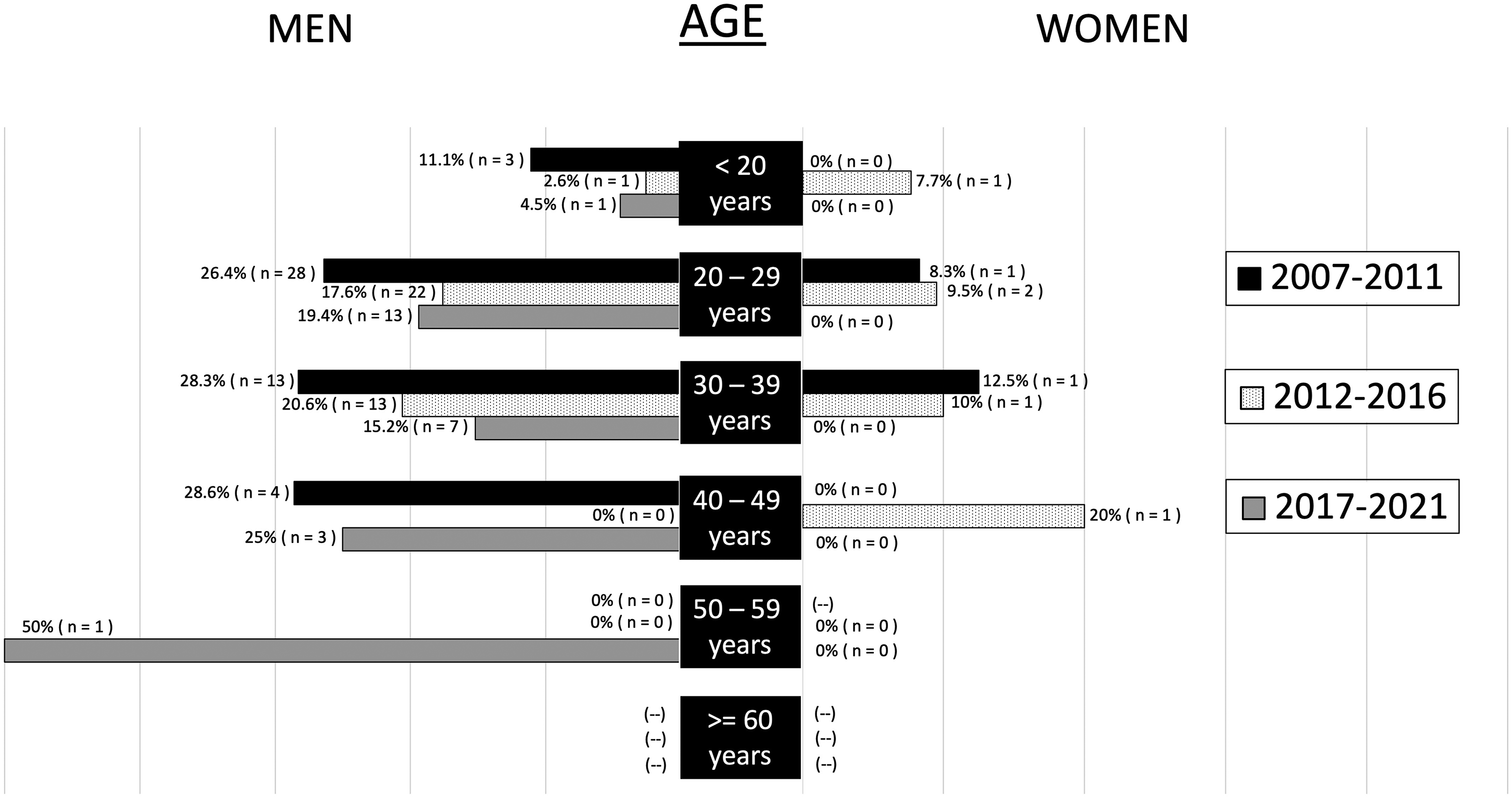
Current daily smoking by age, sex and time periods in patients who received ACLR between 2007 and 2021.
Comparison of smoking prevalence in patients who underwent ACLR and the general population in HK
The prevalence of cigarette smoking in the general population of HK5–8 and a subgroup of patients who received ACLR is presented in Figure 4.
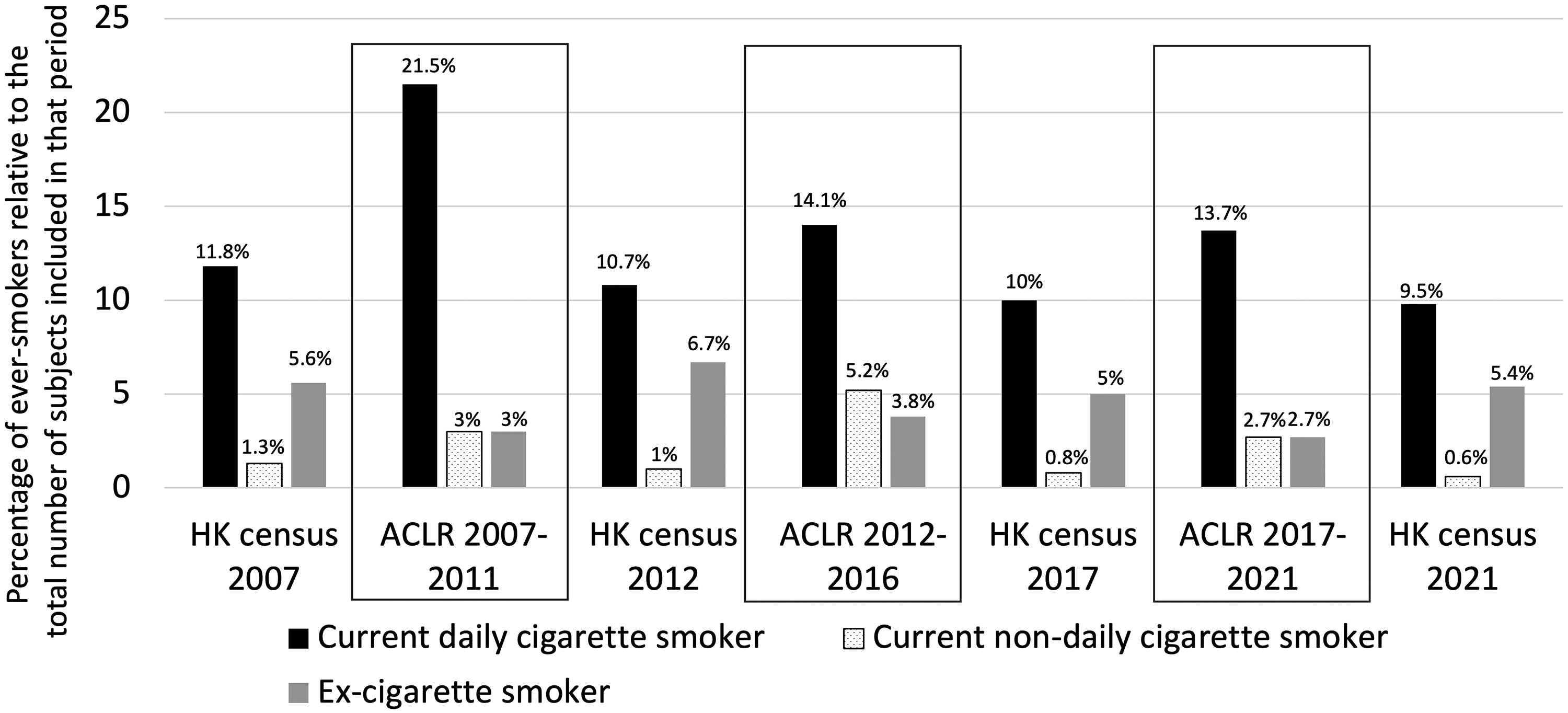
There was a steady decrease in the prevalence of current daily cigarette smoking in HK between 2007 and 2021, regardless of whether it was in the general population or the subgroup of patients who received ACLR. However, the prevalence of daily cigarette smokers in the subgroup of patients who received ACLR was around 1.3 to 2 times that of the general population in the comparable time periods (Figure 4). Regarding current non-daily cigarette smokers, this declining trend was only observed in the general population, not in the subgroup that received ACLR.
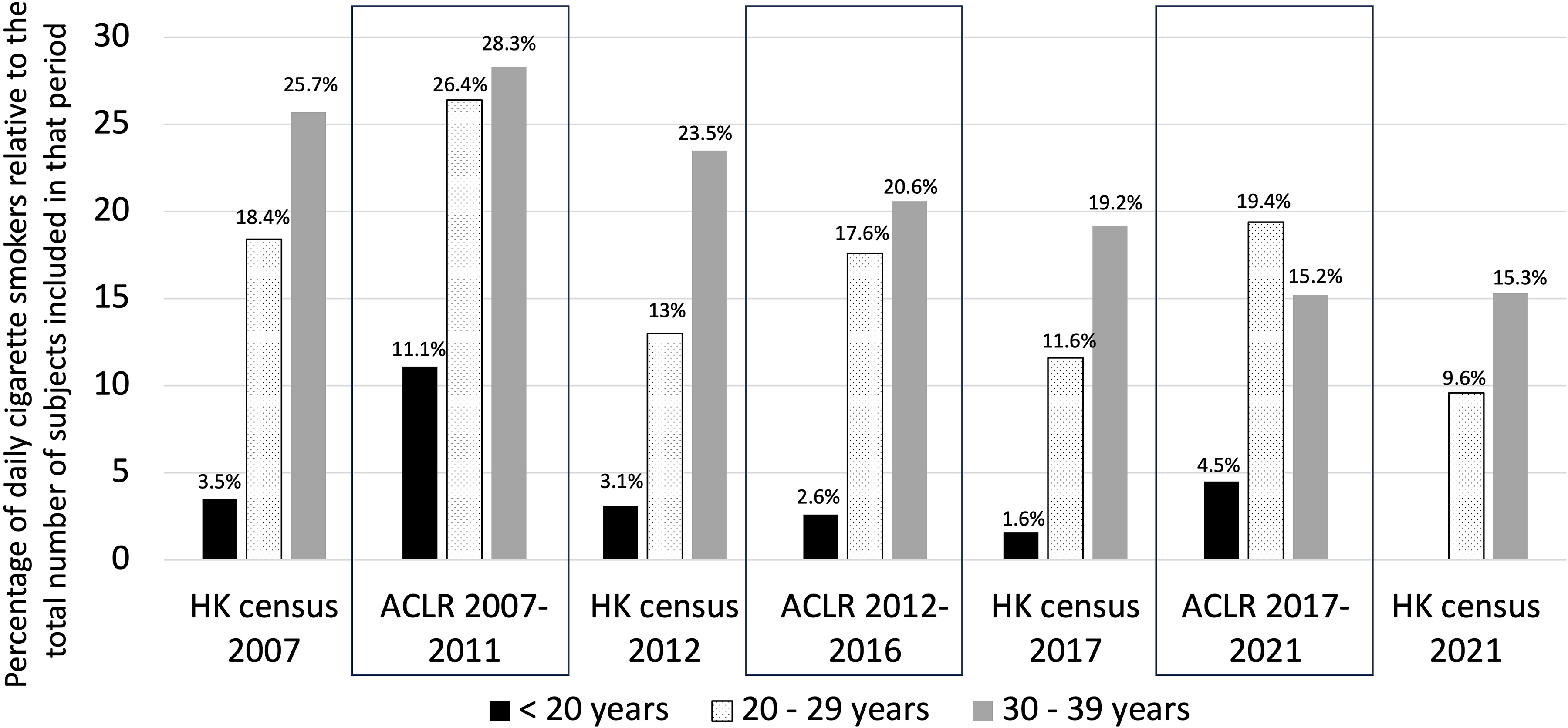
Over 75% of ACLRs were performed in the subgroup of men aged <40 years old. A more detailed comparison was performed between the general population and the patients who received ACLR in this subgroup (Figure 5). A progressive reduction in the prevalence of current daily smokers over the past 15 years could be observed in the general population, regardless of the age groups <20 years old, 20–29 years old, or 30–39 years old. However, regarding men who received ACLR, a similar trend could only be found in the age group 30–39 years old. For men who received ACLR in the age groups under 20 years old and 20–29 years old, a decline in the prevalence of daily smoking could only be found between the time periods 2007–2011 and 2012–2016. The prevalence of daily smoking in male ACLR patients aged <20 years old in 2007–2011 was 11.1%, while for 2012–2016 and 2017–2021 it was 2.6% and 4.5%, respectively. The corresponding figures for the age group 20–29 years were 26.4%, 17.6%, and 19.4%, respectively. When the corresponding age groups were compared at similar time points, the prevalence of current daily smoking for men aged 20–29 years was always higher in patients who received ACLR than in the general population, ranging from 1.4 times to 2 times higher (Figure 5). A reduction in the prevalence of smoking can be seen for men aged 30–39 years, regardless of whether they were patients who received ACLR or part of the general population, between 2007 and 2021. The reduction in the prevalence of daily smoking between consecutive 5-year intervals ranged from 5.4% (between 2012–2016 and 2017–2021) to 7.7% (between 2007–2011 and 2012–2016) in men who received ACLR, while for the general population, it ranged from 2.2% to 4.3%.
Discussion
The most important findings of the current study were: (1) the prevalence of current daily cigarette smoking in patients who received ACLR at a regional hospital in HK between 2007 and 2021 was 16.4%, while that for the general population was 11.8%, 10.7%, 10.1%, and 9.5% in 2007, 2012, 2017, and 2021, respectively.5–8 (2) The highest rates of current daily cigarette smoking between 2007 and 2021 in patients who received ACLR were in the age groups 20–29 years (21.1%) and 30–39 years (21.3%) in men (Figure 2). (3) The prevalence of daily cigarette smoking for male ACLR patients aged under 20 years between 2007 and 2021 was high (5.7%) (Figure 2), compared to the reported prevalence of the general population of the same sex and age group (3.5% in 2007, 3.1% in 2012, and 1.6% in 2017) (Figure 5). (4) Despite a steady decline in the smoking rate in the general population [census reports], a progressive drop in the prevalence of daily smoking in patients who received ACLR was only observed in men aged 30–39 years, not in the other age groups (Figure 5). However, the magnitude of the drop in this subgroup was approximately two times that of the drop in the general population of the same age group and sex (Figure 5).
The prevalence of current daily smoking for the whole cohort reported in this study was 16.4%. It was comparable to the reported figure of 13.5% in a large-scale study of 217,541 ACLRs conducted in the United States between 2010 and 2019. 4 The rate of ever-smoking (including current daily smoking, current non-daily smoking, and ex-smoking) was 27% in men and 7% in women in the current study (Figure 1). These rates were lower than those reported in a study conducted in South Korea (39.7% in men and 23.8% in women). 3 However, the discrepancy may be explained by the difference in the prevalence of smoking between the general population of South Korea and HK. According to the Global Burden of Disease Study 2019, the age-standardised prevalence of smoking in men and women was 42.5% and 5.2%, respectively, in South Korea. 1 The reported prevalence of current daily smoking in HK in the 2007 and 2021 censuses was 20.5% and 16.7%, respectively, for men, and 3.6% and 3%, respectively, for women.5,8
However, the findings of a higher prevalence of daily cigarette smoking in patients who received ACLR (16.4%) compared to the general population of HK (11.8% in the 2007 census, 10.7% in the 2011 census, 10.1% in the 2017 census, and 9.5% in the 2021 census)5,8 are startling considering the well-known health risks associated with smoking, particularly in the context of young athletes who are often advised against it. The difference in the age and sex composition between the general population and the subgroup that received ACLR, in which men aged <40 years accounted for 77% of the whole cohort, may be a reason behind this. The reported prevalence of daily cigarette smoking in men aged under 40 years was 22.1%, 14.6%, 16.1%, and 13.3% in the 2007 census report, 2012 census report, 2017 census report, and 2021 census report, respectively.5–8 Compared to an 18.7% prevalence of daily smoking in men aged under 40 years who received ACLR between 2007 and 2021, the difference in age and sex composition is unlikely to be the only explanation behind this alarming figure. One possible explanation for this observation is that smoking is a risk factor for anterior cruciate ligament (ACL) rupture, and smokers are more prone to suffering from ACL injury. Smokers are known to have inferior outcomes after ACLR than non-smokers.9,10 However, there is not yet any concrete evidence demonstrating a direct association between smoking and primary ACL injury. In a subgroup of ACLR patients who smoked, tobacco use is associated with a two-fold increase in the risk of ACL injury in the contralateral knee. 11 Additionally, smokers are known to suffer from delayed maturation of the ACLR graft 2 and have a higher chance of revision of the ipsilateral ACLR. 11 In order to find out whether smoking is a risk factor for primary ACL injury, a territory-wide prospective epidemiology study examining the relationship between smoking and first-time ACL injury should be performed.
The prevalence of daily smoking in male ACLR patients under 20 years old and 20–29 years old reported in the current study was high (5.7% and 21.1%, respectively). Smoking is associated with a two-fold increase in the chance of revision surgery secondary to ACLR graft rupture. 11 As shown in the current study, a majority of patients who receive ACLR are in this age group. According to a national registry study including 18,425 ACLR patients, more than 75% of patients were <30 years old. 12 Young age is the most important factor predicting ACLR graft rupture. The reported short-term graft rupture rate ranged from 7% 13 to 14% 14 in patients younger than 25 years old. Young patients were also more ready to receive revision ACLR, likely related to the higher demand to return to pivoting sport. 15 The impact of a high prevalence of daily smoking in a group of young patients who receive ACLR is expected to result in a cascading increase in the incidence of ACLR graft rupture and revision surgery. The burden on the healthcare system is significant. Despite the anti-smoking campaign carried out by the government in the past 20 years, which has successfully led to a progressive decline in smoking in the general population, the author did not see a corresponding decrease in the prevalence of smoking in male patients younger than 30 years old who received ACLR at the author's institute between 2012 and 2021 (Figure 5). There is a need for the government to implement more focused anti-smoking campaigns and cessation support programmes tailored specifically for these young athletes, as there is a common misconception that they do not smoke.
In addition to being associated with a higher graft rupture rate after ACLR, 16 smoking has been linked to other poorer outcomes following ACLR. Research indicates that smokers have an increased likelihood of post-operative complications such as thromboembolic disease and infections.4,11 Additionally, smokers tend to suffer from more persistent knee pain, reduced knee function, and have a decreased probability of resuming sports activities at the level before injury.3,10 The higher smoking prevalence among young athletes leads to worse clinical outcomes and an increased likelihood of revision in patients who undergo ACLR in HK.
Despite the prevalence of smoking in patients aged 30–39 years being high (21.3%), it is encouraging to notice that there is a progressive decline in the daily smoking prevalence in this age group between 2007 and 2021 (Figure 5). This parallels the reduction of smoking prevalence in the general population, but to a much greater extent. The magnitude of the drop between consecutive 5-year time points in male patients aged 30–39 years who received ACLR was approximately two times that of the decline in the general population of the same age group and sex (Figure 5), indicating that targeted efforts within this demographic can yield significant results.
Despite current active smoking being associated with an increased risk of infection and retear in rotator cuff repair compared to non-smoking, it has been reported that there is no difference in retear and infection rates between patients who quit smoking more than six months prior to rotator cuff repair and non-smokers. 17 It is not known whether a similar relationship exists in ACLR. However, in the interest of the patients and to improve clinical outcomes, chronic smokers should be advised to quit smoking before undergoing ACLR. 18
Limitation
Firstly, the definition of smoking used in this study does not include the consumption of e-cigarettes and heated tobacco products, although these types of products are becoming more popular among the younger generation and are known to be associated with inferior results after orthopaedic surgery. 19 Additionally, although the definition of cigarette smoking adopted in this study closely aligns with that of the HK census, minor differences exist. For example, the youngest subjects included in the HK census were 15 years old, while for the current study, they were 14 years old. These differences may introduce bias in the results. Secondly, due to the very small number of women smokers in this series, the analysis did not include a detailed comparison of the smoking prevalence between women who received ACLR and that of the general population. Thirdly, the retrospective nature of the study made it impossible to investigate the possible causal relationship between smoking and first-time ACL injury. Fourth, patients with unknown smoking status were excluded from this study, which introduces bias. Finally, patients self-reported their smoking status at a pre-operative assessment clinic, one week prior to the scheduled ACLR. The data were documented prospectively using a standard research documentation form at the time of the pre-operative assessment clinic. However, no verification was conducted against other available written medical records (e.g. medical records from non-sports medicine consultations within the hospital authority or private practices). Since the smoking status was prospectively documented one week before the ACLR, recall bias is expected to be minimal. However, other biases related to self-reporting, such as social desirability bias, cannot be entirely ruled out.
Conclusion
The prevalence of current daily cigarette smoking in patients aged under 30 years old who received ACLR in HK is alarmingly high. There is a pressing need for the government to implement more focused anti-smoking campaigns and cessation support programmes tailored specifically for these young athletes, as there is a common misconception that they do not smoke.
Supplemental Material
sj-doc-1-otr-10.1177_22104917251373090 - Supplemental material for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study
Supplemental material, sj-doc-1-otr-10.1177_22104917251373090 for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study by WP Yau in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-pdf-2-otr-10.1177_22104917251373090 - Supplemental material for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study
Supplemental material, sj-pdf-2-otr-10.1177_22104917251373090 for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study by WP Yau in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-3-otr-10.1177_22104917251373090 - Supplemental material for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study
Supplemental material, sj-docx-3-otr-10.1177_22104917251373090 for The prevalence of smoking in patients who received anterior cruciate ligament reconstruction in Hong Kong – a retrospective cross-sectional study by WP Yau in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.