
Abstract
Reverse shoulder arthroplasty (RSA) has been a widely used surgical intervention for management of complex shoulder pathologies, including proximal humeral fractures, rotator cuff arthropathy and severe shoulder osteoarthritis. However, two critical independent factors may potentially influence postoperative outcomes: (1) the number of peripheral screws used for glenoid fixation and (2) greater tuberosity migration. This study analysed a cohort of 28 RSA patients to assess whether the number of peripheral screws affects loosening rates and whether postoperative greater tuberosity migration impairs abduction and forward flexion. Statistical analysis revealed no significant association between screw count and loosening (p = 0.62), but tuberosity migration was linked to significantly reduced abduction (p = 0.028). These findings suggest that surgical focus should prioritize the stability of tuberosity fixation, also excessive peripheral screw use may not be necessary.
Keywords
Introduction
Background
Reverse shoulder arthroplasty (RSA) is a widely used surgical procedure for complex proximal humeral fractures, irreparable rotator cuff tears and severe osteoarthritis. 1 Unlike anatomic total shoulder replacements, RSA provides a medialized centre of rotation, enhancing deltoid efficiency for arm elevation.
However, two persistent challenges influence the long-term outcomes of RSA: achieving stable glenoid fixation and maintaining proper tuberosity positioning in fracture cases.
Glenoid component stability remains paramount for implant longevity. While the central screw or central peg provides primary fixation, the role of peripheral screws in preventing micromotion remains a topic of debate. 2 Some surgeons advocate for maximizing screw quantity to enhance stability, while others suggest fewer screws may suffice and minimize bone damage. Moreover, in proximal humerus fracture cases, greater tuberosity healing significantly impacts functional outcomes through its effect on rotator cuff integrity. Tuberosity migration can disrupt rotator cuff function, leading to reduced active motion. 3
This study addresses these critical questions through analysis of a 28-patient cohort, evaluating both screw configuration effects on loosening and greater tuberosity migration consequences for active range of motion in shoulder abduction and forward flexion. Our study aims to provide evidence-based guidance for surgical decision-making in RSA procedures.
Study objectives
This study investigates:
Does the number of peripheral screws influence loosening rates? Does greater tuberosity migration impair abduction and forward flexion?
Methods
Data source
This research study was conducted in compliance with ethical guidelines and was reviewed and approved by the Hospital Authority Clinical Research Ethics Committee. The hospital database in Caritas Medical Centre, Hong Kong was reviewed and all patients with RSA performed from August 2018 to December 2024. For inclusion criteria, all patients undergoing RSA at our institution, with a minimum follow-up of 6 months and available latest follow-up radiographs were included. For exclusion criteria, patients who defaulted follow-up or had less than 6 months of postoperative follow-up were excluded from the analysis.
A retrospective review of 28 RSA patients was conducted. Data included:
Demographics
Age distribution
Mean age: 73.2 years (SD = 8.3; range = 54–86) Stratifications: < 65 years 10.3% (n = 3), 65–75 years (n = 11), > 75 years 51.7% (n = 15) Sex distribution
20 female patients (69.0%), 9 male patients (31.0%) Primary diagnosis
21 proximal humerus fractures, 5 cuff arthropathy, 2 shoulder osteoarthritis Comorbidities
Hypertension 82.8% (n = 24), Diabetes mellitus 55.2% (n = 16), Prior cerebrovascular accident 13.8% (n = 4) Variables: Number of glenoid peripheral screws, tuberosity migration status. Outcomes: Loosening, abduction active range of motion (AROM), forward flexion AROM.
Original and latest follow-up radiological assessment was reviewed for all RSA cases. Loosening was radiologically defined by either: (1) progressive radiolucency greater than 2 mm in width surrounding the glenoid component, or (2) measurable migration (>5° tilt or >2 mm displacement) from the initial postoperative position. These criteria were adapted from, 4 suggesting their significant association with impending implant failure warranting revision surgery.
For all fracture RSA cases, superior migration of the greater tuberosity was evaluated on shoulder anteroposterior radiographs, defined as greater than 5 mm proximal displacement from the postoperative position 5 with or without final bony union. Two blinded orthopaedic surgeons independently assessed all radiographs, with consensus reached through discussion for discrepant cases (Figures 1–3).
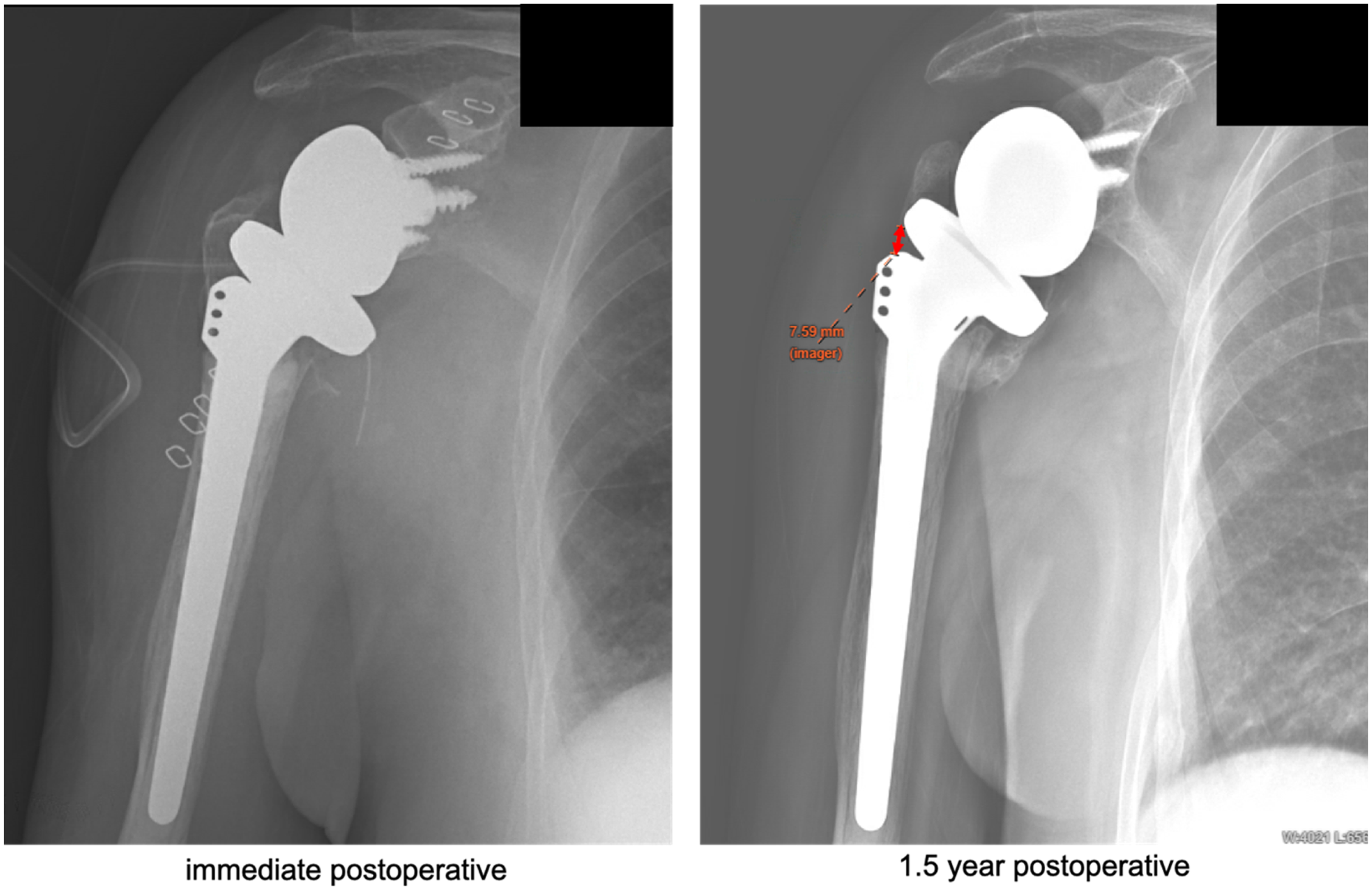
Measurement of greater tuberosity migration on anteroposterior shoulder radiograph.
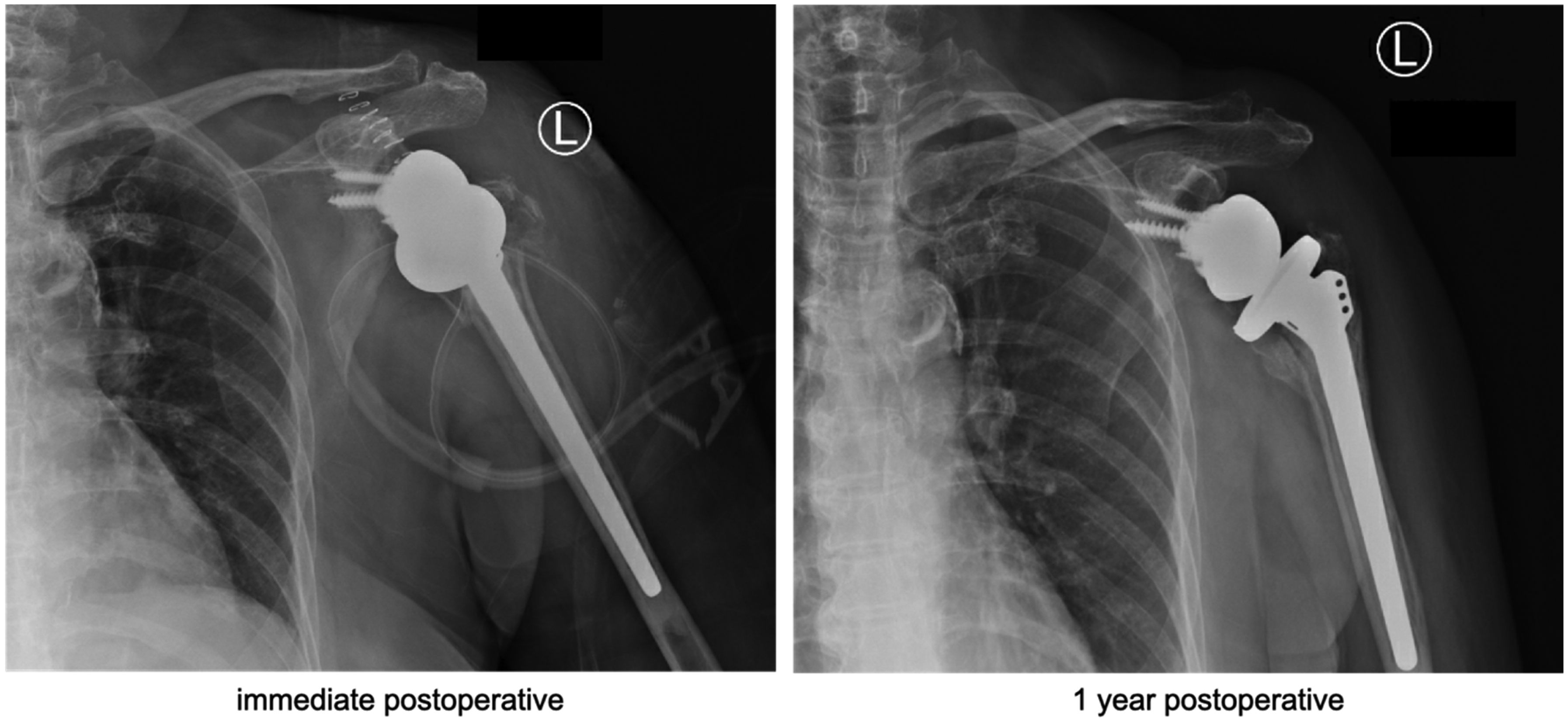
Illustration of RSA fracture case demonstrating healed greater tuberosity without migration. RSA: reverse shoulder arthroplasty.
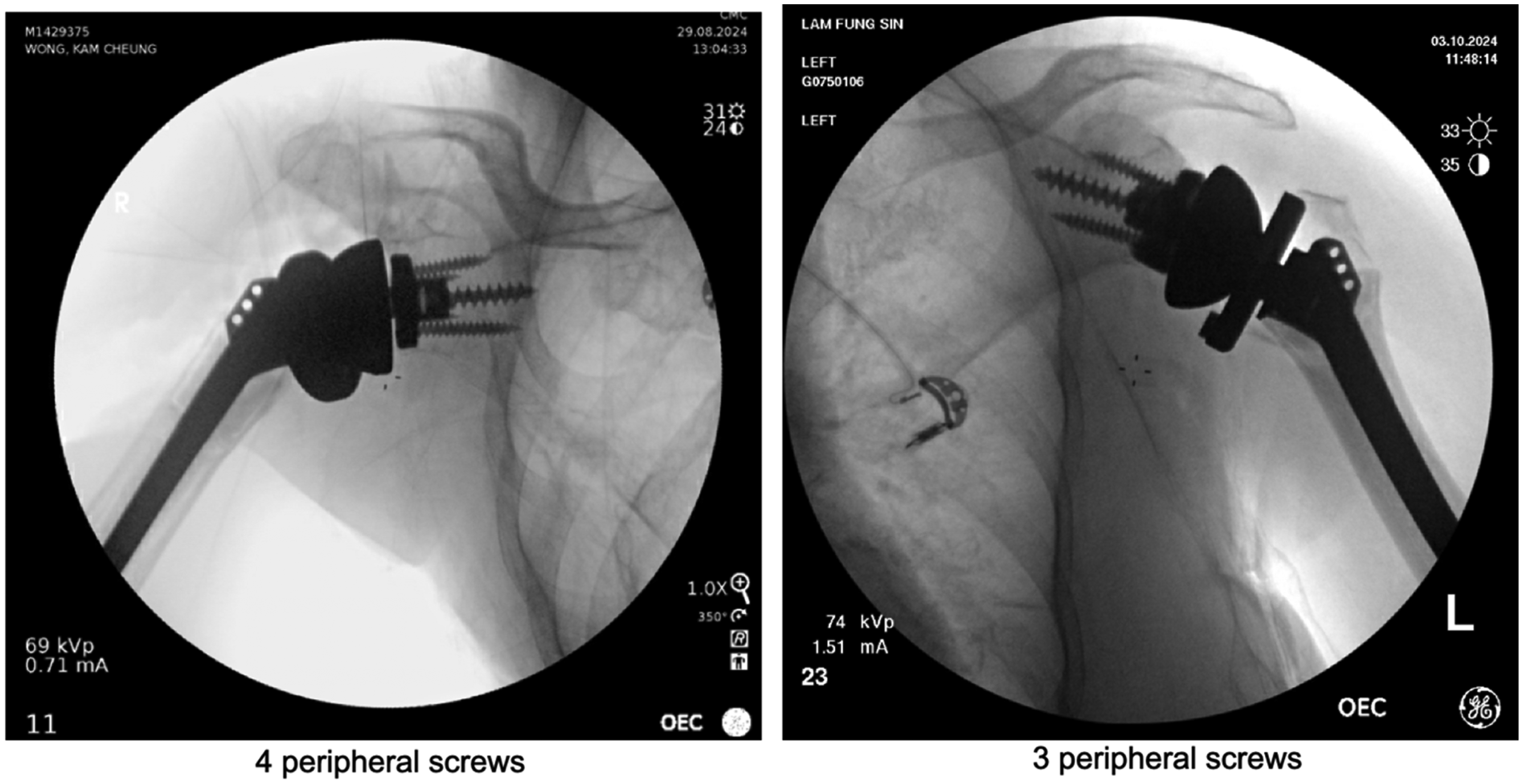
Glenoid fixation configurations comparing four peripheral screws (left) and three peripheral screws (right).
Statistical analysis
Mann–Whitney U test was used to investigate the effect of number of peripheral screws on effect of loosening among all 28 patients undergone RSA.
Independent t-test was used to investigate the effect of greater tuberosity migration on (1) shoulder abduction range and (2) shoulder forward flexion range among 23 RSA patients with fracture as surgical indication. Normal distribution was confirmed using Shapiro–Wilk Test.
Results
Peripheral screws and loosening
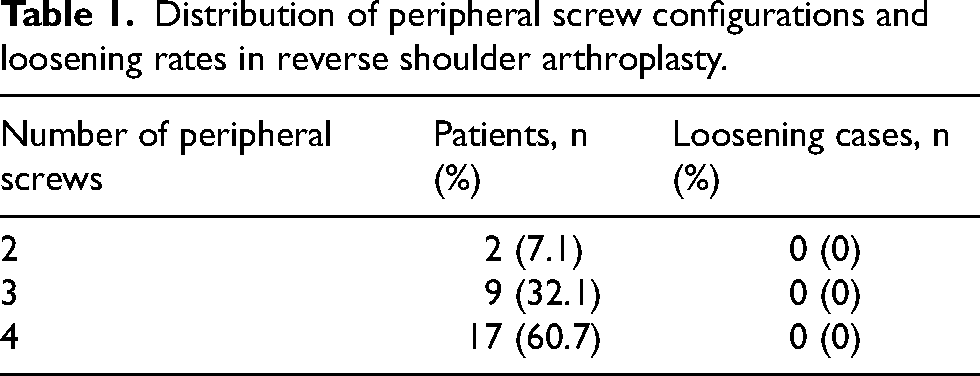
Our study compared the loosening rate among variable number of peripheral screws. Statistical findings showed no significant difference in loosening between screw groups (p = 0.62) (Table 1).
Distribution of peripheral screw configurations and loosening rates in reverse shoulder arthroplasty.
Greater tuberosity migration and active range of motion
Statistical findings showed shoulder abduction range was significantly worse with tuberosity migration (p = 0.028). There is a trend towards reduction in forward flexion range in tuberosity migration group, however, not statistically significant (p = 0.096) (Table 2).
Comparison of active range of motion between patients with and without greater tuberosity migration.
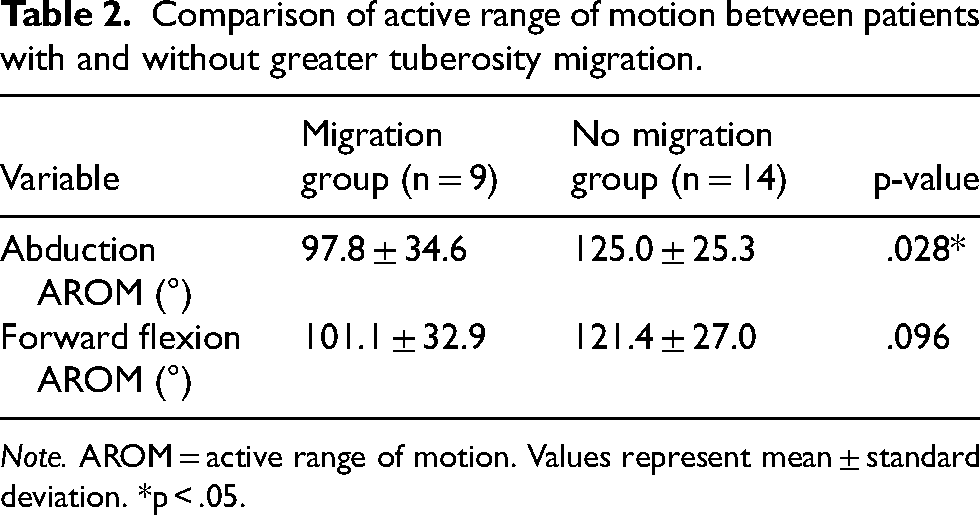
Note. AROM = active range of motion. Values represent mean ± standard deviation. *p < .05.
Discussion
Peripheral screws and loosening
The relationship between number of peripheral glenoid screw and component loosening plays a critical role in biomechanical consideration when performing RSA. Our findings demonstrate no statistically significant association between the number of peripheral screws (ranging from 2 to 4) and implant loosening rates (p = 0.62). Our results contrast with some earlier biomechanical studies that suggested additional screws improve stability. 6 Our observation aligns with emerging biomechanical evidence suggesting that the central screw or peg provides the primary stability in modern RSA designs, while peripheral screws may serve a secondary role in load distribution rather than being the dominant factor of preventing micromotion and loosening. 7 Another cadaveric study also showed no statistical difference in baseplate motion between 2-screw and 4-screw configuration. 8 The biomechanical rationale may relate to the differential load transfer mechanisms in RSA. In the reverse shoulder configuration, the centre of rotation is medialized, altering the force vectors acting on the glenoid component. 9 This modified biomechanical configuration reduced the dependence of stability on peripheral screw fixation, particularly when a robust central screw fixation is achieved.
Our cohort results showed peripheral screws pose no additional benefit against loosening. Indeed, several factors also contribute to stable fixation. First, bone quality plays a significant role in stable fixation. 2 Osteoporotic bone is common among the RSA patient population. The purchase of peripheral screws may be compromised. Second, the trajectory and positioning of screws may be more important than their quantity (Hopkins et al., 2014). Optimally placed screws could engage the strongest available bone stock and increase stability, rather than simply increasing screw number. 6 Third, the phenomenon of stress shielding should be considered. Excessive peripheral fixation might weaken surrounding bone and paradoxically lead to bone resorption and periprosthetic loosening. 10
The mean follow-up duration of 24.5 months in our study provides adequate time for early loosening to manifest. However, long-term follow-up e.g. 5 years would be valuable to assess midterm and late loosening patterns. 11
These findings have important practical implications for surgical strategy. The absence of a clear advantage for higher screw numbers suggests that surgeons can confidently use fewer screws when bone quality or anatomical constraints make additional screw placement challenging. This flexibility may be particularly valuable in revision scenarios or cases with glenoid bone loss. 12 Furthermore, reducing screw number allows shorter operative time, minimizes neurovascular injury risk and preserves bone stock for potential future revisions.
However, these conclusions must be balanced against the need for adequate initial stability and bone purchase. Our data should not be interpreted as suggesting that peripheral screws are unimportant, but rather that screw quantity may be less critical than their quality of placement and the overall construct stability. The optimal approach should aim to achieve secure initial central fixation, followed by adding peripheral screws judiciously based on intraoperative assessment of stability rather than adhering to a rigid numerical guidelines.
Future research directions may include larger multicentre comparative studies with standardized screw placement protocols and long-term follow-up to assess late loosening patterns. Our local patient population tends to have smaller glenoid sizes. Given the mean glenoid width size of 25.3 mm and median of 24.6 mm in our cohort, tailored screw placement recommendations may be beneficial to optimize surgical outcomes.
Tuberosity migration and functional outcomes
The impact of greater tuberosity migration on functional outcomes among RSA in patients suffering from proximal humeral fractures represents a critical clinical concern. Our findings showed statistically significant reduction in shoulder abduction range in tuberosity migration group (97.8° vs. 125.0°, p = 0.028). This observation aligns with the biomechanical principles of RSA, where proper tuberosity healing is essential for maintaining rotator cuff function. 3 The disruption of cuff tendon insertions due to tuberosity migration may lead to deficit of shoulder abduction. Despite the fact that deltoid serves as the primary elevator, rotator cuff synergise to optimize force coupling across the glenohumeral joint. Moreover, superior migration of greater tuberosity causes impingement over acromion during shoulder abduction and forward flexion, therefore hindering range of motion and causing pain. 13
A shorter mean follow-up in the tuberosity migration group was observed (18.4 vs. 27.8 months, p = 0.043). The data interpretation must take into consideration that shorter follow-up may potentially underestimate the long-term functional plateau. Yet, longitudinal studies suggested that RSA patients showed variable length of functional recovery of shoulder abduction and forward flexion. RSA patients achieved 72% to 91% functional improvement after 6 months. This implied our findings may represent near-final outcomes.
Surgical technique appears crucial in mitigating migration risk. Our cohort's migration rate was 32.1%, comparable with literature values of around 31.7% to 40% for fracture RSAs.14,15 It highlighted the technical challenge of achieving stable tuberosity fixation in osteoporotic bone. In our centre, both greater and lesser tuberosity fragments were reduced and securely fixated to the humeral stem component using 5-Ethibond sutures passed through strategically placed drill holes in the humeral cortex. Modern strategies suggested use of tensioning devices like cable cerclage to increase tuberosity fixation stability. 16 Another systemic review showed the use of uncemented pressfit stem is associated with higher greater tuberosity healing rate, yet no significant difference shown in functional outcome. 17
In conclusion, tuberosity migration significantly impairs abduction after RSA for proximal humerus fractures, leading to impingement and functional loss. While RSA's inherent design provides a functional salvage, optimal outcomes require meticulous tuberosity fixation and individualized rehabilitation.
Future research directions may address the gap in tuberosity repair technique comparison, like evaluating cable fixation versus suture fixation.
Limitations and future research
Limitations
This study has several limitations that warrant consideration. First, the small sample size limits the statistical power to detect significant associations between screw configurations and loosening. Second, the relatively short follow-up duration in some patients (less than 2 years) may not fully capture late complications or long-term functional outcomes. Third, the heterogeneity in fracture patterns among proximal fracture patients (three-part and four-part fractures with varying degrees of displacement and bone quality) may become confounding factors that could influence the results. These factors suggest caution when generalizing the findings to broader patient populations.
Future research directions
Future research should focus on three key areas. First, larger multicentre studies with standardized protocols are needed to validate the relationship between screw configurations and implant stability. Second, biomechanical studies comparing different screw fixation techniques, such as variable-angle versus fixed angle locking screw designs, could shed light on optimal fixation strategies. Third, long-term clinical outcomes of tuberosity fixing strategies, including the use of bone grafts and enhanced fixation methods, could be assessed to refine surgical techniques for fracture cases. Addressing these gaps could help optimize RSA implant stability and functional outcomes.
Conclusion
This retrospective study found that peripheral screw count does not significantly affect loosening. Greater tuberosity superior migration significantly reduces shoulder abduction range. Surgeons are advised to focus on optimal screw positioning and secure tuberosity fixation rather than maximizing screw quantity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.