
Abstract
Inferior pole patellar fractures present surgical challenges due to comminution and small fragment size. Conventional methods, such as transosseous suturing and separate vertical wiring (SVW), are associated with fixation failure and implant-related complications. This study introduces a modified non-metallic SVW (NM-SVW) technique using high-tensile polyethylene sutures (FiberWire® and FiberTape®) with cerclage augmentation to enhance stability and reduce implant-related issues. A retrospective case series of seven patients (mean age 70.8 years) treated between April and August 2024 was analyzed. Surgical outcomes, including radiographic union, clinical function, and complications, were assessed. All fractures achieved union within 11.1 weeks on average. At 6 months, the mean Böstman score was 28.6, indicating excellent knee function. No fixation failures or implant-related complications were observed. The NM-SVW technique provides a safe and effective alternative for comminuted inferior pole patellar fractures, offering strong fixation while minimizing hardware-related issues. Further studies with larger cohorts and longer follow-ups are needed to confirm these findings.
Keywords
Introduction
Inferior pole patellar fractures account for approximately 9.3% to 22.4% of all patellar fractures. 1 Although generally extra-articular, displacement of these fractures can compromise the knee's extensor mechanism, often making surgical intervention necessary. The main goal of surgery in these cases is to restore functional stability and mobility of the knee, rather than achieving a perfect anatomical reduction.2,3
These fractures are usually comminuted, with the small fragments posing challenges for stable internal fixation. One of the conventional approaches for managing comminuted inferior pole fractures is transosseous suturing. However, this approach can result in patellar shortening, alterations in patellofemoral joint mechanics, and potential long-term complications such as reduced quadriceps strength. 4
Another frequently performed technique, separate vertical wiring (SVW), has gained attention for showing comparable clinical outcomes with fewer complications related to bone healing.2,5,6 Biomechanical studies in cadavers indicate that SVW offers a significantly higher ultimate load to failure and improved mechanical stability by incorporating three tension bands. 7 However, fixation failures have been observed with sudden forceful knee contractions, causing the metallic to cut through the distal comminuted and fragile bone fragment, making a hinged knee brace recommended for temporary immobilization during the early postoperative period.3,7 Studies show that supplementing the construct with cerclage or rim plate can further increase the load to failure and lower the risk of vertical wire cut-through, thus improving the repair's stability and durability.3,8,9,10 However, metallic wire fixation techniques for patellar fractures are often associated with implant-related complications, including wire breakage from fatigue, migration or loosening, and skin irritation.11,12,20 Non-metallic suture-based fixation, on the other hand, has shown similar functional outcomes to metallic implants, with fewer hardware-related complications and a reduced need for implant removal.13,14,15,16 High-tensile sutures offer comparable strength to 18-gauge stainless steel wire, making them a viable alternative to traditional metal-based fixation.17,18
To address these challenges, we present a modified approach that used non-metallic separate vertical wiring (NM-SVW) with an added cerclage for comminuted inferior pole patellar fracture fixation. In this approach, we used high-tensile polyethylene sutures and tape instead of metallic wires or plates to reduce implant-related complications. To our knowledge, this technique has not been previously reported in the literature. This study aims to evaluate the outcomes of this fixation method for comminuted inferior pole patellar fractures, including radiographic and clinical assessments, functional results, postoperative complication rates, fracture union rates, and Böstman grading scores. 19
Methods
This study followed a retrospective case series design, with informed consent obtained from each participant. Eligible patients included those aged 18 years or older who presented with the AO Foundation/Orthopaedic Trauma Association (AO/OTA) fracture classification 34-A extra-articular patellar fractures. Between April 2024 and August 2024, seven patients with comminuted inferior pole patellar fractures underwent surgery with our technique by a single senior surgeon for consistency. Regular postoperative evaluations, including clinical range of motion assessments, radiographic monitoring for bony union, complication rate and function scores were conducted. All radiological results were assessed by two independent senior surgeons. Major complications were defined as deep wound infection, loss of fixation and revision surgery.
Surgical technique
We present our modified NM-SVW technique, employing FiberWire (Arthrex®, Naples, FL, USA), a high-tensile-strength suture featuring an ultrahigh molecular weight (UHMW) polyethylene core with braided polyester sheath and silicone coating, to replace the conventional metallic wire. The construct is augmented with a cerclage using FiberTape (Arthrex®, Naples, FL, USA), a 2-mm tape-shaped polyblend braid with similar composite properties to provide additional compression and prevent cut-through of distal fragments (Figure 1).
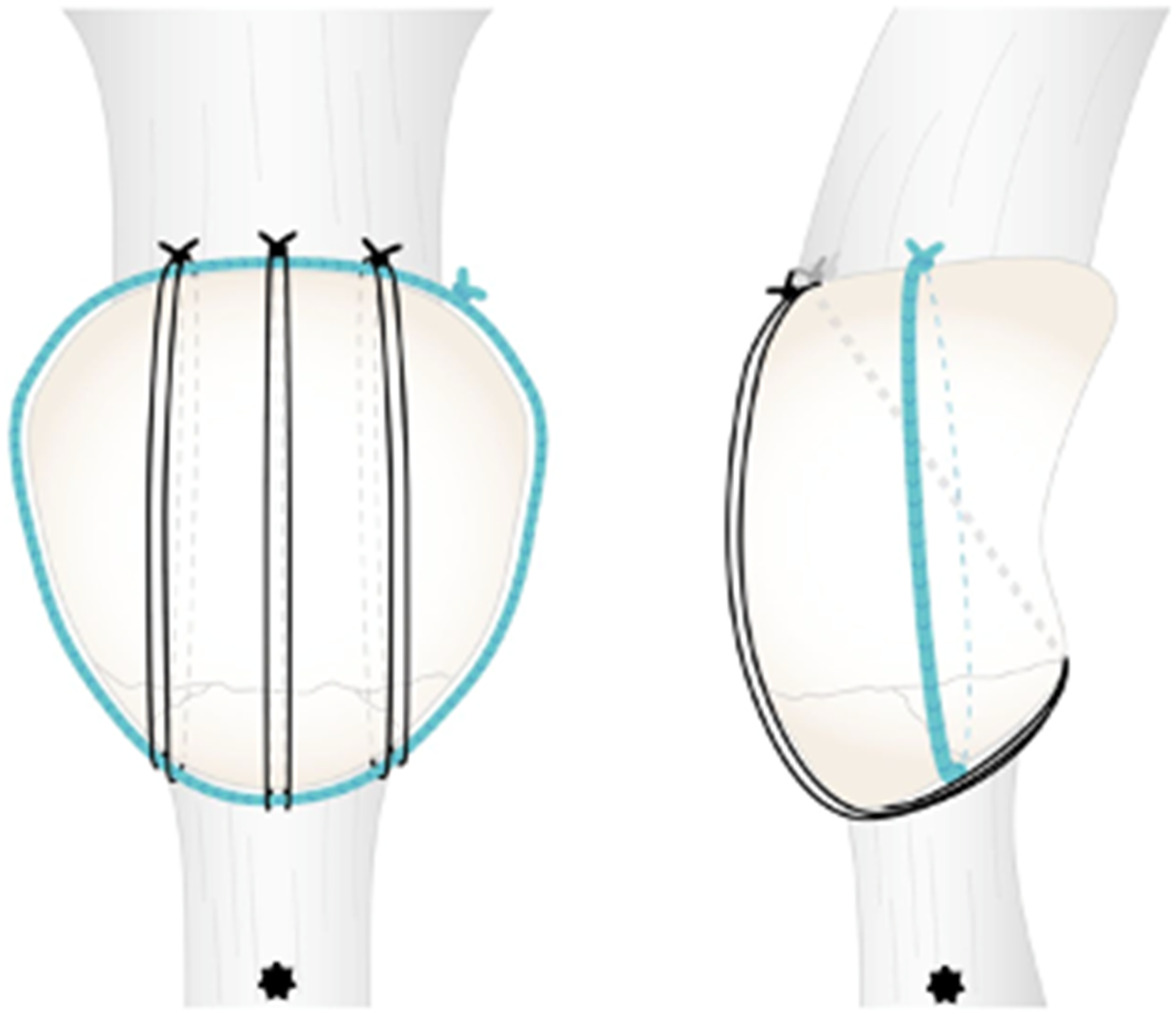
(*) Distal side. Illustration of the construct of the FiberTape circumferential cerclage and the FiberWire separate vertical wiring.
All surgeries were conducted with patients positioned supine under spinal anesthesia with a sandbag placed under the operating limb. All patients received a prophylactic antibiotic injection with intravenous dose of 2 g of cefazolin unless contra-indication. A pneumatic thigh tourniquet was used to provide a bloodless operative field.
A midline longitudinal incision over the patella was made. The length of the incision depended on the patella length, usually extending from just above the patella to the distal pole of the patella. After a full thickness skin flap elevation, the whole patella was exposed. The fracture site was debrided to remove excessive soft tissue that had been trapped between the fracture ends. A circumferential cerclage with FiberTape was wrapped around the patella by a wire passer in the usual manner (Figure 2). Three distal-posterior to proximal-anterior intraosseous tunnels were drilled in the proximal fragment using 1.4-mm Kirschner wires (K-wires) with the help of an aiming jig (Figure 3). A suture retriever was used to pass a double-stranded FiberWire through each of the three tunnels. All three FiberWire were then wrap around the distal fragment vertically and pass through the patella tendon just distal to the cerclage (Figure 4). Unless it was too comminuted, the fracture was temporarily held with a reduction clamp gently before tightening. Subsequently, the circumferential cerclage was tensioned using a 40-pound-force (lbf) tensioner (Arthrex® FiberTape Cerclage, Reusable) and the three vertical double-stranded FiberWire were sequentially tightened with the knee in mid-flexion position (Figure 5). All knots were securely buried beneath the quadriceps tendon. Intraoperative fluoroscopy was employed to confirm fracture reduction. Stability of fixation in full range of motion was tested intra-operatively before wound closure.

(*) Distal side. Arthrex® 2 mm FiberTape was first wrapped around the patella without tensioning.

(*) Distal side. Three intraosseous tunnels were drilled in the proximal fragment using Kirschner wires (K-wires) with the help of an aiming jig.

(*) Distal side. A double-stranded Arthrex® FiberWire was passed through each tunnel and wrapped around the distal fracture fragment distal to the FiberTape cerclage.

(*) Distal side. The circumferential cerclage was tensioned first and subsequently the three vertical double-stranded FiberWire were tensioned using a 40-pound-force (lbf) tensioner.
Postoperatively, full weight-bearing ambulation was allowed with a hinged knee brace set at 0–30 degrees for 2 weeks. The range of motion increased to 0–60 degrees from post-operation week-2, and to 0–90 degrees from post-operation week-4. Full range of motion was allowed on postoperative week-6.
Results
In this study, seven patients were included, consisting of five females and two males, with an average age of 70.8 years (range: 57–83 years). Two patients were injured on duty. All patients presented with a AO/OTA 34.1 comminuted fracture of the inferior pole of the patella with average number of fragments being 2.71 (range 2–4) and the displacement between proximal and distal pole was 10.7 mm (range 6–27 mm) The mean operative time was 88 minutes (72–130 minutes) and average blood loss was 21.4 ml (range 5–50 ml). The average time to achieve radiological bony union was 11.1 weeks (6–20 weeks). The patient demographics are shown in Table 1.
Patient demographics.
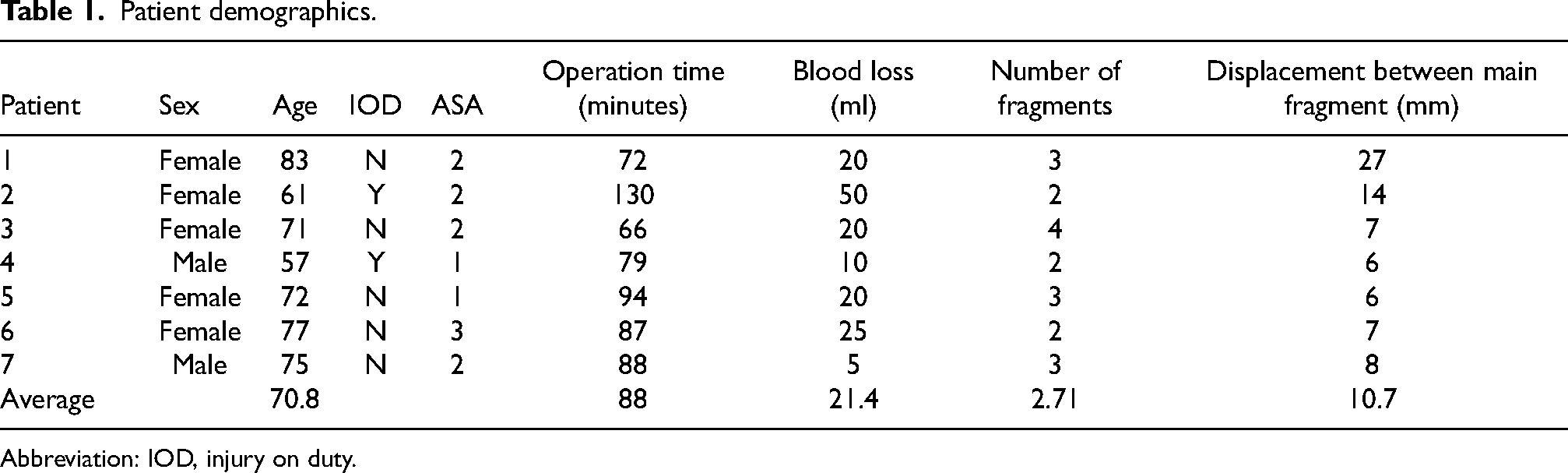
Abbreviation: IOD, injury on duty.
One case (patient 2) underwent revision surgery 3 weeks after the initial fixation, which had failed due to loosening of the construct. The initial procedure involved traditional transosseous suturing with a figure-of-eight tension band using FiberWire and FiberTape. The revision was performed using our NM-SVW technique, resulting in successful bony union 17 weeks post-revision (Figure 6).
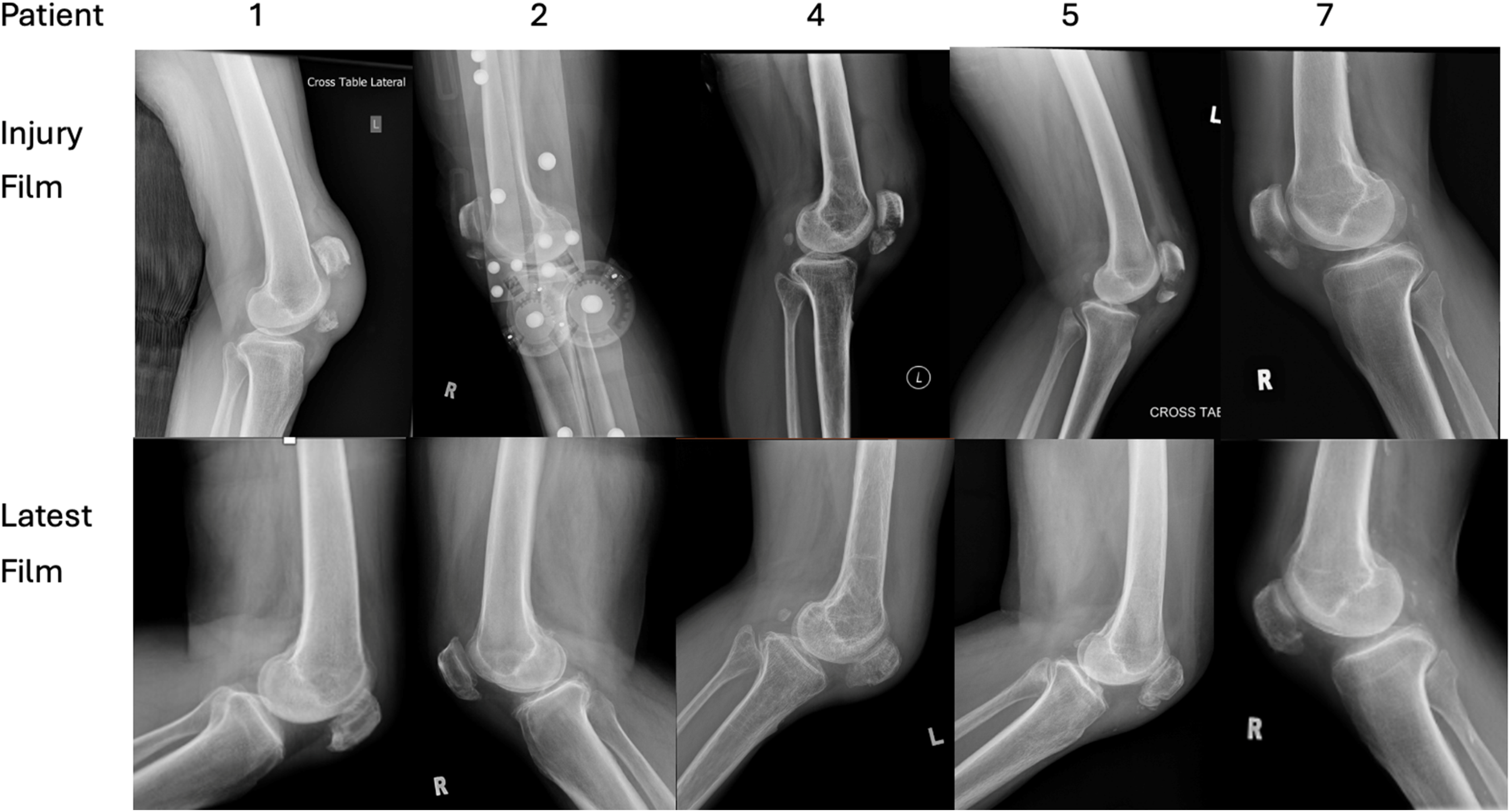
Examples of patients comparing injury and latest film.
All patients had at least a 6-month follow-up duration (6–10 months). The mean Böstman score for knee function at the latest follow-up was 28.6 (26–30). No major complications were identified. All patients achieved complete fracture union without needing additional surgical intervention or implant removal. Postoperative knee clinical function and radiological outcomes are shown in Table 2.
Post operative knee clinical and radiological assessment.
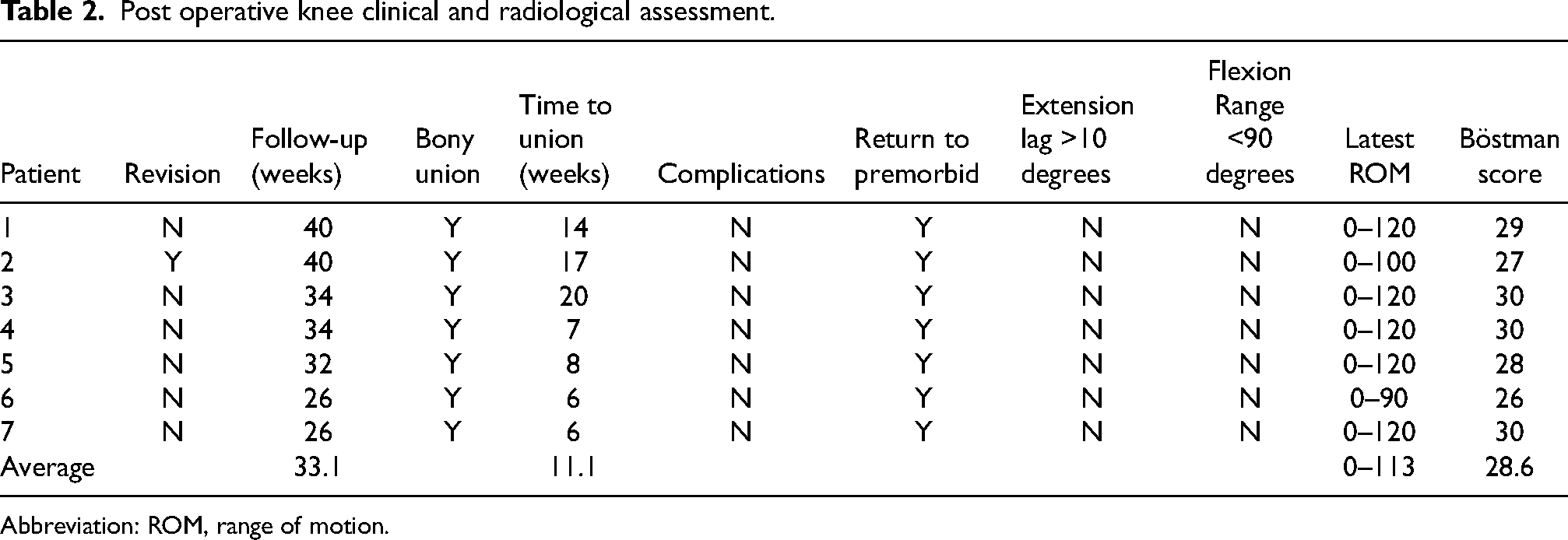
Abbreviation: ROM, range of motion.
Discussion
Fixation of inferior pole patellar fractures remains challenging, primarily due to comminution and the small size of the fragment. Despite the availability of several fixation techniques, traditional transosseous suturing and the SVW method have shown comparable clinical results and bone healing rates. 5 Multiple modifications of the technique have also been published.3,9 Despite multiple studies, there remains no clear consensus on the ideal fixation approach for these fractures. 14
Since it was first introduced, SVW with metal wires has gained acceptance as a dependable method for treating inferior pole patellar fractures. 10 However, fixation failures have been reported, often due to bone fragment cut-through by vertical wires in comminuted fractures. To address this issue, additional stabilization methods, such as rim plating, have been explored. These techniques have shown promising results by enhancing load capacity and reducing the risk of wire cut-out, with patients achieving bone union and no radiological signs of fixation failure. 9
Biomechanical studies have further illuminated the constraints of SVW with metal wiring showing that the ultimate failure load of SVW with only metal wire is around 250 N, while the quadriceps femoris muscle can exert forces up to 316 N during full extension in a cadaveric study. 17 One cadaveric study showed that the combined technique of SVW with cerclage augmentation significantly improved strength, with the ultimate failure load for the combined technique reaching 324.9 ± 50.6 N, compared to 216.4 ± 72.4 N for SVW alone. 8
Although metallic implants are commonly used for patellar fracture fixation, complications such as pain, implant prominence, and hardware failure remain prevalent, often necessitating implant removal. Studies have indicated that a significant proportion of reoperations are due to these implant-related issues. 20 High-tensile sutures have emerged as an alternative, offering comparable mechanical strength to stainless steel wire. Research has demonstrated that a double-stranded FiberWire construct achieves failure strength similar to metal wire (636 N vs. 580.7 N), suggesting that sutures may provide adequate stability while potentially reducing hardware-related complications. 18
In this case series, we describe a modified technique that has not been previously reported in the literature. Our NM-SVW approach utilizes the concept of combined method with SVW and cerclage. We further reinforced the fixation by adding FiberTape cerclage, which served as a rim support to minimize the risk of FiberWire cut-through and provide extra circumferential compression. Double-stranded FiberWire sutures were used to replace the metallic wire to reduce complications associated with metallic implants, while maintaining load-bearing strength comparable to stainless steel wire.
Our study achieved positive early clinical and radiological outcomes, with all patients attaining complete bony union and stable fracture fixation. No wound complications or implant-related issues were observed. None of the cases required revision surgery or implant removal. These results suggest that this modified technique may serve as a viable and safe option for managing comminuted inferior pole patellar fracture. Additionally, we successfully employed this technique in a revision case following a failed fixation of inferior pole fracture, indicating its potential as both a primary or secondary treatment option in similar cases.
This study is limited by its retrospective nature, small sample size and a short follow-up period. Prospective randomized trials with larger participant groups are needed to confirm the efficacy of this surgical approach.
In summary, our findings indicate that a modified NM-SVW technique using sutures and tape can yield favorable outcomes. This technique may offer an effective alternative for treating inferior pole patellar fractures, potentially reducing the risk of fixation failure and symptomatic hardware complications. However, to further validate its efficacy and safety, additional patient data and longer follow-up periods are necessary.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.