
Abstract
Background
Segmental fractures of long bones often result from high energy trauma. Anatomical reduction of the intercalated segment results in further devascularisation and increases risk of non-union. A less invasive approach is presented here in an attempt to handle these difficult fractures.
Methods
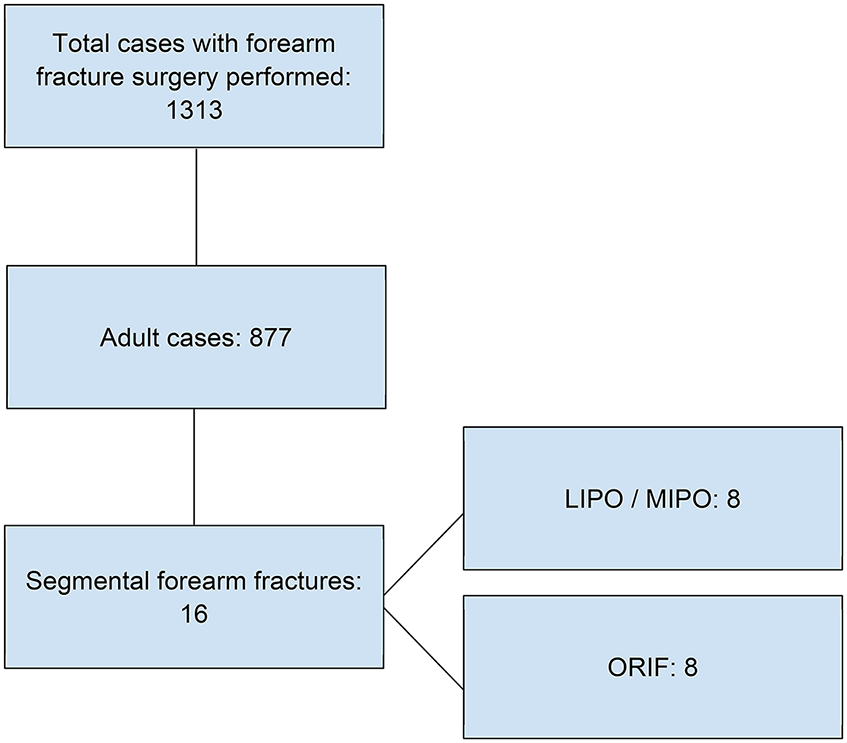
From 2008 to 2023, eight consecutive cases of patients with segmental forearm fractures treated with pre-bend or anatomical plate using either minimal or less invasive approach were analysed retrospectively. The surgical techniques and relevant anatomy are explained and illustrated with cases. The clinical outcomes including range of rotation and function, and rates of non-union and infection were compared to eight other cases of segmental forearm fractures treated with traditional open reduction and internal fixation (ORIF).
Results
Seven segmental ulna and three segmental radius fractures were fixed using less invasive approach. Four patients attained good range of movement and normal activity of daily living function. One patient required revision ORIF with bone graft. No iatrogenic neurovascular injury was noted.
Conclusion
Less invasive approach is a feasible alternative for segmental forearm fractures, especially if there is severe soft tissue injury. High rate of fracture union can be achieved with less surgical damage to the injured forearm.
Introduction
Forearm fractures can cause long-term functional impairment especially in terms of reduced range of rotation. Therefore, anatomical fixation, by means of open reduction and internal fixation (ORIF), is usually advised for adult patients with such fractures. It is supported in the literature showing very good surgical outcomes over the last decades.1,2
It was found that most of the previous studies on this topic include cases with varying energy of trauma resulting in different fracture patterns, degree of fracture comminution, and soft tissue injury. 3 This can cause significant heterogeneity and may not represent more severe cases.
Segmental forearm fracture is usually fixed by either intramedullary pinning, nailing, or ORIF. Intramedullary nailing is commonly used for fixation of long bones like the femur but may not be feasible for the forearm. Previous literature also showed mixed results of the existing forearm nailing implant. 4 Therefore, ORIF remains the mainstay of treatment for these fractures. For some cases it can be anatomically reduced if there is no severe comminution, otherwise it can be fixed with a bridging plate.
In this case series, we would like to introduce the operative techniques used in our centre to fix these fractures that are commonly associated with significant soft tissue injury. Two surgical techniques are used in this study aiming to minimise soft tissue trauma while applying bridging plate across the fracture. Minimally invasive plate osteosynthesis (MIPO) is used for segmental ulna fracture, while less invasive plate osteosynthesis (LIPO) is used for segmental radius fracture. The operative technique and clinical outcomes are discussed.
Study design
Patients undergoing surgery for forearm fracture during the period from 1 January 2008 to 31 December 2023 are retrieved in the computer record of our hospital. Paediatric patients, defined by age less than 18, were excluded because these fractures are usually fixed differently with Kirshner wires (K wires) due to their remodelling potential and the aim to preserve physis. Fractures not involving the diaphysis, such as fractures confined to the olecranon process, radial head and neck, and distal radius were excluded from this study.
Cases were assessed and reviewed to determine if the fracture pattern is segmental or not. Segmental fracture is defined by the presence of completely mobile and sizable fracture fragment(s) in between the most proximal to the most distal ends of the fracture. It is not uncommon to have fracture comminution in these cases due to high energy trauma. Cases with butterfly fragment only were excluded from this study. Examples were shown in Figures 1 and 2.

Butterfly fragment.

Segmental fracture.

MIPO for ulna shaft fracture.
Operative record was assessed to determine if ORIF or LIPO/MIPO techniques were used in at least one of the forearm bones.
Demographics
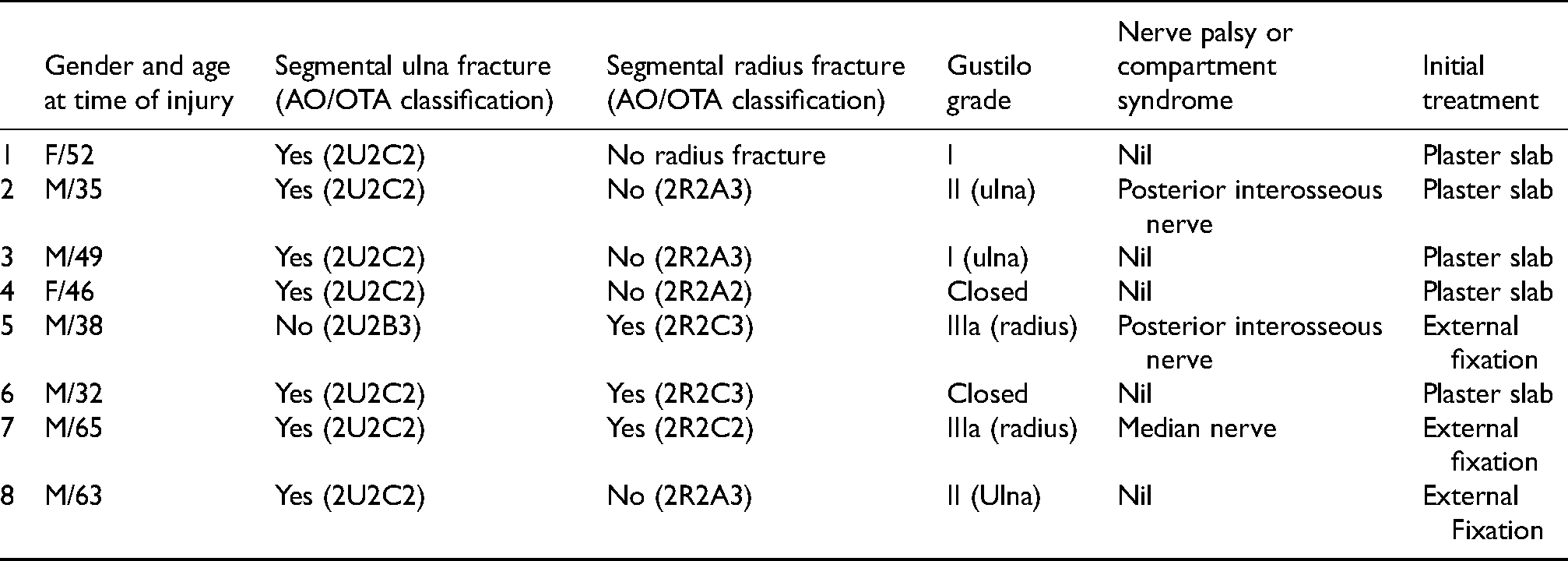
Eight cases of segmental forearm fractures fixed with LIPO/MIPO are included in this case series. Their age ranged from 32 to 65 years old. The soft tissue condition on admission was documented. Three patients required emergency external fixation.
Technique (ulna)
Fixation of the ulna is more straight forward, allowing the use of MIPO. The ulna is relatively straight and superficial. Plate can be applied subcutaneously without much problem (Figure 3). Therefore, the ulna is fixed first in cases of both bone segmental fracture. We prefer anatomical locking plates for the fixation of the ulna. Either a straight plate or a long anatomical olecranon plate with diaphyseal extension can be used, depending on the fracture level.
Reduction of the segmental fracture can be done by different means. An axial K wire can be inserted, usually proximal to distal in our series. The middle fragment can be manipulated by closed means to let the K wire pass through the fracture. In irreducible cases, incision was extended to the fracture end to aid reduction. With the intramedullary K wire acting as temporary reduction, MIPO can be performed. Particular care was taken during drilling and screw insertion. If necessary, the K wire can be retracted out bit by bit to allow more intramedullary space while the surgeon performs axial K wire assisted MIPO starting from one end of the fracture (Figure 4). Fine tuning of reduction could be done with percutaneous insertion of reduction hook or clamp.
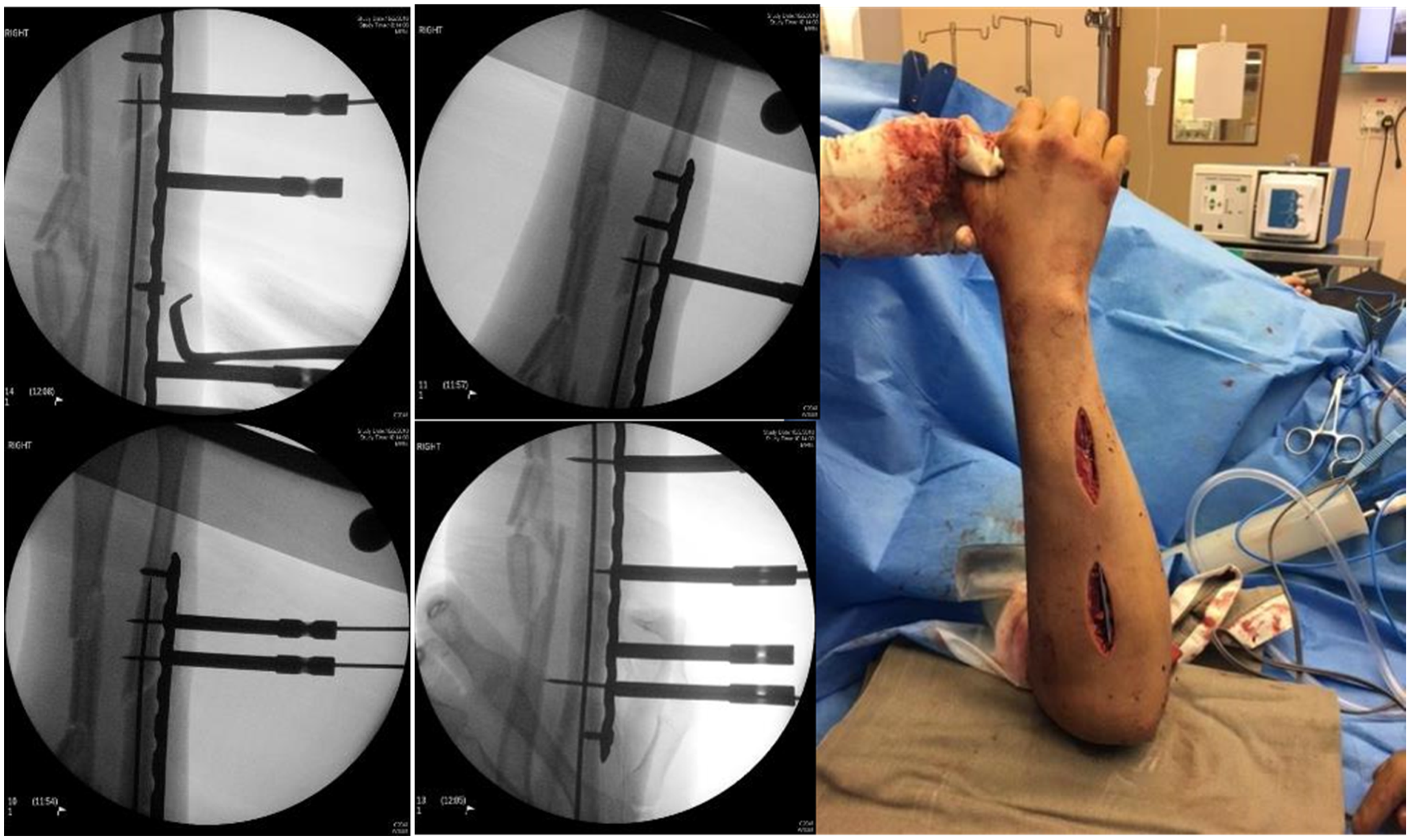
K-wire insertion for temporary fixation, allowing MIPO.

Pre-operative pre-bending of radial plate using life-size mirror image of the opposite forearm X-ray print-out, and the postoperative X-ray of the same patient.
Technique (radius)
Fixation of the radius is more challenging than the ulna due to its complicated and compact anatomical arrangement. Multiple neurovascular structures have to be protected during the operation. Two key differences, including preoperative templating and use of LIPO, are required to ensure good clinical outcomes.
Preoperative templating is essential to match the native radial bowing, allowing proper fitting of the plate onto the radius (Figure 5). For the earlier cases, we took an X-ray of the contralateral forearm. The radiograph was then flipped left to right and then printed out with the correct magnification. Reconstruction locking plate is chosen because it is easier to bend on the coronal plane to match the radial bowing. A plate with appropriate length can be selected and contoured using the print-out to fit the radial bowing. In recent years, three-dimensional (3D) printing can also be used. It is a very helpful tool that can allow the surgeon to confidently contour the plate onto the 3D bone model pre-operatively. After bending the plate, it can be sterilised and used intra-operatively.
In most cases, after ulnar shaft reduction was achieved, radial shaft fracture alignment was achieved by ligamentotaxis. With ulna reduced, radius was usually plated in supination as the interosseous membrane will help reduction, occasionally, if the patient had external fixation performed previously, the Schanz screw can also be used to assist reduction.
LIPO was then performed, with the aim of minimising soft tissue dissection while ensuring important structures are protected. A long skin incision was made, followed by the insertion of prebent plate through an extraperiosteal tunnel across the fracture. Bridging plate was inserted through a tunnel under the flexor pollicis longus and pronator teres under direct visualisation but without complete dissection (Figure 6). Proximally the interval is between flexor digitorum superficialis and supinator muscle. Distally we use the modified Henry approach between flexor carpi radialis and radial artery, followed by elevating the pronator quadratus to expose the volar distal radius for plate insertion and tunnelling. The volar surface of the radius is relatively flat from metaphyseal–diaphyseal junction to the radial tuberosity. The pre-contoured plate can fit the bone well without the need to further bend the plate or dissect the muscles. Screws are inserted percutaneously after gentle blunt dissection.

LIPO of the radius with reduction by means of ligamentotaxis.
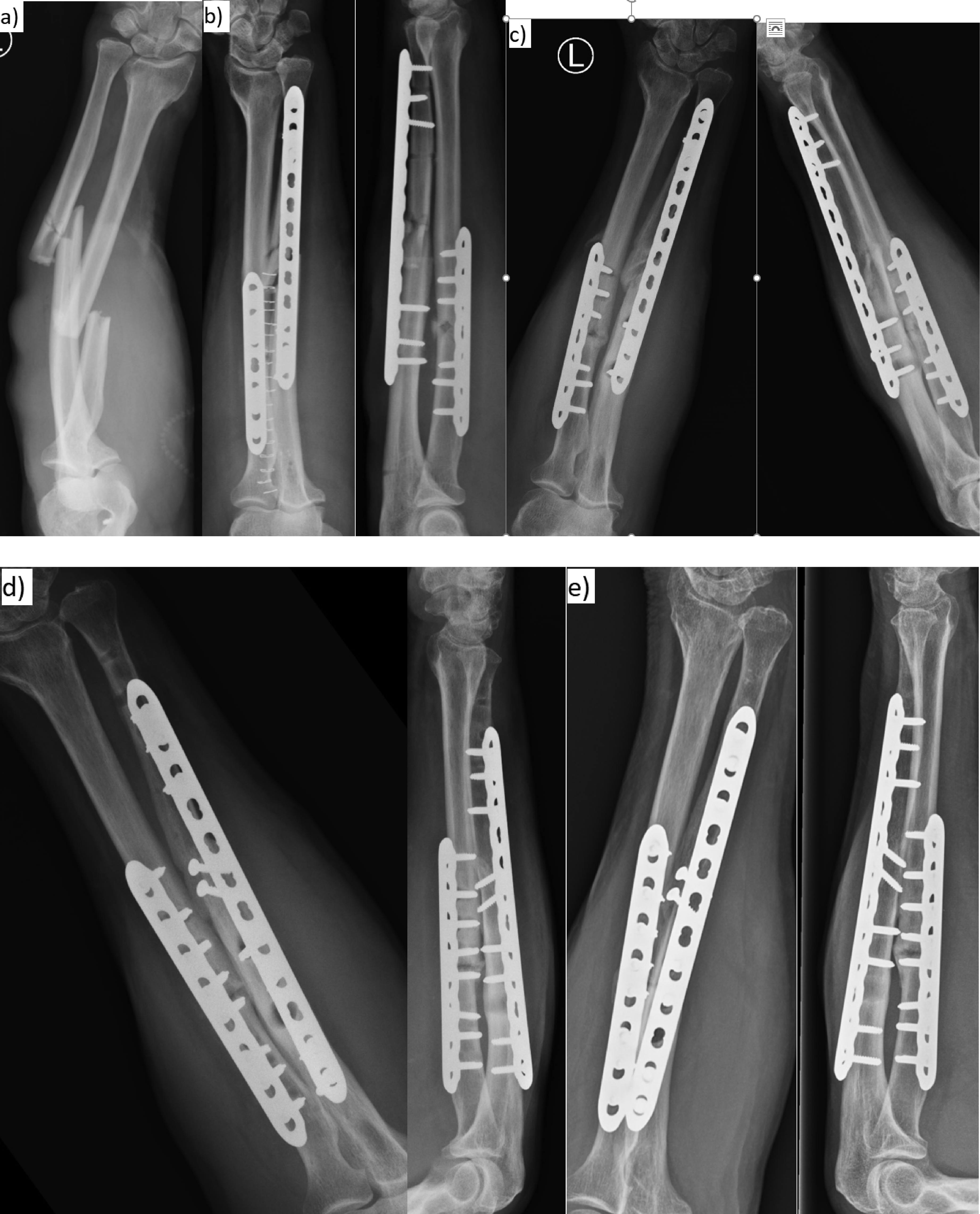
(a) Injury film of Case 8. (b) Initial fixation. (c) Hypertrophic non-union at eight months. (d) Revision ORIF. (e) Latest radiograph.
One of the important structures at risk is the anterior interosseous nerve at the mid-shaft level of the radius. To avoid damaging it, the plate should be inserted radial to the flexor pollicis longus muscle. Intraoperative use of X-ray is also crucial to ensure the plate is positioned on the bone and not skewed into the interosseous space. Another structure at risk is the posterior interosseous nerve (PIN). The forearm can be supinated to move the PIN dorsally, away from the surgical field.
Results
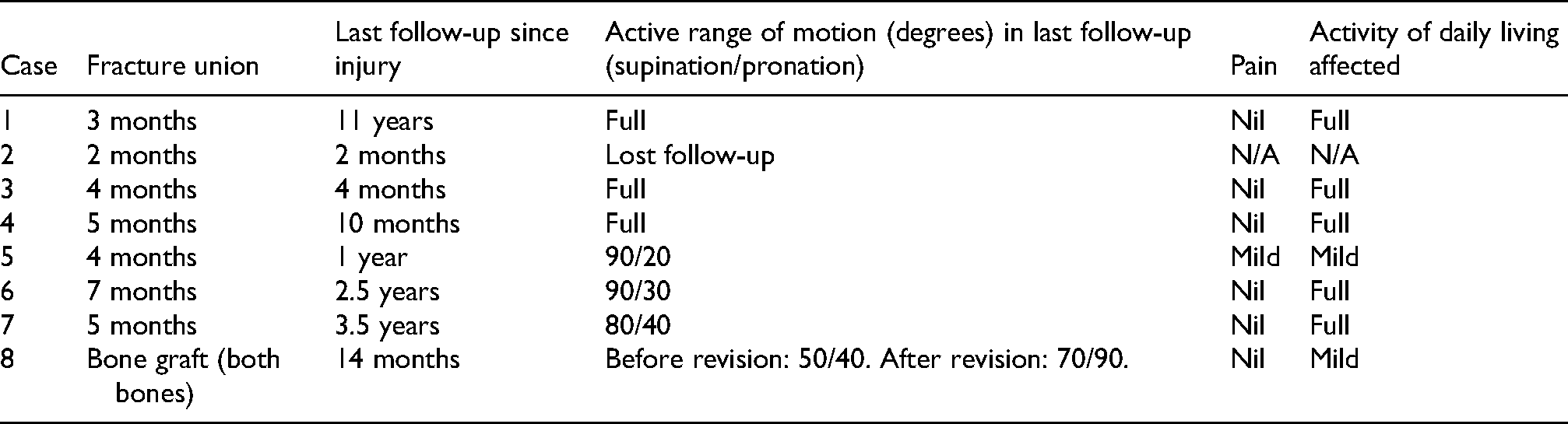
Seven out of the eight cases with LIPO achieve fracture union without the need of further surgical intervention. There was no osteonecrosis of the middle segment. No iatrogenic neurovascular injury was noted. Most of them reported no pain or functional deficit after fracture union.
The two cases requiring revision surgery are discussed in more detail. For our last case in this group (Figure 7), he underwent revision fixation with artificial bone substitute by traditional ORIF technique at post-op eight months due to infective non-union of both bones. Intra-operatively, there was yellowish turbid fluid over the fracture sites. The implants were loosened with hypertrophic non-union. Intraoperative culture came back to be coagulase negative Staphylococcus which was sensitive to gentamicin. Debridement was performed. Gentamicin-impregnated collagen matrix (Collatamp G, EUSA Pharma Europe, Oxford, UK) was inserted for infection control. Both bones were revised with LCP plate. During his latest follow-up in December 2024 (six months after the second operation), he had no forearm pain. The active supination and pronation ranges were 70° and 90° respectively. Radiologically, complete union was seen over the previous ulna fracture. For the radius, increasing amount of callus was seen across the fracture site with evidence of union at far cortex in December 2024.
There is another case (Case 5) with fracture union but required tendon transfer. He had Gustilo IIIa open fracture with PIN palsy on admission. It was observed that there was only partial recovery of the PIN palsy, with no active extension over his right thumb metacarpophalangeal joint and interphalangeal joint. Tendon transfer from palmaris longus to extensor pollicis longus was performed six months after the injury with restoration of motion afterwards.
Comparison with ORIF cases
Eight other cases with segmental forearm fractures were treated with traditional ORIF. There was neither compound fracture nor distal neurovascular deficit on admission. One case (Case 3) suffered from compartment syndrome with fasciotomy performed. ORIF was used instead of less invasive techniques in order to achieve anatomical reduction. The results were as follows:
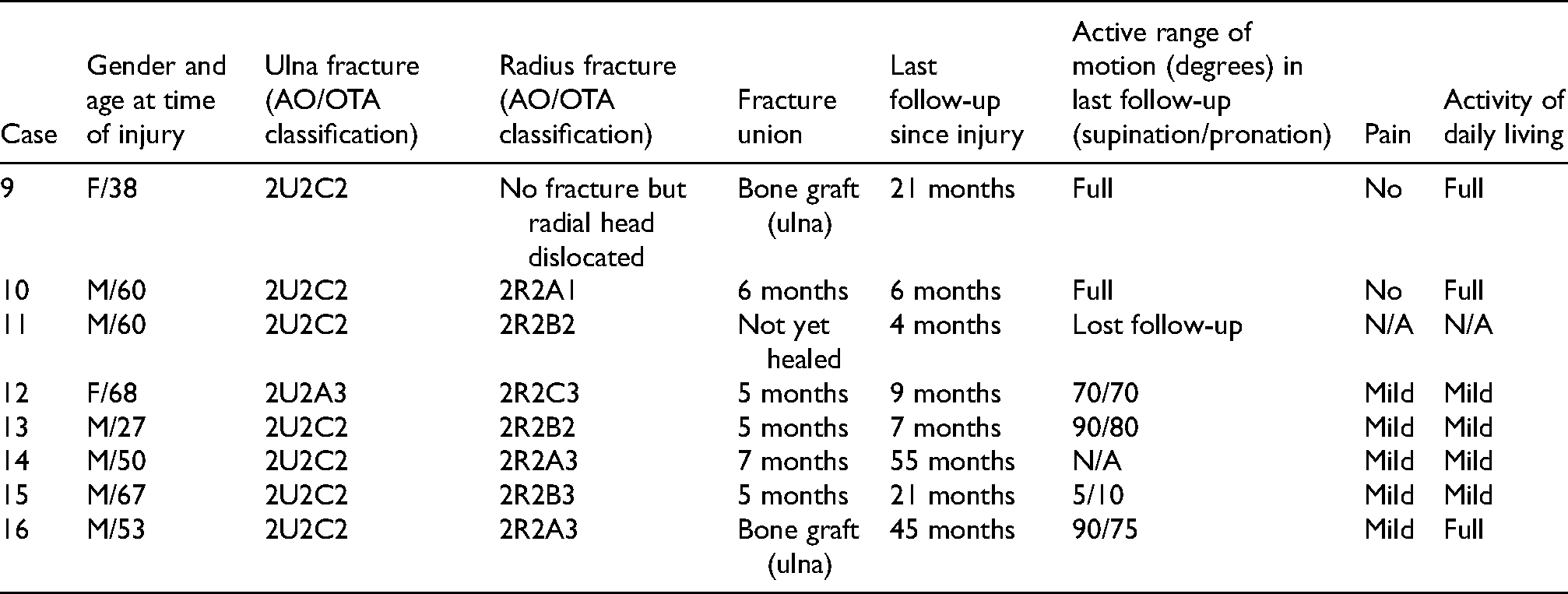
One case (Case 14) was complicated with postoperative infection. He was an active intravenous drug user with multiple fractures on admission after falling from height, including left forearm segmental fracture, right distal humerus fracture, right olecranon fracture, right femur shaft fracture, right patella fracture, left os calcis fracture, and skull fracture. He was admitted for left forearm abscess seven months after forearm fracture fixation. On examination, there was a 0.5 cm × 0.5 cm ruptured pustule just ulnar to the previous ulnar scar. Radiograph showed delayed union. Incision and drainage were performed. The fracture remained non-union. Subsequently, there was a new abscess formation at proximal part of the scar more than one year after the first incision and drainage. Another operation was done to drain the new abscess. The patient refused removal of implant or bone grafting. During the last follow-up 55 months after the initial injury, the previous wounds healed. There was no tenderness at the left forearm fracture sites. Radiograph still showed non-union. He defaulted follow-up afterwards.
Another case (Case 15) had extensive heterotopic ossification (HO) with subsequent synostosis at distal forearm level. Excision of HO was refused by the patient. When he was last seen in our clinic, he did not have any pain. He reported that despite his grossly limited rotation range, he was able to perform most of his activity of daily living. He accepted his current range and did not want any further intervention.
For the two non-union cases after ORIF (9 and 16), the fracture healed after bone graft. Intraoperative culture was negative in both cases.
Discussion
MIPO and LIPO are techniques evolved from the traditional ORIF. In ORIF, the fracture site is well exposed with the fracture haematoma evacuated. Small bone fragments that could not be fixed are often removed. Adequate periosteal elevation is performed before plate osteosynthesis. However, extensive periosteal stripping during ORIF could potentially lead to increased risk of non-union and infection, especially in patients with pre-existing severe soft tissue injuries. The subsequent soft tissue management could also be difficult for these patients with ORIF performed.
Other than facilitating further soft tissue management postoperatively, MIPO and LIPO may also improve fracture healing. The fracture site is often left untouched. The plate is then inserted through a submuscular extraperiosteal tunnel. Screws are then inserted to the plate. With preservation of more periosteum and fracture haematoma, the blood supply to the fracture is not jeopardised during fracture fixation. Preservation of blood supply is one of the essential elements for fracture healing. Therefore, MIPO is also used for other long bone fractures such as the femur. For the forearm, existing literature for MIPO is mostly limited to isolated closed ulna shaft fracture, with a case series showing good outcome for treated with MIPO. 5
The drawbacks of MIPO and LIPO for the forearm include the challenge to achieve anatomical reduction, and the risk of injury to neurovascular structures. Without exposing the middle fragment, reduction is more difficult. There is also a cadaveric study suggesting that MIPO percutaneous screw insertion for the volar approach of the radius could endanger various nerves over the forearm. 6 By limiting this study to segmental fractures and the use of LIPO instead of MIPO when fixing the radius, we can focus on those patients with more severe soft tissue trauma and more benefits from a less invasive but safe approach.
It is controversial whether to fix segmental fractures by ORIF or MIPO/LIPO. As previously mentioned, while the soft tissue envelope is better preserved with MIPO/LIPO, the trade-off is the inability to achieve perfect anatomical reduction. Without anatomical reduction, the patient could not restore full rotation of the forearm. Such malrotation could result in functional deficit. In the literature, patients can obtain 80° of pronation and 82° of supination after forearm fracture ORIF. 7 In this study, good rotation ranges could also be seen in our ORIF cases except the case with synostosis. In the MIPO/LIPO group, some of the cases had significant limitation in pronation. In a cadaveric study, a residual angulation of 20° could lead to functionally important loss of rotation while that of 10° would not. 8 This could indicate that there was considerable amount of malrotation using our less invasive technique. Nevertheless, while most of these patients have reduced pronation range, it can be at least partially compensated by shoulder abduction. 9
Infection was another concern when treating these fractures. There was one infective non-union (Case 8) after MIPO/LIPO, and one superficial infection (Case 14) after ORIF. The risk of postoperative infection was 12.5% in this series in both groups of patients. This is higher than what was quoted in the literature, with one case series suggesting 4% (one out of 25 cases) in both-bone diaphyseal open fractures. 10 One of the reasons for the increased incidence in this study could be the fact that segmental fractures are a result of high energy trauma with associated soft tissue injury. More cases will have to be recruited before this hypothesis can be confirmed. From this study, both groups seem to have similar infection risk.
Non-union did occur in our case series but these complications were successfully managed by revision surgery. Non-union is a known risk that can occur in up to 5% of cases with forearm ORIF performed. 11 In this study, one case in the MIPO/LIPO group and two cases in the ORIF group required revision ORIF with bone graft due to non-union. Of note, although six patients in the MIPO/LIPO group presented with compound fractures, all but one case achieved fracture union. The one non-union case was successfully treated with bone graft. This is a better result than the ORIF group, which include no compound fracture. This shows that the less invasive approach likely can decrease risk of non-union by preserving the biology, and can be considered in cases with significant soft tissue trauma.
In summary, whether a case with segmental forearm fracture is fixed by ORIF or a less invasive approach should be decided on a case-by-case basis. If there is no wound, ORIF remains the gold standard. If there is soft tissue compromise, the trade-off between malrotation and potential increased risk of infection and non-union has to be considered. The patient's age and premorbid status, and the fracture pattern should also be taken into account. For example, if one of the forearm bones was simple fracture while the other was segmental, the former can be plated by traditional ORIF with compression to guarantee correct length and rotation. The surgeon can then decide whether to fix the remaining segmental fracture by ORIF or MIPO/LIPO depending on the soft tissue status.
There are limitations in the present study. It is a single-centre study with a small number of cases spanning a long period of time. Adult segmental forearm fractures are not a common injury, as more than 90% of these forearm fractures are either simple or wedge fractures instead of segmental fractures. In these cases, there is no indication to abandon the use of well-established ORIF technique to achieve anatomical reduction and inter-fragmentary compression. Being a retrospective study, there was some limitation in data collection. One out of eight patients defaulted follow-up, which could lead to under-estimation of complication rate.
Another major limitation of this study is that the degree of malrotation after fixation remains unknown. The limited rotation range can also be attributed to postoperative stiffness other than malrotation. Postoperative computed tomography (CT) would be necessary to determine any malrotation. Further studies such as a multi-centre prospective study with defined protocol and inclusion criteria for MIPO/LIPO, and the use of CT to investigate for malrotation postoperatively would give more insight on the use of this technique.
Conclusion
The definitive fixation of segmental forearm fractures is still an evolving topic, with new implants under development for better functional outcomes. We hereby present an alternative to the traditional ORIF to fix these fractures in the forearm. With detailed pre-operative planning and good intra-operative techniques, it is believed that the MIPO/LIPO approach can be beneficial to these patients, as shown in the generally good outcomes in this case series.