
Abstract
Introduction
Developmental dysplasia of hip (DDH) is a major paediatric musculoskeletal problem that can cause lifelong disability if left untreated. Hong Kong currently adopts universal clinical assessment and selective ultrasound screening. This study aims to obtain a cluster-based epidemiology of DDH and to evaluate the effectiveness of the current screening system. It is also aimed to look for implication of capsular laxity and to propose optimal timing for first ultrasound.
Methods
Records of children referred to orthopaedics clinic in a major regional hospital for suspected DDH with ultrasound hips performed in 2017–2019 were reviewed. Patient demographics, ultrasound results, treatment and outcome of DDH were reviewed.
Results
Totally, 929 patients were referred with ultrasound hips done. Twelve of them were diagnosed with DDH. Another 2 patients presented late. The incidence of DDH in 2017–2019 was 0.89/1000 live births and delay diagnosis was 0.13/1000 live births. The open reduction rate was 0.19/1000 live births. Ninety-one patients had capsular laxity and normal follow-up ultrasound. Patients with capsular laxity were significantly younger than those without capsular laxity by Mann–Whitney U test. A statistically significant higher proportion of patients was found to have capsular laxity if first ultrasound was done before 6 weeks old (p < 0.001).
Conclusion
The incidence of DDH in the studied cluster is comparable to local study published a decade ago. The current system is justified given the comparable results of late diagnosis and open reduction rate to other developed countries. Purely capsular laxity is benign ultrasonographic finding and 6weeks old is a reasonable time to perform the first ultrasound to prevent overdiagnosis of it.
Introduction
Developmental dysplasia of the hip (DDH) is a major paediatric musculoskeletal problem that can lead to lifelong hip dysfunction and disability if missed and left untreated. Early detection and prompt treatment improve the outcome of DDH. Yet it remains debatable between selective ultrasound screening and universal ultrasound screening for the detection of DDH.1–4 The optimal timing of ultrasound is also controversial.5,6
Universal clinical assessment and selective ultrasound screening of suspected cases of DDH have been adopted in Hong Kong. Children after birth will have serial clinical examinations of hips done by different parties at different ages. They will be referred to the orthopaedics specialty clinic if there is any clinical suspicion of DDH. If there are clinical signs of a dislocated hip or dislocatable hip after seen by orthopaedics surgeons, the patient will be treated promptly with Pavlik Harness (PH). If there are no clinical signs of a dislocated hip or dislocatable hip, a routine ultrasound hip will be arranged to rule out DDH (Figure 1, flowchart of DDH screening in the studied cluster). In 2011, the point prevalence of DDH in Hong Kong Island was 0.87/1000 live births. 7 It was suggested that the protocol of universal clinical assessment and selective ultrasound screening for DDH is justified.
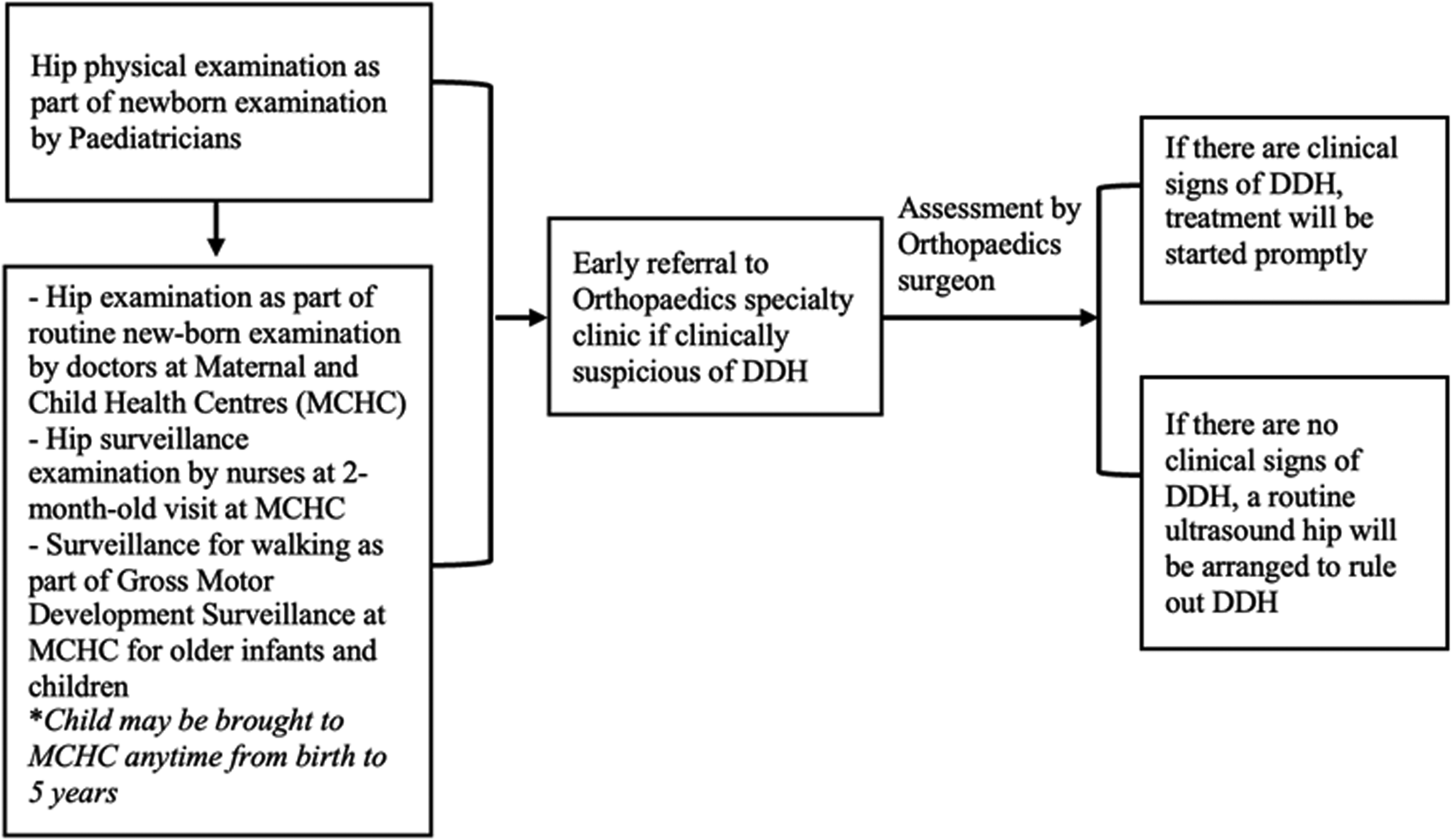
Flowchart of DDH screening in the studied cluster.
It has also been noted that some radiologists reported capsular laxity while performing ultrasounds hips for DDH. There is limited data regarding this finding but it is believed to be a benign physiological finding. It would be reported in the ultrasound results when there is normal findings in terms of alpha angle, beta angle and hip coverage, but the radiologists subjectively feel that the hip joint is lax on dynamic stress test but to not the extent of subluxation or dislocation. A follow-up ultrasound would be suggested for capsular laxity.
The study aims to obtain an updated cluster-based epidemiology data of DDH and to evaluate the effectiveness of the current screening system in the cluster. Also, we would like to look for the correlation between the ultrasound finding of capsular laxity and age, aiming to propose the optimal timing for the first ultrasound.
Materials and methods
Records of children referred to orthopaedics specialty clinic in a major regional hospital in Hong Kong for suspected DDH with ultrasound hips performed between 1 January 2017 and 31 December 2019 were reviewed. Patients with hip dysplasia with teratological causes or severe congenital disorders were excluded. Those referred to the clinic but defaulted to the arranged ultrasound hips or had private ultrasound hips performed were also excluded.
Data reviewed included basic demographics including gender, age of first attendance to the clinic, reason for referral and laterality. Ultrasound results including alpha angle, beta angle, hip coverage and dynamic stress test results including whether or not there is capsular laxity were reviewed. Treatment and outcome of DDH regarding whether to use conservative management or operative management were also reviewed.
Diagnosis of DDH was made based on clinical examination supported by radiological imaging. Those with static ultrasonography results of Graf type IIc or above or poor coverage of less than 1/3, or with dynamic ultrasonography results of subluxation or dislocation of the hip joint were diagnosed as DDH.
Patients with late presentation of DDH were reviewed separately in the study. It is defined as DDH presenting after 6 months old. The diagnosis was made with X-ray showing subluxation or dislocation of hip.
Statistical analysis was performed using IBM SPSS version 29.0.2.0(20). Chi-squared test was used to compare two categorical variables. Mann–Whitney U test was used to compare two categorical and continuous variables.
Results
There were 970 patients referred for suspected DDH between 1 January 2017 and 31 December 2019. Forty-one of them were excluded because they defaulted to the arranged ultrasound hips or had private ultrasound hips done. The remaining 929 patients had ultrasound hips done in the studied hospitals (accounted for 5.9% of live births in the cluster).
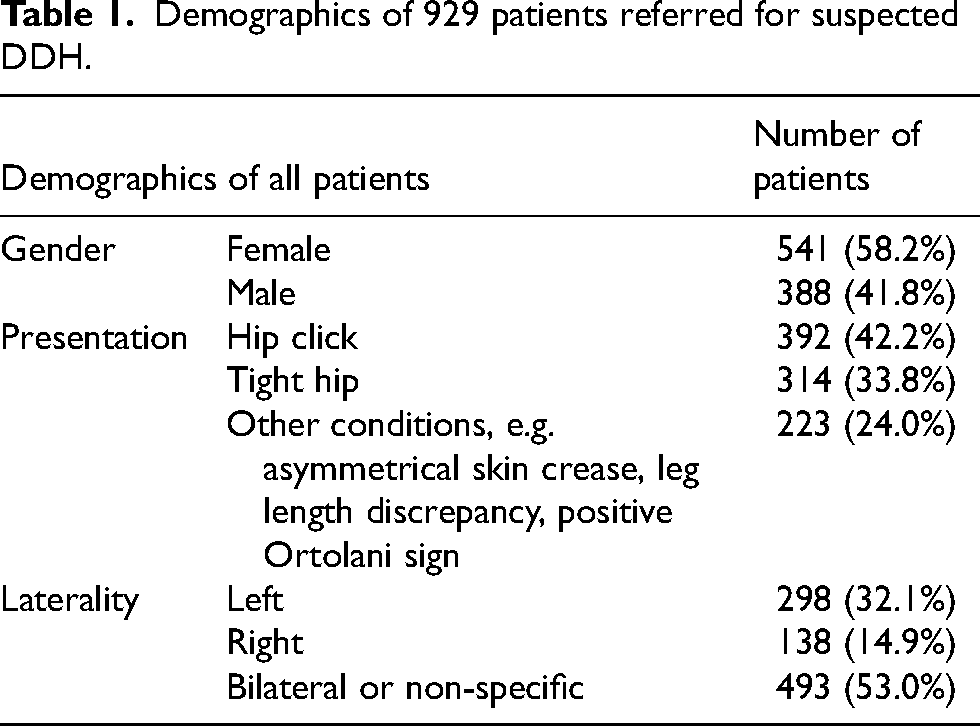
There were 541 (58.2%) female patients and 388 (41.8%) male patients. For the reason of referral, 392 (42.2%) of them were referred for hip click, 314 (33.8%) were referred for tight hip, 223 (24.0%) were referred for other conditions such as asymmetrical skin crease, leg length discrepancy, and positive Ortolani sign. For the side of involvement, 298 (32.1%) of them involved the left hip, 138 (14.9%) involved the right hip, and 493 (53.0%) involved bilateral hips or not specified side. The mean and median age of first attendance in SOPD were 55 and 42 days old, ranging from 5 days old to 176 days old (Table 1, demographics of 929 patients referred for suspected DDH).
Demographics of 929 patients referred for suspected DDH.
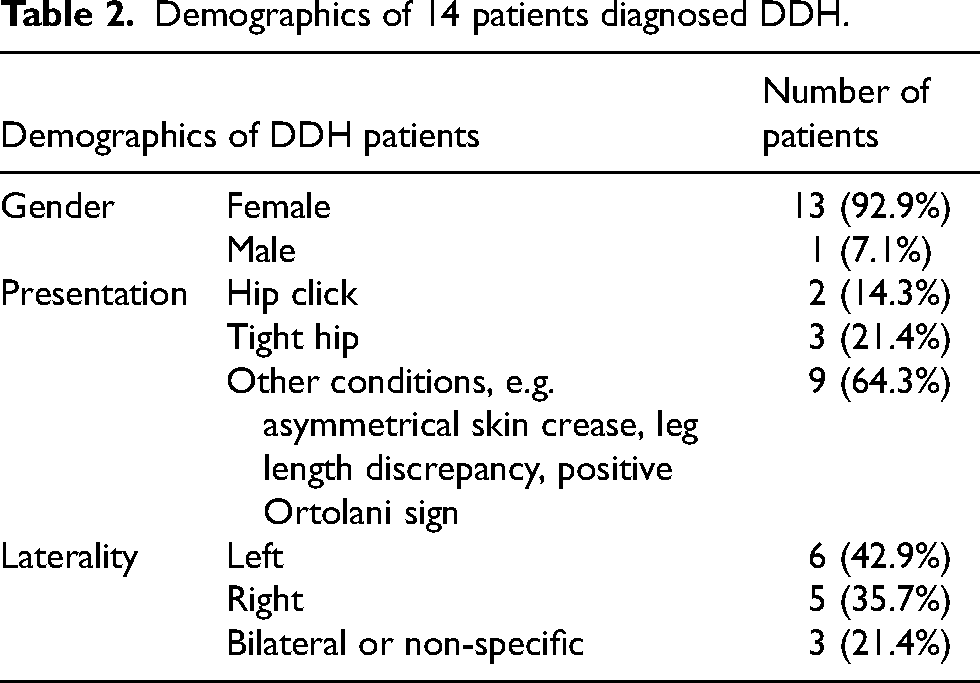
There were 14 patients diagnosed with DDH from 2017 to 2019, of which, 12 patients were diagnosed before 6 months old supported by the selective ultrasound screening. Two patients were late presentation. Live births in the studied cluster from 2017 to 2019 were 15,691. The incidence of DDH from 2017 to 2019 was 0.89/1000 live births. The mean age of presentation to the orthopaedics specialty clinic was 35 days, range from 5.5 days to 80 days. The female-to-male ratio was 13:1. There were 3 bilateral DDH, 6 left DDH and 5 right DDH. Among those 12 patients diagnosed by the selective ultrasound screening, 2 of them presented as hip click, 3 presented as tight hip, and 7 presented as asymmetrical skin crease (Table 2, demographics of 14 patients diagnosed DDH). Two patients had positive Ortolani sign in physical examination by orthopaedic surgeon during the first attendance to the orthopaedics specialty clinic, and treatment was started after examination. The other 10 patients had static or dynamic ultrasound findings of DDH, and treatment was started after ultrasound.
Demographics of 14 patients diagnosed DDH.
As for the 2 patients who presented late for DDH, one with bilateral DDH presented at 592 days with leg length discrepancy, and another patient with left-side DDH presented at 1091 days with leg length discrepancy and gait disturbance. The late diagnosis rate of DDH was 0.13/1000 live births.
Ultrasound results
Ultrasonography was performed on both hips of the 929 patients (1858 hips were examined in total). Graf classification was analysed in terms of hips. There were 1806 hips classified as type I, 36 classified as type IIa, 9 classified as type IIb, and 7 classified as type IIc or above (Table 3, ultrasound results with Graf classification).
Ultrasound results with Graf classification.
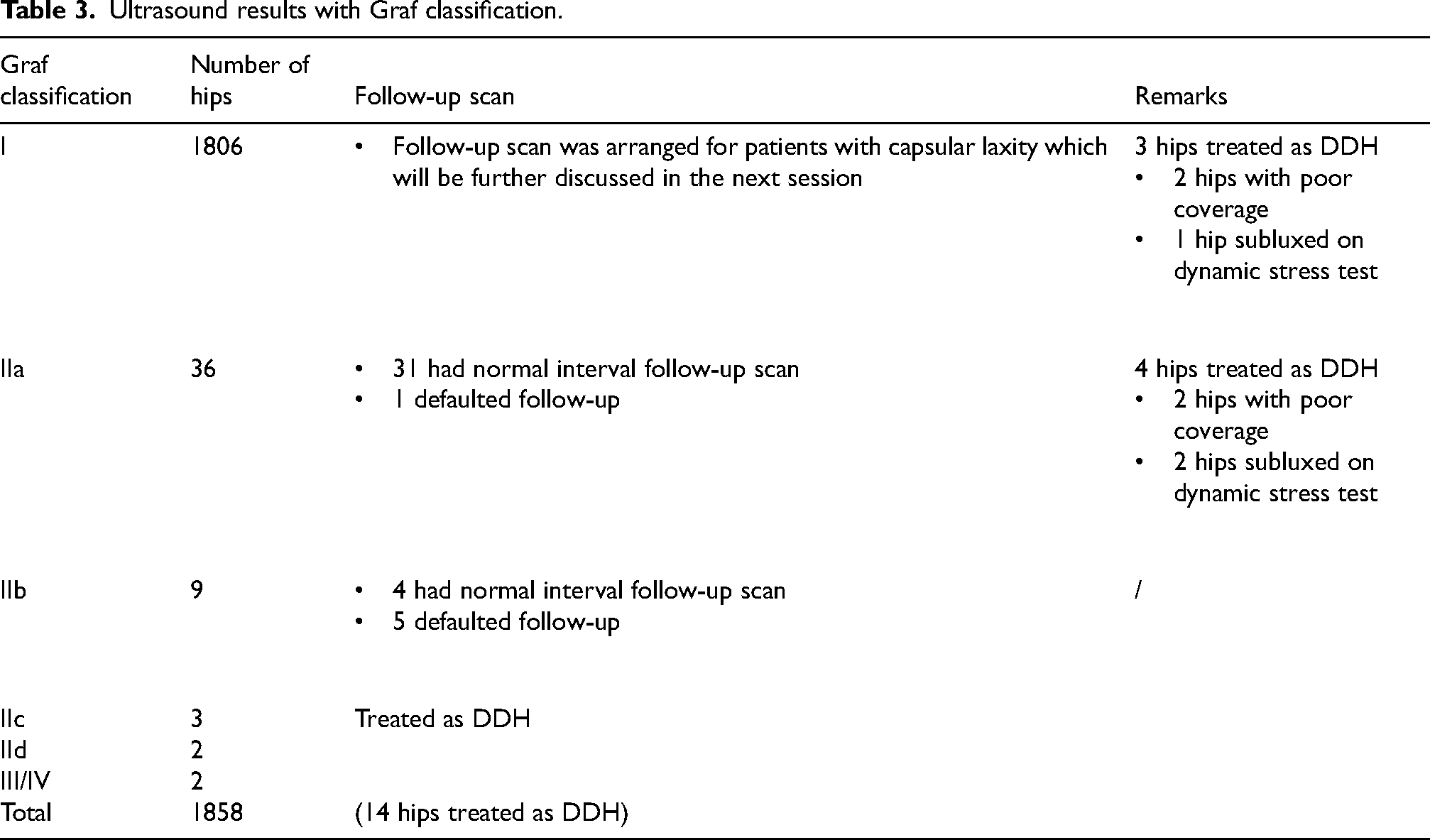
For those 36 hips classified as Graf IIa, apart from the 4 hips that were treated as DDH due to poor coverage or subluxed on the dynamic stress test, the remaining 31 of them had normal interval follow-up ultrasound scan and 1 defaulted follow-up. For the 9 hips classified as Graf IIb, 4 of them had normal interval follow-up scans and 5 of them defaulted follow-up.
There were 14 hips treated as DDH. (Among the 12 patients diagnosed with DDH by the selective ultrasound screening, 2 had bilateral hips affected, 5 were left-sided and 5 were right-sided.) Among the 14 hips treated as DDH, 3 of them were classified as Graf I, 4 of them were Graf IIa, 3 were Graf IIc, 2 were Graf IId and 2 were Graf III or IV.
Capsular laxity
The study further analysed the ultrasound results of capsular laxity. It was defined as the subjective feeling of the radiologists to feel that the hip joint is lax on dynamic stress test but to not the extent of subluxation or dislocation. Patients who had normal clinical findings with ultrasound results of bilateral hips Graf type I, adequate hip coverage, and no subluxation or dislocation in the dynamic test were included for further evaluation. There were 870 patients fulfilling the criteria. Among these patients, 91 patients (10%) had capsular laxity. Thirty-five of them had bilateral hip involvement while 56 of them had unilateral hip involvement. Follow-up ultrasound performed at around 6 weeks-time was normal. All patients did not need treatment.
For those 779 patients without ultrasound findings of capsular laxity, the mean and median age for them to receive the first ultrasound were 75 days old and 78 days old. As for those 91 patients with findings of capsular laxity, the mean and median age to receive the first ultrasound were 43 and 41 days old. Using the Mann–Whitney U test, patients with capsular laxity had their first ultrasound done at a younger age than those patients without capsular laxity and it was statistically significant. (Figure 2, the mean rank for patients with capsular laxity was 229.79, and the mean rank for patients without capsular laxity was 459.53, p < 0.001.)
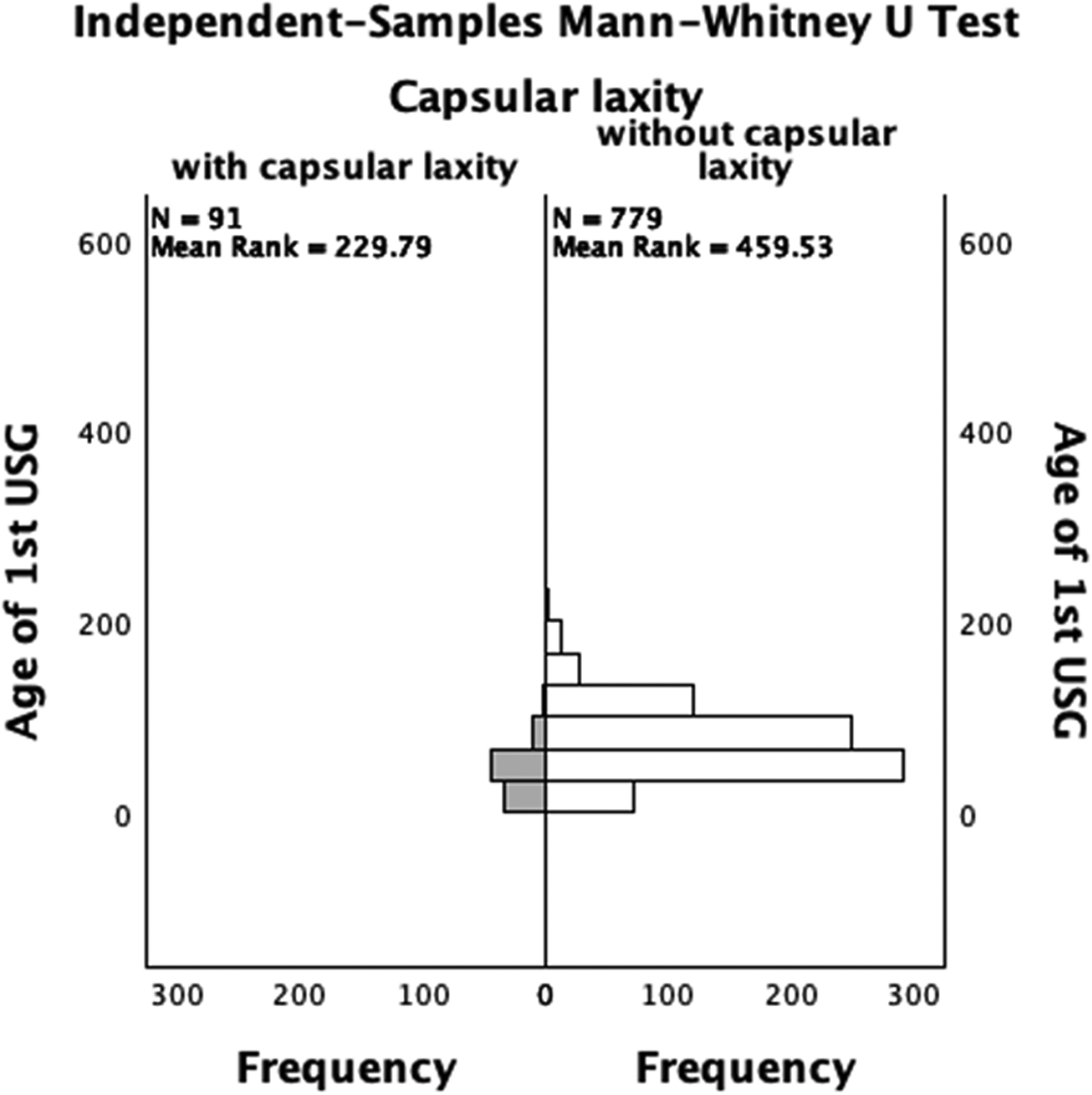
Mann–Whitney U test: age of first ultrasound for patients with capsular laxity and without capsular laxity, p < 0.001.
Of those patients with results of capsular laxity in the ultrasound results, 50 of them (55%) had their first ultrasound done before 6 weeks old and 41 of them (45%) had their first ultrasound done after 6 weeks old. Using the Chi-squared test, 23.6% of patients were found to have capsular laxity if the ultrasound was done before 6 weeks old, while 6.2% of them were found to have capsular laxity if the ultrasound was done after 6 weeks old. A higher proportion of patients were found to have capsular laxity if the first ultrasound was done before 6 weeks old and it was statistically significant (Table 4, Chi-Squared test Pearson Chi-Squared value 51.558, p < 0.001).
Chi-squared test for patients with and without capsular laxity, with ultrasound done before and after 6 weeks old.
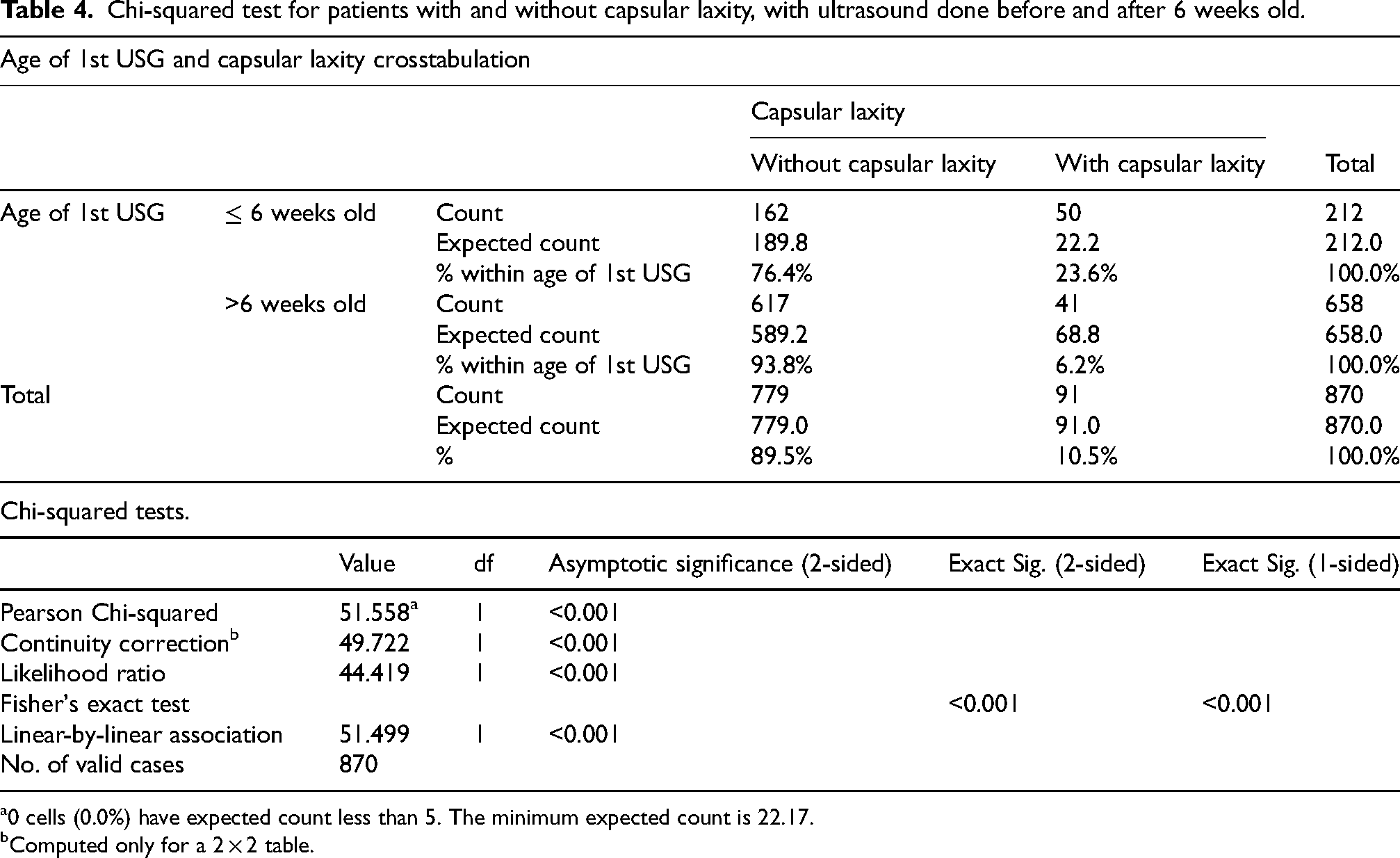
0 cells (0.0%) have expected count less than 5. The minimum expected count is 22.17.
Computed only for a 2 × 2 table.
Treatment and outcome of DDH
Twelve patients diagnosed by the selective ultrasound screening program were treated with PH. Eight (67%) of them succeeded and the mean age of starting PH was 31.75 days old (range 6–56 days old). Four (33%) patients failed PH and required further operative management. The mean age of starting PH was 86.5 days old (range 65–103 days old). Three patients received close reduction of the hip with arthrogram and casting. One patient received major operation with open reduction. As for the 2 patients who presented late with DDH, both of them required open reduction and osteotomy. The rate of open reduction was 0.19/1000 live births.
Discussion
The study found that the incidence of DDH in the studied cluster from 2017 to 2019 was 0.89/1000 live births. This figure is comparable to the local study in Hong Kong Island done by The University of Hong Kong in 2011. 7 The incidence of DDH in different localities of Hong Kong has been similar over the years.
Study results also showed that patients with ultrasound results of capsular laxity all had normal follow-up ultrasound scans. It is a normal ultrasound finding and is statistically significantly associated with the age to perform the first ultrasound. The younger the patient, the more likely they have capsular laxity. Based on the study results, for patients with no signs of hip instability or dislocation in physical examination, if the first ultrasound was postponed to 6 weeks old, 55% of rescan ultrasound can be prevented due to purely capsular laxity.
The appropriate timing for ultrasound is controversial. There have been studies suggesting that the ultrasound of hips should be performed on older infants to improve screening accuracy. A study done in Taiwan in 2019 suggested that the false positive rate can be reduced if the ultrasound hips is performed after 4 weeks. 6 Reducing the false positive rate and improving the accuracy of screening help to reduce parental anxiety. As noted in our study, capsular laxity is related to younger age of patients and it turns to normal with aging. The waiting time for the rescan ultrasound can cause parental anxiety. It also requires further follow-up imaging and a follow-up visit to the clinic. Postponing the ultrasound to 6 weeks old helps to prevent overdiagnosis of capsular laxity and prevent rescan ultrasound. It helps to better allocate our resources to meet the increasing demand in the future, as it has been noticed that there are increasing numbers of referrals for suspected DDH and ultrasound hips performed despite the decrease in the birth rate.
It raised a question that if the first ultrasound scan was postponed to 6 weeks old, would it lead to delayed diagnosis of DDH and subsequently delay in initiation of treatment? First, if patients demonstrate positive signs that raise high suspicion of DDH during clinical examination, such as a positive Ortolani sign, they will be investigated and treated promptly. The postponement in ultrasound hips is suggested for patients with normal physical examination. There is a retrospective case-control study in 2019 published in the Journal of Paediatric Orthopaedics that compared the outcomes of patients who started PH at different ages. 8 In the study, patients were divided into 3 different groups which started PH less than 30 days, between 30 and 60 days, and more than 60 days. It showed that there was no significant difference in the failure rate of PH by age. With a reasonable postponement of the first ultrasound, it will not affect the functional outcome of treatment.
It is shown that the current selective ultrasound screening program prevented 8 patients with DDH (8/14, 57%) from having operative treatment. Of the 4 patients who required further operative treatment after PH, 3 of them were able to be managed by arthrogram and close reduction while only 1 of them required major operation with open reduction. Counting the 2 patients who presented late with DDH that required open reduction and osteotomy, there were 3 patients requiring open reduction surgery. The rate of open reduction was 0.19/1000 live births. The late diagnosis rate of the hip screening program was 0.13/1000 live births. The late diagnosis rate and the rate of open reduction surgery of the current screening program are comparable to the figures in other developed countries. For example, the late diagnosis rate in Edinburg from 1962 to 1982 was 0.5/1000 live births, 9 and the rate for open reduction for DDH in Austria in 2004 was 0.13/1000 live births. 10 An effective screening program for DDH should help to diagnose patients with DDH promptly so that they can be treated accordingly and to prevent the rate of major operation. Meanwhile, it needs to be cost-effective. The late diagnosis rate with the current selective ultrasound screening program is comparable to other developed countries, and with the low incidence of DDH in our locality, the current selective ultrasound screening program is justified and effective.
Reviewing our 2 patients who presented late, one patient had the new born examination done in the private sector all along until she developed leg length discrepancy and was referred to our clinic. It is recommended that the serial clinical examination and surveillance of the hips be adhered to in the health sectors, hopefully increasing the likelihood of early diagnosis. The other patient presented late has bilateral DDH. She presented with reduced abduction range of both hips which the range of movement of abduction over the right side was 60° and the left side was 70°. With the reduction in the abduction range of hips in infants, doctors and nurses should raise suspicion about this abnormal physical examination finding and refer to Orthopaedics surgeons promptly for further investigation.
One limitation of this study is that the study duration was relatively short. A longer-term study would be better. Also, the figure can be overestimated or underestimated because several patients could not be included in the study, including those born in the studied cluster but presented to hospitals in other clusters and those who defaulted to follow-up in our unit. Given this limitation, a central registry for DDH is recommended for future research purposes and to better analyse our local data.
Conclusion
The incidence of DDH in the studied cluster between 2017 and 2019 was 0.89/1000 live births. The late diagnosis rate in detecting DDH and the rate of open reduction with the current screening program are comparable to those of other developed countries. The current program with universal clinical assessment and selective ultrasound screening for DDH is justified and effective. Moreover, a reasonable postponement of the first ultrasound to 6 weeks old for patients without clinical signs of hip dislocation is suggested to prevent overdiagnosis of capsular laxity which would need repeated ultrasound scans and follow-ups.
Footnotes
Author contributions
All authors had full access to the data, contributed to the study, approved the final version for publication and took responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the NTWC ethics committee with the reference number NTWC/REC/22049. Patient consent was waived by the ethics board.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.