
Abstract
This study investigates the use of a bioinductive collagen scaffold patch to enhance the surgical repair of “degenerative” Achilles tendon ruptures in individuals with pre-existing tendinopathy. The aim is to improve tendon healing quality and enhance clinical function. A retrospective case series of patients with acute Achilles tendon ruptures and pre-existing tendinopathy who underwent surgical repair augmented with a collagen implant was analyzed. A mini-open surgical repair was performed using Krakow locking sutures with the augmentation of a collagen patch. Standardized rehabilitation protocols were followed, and participants were followed up for at least 6 months post-surgery. Nine participants were included in the study. No major complications, including re-ruptures, were reported within six months of surgery. Statistically significant improvements were observed in foot and ankle outcome scores. The Victorian Institute of Sports Assessment – Achilles score also showed progressive improvement. The use of a bioinductive collagen patch augmentation in patients with degenerative Achilles tendon rupture appears to be safe and feasible. However, the study's limitations include its retrospective nature and small sample size. Future prospective studies with a control group are needed to provide more comprehensive insights into the efficacy of this surgical procedure. This is the first published case series utilizing this novel bioinductive collagen patch to augment Achilles tendon repairs. These preliminarily positive results on improving the surgical management and outcomes of individuals with this challenging condition of tendinopathy complicated Achilles ruptures warrant further research in this area.
Introduction
The study focuses on the challenging task of managing the surgical treatment of Achilles tendon rupture in individuals with pre-existing tendinopathy. Achilles tendinopathy is a common condition that affects both active and sedentary individuals,1–3 with nearly 30% of individuals who have experienced an acute Achilles tendon rupture reporting a history of pre-existing tendinopathy. 4
Surgical treatment of Achilles tendon rupture in individuals with pre-existing tendinopathy poses a unique challenge due to the mechanical deficiencies in a weakened tendon.5–7 The presence of tendinopathy can compromise the tendon's structural integrity and healing capacity, making it more susceptible to re-rupture and poor functional outcomes.8–10 In such cases, multiple strategies are often implemented to address both the acute rupture and the chronic tendinopathy.11,12 These strategies can range from more conservative rehabilitation programs to additional surgical procedures,13–16 such as a flexor hallucis longus tendon transfer, to reinforce the weakened tendon.17–19
However, orthopedic surgeons are continually searching for innovative strategies to enhance the healing process and improve the quality of tendon repair. 20 One promising solution that has shown success in other musculoskeletal conditions, such as massive rotator cuff tears, is the use of a bioinductive collagen scaffold patch.21–23 Bioinducible collagen implants are used in rotator cuff regeneration. Histologic and MRI imaging of the new tendon after implantation showed full integration of the implant and no inflammation or foreign body reaction. Clinical parameters, thickness, and MRI signal of the tendon improved significantly at 6 months. Meanwhile, good re-tear rates and patient outcomes are also obtained. This bioinductive collagen implant acts as a scaffold, providing structural support and promoting the recruitment and differentiation of cells involved in the healing process. It has been shown to accelerate healing and improve the quality of tissue repair in various applications.
There have been previous case reports on utilizing a bioinductive collagen patch as a surgical augmentation in tendinopathy patients.24,25 This study is currently the only case series on this surgical technique. The findings of this study may have implications for improving the surgical management and outcomes of individuals with this challenging condition. Ethical approval was obtained from the Clinical Research Ethics Committee of the New Territories East Cluster (Ref: 2024.088). The study was registered at clinicaltrials.gov (NCT06252389).
Methods
Study design
This article presents a retrospective case series investigating the treatment of Achilles tendon rupture complicated by pre-existing tendinopathy with repair augmented by a bioinductive collagen implant. The study was drafted following the STROBE/PROCESS guidelines. 26
Participant recruitment
A retrospective review of patient data was accessed on 1 February 2024; it included patients from the Prince of Wales Hospital, between 1 June 2022 and 31 July 2023. Data were de-identified and anonymized after extraction, and researchers could not identify individual patients. Verbal consent was obtained by the researcher, witnessed by the clinic assistant/nurse, prior to patients answering the scoring questionnaires.
Inclusion criteria
Patients who underwent acute Achilles tendon repair augmented with a bioinductive collagen implant.
Pre-operative ultrasound confirmation of underlying tendinopathy as reported by a radiologist.
The follow-up period is at least 6 months.
Exclusion criteria
Patients who had undergone recent Achilles interventions within the past 3 months (e.g. PRP injections).
Patients with physical or psychological conditions that hindered adherence to rehabilitation (e.g. lower limb surgery within the past 1 year).
Minors or those mentally incapable of providing consent.
Pregnant individuals.
Individuals with allergies to bovine material.
Intervention
The Achilles repair procedure involved utilizing double-strand Krakow locking sutures. 8 A skin incision of ∼2 cm, the standard mini-open skin incision size used in our hospital, is adequate to inset the bioinductive collagen patch. After adequate repair, the rupture site was augmented with a Bovine Collagen 1 scaffold (Regeneten, Smith and Nephew) placed as an on-lay. The collagen patch was anchored with four soft tissue anchors: two proximal stumps and two distal stumps (Figure 1). All surgeries were performed or directly supervised by a foot and ankle surgeon with over 10 years of orthopedic experience.

Intraoperative photo showing the suturing of the bioinductive collagen scaffold as an on-lay after an Achilles tendon repair with a mini-open paramedial skin incision.
Rehabilitation
All participants followed a standardized rehabilitation protocol used in our hospital for all Achilles tendon repair cases. This regime included two weeks of non-weight-bearing walking with a dorsal splint in plantar flexion, followed by two weeks of partial weight-bearing walking with a 20-degree heel wedge, and then two more weeks with a 10-degree heel wedge. 27 Full weight-bearing walking was initiated at 6 weeks, along with progressive strengthening of the calf muscles.
Follow-up and outcome measures
Participants were followed up as per the usual protocol in the orthopedic outpatient clinic at the Prince of Wales Hospital. Clinical scores were recorded during these visits, and additional assessments were conducted in the sports biomechanics laboratory. Outcome measures were taken at 2 weeks, 6 weeks, 3 months, and 6 months of follow-up. Symptoms were measured using the Foot and Ankle Outcome Score (FAOS) at each follow-up time point, 28 and a more specific Achilles function measure, the Victorian Institute of Sports Assessment – Achilles (VISA-A), 29 was measured at 6 months. In cases of missing data, an intention-to-treat analysis was performed.
Results
Nine participants were found to meet the eligibility criteria for the study, comprising seven males and two females. The average age of the participants was 45, with a range of 18–83. Out of the nine participants, four had a right side rupture, while five had a left side rupture. According to the radiologist, seven participants had mild tendinopathy severity, while two had moderate severity. No participant had a severe tendinopathy condition. The average follow-up time for the study was 348 days, ranging from 207 to 560 days.
There were no cases of re-rupture within 6 months of operation. However, one case of suture abscess was reported, which required a course of oral augmentin and alternate-day nurse dressing; no re-operation was required.
The study showed statistically significant improvement in all areas of foot and ankle outcome score (Table 1). Symptom improvement was observed from immediate post-operation with a p-value of < 0.01. Pain improvement was observed at 6 months from immediate post-operation, with a p-value of 0.003. Activities of daily living improvement were observed at 6 months post-operation, with a p-value of < 0.001. Sporting ability subsection improvement was observed with a p-value of < 0.002. Finally, quality of life subsection improvement was observed at 6 months post-surgery with a p-value of < 0.001 (Figure 2). The VISA-A score also showed progressive improvement and was 51 at 6 months (Figure 3).
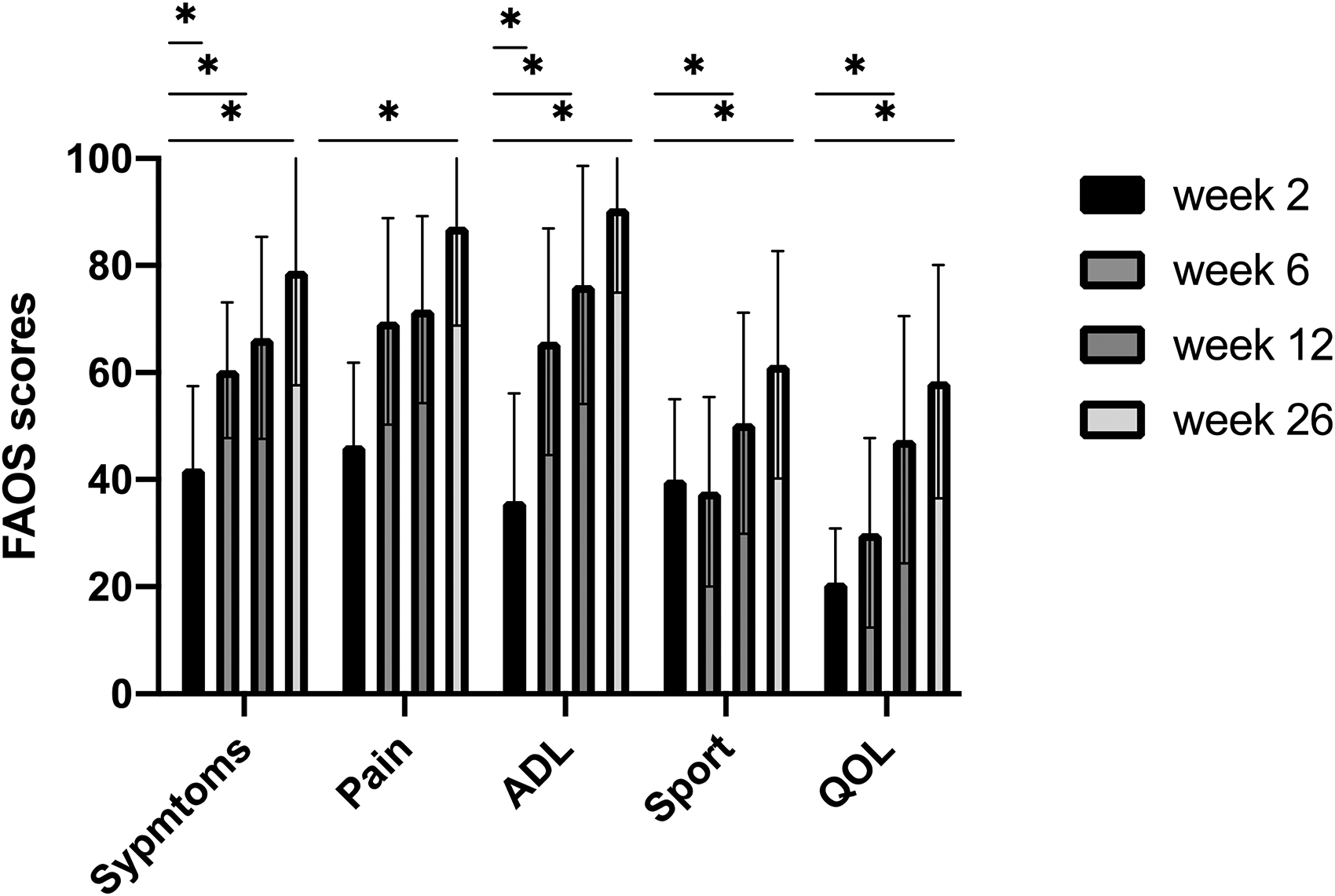
Statistical significant improvements in the foot and ankle outcome scores, * p < 0.05.
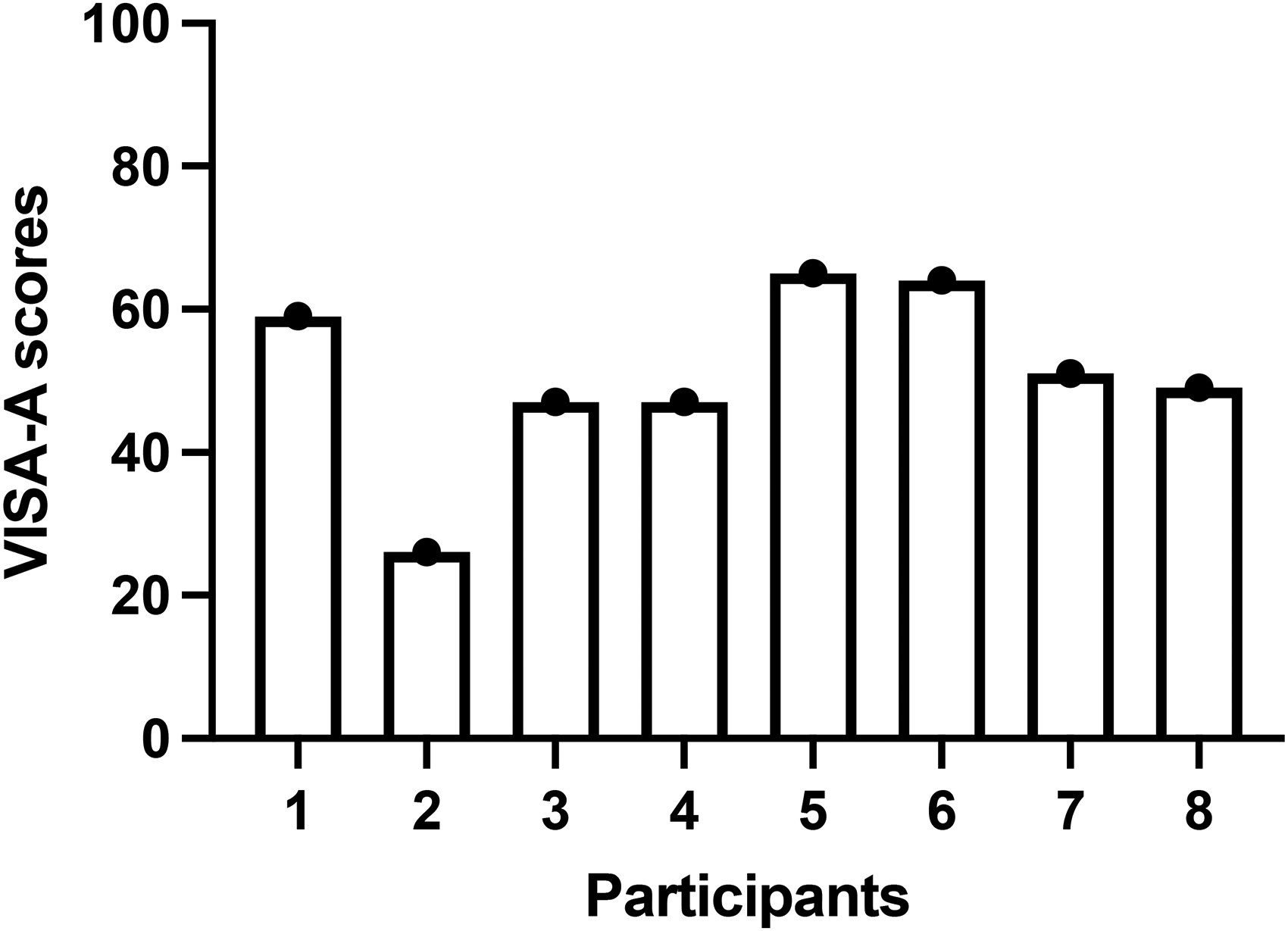
Interval in the Victorian Institute of Sports Assessment – Achilles (VISA-A) at 6 months.
Comparison of foot and ankle outcome scores (FAOSs) at different assessment points.
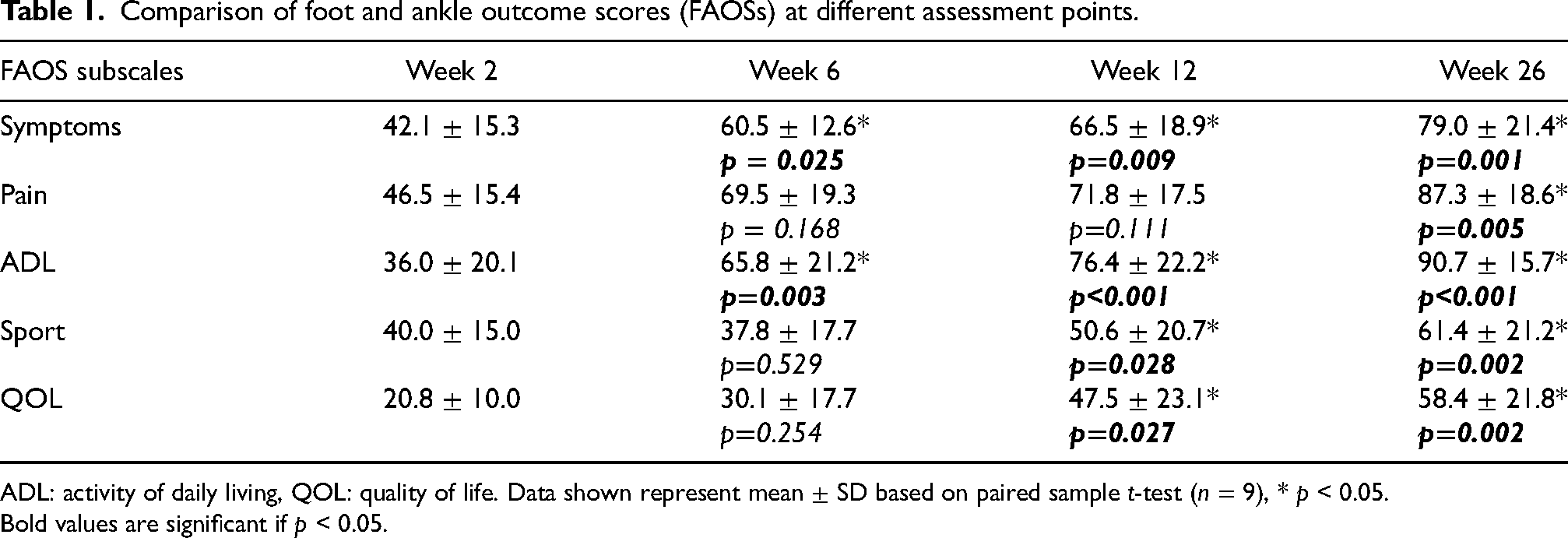
ADL: activity of daily living, QOL: quality of life. Data shown represent mean ± SD based on paired sample t-test (n = 9), * p < 0.05.
Bold values are significant if p < 0.05.
Discussion
The use of Regeneten augmentation in patients with degenerative Achilles tendon rupture has been found to be technically feasible and safe, 24 without any major clinical complications. Although the sample size of this study is small, early re-rupture rates are not seen. However, some reports suggest a re-rupture rate of 2% in the at-risk population of pre-existing tendinopathy, which was targeted in this study.9,10 While solid conclusions cannot be drawn from a case series, this study involved only at-risk individuals and did not have any re-rupture rate.
The surgical procedure has minimal complications, although one patient with a history of poorly controlled diabetes was complicated with a stitch abscess, which required antibiotics. Patients perceived significant improvement in symptoms and function, even though this is a select group of tendinopathy patients complicated with an acute traumatic rupture. However, the group seems to perform similarly to healthy Achilles repair patients.
This study has some limitations, with the limitation of a case series being a major one. Because this is a novel use of the Regeneten implant in the Achilles tendon, the only existing literature are sporadic case reports. Therefore, we believe there is still reason to report a case series; we fully acknowledge that further studies should ideally include a control group in a prospective randomized clinical trial. As a novel treatment, we have included nine consecutive cases in the study and acknowledge that we must interpret the data cautiously. We believe the data generated in this study can be a foundation for future prospective randomized clinical trials on the subject.
The study has shown the effect of an easy-to-follow surgical procedure that may help enhance the healing quality of degenerative Achilles tendon ruptures. While current management ranges from a flexor hallucis longus transfer to a tendon graft,18,19 which may produce good clinical outcomes, it is a more complex surgical procedure. The collagen patch-augmented repair may decrease the need for tendon transfers or turndown flaps and potentially accelerate the healing timeframe on tendons. In our series, the standard rehabilitation for non-tendinopathy complication Achilles rupture repair was used. This may change the “slower rehabilitation” clinical strategy of surgeons who repair the tendon rupture as usual, but adopt a much more conservative rehabilitation regime compared to normal Achilles tendon repair cases without tendinopathy.
Moreover, if augmentation with a collagen scaffold can enhance and accelerate the healing of tendon rupture, it will have significant clinical implications, particularly for tendinopathy complicating “degenerative” ruptures. This will be an interesting future research direction regarding augmentation technologies.
Conclusion
This study presents the first published case series on utilizing a novel bioinductive collagen patch to augment Achilles tendon rupture in the at-risk group of patients with pre-existing tendinopathy. The clinical results are positive and can serve as a valuable foundation for future research in this area.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SKKL and PSHY have been faculty for Smith and Nephew, however, there is no direct funding related to this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.