
Abstract
Background
There is a notable lack of data concerning the morphology of the distal radioulnar joint (DRUJ) in the Chinese population. This study aims to evaluate the normal parameters of the wrist and DRUJ using multiplanar reconstruction (MPR) computed tomography (CT) images in a cohort of Chinese subjects.
Methods
A total of 39 subjects with 42 CT wrist scans, collected between July 2018 and December 2021, were retrospectively selected and processed into MPR images using OsiriX MD software. The assessed parameters included radial height, radial inclination, palmar tilt, ulnar variance, DRUJ angle and sigmoid notch morphology (based on Tolat's cadaveric study).
Results
The wrist parameter results were consistent with those of previous studies. The coronal morphology of the DRUJ was categorized as C-type (50%), Flat-shape type (26%), Ski-slope type (14%), and S-type (10%). The C-type sigmoid notch was the most prevalent morphology, representing 50%.
Conclusion
MPR CT shows strong reliability in assessing wrist and DRUJ parameters. These measurements are clinically relevant for the evaluation and treatment of wrist pathologies and will contribute to future clinical research.
Keywords
Introduction
Wrist pathology is common yet can be challenging to diagnose and manage. Clinical examination and plain wrist radiography remain the standard routine practices. Hence, normal reference values of radiographic indices are important for objective assessment of wrist conditions; therefore, these indices have been extensively documented in the past.1–3
Although the majority of patients with normal radiographs have good prognosis, serious wrist injuries can be left undiagnosed and give rise to chronic pain and long-standing functional impairment.4–6 Furthermore, wrist radiographs generally provide limited measurements in posteroanterior and lateral views, while the transverse plane of distal radioulnar joint (DRUJ) cannot be readily assessed.
Addressing the inherent limitation of plain radiography, computed tomography (CT) scans could provide higher resolution and more accurate anatomical evaluation of wrist & DRUJ anatomy. In 1996, Tolat described the morphological configurations of DRUJ in the transverse and mid-coronal planes from 50 cadaveric wrists. 7 Four types of sigmoid notch were identified, these are Flat-type, Ski-slope type, C-type, and S-type in the transverse plane. With the help of the multiplanar reconstruction (MPR) technique, a consistent and reproducible plane of the wrist joint can be identified. These CT images can be utilized to analyze DRUJ morphology and facilitate the practical study of wrist anatomy. This approach offers a more accessible tool for examining wrist morphology on a larger scale.
The literature indicates that morphological variations in the wrist and distal radioulnar joint (DRUJ) can impact wrist pathology.1,8–11 To the best of our knowledge, local studies have only examined normal dimensions of radiological indices using plain radiographs. 12 Additionally, data on the DRUJ in the Chinese population are limited. Consequently, this study aims to offer a non-invasive and reproducible technique for evaluating the normal radiographic indices of the wrist and DRUJ through MPR CT images.
Materials and methods
Study design and patient selection
All CT scans of wrist performed at our institution between July 2018 and December 2021 were retrospectively reviewed. Inclusion criteria were adult subjects aged 18–75 years of Chinese ethnicity. Exclusion criteria were (1) patients with previous distal radius or ulna fractures, (2) congenital wrist deformities, (3) radiological evidence of wrist or DRUJ arthritis, (4) systemic inflammatory arthritis, and (5) CT scans showing less than 6 cm of radius length.
CT imaging was performed using a standardized protocol with the subject's forearm in maximum supination. Forty-two standardized CT scans met the criteria, including three subjects with bilateral wrist imaging. All CT imaging underwent MPR, with measurements taken in axial, mid-coronal, and sagittal planes using Osirix MD DICOM viewer software.
Measurements
The standardization of radiographic measurements necessitated the establishment of reference planes. We first identified the coronal plane best showing the distal radial shaft. The mid-sagittal plane refers to the longitudinal radial axis in this plane, defined by a line intersecting two points at the midpoint of the radial diaphysis, positioned 3 cm and 6 cm proximal to the lunate facet of the radius. 13 The axial plane was perpendicular to the mid-sagittal plane, at the level where Lister's tubercle is most prominent. The Mid-coronal plane was finally established by connecting two points in the axial plane: one at the midpoint of the sigmoid notch apex and the other bisecting the most dorsal aspect of Lister's tubercle and the volar cortex of the radius (Figure 1).
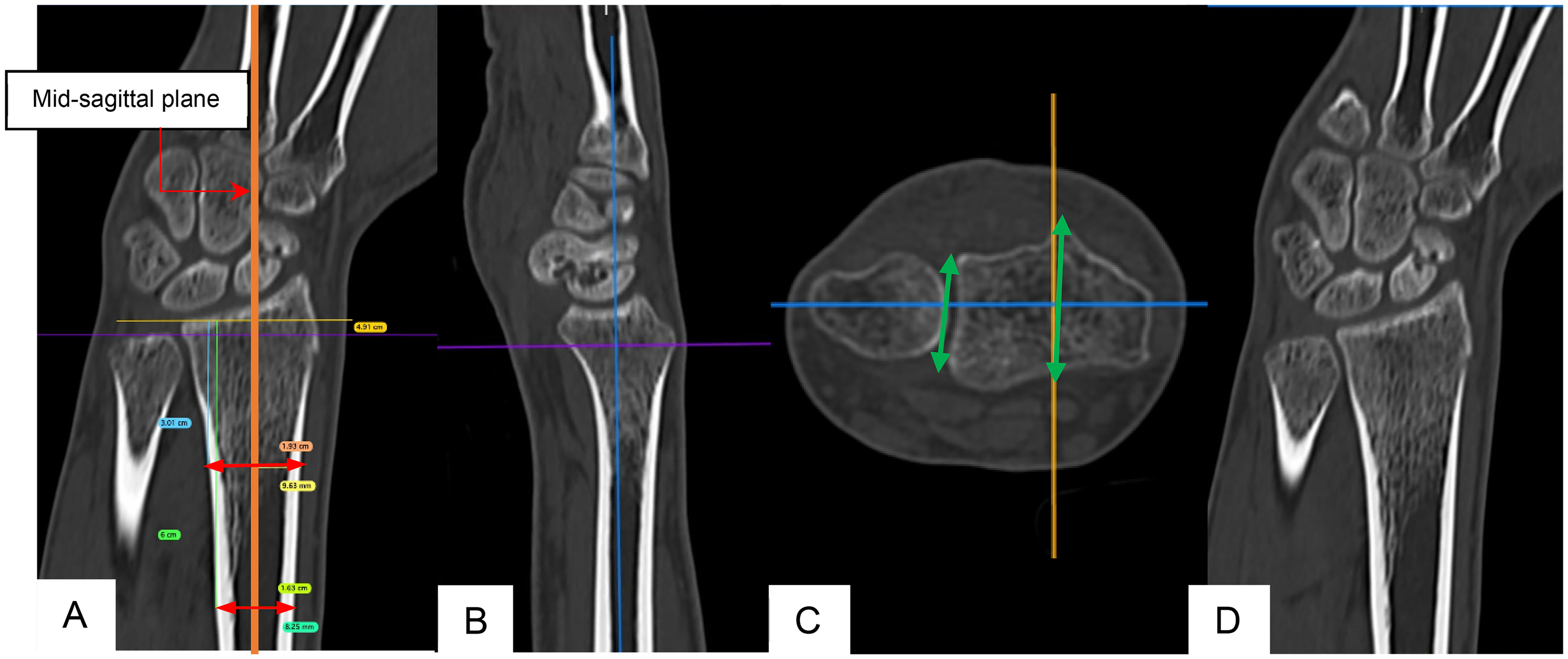
Radiographic examples to define standard planes. (A) The longitudinal axis of radius defines the mid-sagittal plane. (B) Mid-sagittal plane. (C) Mid-axial plane. (D) Mid-coronal plane, derived from the two midpoints in axial plane.
Measurements in the mid-coronal plane included DRUJ angles, DRUJ morphological types, radial height, radial inclination, and ulnar variance. DRUJ angle and morphological types were assessed following Tolat et al. 7 The DRUJ angle was measured between the sigmoid notch articular surface and the ulnar longitudinal axis. Three distinct DRUJ morphological types were identified: Type 1, characterized by parallel alignment between the sigmoid notch and ulnar axis (DRUJ angle −10° to 10°); Type 2, featuring an oblique joint surface with distal angle formation (DRUJ angle >10°); and Type 3 (reverse oblique), exhibiting proximal angle formation with opposite obliquity to Type 2 (DRUJ angle < -10°) (Figure 2).7,14
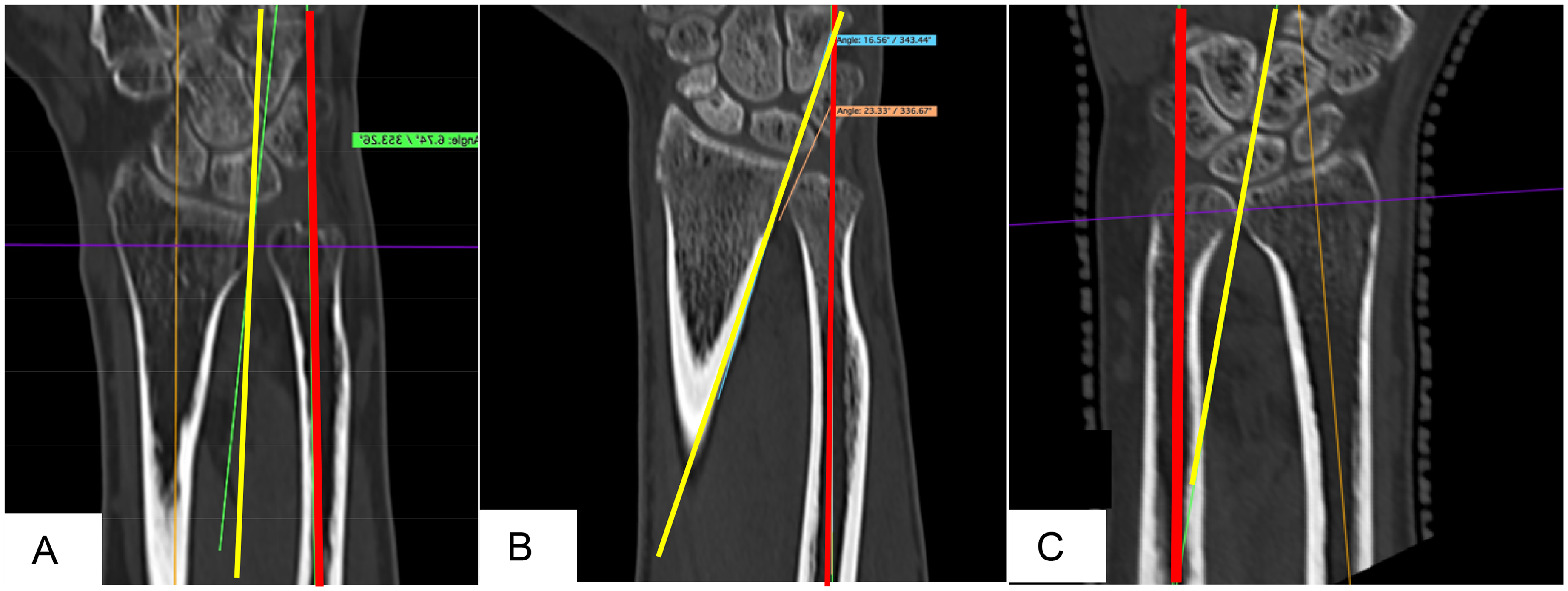
(A) Type I DRUJ, parallel, (B) type II DRUJ, oblique, (C) type III DRUJ, reverse oblique. DRUJ: distal radioulnar joint.
Radial height was quantified as the perpendicular distance between two parallel lines: one through the radial styloid apex and another through the lunate fossa articular surface, both perpendicular to the radial longitudinal axis. 15 Radial inclination was defined as the angle between the perpendicular to the radial longitudinal axis along the distal radius articular surface and a line extending from the radial styloid tip. Ulnar variance was determined using the perpendicular method, which measures the vertical distance between two lines contacting the distal ulnar aspect of the radius and the distal cortical rim of ulna, both drawn perpendicular to the longitudinal axis of radius. (Figure 3). 16
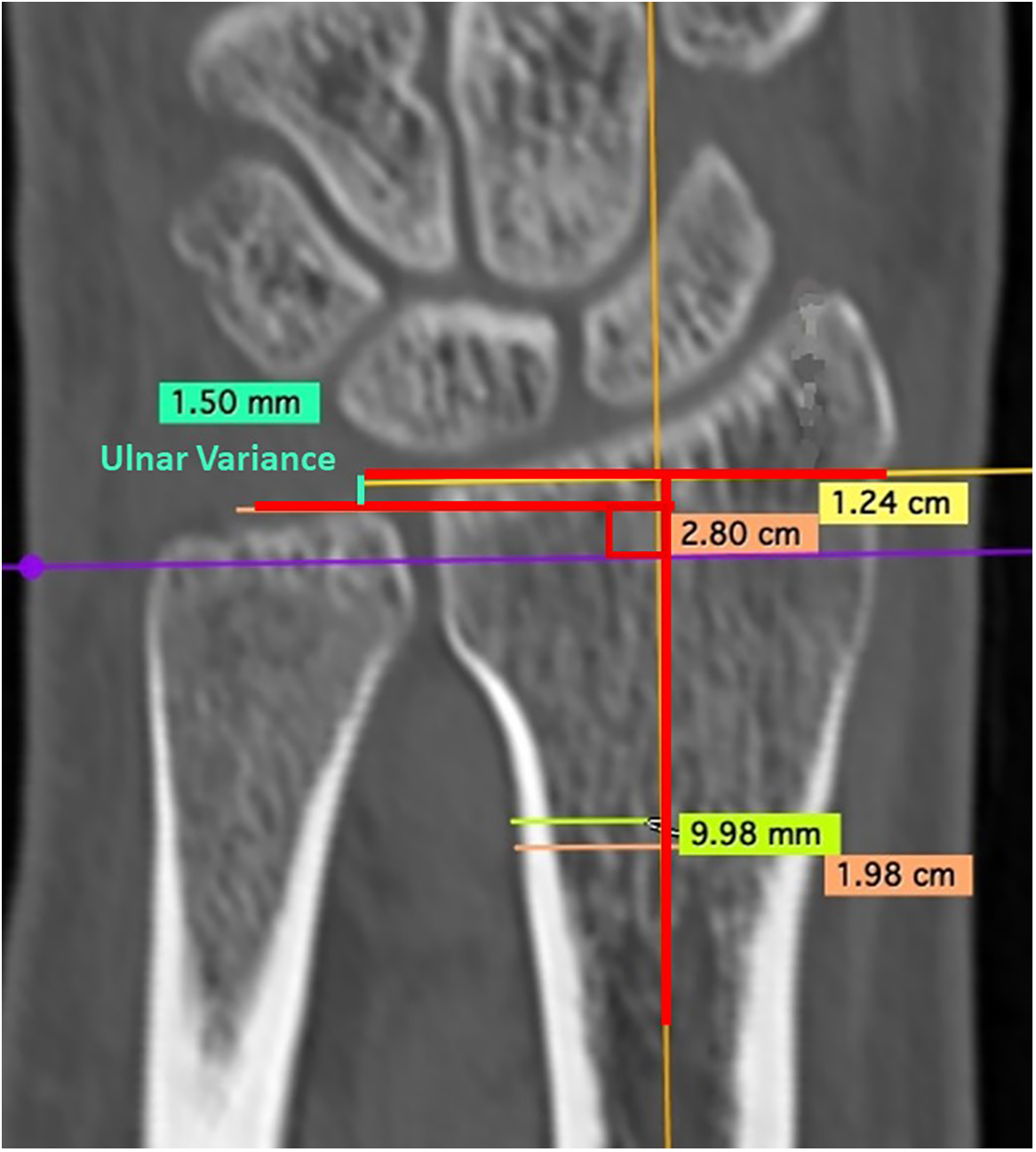
Examples of positive ulnar variance in MPR CT images. Ulnar variance was measured according to the perpendicular method. MPR: multiplanar reconstruction; CT: computed tomography.
In the mid-sagittal plane, volar tilt was measured as the angle between the perpendicular to the radial longitudinal axis and the tangential line along the dorsal-to-palmar radial surface slope.
In the axial plane, sigmoid notch morphology was evaluated at the level where Lister's tubercle is most prominent. Measurement is documented by two independent investigators: a hand consultant surgeon and an orthopedic resident. The sigmoid notch configuration was categorized according to Tolat et al.'s cadaveric study into four distinct patterns: flat-face, ski-slope, C-type, and S-type (Figure 4). 7 To assess intra-observer reliability, measurements were repeated with a minimum interval of 2 weeks. Both intra- and inter-observer reliability were statistically analyzed using Cohen's kappa coefficient (SPSS version 26.0).
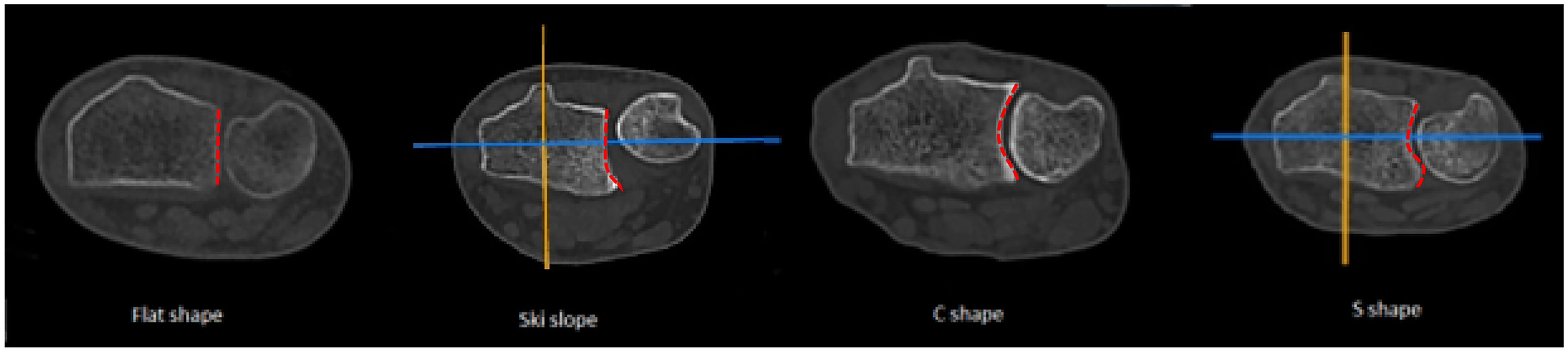
Morphology of sigmoid notch. Flat, Ski-slope, C & S shape.
Results
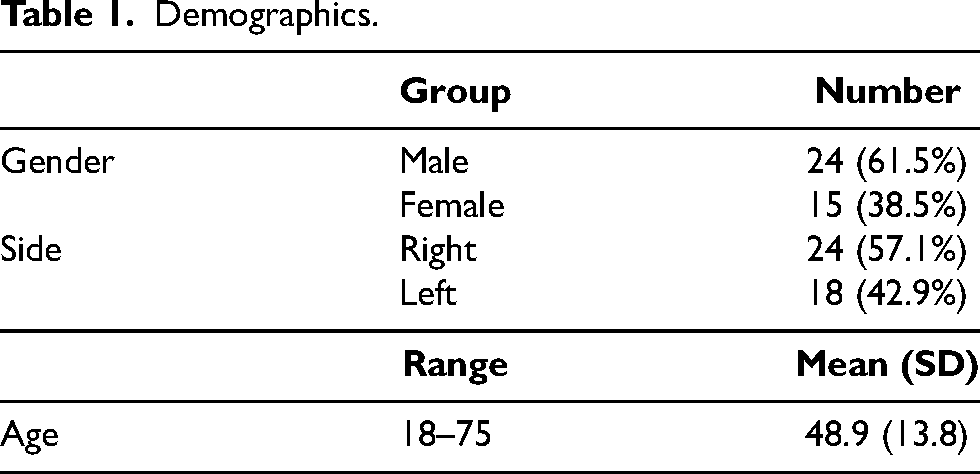
Demographics are presented in Table 1. The study cohort comprised 39 Chinese patients (24 males, 15 females) with 42 wrist CT scans. The distribution included 24 right and 18 left wrists, with a mean age of 48.9 ± 13.8 years.
Demographics.
Quantitative measurements and results are summarized in Tables 2 and 3. Mean radial height was 10.7 ± 2.2 mm, radial inclination 23.7° ± 3.0°, ulnar variance −0.66 ± 1.69 mm, volar tilt 13.5° ± 3.8°, and DRUJ angle 6.4° ± 10.3°. In the mid-coronal plane analysis, DRUJ morphological distribution revealed Type I in 23 cases (55%), Type II in 17 cases (40%), and Type III reverse oblique in 2 cases (5%).
Results.
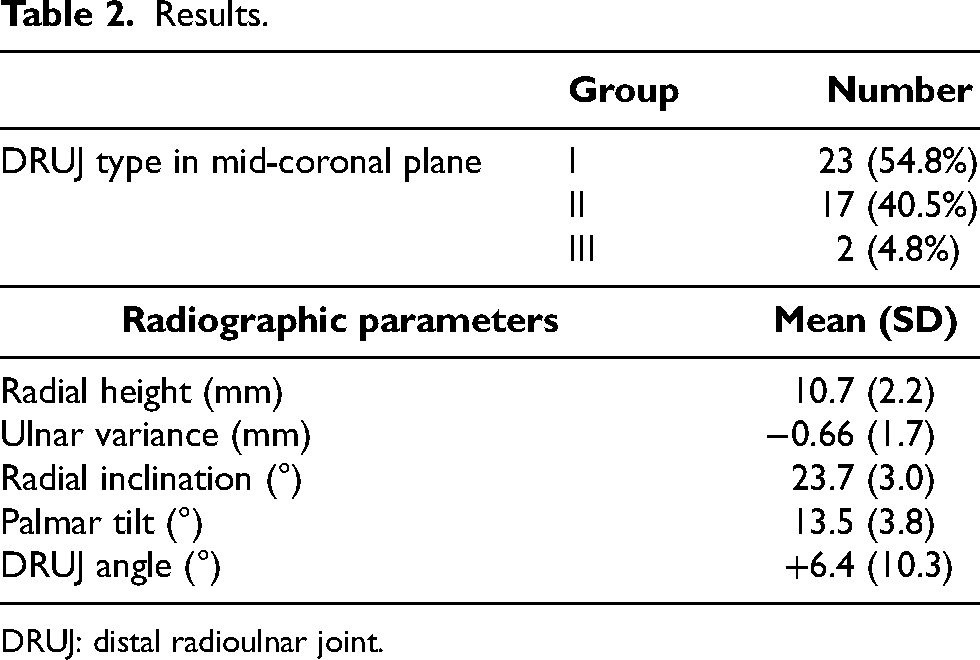
DRUJ: distal radioulnar joint.
Sigmoid notch morphology.
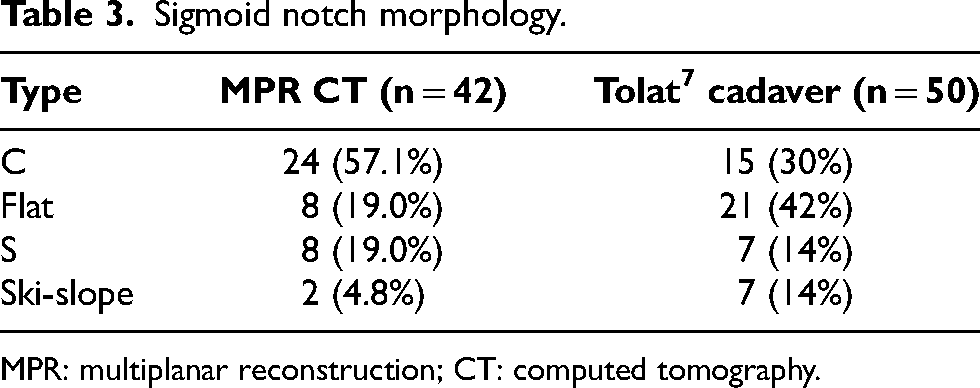
MPR: multiplanar reconstruction; CT: computed tomography.
Axial plane evaluation demonstrated four distinct sigmoid notch morphologies: C-type predominated (50%), followed by flat-shape (26%), ski-slope (14%), and S-type (10%). Reliability analysis of sigmoid notch morphologies in axial plane revealed high concordance, with the intra-observer Cohen's kappa values of 0.92 for the first observer and 0.85 for the second observer, alongside an inter-observer reliability of 0.84. In the three cases with bilateral wrist imaging, sigmoid notch morphology demonstrated symmetry between contralateral sides.
Discussion
The DRUJ constitutes a sophisticated articulation facilitating stable forearm rotation, despite inherent anatomical constraints. The sigmoid notch's radius of curvature approximately doubles that of the ulnar head, resulting in limited osseous congruity.7,17 Stuart's biomechanical analysis demonstrated that bony architecture contributes merely 20% to DRUJ stability, while soft tissue structures including the triangular fibrocartilage complex, interosseous membrane, extensor carpi ulnaris, and pronator quadratus provide the predominant stabilizing force. 18 Disruption of either osseous or soft tissue components can significantly impair wrist biomechanics and function, particularly in cases of distal radius or ulnar styloid fractures.19–21
Analysis of DRUJ and distal radius anatomical parameters in the Chinese population yielded reference values crucial for evaluation and treatment of wrist pathologies. While most radiographic parameters aligned with previous studies, our findings regarding ulnar variance showed notable differences.2,3,12,13,22 Contrary to literature suggesting ulnar plus variance predominance in Chinese adults and slight negative variance in Caucasians, our cohort demonstrated predominantly ulnar minus variance (45% of cases) with a mean of −0.66 mm. 1 This discrepancy may be attributed to forearm positioning during measurement, as supination can cause distal radius migration, decreasing ulnar variance by approximately 1 mm compared to full pronation. 23 Among the 19 cases presenting with negative ulnar variance, 12 exhibited measurements > -2 mm, potentially indicating neutral variance when assessed in full pronation on standard wrist radiographs.
Morphological analysis revealed four distinct sigmoid notch configurations in the axial plane and three DRUJ variants in the coronal plane, consistent with previous studies. 7 Reliable intra- and inter-observer reliabilities for sigmoid notch morphology in the axial plane were demonstrated. While type I DRUJ predominated in the coronal plane, aligning with Western populations, axial plane analysis showed C-type sigmoid notch prevalence (57%) with flat-face configuration comprising only 19% of cases, contrasting with previous cadaveric studies where flat-face type represented 42%. 7 This disparity suggests potential ethnic variations in DRUJ anatomy. The clinical significance of C-type sigmoid notch prevalence could relate to enhanced DRUJ stability, as supported by Tsukuda et al.'s CT analysis demonstrating uniform stress distribution patterns in this configuration. 24
There were some limitations in our study. The retrospective nature of this analysis presents an inherent limitation. Additionally, the restricted sample size precluded meaningful analysis of bilateral anatomical symmetry. The assessment of sigmoid notch morphology relied solely on CT-based osseous anatomy, without accounting for articular cartilage contributions. Previous MRI and cadaveric investigations have demonstrated variable cartilage thickness distribution across the sigmoid notch in the axial plane, with maximal thickness centrally and progressive thinning toward dorsal and volar aspects. 25 Further research exploring the impact of articular cartilage on sigmoid notch morphology would be valuable. We believe that the cartilage thickness is minimal and do not affect the sigmoid notch morphology. Lastly, technical limitations included CT slice thickness parameters (5 mm axial, 3 mm coronal and sagittal planes), which potentially affected the precision of defined anatomical planes.
Conclusion
In conclusion, MPR CT constitutes a non-invasive, efficient, and reproducible modality for comprehensive DRUJ and wrist anatomical assessment. This study establishes normative DRUJ and wrist parameters within the Hong Kong Chinese population, enabling future investigations into the relationship between DRUJ morphological variants and wrist pathologies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics considerations
This study was approved by the institutional review board at our hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.