
Abstract
Thumb carpometacarpal joint (CMCJ) osteoarthritis (OA) is the second most common arthritis of the hand. Surgical treatment options can be variable and there is yet a gold standard choice. With the benefit of being minimally invasive, arthroscopic partial trapeziectomy with suture button suspensionplasty (Mini Tightrope) is now gaining popularity in treating patients with CMCJ OA who have failed conservative treatments. It is thought that this treatment option offers similar functional improvements in patients while avoiding the need for a large wound and potential donor site morbidities as in ligament reconstruction and tendon interposition. In this retrospective study, we are going to review the intermediate-term clinical and radiological outcomes of a series of local patients. Clinical outcomes include visual analog scale pain score, grip strength, pinch strength, and Quick Disabilities of Arm, Shoulder & Hand score before operation and in the latest follow up while radiological outcome of thumb metacarpal subsidence was also evaluated. To our understanding, this is a study regarding the same kind of treatment with the longest follow-up time in Hong Kong.
Keywords
Introduction
Thumb carpometacarpal joint (CMCJ) was first being described as a saddle joint by Fick in 1854 and it allows thumb movement in flexion, extension, adduction, and abduction, which can be combined to form more complex movements such as opposition. Stability of the thumb CMCJ is mainly contributed by its surrounding ligaments, including the palmar ligament, dorsoradial ligament, intermetacarpal ligament, and posterior oblique ligaments. 1 Joint hypermobility is a cause of thumb CMCJ OA, which can be explained by the intrinsic joint configuration and secondary to ligamentous laxity. The minimal bone congruity results in large contact stresses in the joint by limiting the available surface area to effective load transmission while attenuation of the palmar ligament also contributes to joint instability and subsequent OA changes. 2 As a result of its inherent mobility and associated load bearing in pinch, thumb CMCJ is particularly vulnerable to arthritic changes. Thumb CMCJ OA is found to be the second most common arthritis of the hand, affecting 1 in 4 women and 1 in 12 men. 3
Regarding the treatment options for thumb CMCJ OA, conservative measures include activity modification, application of an orthosis, use of nonsteroidal anti-inflammatory drugs, and local corticosteroid injection to joint. On the other hand, there are numerous surgical options, but the reference standard nowadays is still considered to be trapeziectomy with ligament reconstruction and tendon interposition (LRTI) using the flexor carpi radialis (FCR) tendon. Use of other donor sites, such as the abductor pollicis longus tendon or only half of the FCR tendon have also been proposed.
Summary of patients’ demographics.
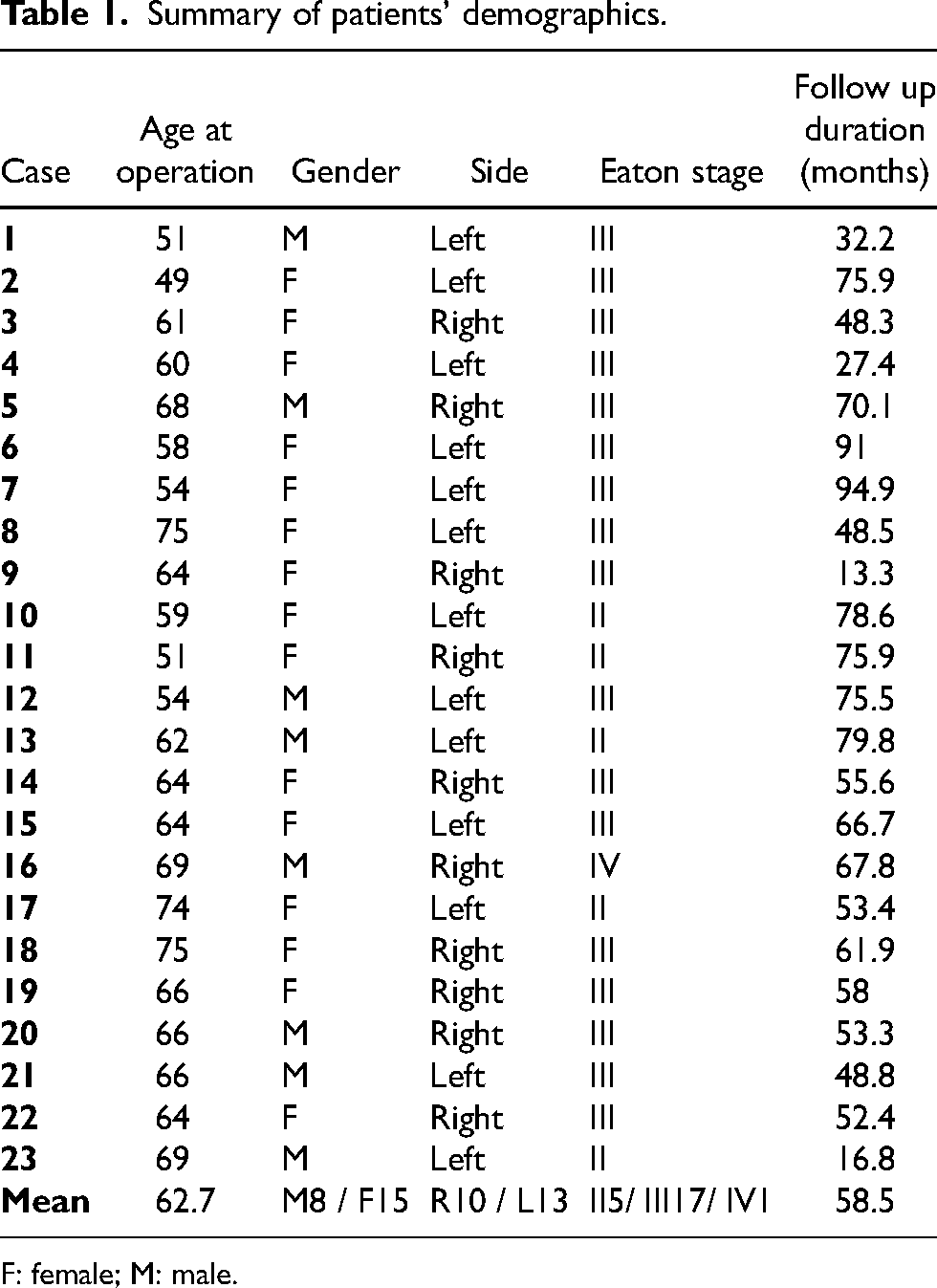
F: female; M: male.
Recently, arthroscopic partial trapeziectomy with suture button suspensionplasty (Mini Tightrope) is gaining its popularity for the treatment of thumb CMCJ OA given its minimally invasive nature. It is thought that this treatment option offers similar, that is, noninferior, postoperative benefits as compared to LRTI. In this study we describe its functional and radiological outcomes in a series of Hong Kong patients.
Summary of patients’ functional outcomes.
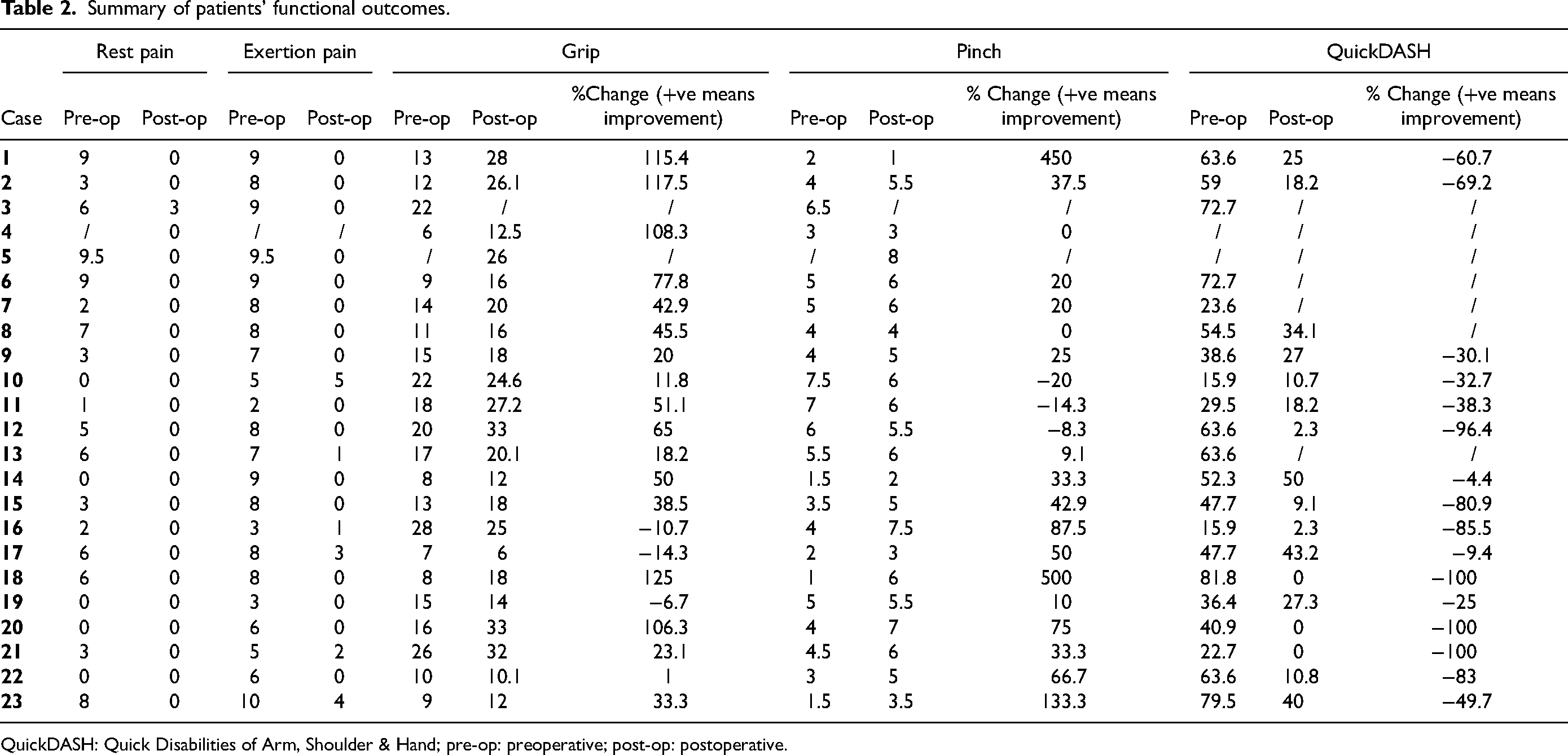
QuickDASH: Quick Disabilities of Arm, Shoulder & Hand; pre-op: preoperative; post-op: postoperative.
Methods
Patients with thumb CMCJ OA who have failed conservative management and were being subsequently treated with arthroscopic partial trapeziectomy with suture button suspensionplasty from 2015 to 2020 in two local hospitals in Hong Kong (Prince of Wales hospital and Alice Ho Miu Ling Nethersole Hospital) were retrospectively reviewed. Inclusion criteria includes (1) CMCJ OA in Eaton stage 2 or above; (2) operation done between 1 January 2015 and 31 December 2020; (3) failed conservative management with a combination of nonsteroidal anti-inflammatory drugs, application of an orthosis, and/or local corticosteroid injection to joint. Patients who had pre-existing regional trauma or injury, additional reconstructive surgical treatment of non-CMCJ arthritis, inflammatory arthritis, major unrelated comorbidity (e.g. end-stage malignancy) and those with follow up less than 1 year were excluded from our study.
Demographic data of all eligible patients were identified and retrieved from the Clinical Management System (CMS). Functional outcomes, including visual analog scale (VAS) pain score, grip strength, pinch strength, and Quick Disabilities of Arm, Shoulder & Hand score (QuickDASH) before operation and in the last follow up (up to 2023) were assessed by occupational therapists and data was obtained from CMS. Radiological outcome of thumb metacarpal subsidence was evaluated. Radiological outcome of thumb metacarpal subsidence was monitored by measuring the trapezial space (TS) to proximal phalanx (PP) ratio on standard posteroanterior view of hand x-ray first taken immediately after operation, 1 year after operation and 5 years after operation for those patients with longer duration of follow up. TS was measured from the mid-point of first metacarpal base to that of the distal margin of trapezium while the length of PP was measured from the mid-point of PP base to that of its distal articular surface (Figure 1). Using the TS to PP ratio rather than the absolute value of TS is more precise in monitoring the degree of thumb metacarpal subsidence as it eliminates errors arising from any rotation while the x-ray was taken. Data analysis was conducted by SPSS system (version 26). The p value <0.05 was considered to be statistically significant. Ethical approval was obtained from Joint CUHK-NTEC CREC Ethics committee, with the reference number of CREC 2020.566.

Measurement of the trapezial space (TS) and long axis of proximal phalanx (PP). TS/PP ratio is used to monitor radiological subsidence of thumb metacarpal.
Summary of patients’ radiological outcomes.
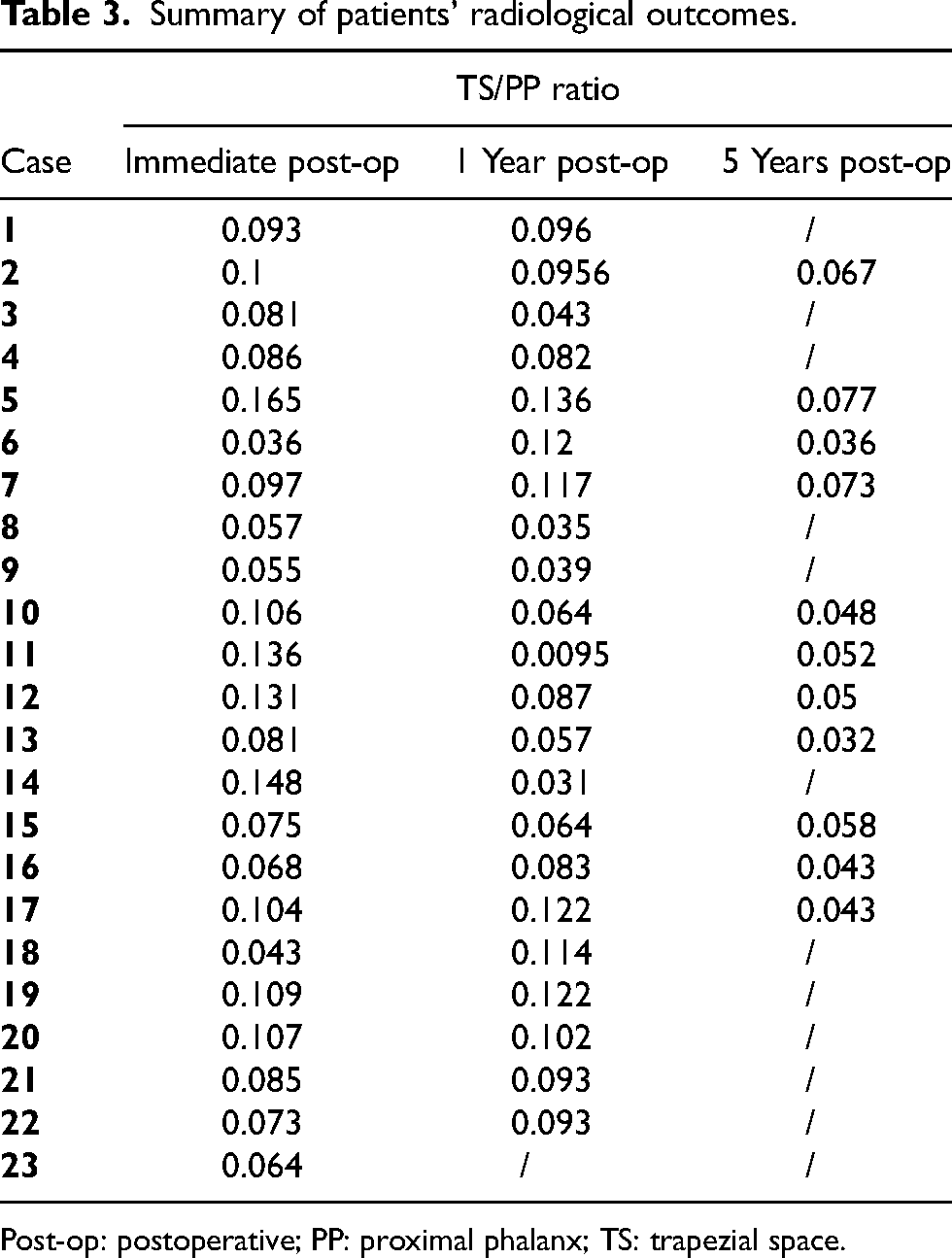
Post-op: postoperative; PP: proximal phalanx; TS: trapezial space.
Results
From 1 January 2015 and 31 December 2020, 23 thumbs in 21 patients with thumb CMCJ OA were recruited. Seven were male and 14 were female patients with a mean age of 63 years old (range from 49 to 75 years old). The majority of our patients were in Eaton stage III (stage II: 5, stage III: 17, stage IV: 1 case, respectively) at the time of operation (Table 1). Before the operation, all patients demonstrated tenderness over thumb CMCJ and hyperextension stress test was positive during physical examination.
Summary of outcomes analysis.
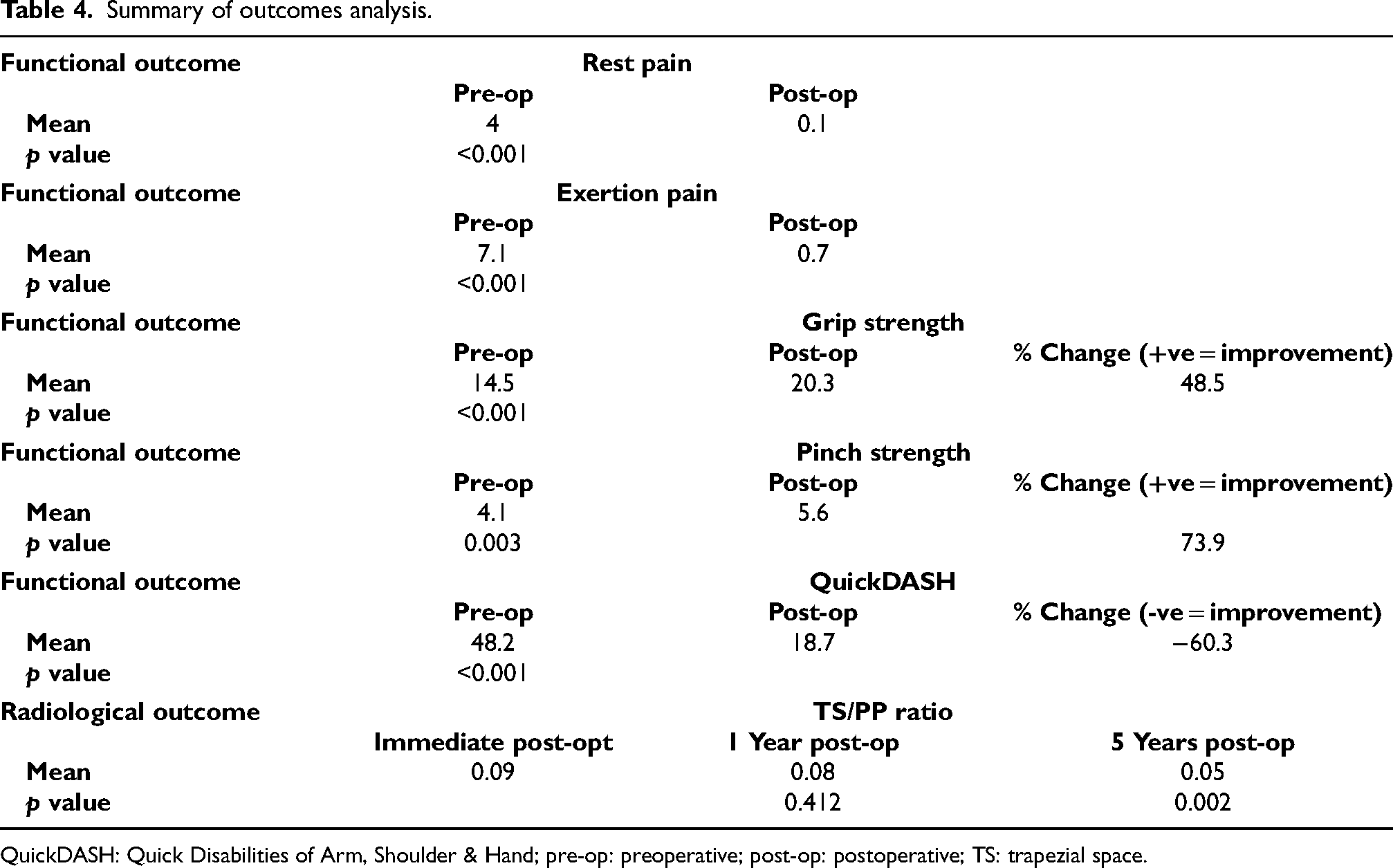
QuickDASH: Quick Disabilities of Arm, Shoulder & Hand; pre-op: preoperative; post-op: postoperative; TS: trapezial space.
All surgeries were performed by hand surgeons in two hospitals under either local, plexus, or general anesthesia (local anesthesia: 12, plexus anesthesia: 7, general anesthesia: 4 cases, respectively). The patient was in supine position, and the operated arm was put on a hand table. The operated arm was prepared and draped from the hand to the upper arm level. The operated arm of the patient was placed on the metal base plate of the sterilizable wrist traction Tower (ConMed Linvatec Corp., Goleta, CA), with shoulder abducted at 80°, elbow flexed at 90°, and forearm in supinated rotation. The thumb was suspended by a single nylon Chinese finger trap with 8lbs of vertical traction was sufficient to distract the CMCJ. Other fingers were warped around the traction tower and padded with padding. CMCJ arthroscopy was performed with 1.9 mm arthroscope via 1R and 1U portals. The position of 1U portal could be identified by palpating the radial border of the second metacarpal and ulnar border of the thumb metacarpal from its shaft to the base, the confluence of the second and thumb metacarpal base pinpoints the location of IU portal. 1R portal location could be located by releasing the thumb from traction, passively extending and adducting the thumb, the radial base of the metacarpal became prominent and the 1R portal was palpable just proximal to the prominence. And 2% lignocaine with 1:200,000 adrenaline was injected through a 25-G needle to the portal sites, to the subcutaneous layer, and to the capsule only to provide portal site local anesthesia and minimize portal site bleeding. Transverse skin incision in line with the skin crease was created over the IU portal site to have better scar healing while vertical skin incision for IR portal in order to incorporate the skin incision for Mini Tightrope placement. The tip of a curved mosquito hemostat was used to gently dilate the portal site until the joint capsule is perforated. An arthroscopic cannula with blunt ended trocar was gently placed though the portal. After removing the trocar, the cannula was then connected by long tubing to a 3-litre saline bag hanged at 1.5 m above to provide gravity driven inflow to the joint. Outflow could be made with an 18-G needle at the thenar portal, which was perpendicular to the 1U portal, through the thenar muscle bulk.

Arthroscopic partial trapeziectomy of 3 to 4 mm was performed at the 1R and 1U portals.
Partial trapeziectomy of 3 to 4 mm was then done by 2.9 mm burr followed by 3.5 mm burr using 1R and 1U portal interchangeably to remove the damaged cartilage and denuded subchondral bone on the distal articular surface of trapezium (Figure 2). The dorsoulnar osteophyte over trapezium was removed as it can block the reduction of proximal phalanx base back into position. Any intra-articular loose body was removed by small joint arthroscopic grasper. The partial trapeziectomy was completed when there was subchondral bleeding and the depth of bone resection is roughly the diameter of 3.5 mm burr. Subchondral bleeding allows hematoma formation, which can help prevent subsidence of the first metacarpal.
After the partial trapeziectomy was finished, the operated arm was released from the traction tower and placed on the hand table. 1R portal site was slightly enlarged distally with radial side of proximal phalanx base bone was exposed. And 1.1 mm specially designed tapered guide pin from the Arthrex Mini TightRope kit (Arthrex, Naples, NL) was inserted from radial side of first metacarpal base to proximal one-third of index finger metacarpal shaft under x-ray guidance. Oblique view with thumb PP and index finger metacarpal overlapped helped assess the position inside the medullary part of two bone to prevent eccentric placement of the bone tunnel that could cause iatrogenic bone fracture. Stab incision was made over proximal second metacarpal shaft and deepened by blunt dissection of the dorsal interosseous muscle with extensor tendon protected. The FibreWire loop of the Arthrex Mini TightRope system (Arthrex, Naples, NL) was passed through the bone tunnels of thumb PP base and index finger metacarpal (Figure 3). The Endobutton on the side of thumb PP base should be flushed with the cortical surface to ensure secure cortical fixation. The FibreWire loop on the index finger metacarapal side was cut open. Another Endobutton was threaded through the two limbs of FibreWire loop and docked onto the cortical surface of index metacarpal. A plain gauze row was placed inside the first webspace to prevent over-tightening the FibreWire loop while placing the secure knot (Figure 4). Before closing the wound, we used the fluoroscopy to assess the proper placement of the Endobuttons (Figure 5). All patients were given a Plaster of Paris thumb spica slab after the operation and discharged on same day. The slab was then being changed to a thermoplastic thumb spica splint upon follow up.

Mini TightRope was inserted from base of first metacarpal to proximal third of second metacarpal.

A plain gauze roll was placed inside the first webspace to prevent over-tightening the FibreWire loop while placing the secure knot.
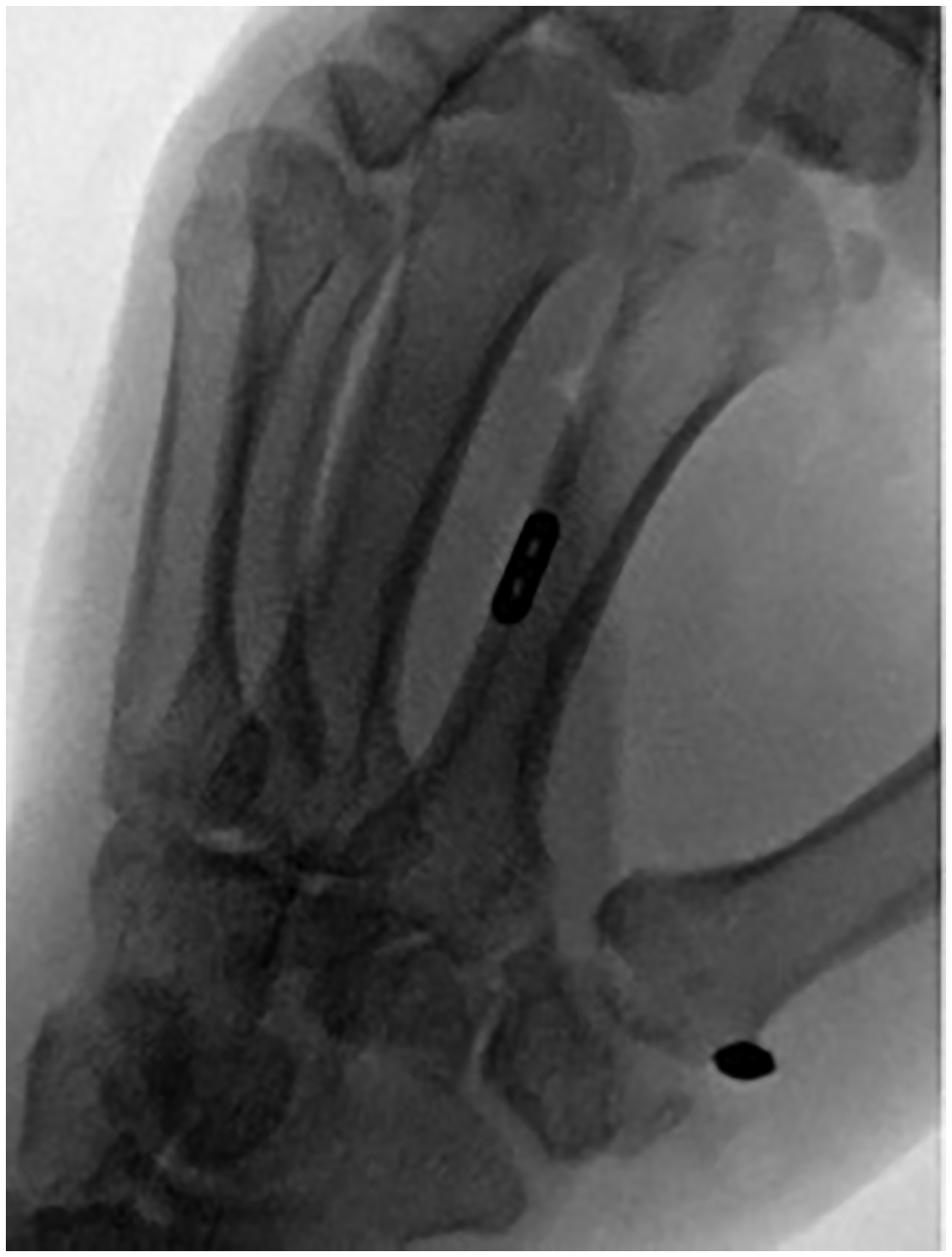
Positions of the endobuttons were confirmed with fluoroscopy.
The mean length of follow up was 58.5 months (range 13.3–94.9 months). Twenty-three cases were included for clinical and radiological outcomes analysisa (Table 2 and Table 3). All patients showed no resting pain in the last follow up except one (27 months after operation) reporting a resting pain VAS score of 3/10. Exertional pain reduced from a mean score 7/10 before operation to 1/10 after operation in the latest follow up (p < 0.001). Mean grip strength improved from 14.5 to 20.3kgf (p < 0.001) while mean pinch strength increased from 4.1 to 5.6 kg after operation (p = 0.003). Mean percentage improvement in grip and pinch strength after operation were 48.5% and 73.9%, respectively. All patients demonstrated improvement in QuickDASH score. The mean QuickDASH score improved from 48.2 to 18.7 (p < 0.001) and the mean percentage improvement was 60.3%. The mean radiological TS to PP ratio on the first x-ray taken after operation was 0.09 while that 1 year after operation was 0.08 (p = 0.412), that is, no statistically radiological subsidence of first metacarpal. However for the 11 patients with longer duration of follow up, the mean radiological TS to PP ratio at 5 years after operation was 0.05, comparing with the images taken immediately and 1 year after operation, there is statistically radiological subsidence of the first metacarpal (p = 0.002) (Table 4).
One complication occurred in our series involving skin impingement over the Endobutton on first metacarpal which required removal.
Discussion
Thumb CMCJ OA can be a debilitating condition to patients as many activities of our daily living require the use of this joint and the presence of pain with or without impaired range of motion can affect their function. For those patients who failed conservative treatments, many surgical options have been described in literatures but none showing superiority over another. 2 Aim of the surgery firstly is to remove the synovitis and osteophytes of the joint and secondary is to prevent the subsidence of thumb metacarpal into the trapezial space after resection. The method of arthroscopic hemitrapeziectomy in combination with suture button suspensionplasty was first described by Cox et al. in 2010. 4 The Arthrex Mini TightRope® system used in that paper was the first generation device with a 2.7 mm drill for bone tunnel opening and a larger 4-hole cortical endobutton for the second metacarpal, which had iatrogenic metacarpal fracture reported in subsequent literatures. 5 On the contrary, we used the second generation device in our series with 1.1 mm guidewire and a 2-hole cortical endobutton. Besides metacarpal fractures, other possible complications related to the Arthrex Mini TightRope® system include infection, injury to surrounding structures (e.g. tendons and nerves), skin impingement, etc., which may require re-operation as in one of our patients. In order to minimize the risks of these potential complications, we suggested that good soft tissue exploration before inserting the guide pin and endobutton should be performed during operation and position of the endobutton should ideally be placed on the side of the metacarpal bone and to be confirmed with intraoperative fluoroscopy. Soft tissue coverage of the endobutton upon wound closure may also help reduce the chance of skin impingement.
In order to achieve a higher successful rate with technique, proper tensioning of the Arthrex Mini TightRope® system is the key. As under-tension may lead to earlier subsidence of thumb metacarpal into the post-trapeziectomy space while over-tension may cause impingement of the thumb and index finger metacarpal bases, limiting thumb abduction.
There are several limitations in our study. First of all, the way to ensure proper tensioning of the Arthrex Mini TightRope® system was not well documented in the operation record and there is no standard method to quantify the degree of tension. Secondly, the amount of radiological subsidence of thumb metacarpal can be affected by nonstandard hand positioning during x-ray assessment. We tried to eliminate this error by using the TS to PP ratio but not measuring the absolute height of the TS alone as its value change considerably with slight change in the position of the x-ray beam and the PP length is relatively constant on different views. Besides, how much subsidence is considered to be clinically significant would also need further investigation as with regard to published articles, some studies found radiological subsidence have clinical impacts on functional outcomes 6 while some found no such correlation. 7 In our review, although there is statistically significant radiological subsidence at 5 years after operation, it did not affect patients’ functional outcomes. Thirdly, the nonstandardized rehabilitation plan for our patients. The duration of thumb spica splint used after operation varied from 2 to 14 weeks in our study and the duration of immobilization may affect the occurrence of postoperative pain, stiffness, or subsidence of thumb metacarpal. Lastly, as this is a retrospective study, some documentation of the outcomes were missing as some old medical records were only available in hard copies and could not be retrieved at the time the manuscript was written. As a result, in order to further evaluate the pros and cons of this relatively new technique, a well-designed prospective randomized controlled trial comparing it to the gold standard technique of LRTI may be warranted.
Conclusion
This is the first local study in Hong Kong to evaluate the long-term outcomes of arthroscopic partial trapeziectomy with suture button suspensionplasty for the treatment of thumb CMCJ OA with a relatively long follow-up period of more than 4 years. Our study demonstrated promising result with improvement in pain, grip strength, and QuickDASH score years after operation without statistically significant subsidence of first metacarpal. It serves as a reliable treatment in this disease entity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Obtained from Joint CUHK-NTEC CREC Ethics committee, with the reference number of CREC 2020.566.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.