
Abstract
Introduction
Osteoarthritis secondary to the developmental dysplasia of the hip (DDH) affects adults in early working age, mostly women. Surgeons aim at the development of the techniques for total hip replacement in these difficult cases. The most challenging step is the placement of an acetabular component. In some studies, it has been proposed to place it the primary (anatomical) acetabular socket.1–3 The acetabular component insertion in the primary or secondary socket according to the surgeon's preference is also mentioned. 4 A few authors advise to place the acetabular component into the secondary acetabular socket in severe cases of DDH.5,6 The aim of our study was to evaluate long-term outcome in hip osteoarthritis patients secondary to DDH with the placement of the acetabular component of endoprostheses both the primary and secondary sockets.
Patients and methods
This is a retrospective study that was registered and approved by the local Ethics Committee (reference number 28/2021/1).
The study included 103 primary total hip arthroplasties in 84 patients with hip osteoarthritis secondary to DDH from November 2008 to December 2011. Nineteen of the patients had bilateral total hip arthroplasties (THA). The right hip was operated on in 52 cases, and the left ‒ in 51 cases. During the follow-up period 4 patients with 4 hips were lost. Ten patients with 10 hips were revised. There were 70 patients (89 hips) in the latest clinical and radiological follow-up (Figure 1).
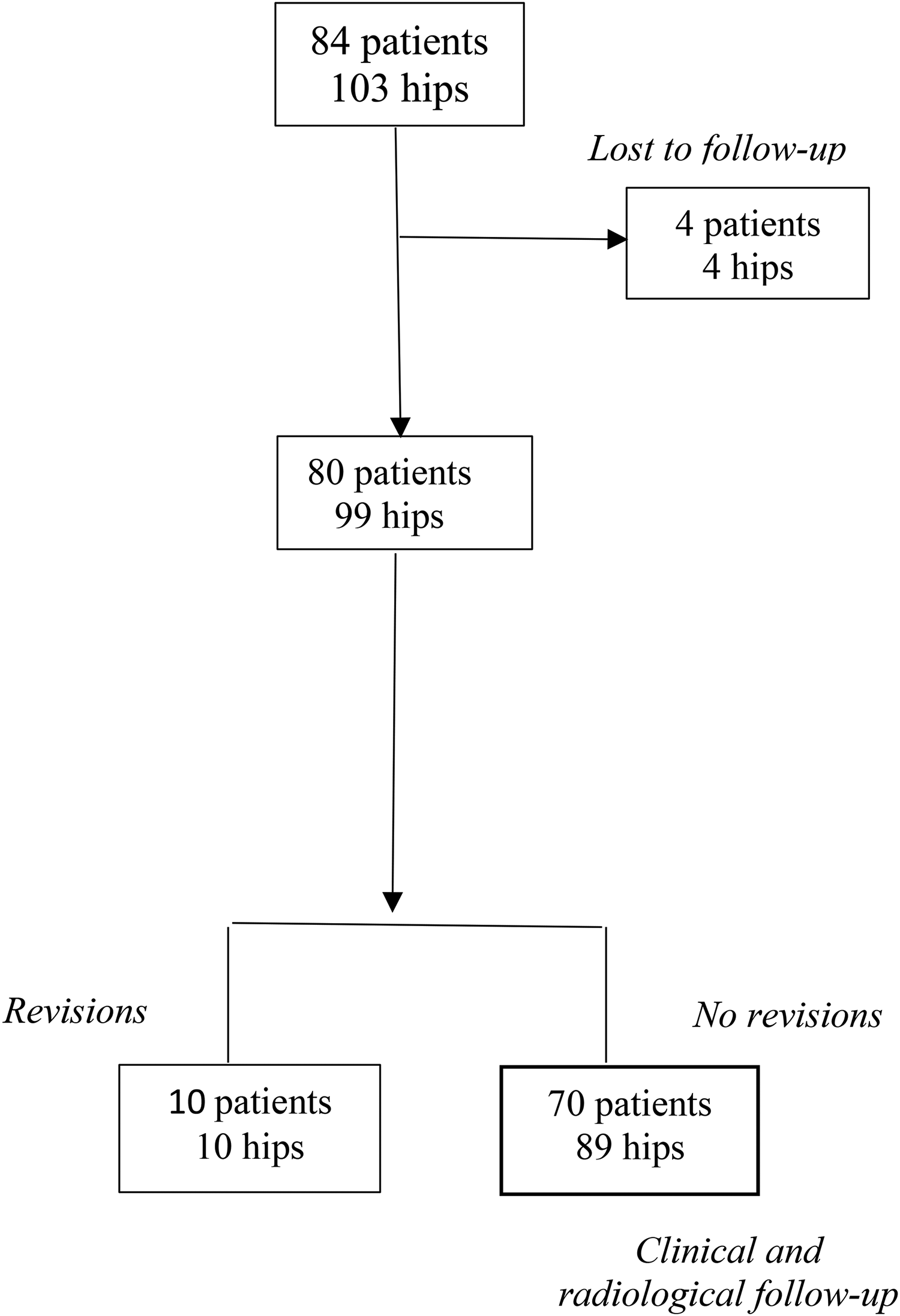
Flow chart of the study participants.
Fifty-six females and 14 males were included in the study. The mean age of the patients in the time of the surgery was 44.4 (20˗78) years. The patients were divided into two groups: group A with the acetabular component placed in the primary acetabular socket, and the group B ̶ in the secondary acetabular socket. Crowe classification was used to distribute the patients in the groups according to the grade of DDH. 7 The primary indications for surgery were severe hip pain and considerable functional impairment.
For radiological evaluation, an anteroposterior (AP) pelvic radiograph and an axial views of the involved hip were obtained to evaluate the acetabular bone stock and the predicted acetabular component coverage, size and position. Preoperative planning was performed by 6 senior orthopedic surgeons who operated on their respective patients by using AGFA digital software preoperative planning tools. The reference point was set to be the hip joints’ rotation center. The rotation center of the hip joint was defined as the center of the femoral head before the surgery and the center of the endoprosthesis head after the surgery. If in the preoperative planning the deviation of rotation center cranially from the anatomical hip center in the AP radiograph was less than 10 mm, we considered the insertion of the acetabular component in the primary socket, if deviation was more than 10 mm ‒ in the secondary socket. 8 The center edge angle characterized the coverage of the acetabular component. The postoperative center edge angle in this study was defined as the angle between a vertical line drawn from the center of the head of the endoprosthesis and the line connecting the center of the head of the endoprosthesis and the lateral edge of the acetabulum. The coverage was considered sufficient if the center edge angle in the AP radiograph was more than 17°. If the center edge angle was less than 17°, the coverage was considered not sufficient and it could be a reason for earlier loosening of the acetabular component. 9
The radiographic examinations were performed on the 3rd postoperative day, 3 months, 1, 2, 5, and 10 years after the surgery.
The offset in this study was defined as the distance between the center of the femoral head of the endoprosthesis and the lateral edge of the greater trochanter.
All preoperative and postoperative radiograph measurements were performed by using orthopedic computer software AGFA Orthopaedic Tools. The postoperative radiological measurements and values are shown in Figure 2.
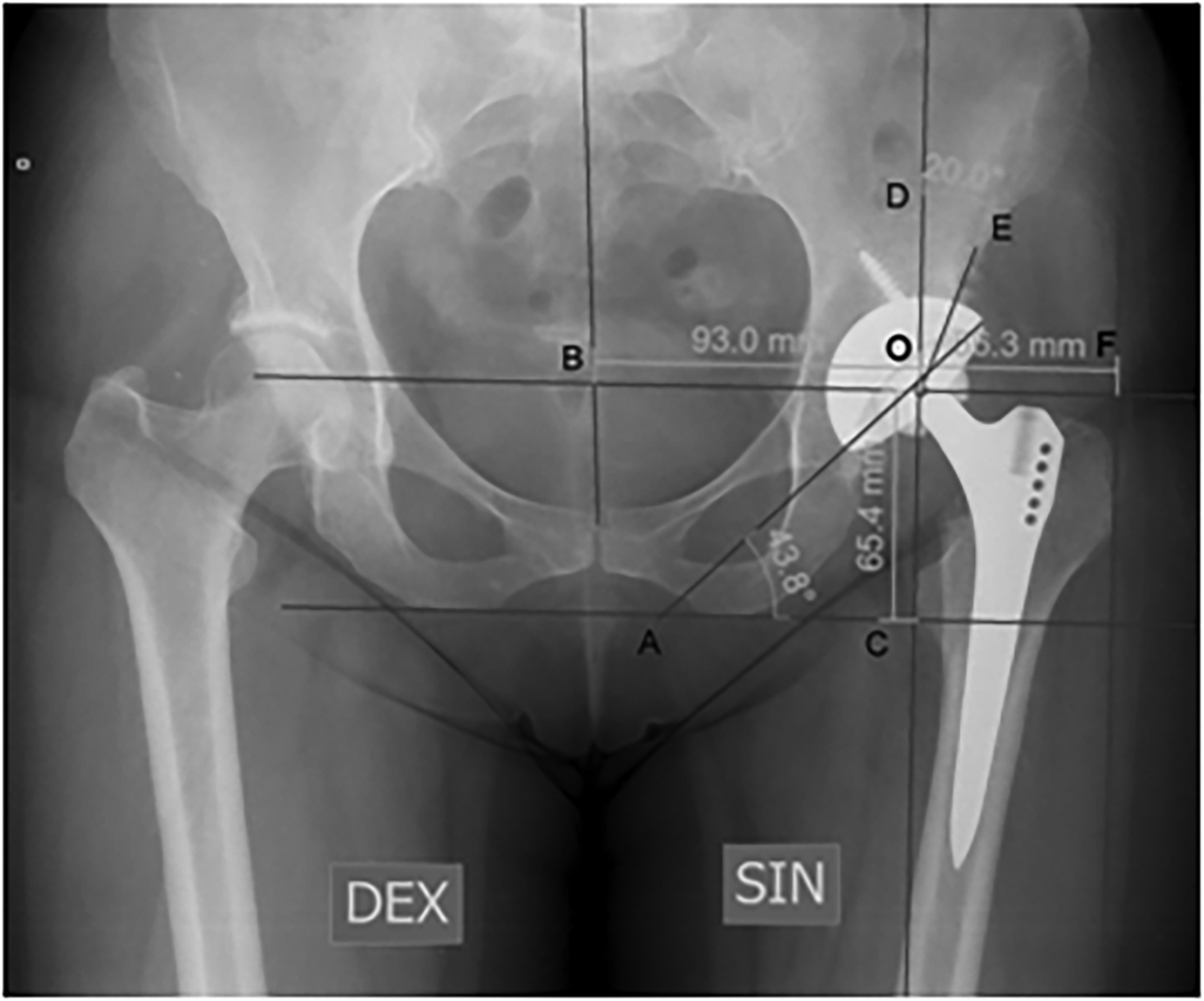
Postoperative digital radiographic measurements on the anteroposterior pelvic radiograph. The acetabular component inclination angle AOC is formed between AO and CO lines; the vertical location of the rotation center is at the end of CO line; the horizontal location of the rotation center is located on the end of BO line; the offset is located in the end of FO line; the center edge angle is formed between DO and OE lines.
All patients were operated on by 6 senior arthroplasty surgeons using anterior or anterolateral approach (90 cases) and posterior approach (13 cases). Cementless fixation was used for all endoprostheses. The average acetabular component size was 52.95 (range: 46 ̶ 64) mm.
In patients with Crowe grade I DDH acetabular component was inserted in the primary socket, in severe DDH (Crowe grades II and III) the decision to place acetabular component in the primary or secondary socket depended on the possibility to achieve adequate bone coverage of the acetabular component. In our study patients with Crowe grade IV DDH had not sufficient bone stock, so more radical surgery was done, including tenotomies of the abductors and adductors, to ensure placement of acetabular component in the primary socket.
All patients were administered antibiotic prophylaxis intravenously using 1 g of Cefazolin before the surgery. In cases where surgery was estimated to last longer than two hours, 1 g of Cefazolin was given during the surgery. Surgery was performed under spinal or epidural anesthesia.
All 70 patients’ assessment before the hip replacement was performed by using the Merle d'Aubigné and Postel score (evaluation of pain, mobility and function). According to this score, outcomes were graded as excellent 17˗18, good 12˗16, fair 6˗11, and unsatisfactory 0˗5 score. 10 An evaluation was performed before the surgery, after 1 year and 10 years after the operation. In patients with bilateral osteoarthritis, we evaluated only the effect of the operated leg.
Analysis of radiographs of the pelvis in two planes was performed to assess the placement of the acetabular component in the primary or secondary socket and to state the causes of revision operations. Radiological evaluation included: the offset and the center edge angle preoperatively and postoperatively, and the acetabular component inclination angle postoperatively.
Endoprosthesis survival rates were analyzed based on our hospital's arthroplasties register data. All patients had given written informed consent to participate in the study.
Group A patients with Crowe grades I and II after the operation walked 4 weeks on crutches, with Crowe grades III and IV – 4˗6 weeks on crutches; group B patients with Crowe grades II and III – 4 weeks on crutches, subsequently full weight bearing was allowed. Physiotherapy included strengthening of abductor and quadriceps muscles.
Follow-up duration was defined from the date of the operation to the date of the last follow-up.
Demographic and surgical variables were expressed as mean, radiographic measurements and clinical scores ̶ as mean and standard deviation. To compare Merle d'Aubigne and Postel scores in two groups before the operation, in 1 year and 10 years follow-up, Mann-Whitney non-parametric test was used. Significance was set at p < 0.05. Kaplan–Meier analysis for implant survival rates was used. The statistical analysis was performed with SPSS program version 25.0.
Results
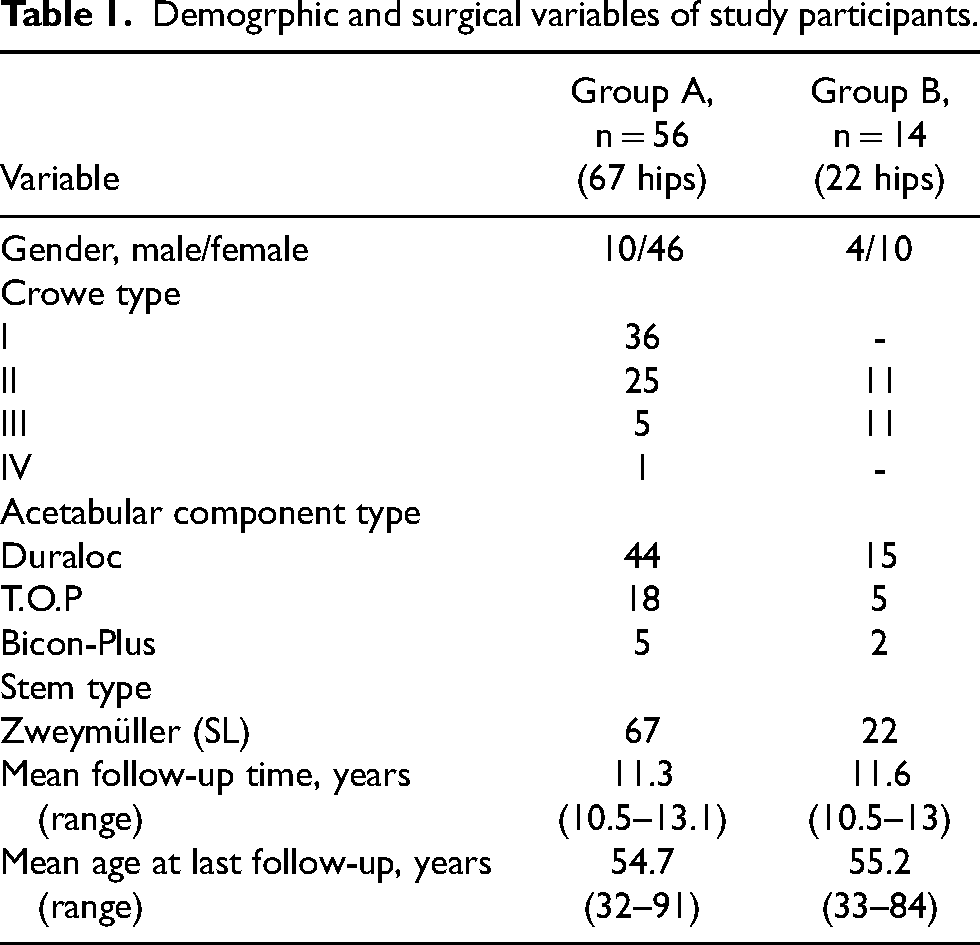
The demographic and surgical variables of the study participants are shown in Table 1.
Demogrphic and surgical variables of study participants.
Ten hips were revised. The causes for revision after the placement of acetabular component in the primary socket were: aseptic loosening n = 5 (2 exchanges of acetabular component: Crowe grade I – 1 hip, Crowe grade IV – 1 hip, 3 exchanges of femoral component: Crowe grade I – 2 hips, Crowe grade IV – 1 hip), polyethylene liner wear n = 1 (Crowe grade I), late deep infection n = 1(Crowe grade I), periprosthetic fractures of the femur n = 2 (Crowe grade I – 1 hip, Crowe grade IV – 1 hip). The cause for revision after the placement of acetabular component in the secondary socket was aseptic loosening n = 1(Crowe grade II).
The comparison of radiological outcomes between the groups in the last follow-up is presented in Table 2. There was no significant difference between both groups.
Comparison of radiological outcomes between groups at final follow-up.
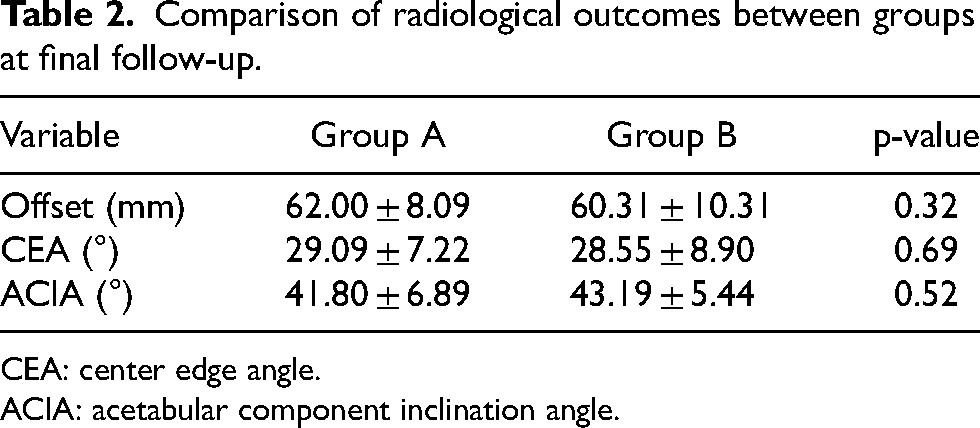
CEA: center edge angle.
ACIA: acetabular component inclination angle.
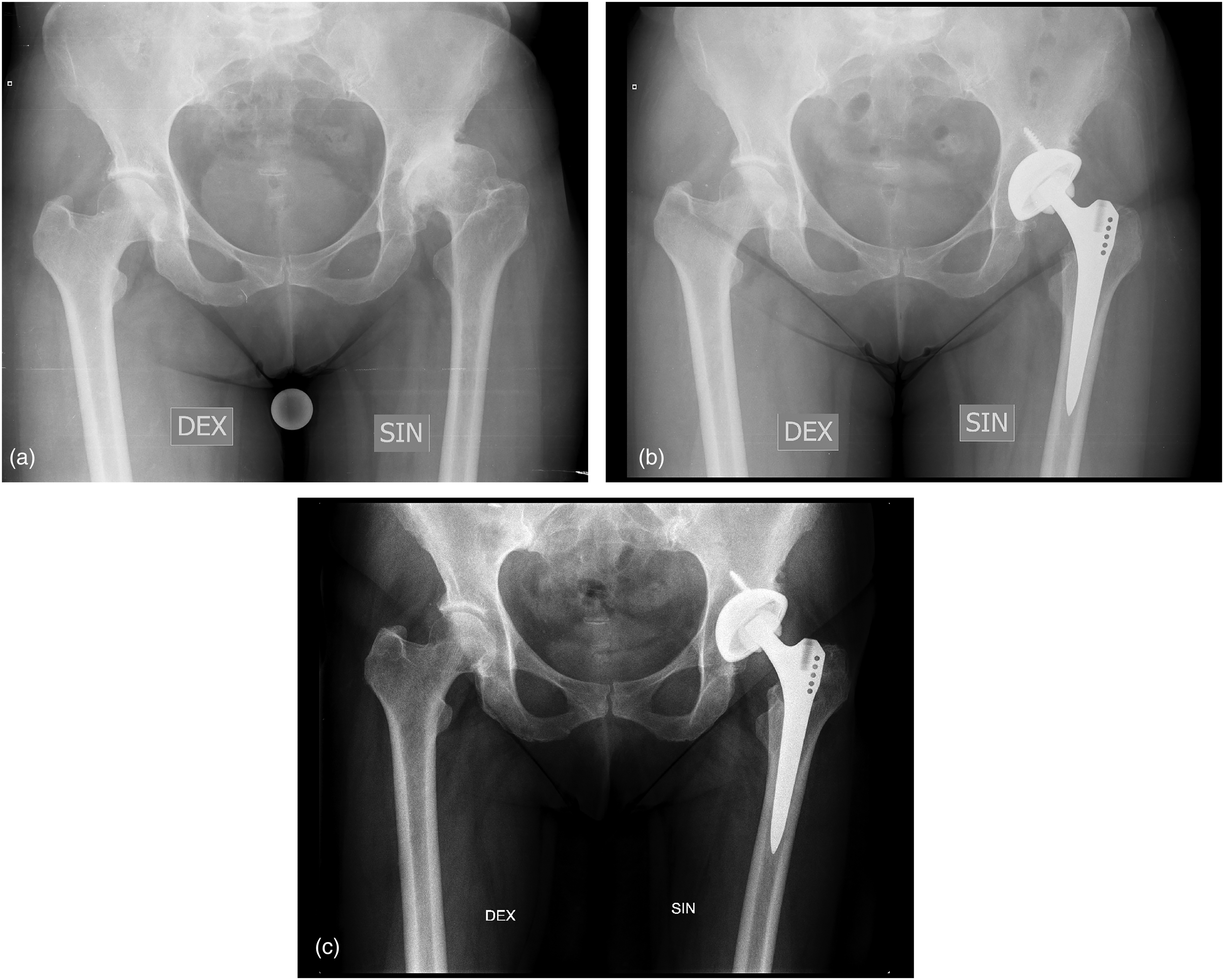
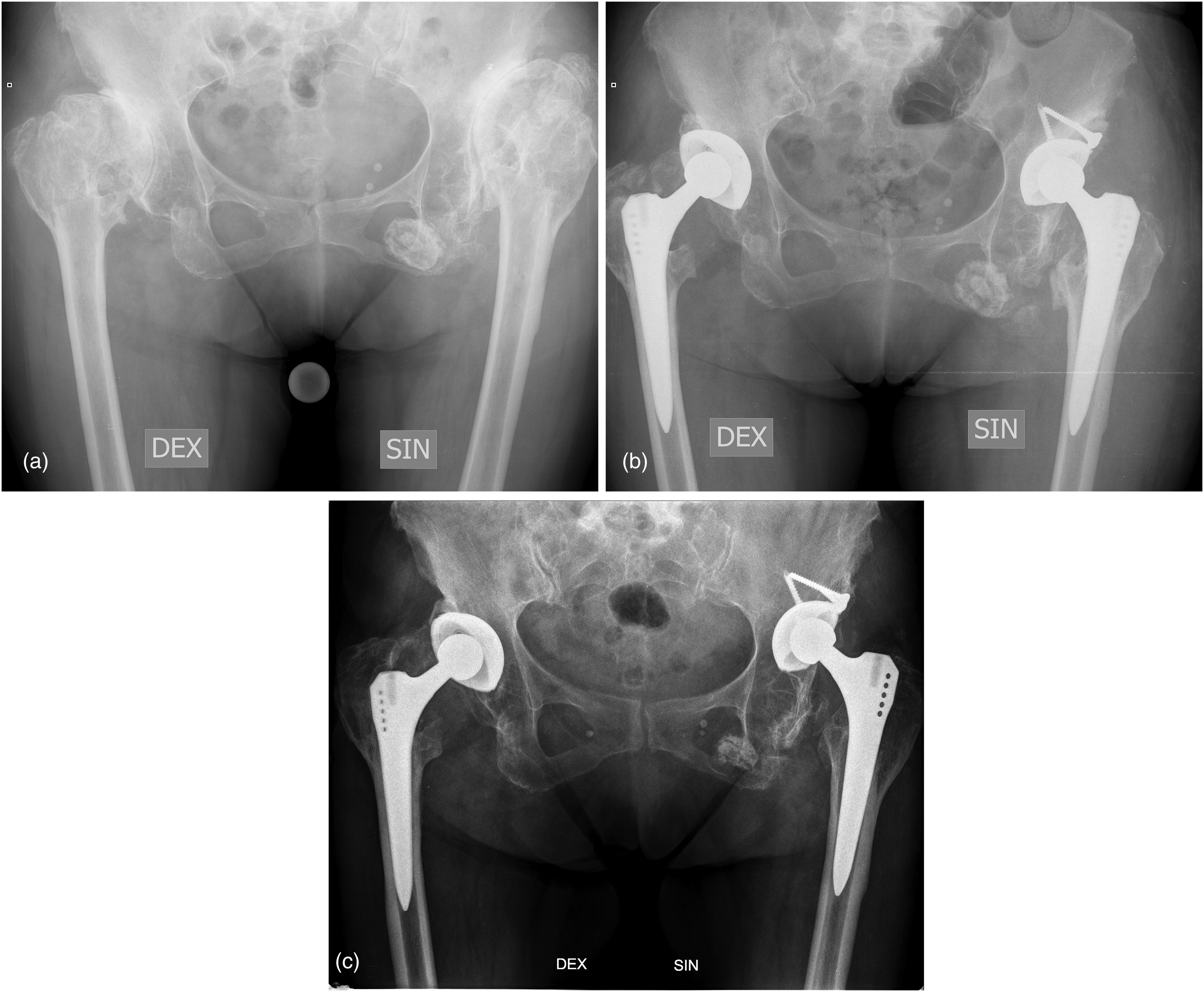
Representative case radiographs of group A are presented in Figure 3, of group B – in Figure 4.
Nine complications developed intraoperatively in group A patients. Six patients had fractures of the calcar region of the proximal femur – two Crowe I, two Crowe II, one Crowe III, one Crowe IV grades. One Crowe grade III patient had a fracture of the ischium bone. In cases of fracture of the proximal femur, the range of operation was increased and osteosynthesis of the femur with cerclage wires was performed. There was one sciatic nerve palsy and one femoral nerve neuropathy caused by traction during surgery, both were Crowe grade II patients.
Functional assessment of group A and group B patients was performed before THA, 1 year, and 10 years after THA by using the Merle d'Aubigné and Postel score.
The preoperative Merle d'Aubigné and Postel mean score for Crowe I was 9.98 ± 2.38, Crowe II ‒ 9.46± 2.18, Crowe III ‒ 7.81 ± 2.26, and Crowe IV grades ‒ 9.25 ± 2.22.
The mean Merle d'Aubigné and Postel score in patients in group A increased from mean 9.63 ± 2.17 preoperatively to 15.48 ± 2.26 in the final follow-up, in group B ‒ from 8.71 ± 2.21 preoperatively to 15.36 ± 1.78 in the final follow-up. No significant functional deterioration was found in the comparison between 1 year and 10 years after THA in both groups (p > 0.05). Functional results’ analysis of the groups A and B is presented in Figure 5.
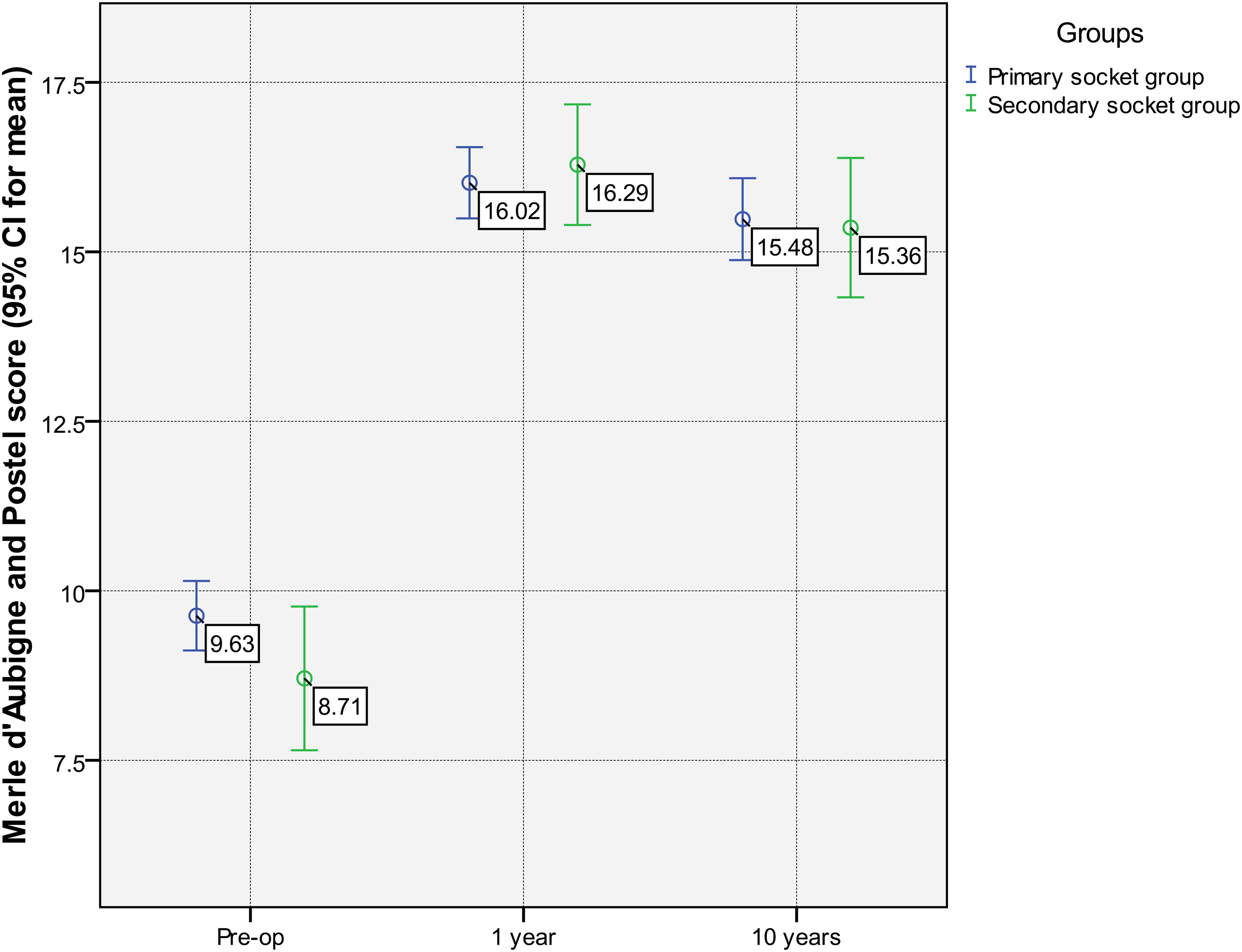
Merle d'Aubigné and Postel score preoperatively, 1 year, and 10 years after total hip arthroplasty in primary socket group (group A) and secondary socket group (group B).
Kaplan-Meyer implant survival was 91.9% in the 10th year the follow-up for all cases (Figure 6).
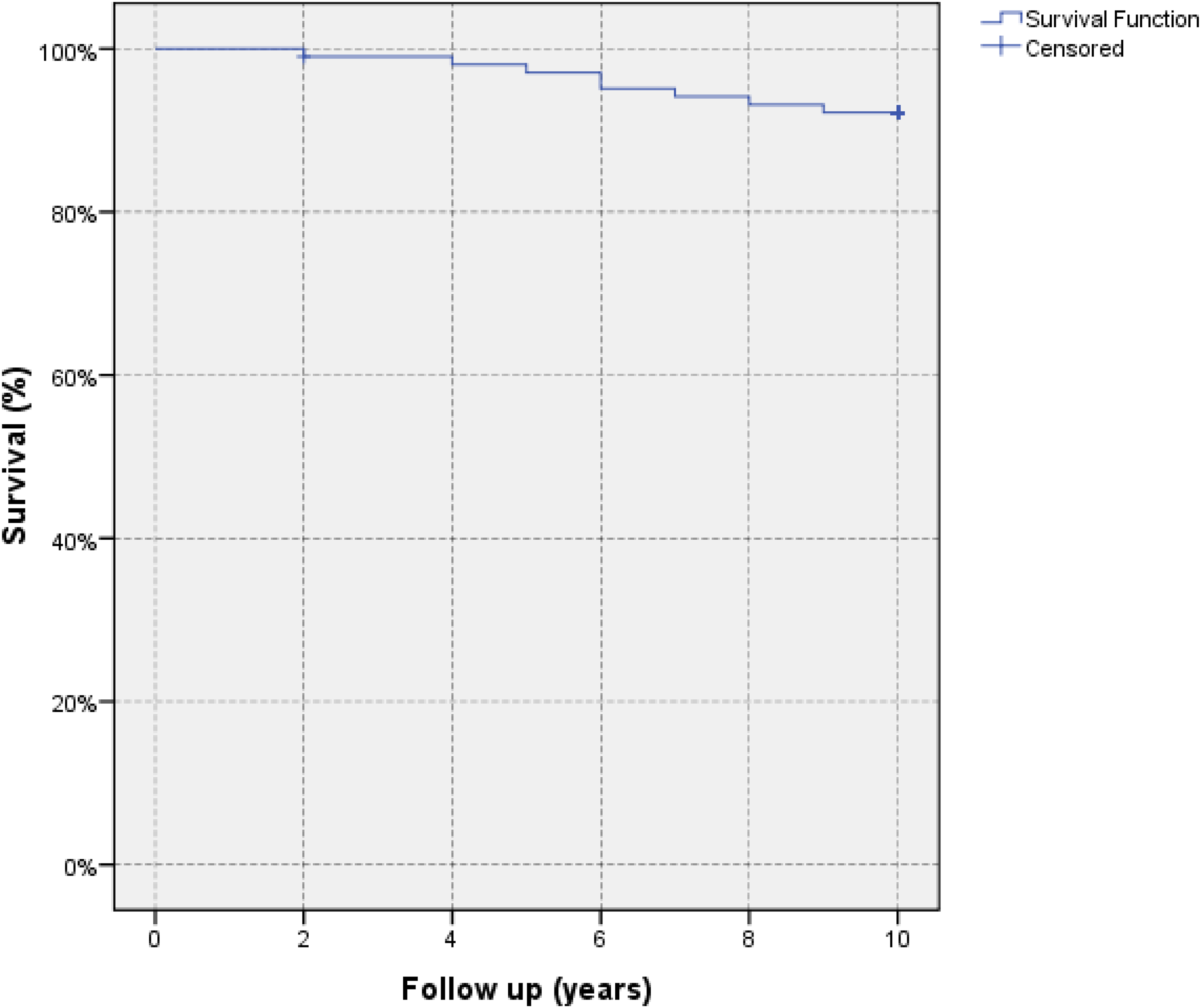
Kaplan–Meyer implant survival analysis in final follow-up.
Discussion
The placement of the acetabular component of endoprostheses in the primary or secondary socket has been the subject of discussion in literature for many years.11,12 It is difficult to achieve acceptable acetabular component coverage at the anatomical socket due to superolateral bone deficiency. De Jong et al. suggested that femoral head structural autograft can be used at the superolateral rim of acetabulum to provide additional support. 13 In turn posterosuperior bone above the primary socket is almost intact and acetabular component can be placed at high hip center. 14 We considered the placement of the acetabular component of endoprostheses in the secondary socket in Crowe grades II and III, where placement in the primary socket was doubtful without shortening of the femur, but adequate coverage of the acetabular component was possible to achieve by placing it in secondary socket. Watts et al. found higher incidence of aseptic loosening with superolateral placement of the acetabular component at a mean follow up of 10 years. 15 Shen et al. reported that medialization of the acetabular component prevented an increase joint reaction force and relieved the burden of abductor muscle which was disfunctional preopereatively due to shortening and subsequent atrophy. 14 In Crowe grades II and III we placed the acetabular component adjacent to the medial wall. In Crowe grade IV we performed placement of acetabular component in the primary socket because the bone stock was insufficient for high standing of this component.
The functional results are of major importance after THA. There was no significant difference between the functional results in patients with placement of acetabular component in the secondary or primary socket. The results in our study were comparable with results described by other long-term studies in recent literature. Montalti et al. reported the average prepoperative Merle d'Aubigne and Postel score as 9.3, postoperative 15.1. 6
The survival rate was reported by Montalti et al. 6 as 95.5% in 15.1 years, Flecher et al. 16 as 94% and Nawabi et al. 97% in 12 years mean follow-up. 17 In our study Kaplan-Meyer implant survival was 91.9% in the 10th year the follow-up for all cases.
Qian et al. discussed that acetabular reconstruction in the high hip center position needs no femur osteotomy and has a low risk for nerve injury. 18 In the current study, we did not find any intraoperative neurologic complications in the group B.
The effect on the biomechanics of the placement of acetabular component in the secondary socket has remained controversial in the literature for many years. Bicanic et al. wrote that a high position of acetabular component may be also acceptable in severe dysplasia cases which prevents the increase of hip load and provides good biomechanical environment for longer hip arthroplasty survival. 19 Thereby the placement of the acetabular component in the secondary socket allows to preserve the compensatory balance of muscles developed for many years. However, Karaismailoglu et al. argued that the high hip rotation center changed the hip biomechanical environment and resulted in abnormal hip biomechanics, which harmed the recovery of abductor muscle and the survival of acetabular component. 20
The short stems have been introduced for the surgery in young patients, including patients with DDH, with the intention of reducing the risk of periprosthetic bone resorption, thigh pain and to preserve as much bone as possible for any further revision. 21 In DDH patients the femoral challenges included a narrow medullary canal, excessive anteversion and high caput-collum-diaphyseal angle with metadiaphyseal mismatch and in these cases short stems can be choosen. 22 Although short stems are described for using in all Crowe grades DDH patients, in our knowledge only mid-term success of these stems in Crowe grade II patients is published. 23 Suksathien et al. stated that Crowe grade II DDH is the upper limit, above which the short stems should not be used. 22 Some authors are aware that there is still a lack of longer-term publications in outcome of short stems. 24 Morales De Cano et al. reported that severely dysplastic hips (Crowe grade III and IV) should be treated with modular stems that allow the possibility of anteversion correction perioperatively. 25 In our hospital standard cementless femoral stems were used also for relatively young patients including those who have osteoarthritis secondary to DDH.
The subtrochanteric osteotomy and shortening of the femur were not performed on group B patients. Tenotomies of abductors, adductors and, in rare cases, ileopsoas muscle were performed on Crowe grade IV patients.
Kaneuji et al. reported grade 1 heterotopic ossification occurred in 6 hips, although not to a degree that would cause a limited range of motion or pain, so no difference of intraoperative complications was observed. 26 We had observed postoperative heterotopic ossification grade I in 3 cases, none was operated on because of heterotopic ossification.
Nawabi et al. mentioned that the placement of an acetabular component in the high hip center may lead to a higher risk of dislocation but a lower risk of neurologic complications. 17 There were no dislocations in our study.
Incompetence of abductor mechanism, decreased range of movements were reportedly associated with the high hip center. 27 To achieve the best possible replacement surgery results, precise criteria for the choice of placement of the acetabular component were important.
Nerve palsies were described related to THA in patients with DDH. 28 In our study there was one sciatic nerve palsy and one femoral nerve neuropathy caused by traction during surgery in group A.
There were several limitations in this study. Firstly, the patients’ different functional demands and ability to recall information might affect the anamnesis and the interpretation of their complaints during the examination, as well as the ability to use the assessment scale. Secondly, patients were of different age groups, body mass indexes, duration of the operations. Different types of endoprostheses were used in the patients and they were operated on by several surgeons. We had difficulty to compare the contralateral side because the other hip had DDH or THA as the patients underwent bilateral THA consecutively, not simultaneously. This might create a disadvantage in homogenization of patients’ groups, group results are not generalizable to larger cohorts. Thirdly, Merles d'Aubigne and Postel's score was used in our hospital to evaluate the functional outcome preoperatively and postoperatively in THA. Although this method was described as objective and simple for the patients, the comparison with similar studies, by using other functional evaluation methods might be limited.
Conclusions
Functional outcome improvement was observed in long-term follow-up in both groups similarly, showing good functional results. Implants showed good survival rate. The placement of the acetabular component of endoprostheses in the secondary socket in Crowe II and Crowe III grades might be considered, where placement in the primary socket is not possible without shortening of the femur and it is possible to achieve adequate coverage of the acetabular component. It can lead to a lower intraoperative, early, and late complication rate. Nevertheless, the choice of placement of the acetabular component depends on the grade of DDH, expected elongation of the leg and the possibility of adequate bone coverage of the acetabular component.
Footnotes
Acknowledgement
The authors thank Karlis Birgelis for statistical analysis and consultation in the preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the local Ethics Committee of the Hospital of Traumatology and Orthopaedics, Riga, Latvia. The number of study approval 28/2021/1.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.